Arylsulfatase I is a prognostic biomarker for head and neck squamous cell carcinoma and Pan‐cancer
Abstract
Background:
Sulfatase gene family members mediate various biological functions in tumor stroma and tumor cell environments. However, the expressions and prognostic value of Arylsulfatase I (ARSI), a sulfatase gene family member, in head and neck squamous cell carcinoma (HNSC) have not been fully established.
Methods:
Arylsulfatase I expressions in pan‐cancer were profiled using publicly available databases. Then, univariate Cox regression, Kaplan–Meier, and the Pearson’s correlation analyses were performed to determine correlations between ARSI expressions and cancer prognosis, immune cell status, and drug sensitivity. Gene set variation analysis (GSVA) and gene set enrichment analysis (GSEA) were used to assess the potential mechanisms underlying ARSI functions in HNSC.
Results:
Arylsulfatase I was highly expressed in 15 cancer types, with significant expressions in HNSC. Elevated ARSI levels were associated with worse prognostic outcomes in HNSC patients. In addition, GSVA and GSEA showed that ARSI was highly involved in tumor cell escape and inflammatory responses. Expressions of ARSI negatively correlated with tumor mutation burden or microsatellite instability and positively correlated with immune‐related genes. Elevated ARSI expressions conferred poor tolerance to daporinad and sinularin, but increased cell sensitivity to dasatinib and XAV939.
Conclusion:
Arylsulfatase I is a promising prognostic and therapeutic target for HNSC.
Article type: Research Article
Keywords: drug sensitivity, GSEA, GSVA, HNSC, prognosis, tumor microenvironment
Affiliations: Department of Otolaryngology, Head and Neck Surgery, The Affiliated Lihuili Hospital Ningbo University Ningbo China; Department of Otolaryngology, Head and Neck Surgery Ningbo Medical Center Lihuili Hospital Ningbo China; Medical School of Ningbo University Ningbo China
License: © 2022 The Authors. Journal of Clinical Laboratory Analysis published by Wiley Periodicals LLC. CC BY 4.0 This is an open access article under the terms of the http://creativecommons.org/licenses/by/4.0/ License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Article links: DOI: 10.1002/jcla.24600 | PubMed: 35870182 | PMC: PMC9459304
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (12.3 MB)
INTRODUCTION
Squamous cell carcinoma (SCC), which arises from precancerous lesions with atypical squamous proliferation, is one of the most common types of pathology in head and neck cancer.ref. jcla24600-bib-0001 The head and neck squamous carcinoma (HNSC) often metastasizes to lymph nodes.ref. jcla24600-bib-0001 Risk factors for HNSC include human papillomavirus (HPV) infections, tobacco consumption, and alcohol use.ref. jcla24600-bib-0002 More than 500,000 patients with HNSC undergo radiotherapy and other therapeutic treatments annually. However, patients with head and neck cancer, especially men, have high recurrence and mortality rates.ref. jcla24600-bib-0003 The lack of reliable, independent biomarkers for early diagnosis as well as prediction of survival and responses to treatment are a challenge to clinical management HNSC.
Chronic inflammation, immune escape, metabolic reprogramming, cellular senescence, and genome mutations are some of the mechanisms involved in carcinogenesis. However, these mechanisms have not been fully investigated in HNSC.ref. jcla24600-bib-0004, ref. jcla24600-bib-0005, ref. jcla24600-bib-0006
Arylsulfatase I (ARSI) is one of the seventeen members of sulfatase gene family, whose aberrant expressions contribute to cancer cell migration.ref. jcla24600-bib-0007, ref. jcla24600-bib-0008 ARSI is mainly expressed in embryonic tissues and is associated with tissue remodeling.ref. jcla24600-bib-0009 However, the role of ARSI in HNSC is yet to be defined. We evaluated the genetic background of HNSC to characterize the significance of ARSI in HNSC progression. Transcriptome and clinical data were extracted from the Cancer Genome Atlas head and neck squamous carcinoma cohort (TCGA‐HNSC). Then, expressions of ARSI in all cancer types were evaluated, and its prognostic value, including in overall survival (OS), disease‐specific survival (DSS), disease‐free interval (DFI), and progression‐free interval (PFI), determined. The associations between ARSI and immune scores, stromal scores, ESTIMATE scores, and tumor purity were also evaluated. Besides, comprehensive analyses of the ARSI gene at tumor mutation burden (TMB) and microsatellite instability (MSI) levels were performed. Then, correlations between differential expressions of ARSI and anticancer drug sensitivity were assessed. Our findings highlight potential tumor immunotherapy targets and provide novel insights into precise diagnosis and early interventions to improve the survival rate of HNSC patients.
METHODS
Data collection and processing
The UCSC XENA website (https://xenabrowser.net/datapages/), which includes various transcriptomic datasets, such as the TCGA portal; the Genotype‐Tissue Expression (GETx) project and Cancer Cell Line Encyclopedia (CCLE) was used in this study. The data are publicly available and open‐ended, and require no ethics approval. We retrieved somatic cell mutations, CNAs, and methylation data on ARSI from tissue samples in 33 cancer types using cBioPortal. Genetic data types, including somatic cell mutations, DNA copy number alterations (CNAs), and DNA methylation, were integrated by cBioPortal (https://www.cbioportal.org/). One HNSC dataset (GSE41613) was downloaded from the Gene Expression Omnibus (GEO) database to validate the prognostic role of ARSI and the relationship between ARSI expressions and infiltrating immune cells.
Analysis of the relationship between ARSI and prognosis
The four major prognostic factors (OS, DSS, DFI, and PFI) were used to define the relationship between ARSI expressions and prognostic outcomes for 33 cancer types using univariate proportional hazards regression. Thereafter, Kaplan–Meier estimates and log‐rank tests were used to assess survival outcomes for several cancer types with elevated ARSI levels and poor prognosis (p < 0.05). The R packages “survival” (http://cran.rproject.org/web/packages/survival/index.html) and “survminer” (https://cran.r‐project.org/web/packages/survminer/index.html) were used in these analyses.
GSVA and GSEA
Using “GSVA” in R, Gene Set Variation Analysis (GSVA), a non‐parametric and unsupervised software algorithm, was employed to analyze the associations between ARSI expressions and hallmark gene sets, which represent well‐defined biological processes in cancers. In addition, gene set enrichment analysis (GSEA; http://www.broadinstitute.org/gsea/) was performed to investigate the significance of ARSI gene signatures. GSEA is a tool for analyzing genome microarray data, creating a molecular signature database based on known positions, characteristics, and functions of different gene sets.
Correlations between ARSI expressions and tumor microenvironment
We systematically analyzed the immune, stromal, and ESTIMATE scores as well as tumor purity in different cancer types using the “estimate” R package. Then, correlations between ARSI expressions and immune infiltrating scores of twenty‐four immune cells, which had been obtained from the Tumor Immune Evaluation Resource (TIMER) database, were evaluated. In addition, Pearson correlation analysis was performed to assess the relationship between ARSI expressions and infiltrating immune cells, including B cells, CD4+ T cells, CD8+ T cells, NK cells, mast cells, macrophages, dendritic cells, and neutrophils.
Correlations between ARSI expressions and TMB, MSI, Immune‐related genes (IRGs), or drug sensitivity
TMB, MSI, and IRGs are significant biomarkers in the tumor microenvironment (TME). The R software was used to assess the relationships between ARSI expressions and levels of TMB, MSI, or IRGs. Associations between ARSI gene expressions and small molecule drugs from Genomics of Drug Sensitivity in Cancer (GDSC, https://www.cancerrxgene.org) were also evaluated.
Statistical analysis
All statistical analyses were performed in R software (version 4.1.1). Differences in ARSI expressions were evaluated using the Student’s t‐test or paired t‐test. Spearman correlation analyses were performed to establish correlations between ARSI expressions and drug IC50. *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001, ns: non‐significant.
RESULTS
ARSI expressions in human cancers and normal tissues
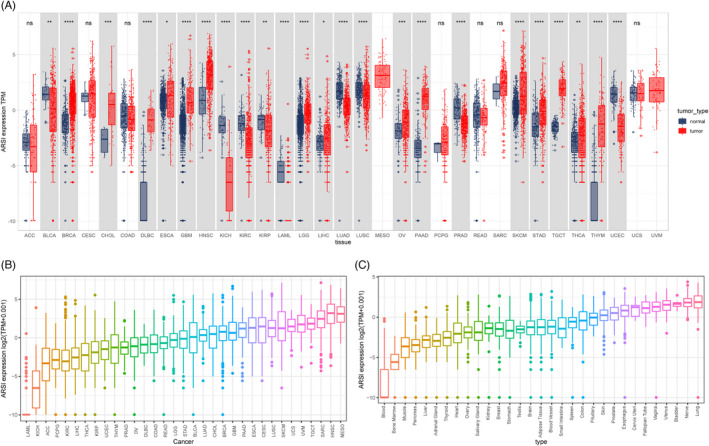
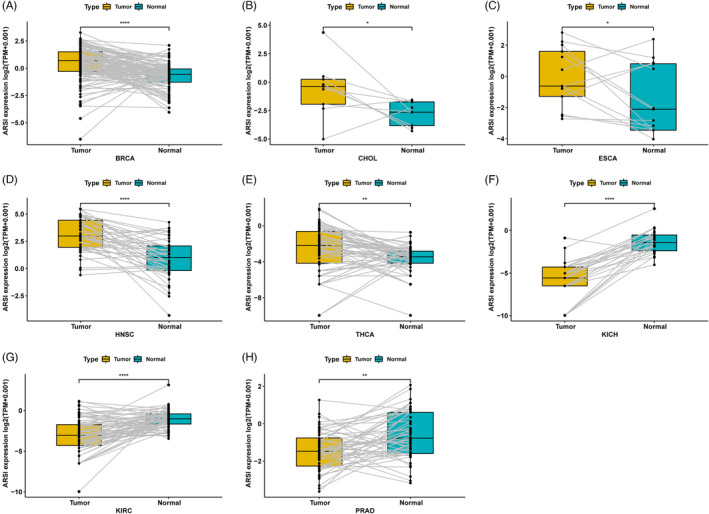
Analyses of data from TCGA and GTEx databases revealed that ARSI expressions in BRCA, CHOL, DLBC, ESCA, GBM, HNSC, LGG, LIHC, OV, PAAD, SKCM, STAD, TGCT, THCA, and THYM tumors were higher, compared with their corresponding normal samples (p < 0.05; Figure 1A). In 33 tumor types, HNSC exhibited the highest levels of ARSI, followed by MESO (Figure 1B). Analysis of physiologic ARSI gene expressions across tissues using the GTEx data set (Figure 1C) revealed elevated expressions in lungs and lowest levels in blood. In addition, ARSI expressions were elevated in TCGA BRCA, CHOL, ESCA, HNSC, and THCA cohorts, compared with adjacent normal tissues (Figure 2A–E). Thus, ARSI may have a significant role in HNSC pathogenesis.
The landscape of ARSI genetic alterations in cancer
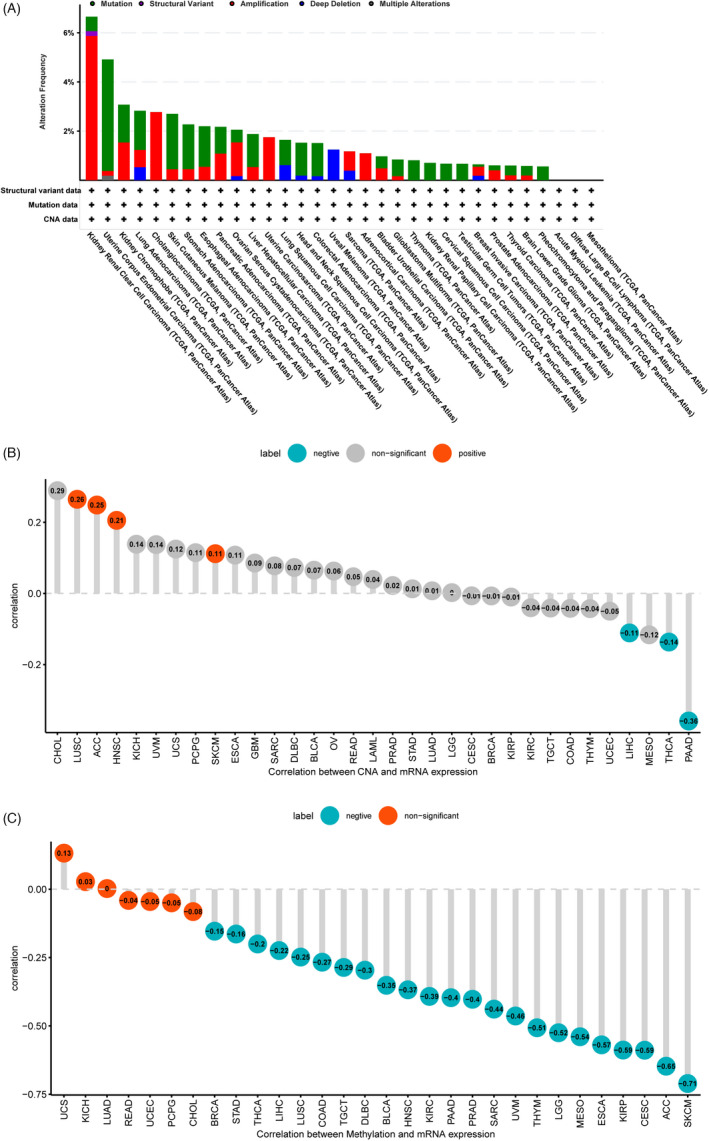
cBioPortal, which has more than 28,000 tumor samples, was used to investigate genetic alterations of ARSI. It was revealed that KIRC had high mutation levels with an ARSI alteration frequency exceeding 6% (Figure 3A). The ARSI genetic alterations were mainly associated with HNSC. Furthermore, there were positive correlations between CNA and mRNA levels of ARSI in LUSC, ACC, HNSC, and SKCM, but negative correlations in PAAD, THCA, and LICH (Figure 3B). Methylation levels of the ARSI promoter were negatively correlated with ARSI expressions in 23 cancer types and were most pronounced in SKCM (Figure 3C).
Prognostic significance of ARSI in pan‐cancer
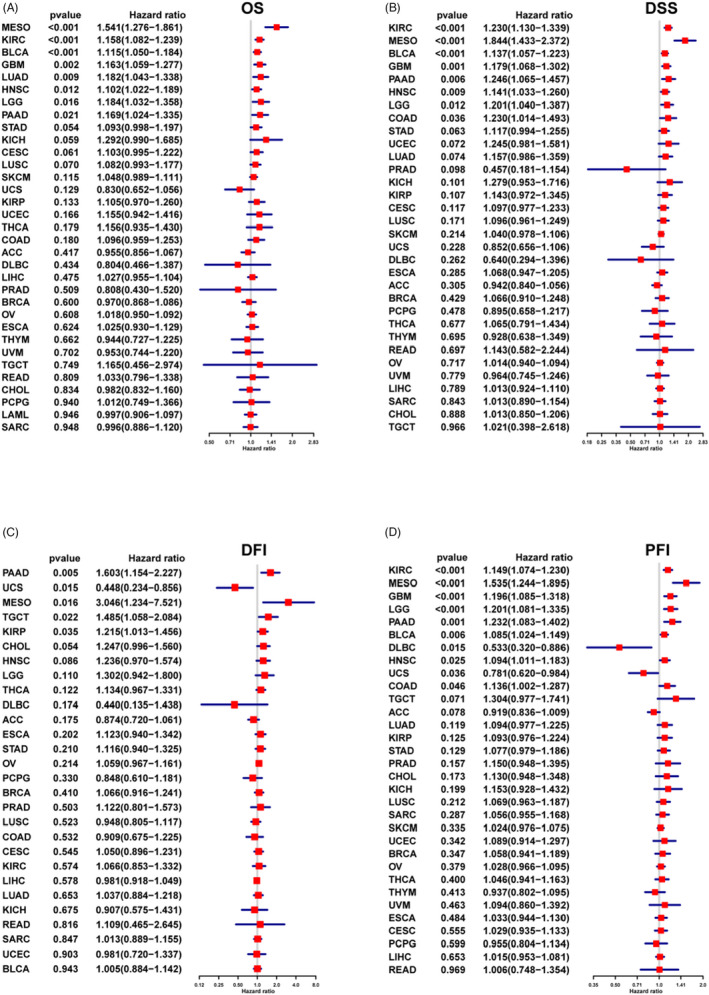
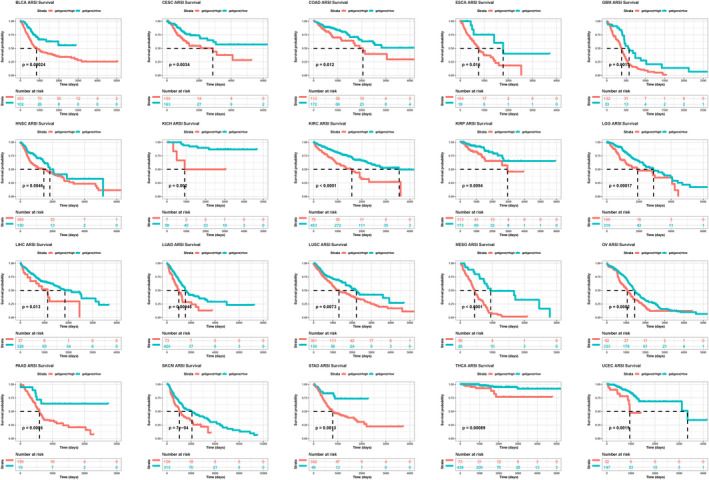
The overall survival analysis revealed that ARSI is a risk factor in patients with MESO, KIRC, BLCA, GBM, LUAD, HNSC, LGG, or PAAD, particularly in MESO (Figure 4A). The DSS analysis revealed significantly high hazard ratios for the ARSI gene in KIRC, MESO, BLCA, GBM, PAAD, HNSC, LGG, and COAD (Figure 4B). The DFI analysis showed that higher ARSI expressions were associated with poorer DFI in PAAD, MESO, TGCT, and KIRP. In contrast, elevated ARSI expressions were significantly associated with better DFI in UCS (Figure 4C). ARSI was found to be a protective factor for patients with DLBC and UCS, and a risk factor for patients with KIRC, MESO, GBM, LGG, PAAD, BLCA, HNSC, and COAD (Figure 4D). Kaplan–Meier survival analysis was used to study the association between ARSI expressions and prognostic outcomes in various cancers. ARSI was found to be a high‐risk gene in 20 cancer types, including BLCA, CESC, COAD, ESCA, HNSC, KICH, KIRC, LIHC, LUAD, LUSC, MESO, SKCM, STAD, THCA, and UCEC (Figure 5). The GSE41613 dataset was used for survival analysis to validate the survival value of ARSI (Figure S1).
GSVA of ARSI
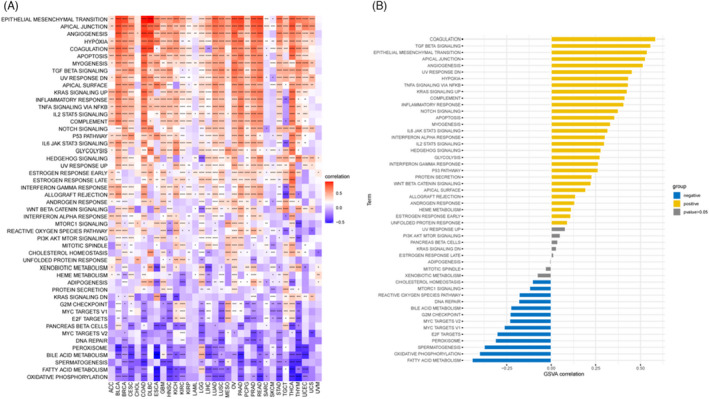
To assess the biological significance of ARSI expressions in different tumor tissues, GSVA was performed to compare gene expressions in 33 tumors with 50 gene sets. Figure 6A shows that some pathways were positively or negatively associated with ARSI expressions in various tumors. In most cancers, ARSI had significant positive correlations with 27 cancer‐related Hallmark pathways, including “EPITHELIAL MESENCHYMAL TRANSITION,” “APICAL JUNCTION,” “ANGIOGENECIS,” “HYPOXIA,” “COAGULATION,” “APOPTOSIS,” “MYOGENESIS,” “TGF BETA SIGNALING,” “UV RESPONSE DN,” “APICAI SURFACE,” “KRAS SIGNALING UP,” “INFLAMMATORY RESPONSE,” “TNFA SIGNALING VIA NFKB,” “IL2 STATS SIGNALING,” “COMPLEMENT,” “NOTCH SIGNALING,” “P53 PATHWAY,” “IL6 JAK STAT3 SIGNALING,” “GLYCOLYSIS,” “HEDGEHOG SIGNALING,” “UV RESPONSE UP,” “ESTROGEN RESPONSE EARIY,” “ESTROGEN RESPONSE LATE ” “INTERFERON GAMMA RESPONSE,” “ALLOGRAFT REJECTION,” “ANDROGEN RESPONSE,” and “WNIERPTACAI‐MINISIGNAHING.” In addition, ARSI exhibited positive correlations with other pathways such as “INTERFERON ALPHA RESPONSE,” “IL2 STAT5 SIGNALING,” “PROTEIN SECRETION,” “WNT BETA CATENIN SIGNALING,” “APICAL SURFACE,” “HEME METABOLISM,” and “UNFOLDED PROTEIN RESPONSE” in HNSC (Figure 6B).
GSEA enrichment analysis of ARSI
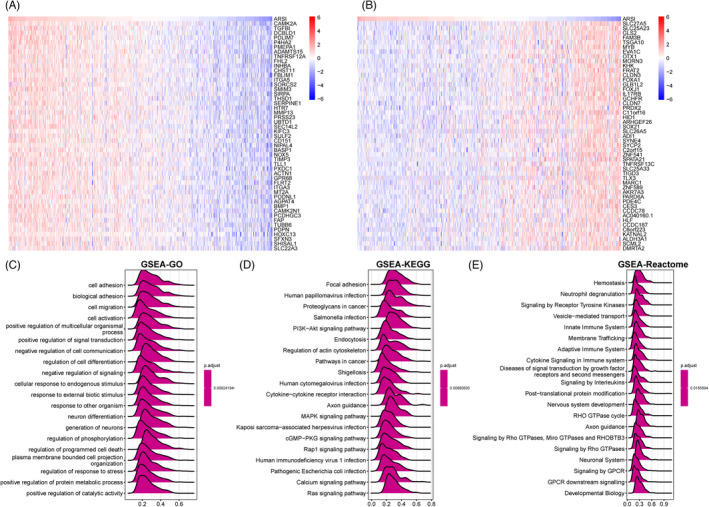
The Spearman test was used to identify differentially expressed genes (DEGs) that were positively and negatively correlated with ARSI in HNSC. The top 50 positively (r > 0) and top 50 negatively (r < 0) correlated genes are shown in heat maps (Figure 7A,B). Thereafter, based on correlation analysis results, GSEA enrichment analysis was performed using “clusterpofiler” in R, which included GO, KEGG, and Reactome annotations. It was established that ARSI was significantly associated with pathways that mediate tumor cell invasion, migration, and metastasis in HNSC (Figure 7C–E).
Correlations between ARSI and tumor microenvironment (TME)
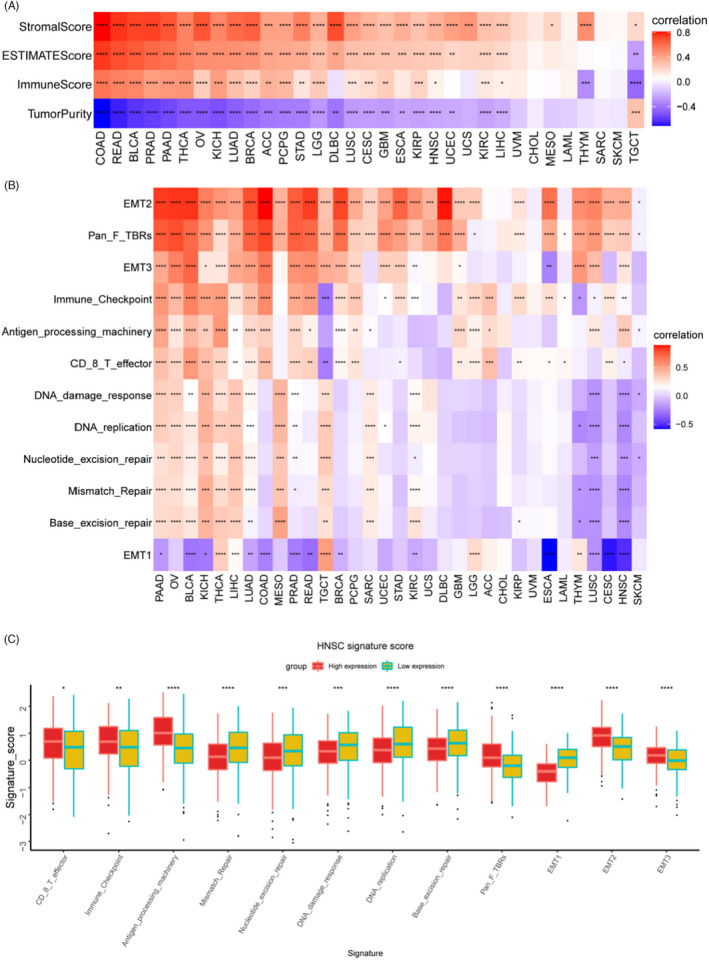
To determine whether ARSI is involved in immune cell infiltrations in the TME, the “ESTIMATE” package was used to evaluate the associations between ARSI expressions and stromal, immune, and ESTIMATE scores or tumor purity (Figure 8A). ARSI exhibited the highest correlations with stromal scores and immune scores in COAD. Besides, apart from TGCT, ARSI was negatively correlated with tumor purity in 24 cancer types (p < 0.05). The relationships between ARSI expressions and immune‐related genes, DNA repair damage, and metastasis‐related pathways were also assessed. There were significant positive correlations between elevated ARSI expressions and the above‐mentioned pathways in PAAD, apart from EMT1 (Figure 8B). Correlations between ARSI transcript levels and signature scores of pathways in HNSC are shown in a boxplot (Figure 8C).
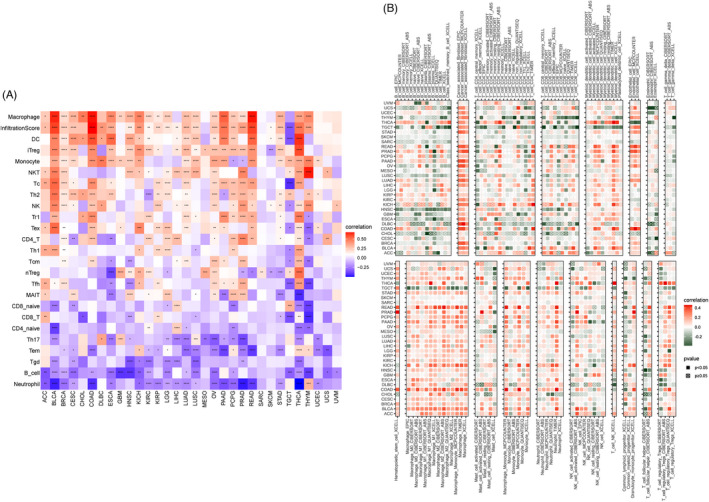
Analysis of data from the ImmuCellAI database revealed that ARSI was positively correlated with infiltration levels of macrophages, DC, iTerg, monocytes, and NKT cells, but negatively correlated with neutrophils, B cells, Tgd, Tem, and Th17 cells in TCGA pan‐cancer (Figure 9A). Analysis of data from the TIMER database showed that ARSI was positively correlated with infiltration levels of macrophages, cancer‐associated fibroblasts, DC, endothelial cells, and monocytes, but negatively correlated with neutrophils, B cells, and follicular helper T cells in TCGA pan‐cancer (Figure 9B). The GSE41613 dataset was used to validate that ARSI is important for immune cell infiltrations in the HNSC microenvironment (Figure S2).
Associations between ARSI and tumor immune responses
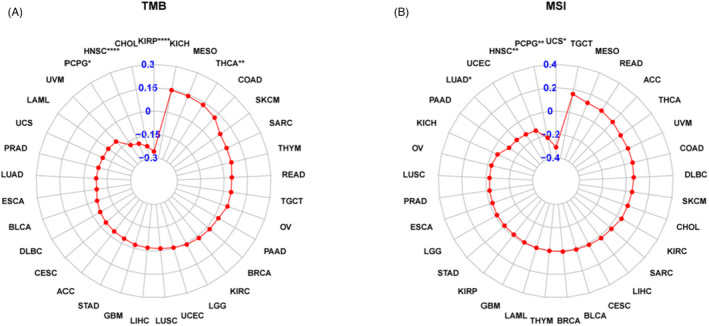
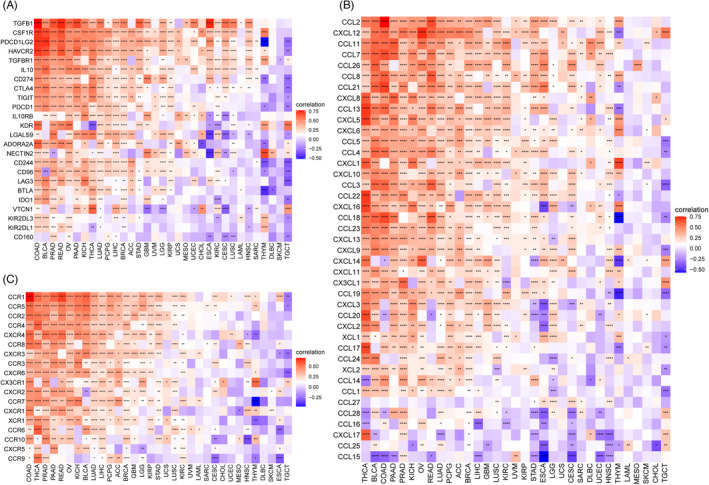
To define the roles of ARSI in immune mechanisms and responses, we assessed the interactions between ARSI levels and TMB, MSI, or IRGs, which could represent tumor immunogenicity and predict responses to immunotherapeutic agents. Figure 10A shows that ARSI mRNA expressions were negatively correlated with TMB in KIRP, HNSC, and PCPG, and positively correlated with THCA. Moreover, ARSI mRNA expressions exhibited negative correlations with MSI in UCS, PCPG, and HNSC (Figure 10B). Pan‐cancer analysis showed that ARSI mRNA expressions were associated with almost all immunosuppressive‐associated genes in most cancers, apart from DLBC and SKCM (Figure 11A–C). Among these cancer types, THCA, BLCA, COAD, PAAD, PRAD, KICH, OV, READ, LUAD, PCPG, ACC, and BRCA exhibited the highest coefficients, implying positive correlations between ARSI mRNA expressions and chemokine‐ or chemokine receptor‐associated genes.
ARSI and drug sensitivity
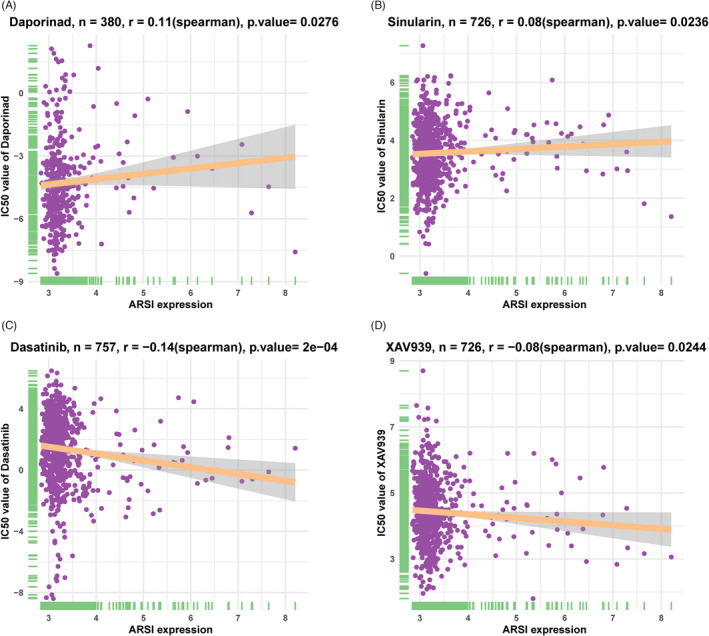
The GDSC data were used for drug sensitivity analysis of the ARSI gene via Spearman correlation tests, which yielded Spearman correlation coefficients. The top 2 positively (r > 0) and top 2 negatively (r < 0) correlated drugs were assessed using the “ggplot2” in R. Figure 12 shows that elevated expressions of ARSI conferred lower tolerance of cells to daporinad and sinularin, but increased cell sensitivity to dasatinib and XAV939.
DISCUSSION
A combination of molecular‐targeted therapies with immune checkpoint inhibitors (ICIs) is an effective therapeutic approach for cancer patients, especially HNSC.ref. jcla24600-bib-0010, ref. jcla24600-bib-0011, ref. jcla24600-bib-0012, ref. jcla24600-bib-0013, ref. jcla24600-bib-0014 Although some of the molecular‐targeted drugs and ICIs for HNSC, such as anti‐PD‐1 antibodies, nivolumab, and pembrolizumab, are effective, genetic changes in patients alter therapeutic responses. Therefore, it is important to identify and validate efficient prognostic and diagnostic biomarkers in HNSC.
Arylsulfatase I is different from all the other members of sulfatase family that span across 8–20 exons.ref. jcla24600-bib-0015 ARSI, a secreted protein that functions in the extracellular environment, is rapidly degraded in the endoplasmic reticulum (ER) or medium. Excess ARSI is retained in the ER, in a denatured form, to lead to SUMF1 degradation.ref. jcla24600-bib-0016 Expressions of ARSI have been evaluated in different human tissues and cancer cell lines.ref. jcla24600-bib-0009 ARSI was found to be principally expressed in embryonic tissues and in the A549 cell line, which originates from lung carcinoma. ARSI is involved in tissue remodeling during tumor growth, as well as during embryonic development. Even though the ARSI gene has been studied, its role in tumorigenesis has not been fully established.
In this study, we found that ARSI levels were highly elevated in tumor tissues, especially HNSC, compared with normal or adjacent non‐tumor tissues. In addition, there was a positive correlation between CNA and ARSI mRNA expressions and negative correlations with dysregulated methylation levels of the ARSI promoter in HNSC. These results suggest that overexpressions and genetic changes in ARSI mediate HNSC tumorigenesis. The prognostic value of ARSI has been reported in various cancer types, including HNSC. Our survival assays revealed that elevated ARSI expressions were associated with poorer prognostic outcomes (OS, DSS, and PFI), relative to low ARSI expressions. In contrast, although DFI was not significantly correlated with ARSI expressions (p = 0.086), there was a trend toward worse DFI for patients with high ARSI mRNA expressions (HR = 1.236, 95% CI = 0.970, 1.574) in univariate analysis. These findings imply that ARSI is a potential prognostic indicator in HNSC.
Our GSVA analysis showed that elevated ARSI expressions in HNSC were associated with consistent and significant dysregulation of coagulation, transforming growth factor (TGF)‐β signaling, epithelial–mesenchymal transition (EMT), apical junction, and angiogenesis gene sets. Furthermore, GSEA analysis showed that cell adhesion, biological adhesion, cell migration, or cell activation were potential mechanisms for HNSC progression. These results imply that ARSI may be associated with cell adhesion and cell migration in the TME, facilitating cancer cell migration and invasion.
In this study, ARSI expressions were associated with tumor‐infiltrating immune cells, which could influence tumor behaviors in multiple cancer types. For instance, ARSI was positively correlated with infiltrations of macrophages, monocytes, and cancer‐associated fibroblasts and negatively correlated with B cells, CD8+ T cells, and follicular helper T cells in HNSC. Macrophages and monocytes exhibited several protumorigenic abilities, which promoted tumor cell proliferation and metastasis.ref. jcla24600-bib-0017, ref. jcla24600-bib-0018 Cancer‐associated fibroblasts secrete numerous extracellular matrix molecules, chemokines, cytokines, and growth factors to create a favorable microenvironment for tumor progression and invasion.ref. jcla24600-bib-0019, ref. jcla24600-bib-0020 We found that ARSI was positively correlated with stromal, immune, and ESTIMATE scores in HNSC. Besides, ARSI expressions were significantly and positively associated with immune‐related and metastasis‐related pathways, but negatively correlated with DNA damage‐related and repair‐related pathways. Data suggest that ARSI may be involved in tumor immune evasion, leading to poor prognosis of HNSC.
Tumor mutation burden is a reliable biomarker for immunotherapeutic responses.ref. jcla24600-bib-0021 Cancer patients with high TMB have poor prognostic outcomes. High‐MSI tumor may have a favorable inflammatory TME and a better sensitivity to ICIs.ref. jcla24600-bib-0022, ref. jcla24600-bib-0023 Besides, IRGs play critical roles in transcriptional and microenvironmental alterations, and represent a novel predictor of clinical efficacy in cancer.ref. jcla24600-bib-0024 Therefore, we assessed the relationship between ARSI expressions and TMB/MSI/IRGs. We found that ARSI expressions had strong negative correlations with TMB and MSI but slightly negative correlations with IRGs in HNSC. These findings show that TMB, MSI, and IRGs mediate the effects of ARSI in molecular‐targeted therapies and ICIs prognosis. Spearman correlation tests showed that HNSC patients with upregulated ARSI levels had poor tolerance to daporinad (r = 0.11) and sinularin (r = 0.08), but were slightly sensitive to dasatinib (r = −0.14) and XAV939 (r = −0.08). These results suggest that HNSC patients with high ARSI expressions may not be suitable for immunosuppressive therapy.
Although our study analyzed ARSI expressions in 33 tumors, our data sources were mainly derived from UCSC XENA and GDSC databases. Besides, we only used retrospective data; thus, there is a need for further validation in larger, prospective clinical trials. In addition, we found that ARSI expressions were associated with immune cell infiltrations and tumor metastasis, but not their causality.
In conclusion, ARSI is a promising prognostic biomarker in pan‐cancer, especially HNSC. These findings may inform clinical decisions and cancer treatment.
FUNDING INFORMATION
This study was funded by Ningbo Health Branding Subject Fund (No.PPXK2018‐02); Zhejiang Provincial Natural Science Foundation of China (LY19H160014; LQ21H130001); Ningbo “Technology Innovation 2025” Major Special Project (2020Z097; 2018B10015); Medical and Health Research Project of Zhejiang Province (2019ZD018; 2021KY307).
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
Supplementary Materials
References
- p90 ribosomal S6 kinase 2 promotes invasion and metastasis of human head and neck squamous cell carcinoma cells.. J Clin Invest., 2010. [PubMed]
- p16 protein expression and human papillomavirus status as prognostic biomarkers of nonoropharyngeal head and neck squamous cell carcinoma.. J Clin Oncol., 2014. [PubMed]
- Sparing the region of the salivary gland containing stem cells preserves saliva production after radiotherapy for head and neck cancer.. Sci Transl Med., 2015
- Inflammation and tumor progression: signaling pathways and targeted intervention.. Signal Transduct Target Ther., 2021. [PubMed]
- Metabolic reprogramming and cancer progression.. Science., 2020. [PubMed]
- Hallmarks of cancer: new dimensions.. Cancer Discov., 2022. [PubMed]
- Lysosomal sulfatases: a growing family.. Biochem J., 2020. [PubMed]
- Sulfation pattern in glycosaminoglycan: does it have a code?. Glycoconj J., 2004. [PubMed]
- Molecular cloning and initial characterization of three novel human sulfatases.. Gene., 2006. [PubMed]
- Molecular alterations and targeted therapy in pancreatic ductal adenocarcinoma.. J Hematol Oncol., 2020. [PubMed]
- Molecular mechanisms and targeted therapies including immunotherapy for non‐small cell lung cancer.. Curr Cancer Drug Targets., 2019. [PubMed]
- Current insights into combination therapies with MAPK inhibitors and immune checkpoint blockade.. Int J Mol Sci., 2020
- Systemic therapies for intrahepatic cholangiocarcinoma.. J Hepatol., 2020. [PubMed]
- Current trends and future prospects of molecular targeted therapy in head and neck squamous cell carcinoma.. Int J Mol Sci., 2020
- Sulfatases and sulfatase modifying factors: an exclusive and promiscuous relationship.. Hum Mol Genet., 2005. [PubMed]
- Characterization of the arylsulfatase I (ARSI) gene preferentially expressed in the human retinal pigment epithelium cell line ARPE‐19.. Mol Vis., 2009. [PubMed]
- Macrophages as key drivers of cancer progression and metastasis.. Mediators Inflamm., 2017. [PubMed]
- Patrolling monocytes control tumor metastasis to the lung.. Science., 2015. [PubMed]
- Cancer‐associated fibroblasts: how do they contribute to metastasis?. Clin Exp Metastasis., 2019. [PubMed]
- Cancer‐associated fibroblasts in hepatocellular carcinoma.. World J Gastroenterol., 2016. [PubMed]
- Development of tumor mutation burden as an immunotherapy biomarker: utility for the oncology clinic.. Ann Oncol., 2019. [PubMed]
- The clinical utility of microsatellite instability in colorectal cancer.. Crit Rev Oncol Hematol., 2021. [PubMed]
- MSI as a predictive factor for treatment outcome of gastroesophageal adenocarcinoma.. Cancer Treat Rev., 2020. [PubMed]
- Identifying baseline immune‐related biomarkers to predict clinical outcome of immunotherapy.. J Immunother Cancer., 2017. [PubMed]