
Compassion Fatigue Among Critical Care Nurses and Physicians: A Scoping Review
Abstract
Introduction:
The continuous engagement with critically ill patients leaves healthcare providers vulnerable to Secondary Traumatic Stress (STS), consequently developing Compassion Fatigue (CF). Nurses’ compassion is crucial for healing and is associated with improved care delivery. Hence the purpose of this review is to evaluate the literature related to CF among Nurses and Physicians in the Critical Care area, with an emphasis on the prevalence of burnout (BO), STS and CF.
Design:
A scoping review.
Methods:
Two main electronic databases, namely Ovid Medline and CINAHL, were used to identify the relevant studies published. Google Scholar, PubMed and hand searching were used to scan the grey literature and otherwise missed peer reviewed literature. Following the title and abstract review, full‐text articles were screened for relevance, and study data were extracted. A narrative approach to synthesising the literature was used.
Results:
There is a lack of consensus on conceptualisation and operationalisation of CF. The predictors of CF vary among studies. Most of the studies reported a low to moderate level of CF. Only 2 studies reported high scores of BO, STS and CF.
Conclusion:
This paper has highlighted numerous gaps which necessitate further investigations. Despite increased recognition of CF in the healthcare field, its impact and preventive interventions remain limited.
Clinical Relevance:
Addressing CF among critical care providers is vital for improving the well‐being of providers, ensuring better patient care, and encouraging healthy and safe work environments.
Article type: Review Article
Keywords: burnout, compassion fatigue, critical care healthcare providers, critical care nurse, secondary traumatic stress
Affiliations: Hariri School of Nursing American University of Beirut Lebanon; Tulane University, School of Social Work New Orleans Louisiana USA
License: © 2025 The Author(s). Nursing Open published by John Wiley & Sons Ltd. CC BY 4.0 This is an open access article under the terms of the http://creativecommons.org/licenses/by/4.0/ License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Article links: DOI: 10.1002/nop2.70410 | PubMed: 41432276 | PMC: PMC12723723
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (511 KB)
Introduction
Nurses’ work‐related stress is higher in certain specialties than in others due to the patients’ increased psychological and physiological needs for compassionate care (Jin et al. ref. 2021). This stress, particularly evident in critical care settings, can result in indirect trauma, as a result of repeated exposure to trauma survivors, ultimately giving rise to psychological conditions such as Secondary Traumatic Stress (STS), Compassion Fatigue (CF), or Vicarious Trauma (Figley ref. 1995; Tarshis and Baird ref. 2019). Critical care nurses are more vulnerable to traumas, which can be psychologically, physiologically, and emotionally draining (Milligan and Almomani ref. 2020). Nurses and physicians frequently encounter critical patients’ conditions, which can lead to STS, a psychological condition stemming from experiencing someone else’s suffering, when left untreated, may evolve into CF. This vulnerability arises from caring for chronically and terminally ill patients, making ethical decisions, managing with medical errors, facing communication challenges, and addressing the needs of patients’ relatives (Curtis et al. ref. 2014; Epp ref. 2012; Todaro‐Franceschi ref. 2013). Critical care nurses and physicians experience moderate to high levels of STS and are particularly susceptible to CF (Perregrini ref. 2019; Salimi et al. ref. 2020). In the United States, CF affects 40% of registered nurses (Perregrini ref. 2019) and 60% of emergency medicine physicians report experiencing STS (Shanafelt and Dyrbye ref. 2012).
Compassion Fatigue refers to a combination of emotional, physical, and psychological exhaustion resulting from prolonged exposure to compassion stress, caregiving, and empathy (Figley ref. 1995; Sorenson et al. ref. 2017; van Mol et al. ref. 2015). It comprises two components: Burnout (BO) and STS (Balch et al. ref. 2009; Stamm ref. 2002)‐ yet CF remains a distinct phenomenon. BO is characterised by emotional exhaustion, depersonalisation, negative attitudes, reduced personal satisfaction, and sadness, Whereas STS is associated with fear and work‐related trauma (Peters ref. 2018). In contrast Compassion Satisfaction (CS) refers to the fulfilment that caregivers derive from helping others and feeling valued in their professional role (Stamm ref. 2002). Compassion Satisfaction is associated with positive emotions gained from effective trauma care and serves as a protective factor against CF (Al Barmawi et al. ref. 2019; Ruiz‐Fernández et al. ref. 2020; Stamm ref. 2012).
Compassion Fatigue is an emerging concept in the Arab world, and it has not yet been thoroughly examined in Lebanon. In a systematic review of studies from the Arab region reported intermediate to high levels of CF among healthcare personnel (Elbarazi et al. ref. 2017). For instance, Jordanian critical care unit nurses, particularly those working in emergency departments, had low to average level of CS and CF (Al Barmawi et al. ref. 2019). Regarding physicians, although BO has been extensively studied, limited research has explored CF among this provider group (Baer et al. ref. 2017; Garcia et al. ref. 2014; Shanafelt and Dyrbye ref. 2012; Shenoi et al. ref. 2018).
A major consequence of CF, BO, and reduced CS is depersonalisation which leads to diminished empathy, heightened stress, depressive symptoms, physical exhaustion and ultimately impaired nurse–patient interaction. The outcomes contribute to increased medical errors, reduced life‐saving success, and lower quality of care (Balch et al. ref. 2009; Balinbin et al. ref. 2020; Cypress ref. 2011; Maslach and Jackson ref. 1981; Rudolph et al. ref. 1997; Shanafelt et al. ref. 2010; Trzeciak et al. ref. 2019; Winters ref. 2018).
Addressing CF among critical care providers is therefore vital to enhance their mental, emotional and psychological well‐being, promoting excellent patient care, and foster healthy and safe work environments. Doing so can provide valuable insight to cultivate healthier, more collaborative critical care teams and ultimately ensuring sustainable, high‐quality care for critically ill patients.
Methodology
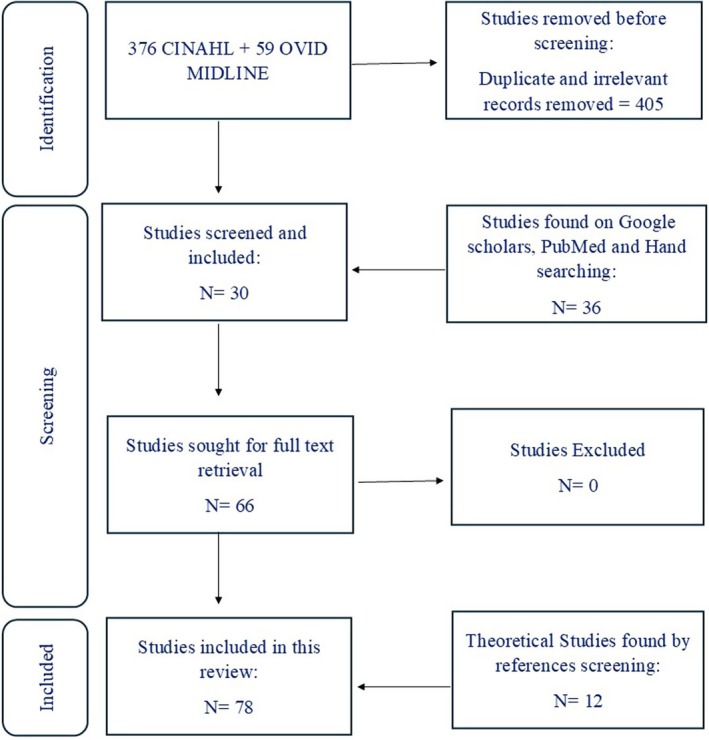
A scoping review enables the exploration of broad, emerging, or complex research topics (Tricco et al. ref. 2018). Therefore, it is considered an appropriate design to address the aim of this review. The purpose of this scoping review is to map the existing literature on CF and to highlight knowledge gaps that can guide future study, regardless of the study designs included. Structurally, this scoping review follows the five‐stage framework set out by Arksey and O’Malley (ref. 2005) which provides a systematic and rigorous approach to examining literature (Davis et al. ref. 2009) by mapping current evidence, summarising research findings, and identifying that warrant further exploration. The five stages are: (1) identifying a research question, (2) identifying relevant literature, (3) selecting literature, (4) charting data, and (5) reporting findings. The search strategy is depicted in the flow diagram below (Figure 1).
Stage 1: Identifying a Research Question
The adopted question for this scoping review is: what does literature detail about CF and CS among critical care nurses and physicians?
Although used interchangeably and indiscriminately, CF is an overarching phenomenon that encompasses both BO, an occupational stressor that arises from workplace strain, and STS which is an acquired trauma that evolves from feeling sufferer’s suffering. The aim of this study was to review both theoretical and empirical literature about what is known about CF and CS among critical care nurses and physicians and identify gaps that need further investigation to advance this area of research.
Stage 2. Identifying Relevant Publications
Two main journal databases were used to conduct this review, Ovid Midline and CINAHL. Additional searches were also conducted on PubMed and Google Scholar to ensure broader coverage of the literature. The search was conducted and included articles published from 2008 to 2023. The search was limited to English‐language publications.
The search strategy combined MeSH terms where applicable and keywords. Search terms were organised into three main concepts and combined using Boolean operators “OR” and “AND” as follows:
Concept 1: Compassion Fatigue, Burnout and Secondary Traumatic Stress
- MeSH terms: Compassion Fatigue/; Burnout, Professional/; Stress Disorders, Post‐Traumatic/
Concept 2: Healthcare Setting
- MeSH terms: Critical Care Nursing/; Critical Care/; Intensive Care Units/
Concept 3: Healthcare Professionals
- MeSH term: Physician/
The three concepts were then combined using the “AND” operator: (Concept 1) AND (Concept 2) AND (Concept 3). For instance: (compassion fatigue OR secondary trauma* OR burnout OR vicarious trauma* OR moral injur* OR PTSD) AND (critical care OR intensive care OR ICU) AND (physician* OR doctor* OR nurse* OR intensivist*).
Further papers were included by ancestry method through reference list screening of selected articles. Studies were included if they (a) examined CF or CS among critical care nurses and/or physicians, (b) were published in English, and (c) used an empirical (peer reviewed publication) or theoretical approaches (review or theoretical studies). Articles were excluded if irrelevant to the CF among nurses and physician concept, not in English, not in tertiary medical facility, a conference abstract.
Stage 3. Publication Selection
CINAHL yielded 376 results, whereas Midline Ovid produced 59 results. Initially duplicates were identified and removed using EndNote (version 20). The first author independently screened titles and abstracts for potential relevance based on inclusion/exclusion criteria Potentially relevant articles were retrieved for full texts screening. Screening was conducted independently by two reviewers; discrepancies were resolved through discussion and consensus to ensure rigour and reduce selection bias. A total of 30 empirical articles were found relevant on these 2 databases. Additionally, 36 other articles were found by Google Scholar alert, PubMed and hand searching of reference lists. Twelve theoretical articles were included as well in this paper found by hand searching and references screening.
Finally, a total of 66 empirical articles and 12 theoretical articles met the inclusion criteria and were included in this review. The study selection process was summarised in a PRISMA‐ScR flow diagram. All articles reviewed in this scoping review are presented in Tables [Link], [Link], [Link], [Link].
Stage 4. Charting Data
Articles were reviewed and key points data from the included studies were charted in the table. Extracted data included, Author, Year, Country, Sample, Measurement tool, Design, Main findings. The data extraction was conducted by the first researcher and reviewed by the research team. To validate the data extraction process, 8 random publications of the included studies, almost 10%, were cross‐checked by a second reviewer from the research team to ensure accuracy and consistency. References were cited by EndNote (version 20). Following the PRISMA‐ScR standards (Tricco et al. ref. 2018), no formal assessment of quality was conducted in this study, as the intention was not to exclude any papers based on quality appraisal.
Stage 5. Data Synthesis
Due to the variety of designs and heterogeneity of the studies found, a narrative synthesis of findings was adopted in this review. Studies found were tabulated and summarised then a content analysis of the data was performed based on the table data. Findings were categorised into themes and then compared with other studies from another settings. This review followed the PRISMA‐ScR evidence‐based guidelines to ensure methodological transparency and reproducibility and help authors improve quality and completeness of reporting in this scoping review.
Results
A total of 70 articles were analysed in this study varying between theoretical and empirical. In the review of the literature, 43 cross sectional studies, descriptive and correlational, were found in addition to 4 mixed methods studies. Participants in these studies were in majority critical care and emergency room nurses and physicians. Thirty‐five out of 47, almost three‐quarters 74.5%, reported scores of CF about their studies’ participants. Half of these studies, 17 studies, reported a low level of CF and BO among three participants. Eight out of these 17 studies were conducted in US (Abou Hashish and Ghanem Atalla ref. 2023; Aslan et al. ref. 2022; Calegari et al. ref. 2022; Faiza Hameed et al. ref. 2022; Hegney et al. ref. 2014; Jakimowicz et al. ref. 2018; Juniarta et al. ref. 2023; Kelly and Lefton ref. 2017; Lopez et al. ref. 2022; Meadors and Lamson ref. 2008; Mooney et al. ref. 2017; Storm and Chen ref. 2021; Weintraub et al. ref. 2016, ref. 2020; Wu et al. ref. 2016; Young et al. ref. 2011).
The other half, 16 studies, were conducted in developing countries with robust presence of Arabic and middle east countries, showed a moderate level of CF and low to moderate level of BO (Ageel and Shbeer ref. 2022; Al Barmawi et al. ref. 2019; Alharbi et al. ref. 2019, ref. 2020a, ref. 2020b; Cicek Korkmaz and Gokoglan ref. 2023; Delle Donne et al. ref. 2023; Ma et al. ref. 2022; Ndlovu et al. ref. 2022; Panagou et al. ref. 2023; Pehlivan Saribudak et al. ref. 2023; Racic et al. ref. 2019; Ruba Sam et al. ref. 2023; Salimi et al. ref. 2020; Subih et al. ref. 2023; Unlugedik and Akbas ref. 2023; Zeng et al. ref. 2023). Only 2 studies report high scores of BO and STS and thus CF, conducted among Critical care nurses in USA and South Korea (Jeong and Shin ref. 2023; Monroe et al. ref. 2020).
The majority of the studies in this review reported moderate to high CS (Ageel and Shbeer ref. 2022; Al Barmawi et al. ref. 2019; Alharbi et al. ref. 2019, ref. 2020a, ref. 2020b; Calegari et al. ref. 2022; Delle Donne et al. ref. 2023; Gribben et al. ref. 2019; Hegney et al. ref. 2014; Jakimowicz et al. ref. 2018; Juniarta et al. ref. 2023; Kelly and Lefton ref. 2017; Lopez et al. ref. 2022; Meadors et al. ref. 2009; Monroe et al. ref. 2020; Mooney et al. ref. 2017; Nasser Ali et al. ref. 2022; Ndlovu et al. ref. 2022; Panagou et al. ref. 2023; Racic et al. ref. 2019; Richardson and Greenle ref. 2020; Ruba Sam et al. ref. 2023; Salimi et al. ref. 2020; Storm and Chen ref. 2021; Weintraub et al. ref. 2016, ref. 2020; Wu et al. ref. 2016; Young et al. ref. 2011).
Only 4 studies reported a low level of CS and these were conducted in China, Pakistan, Egypt and Jordan (Abou Hashish and Ghanem Atalla ref. 2023; Faiza Hameed et al. ref. 2022; Ma et al. ref. 2022; Subih et al. ref. 2023; Zeng et al. ref. 2023).
This review revealed six themes, namely: CF Conceptualisation, CF operationalisation, CF Predictors and consequences, CF Management and Nurses’ perspective about CF.
Theme 1: CF Conceptualisation
There is a lack of consensus in theoretical literature regarding the definition and nomenclature of CF. Terms such as CF, STS, BO, and Vicarious Trauma are often used interchangeably or without clear distinction, leading to confusion. While this overlap reflects the interrelated nature of these conditions, it also obscures their unique characteristics.
Joinson (ref. 1992) was the first to discuss CF and defined it as a distinct kind of BO that is related to care‐giving professions, notably nursing. Figley (ref. 1995) unlike Joinson, distinguished between BO and CF and defined CF as a kind of post‐traumatic stress disorder (PTSD) related to the mental and emotional expenses of caring for others and practical substitute to “STS”.
According to Valent (ref. 2002), CF may exist on a continuum prior to or following BO. Thomas and Wilson (ref. 2004) identified three different traumatic outcomes: CF, STS, and vicarious traumatization and characterise CF as a distinct outcome. CF was defined as a gradual and cumulative process caused by extended, intensive interaction with patients that surpasses a nurse’s endurance limit (Coetzee and Klopper ref. 2010). Whereas Jenkins and Warren (ref. 2012) characterise it as the unavoidable result of dealing with a traumatised (the critically ill patient), and the other of whom is negatively impacted by the first’s traumatic event (the nurse in critical care), occurring unexpectedly as opposed to the gradual onset of BO due to ongoing exposure to stressors. On her turn, Stamm provided a model describing helping others as having two sides, a good one called “CS” and a negative one identified as CF, which consists of two components, BO and STS: CS, BO, and STS. Stamm (ref. 2002, ref. 2005, ref. 2010).
Theme 2: CF Operationalisation
The lack of consensus in defining CF has resulted in the adoption of multiple questionnaires for its assessment. The Professional Quality of Life (ProQOL‐V) questionnaire was used in most of the reviewed studies, with a lesser number using ProQOL‐IV or the Compassion Fatigue Short Scale (CFS) and Compassion Fatigue and Satisfaction Self‐Test (CFST). The various versions of ProQOL reflect the still‐evolving knowledge of CF, with ProQOL‐V including dimensions for CF (BO and STS) and CS. ProQOL‐IV, assesses three domains: CS, BO, and CF/STS. On the other hand, CFS includes BO and Vicarious trauma as component of CF, and CFST is the original long instrument from which ProQOL was developed.
Theme 3: CF Predictors and Consequences
Literature identifies various predictors of CF, generally categorised into demographic, personal, and organisational factors. However, the findings are often contradictory. For instance, while several studies suggest that being female is a predictor of CF, others report no significant correlation between gender and CF or compassion satisfaction (CS) scores. Similar inconsistencies are observed with variables such as age and years of experience. Similar inconsistencies are observed with variables such as age and years of experience. Some studies have established correlations between CF and patient outcomes, yet others have failed to replicate these results. Moreover, certain variables such as anxiety and depression have shown both positive and negative correlations with CF across different studies. A few investigations have also proposed novel predictors—such as nurse–physician collegiality—though these findings have yet to be confirmed through replication.
A strong correlation existed between CF and Post Traumatic Stress Disorder suggesting that those two concepts overlap (Meadors et al. ref. 2009). Similarly, a moderate to strong positive correlation exists between CF and stress (feeling of distress, work related stress, peritraumatic psychological stress, Moral distress), STS (Amin et al. ref. 2015; Kelly and Lefton ref. 2017; Nasser Ali et al. ref. 2022; Uzun et al. ref. 2022; Weintraub et al. ref. 2016, ref. 2020) (Maiden et al. ref. 2011) and witnessing the death of a child (Amin et al. ref. 2015; Meadors et al. ref. 2009).
Moreover, being single, BO scores, personal health issues, colleagues, not talking about stress, emotional depletion, in‐hospital teaching, participating in administrative activities (e.g., documentation) were found to be determinants of CF. In contrast, age (older generation nurses), being married, having a child, having long years of experience, not feeling depressed or emotionally depleted, being “on call”, staying over shift, being recognised, high job enjoyment and satisfaction, exercising, socialising, ethnicity (Hispanics and Indian) were all significant predictors of CS (Amin et al. ref. 2015; Aslan et al. ref. 2022; Delle Donne et al. ref. 2023; Kelly and Lefton ref. 2017; Meadors et al. ref. 2009; Nasser Ali et al. ref. 2022; Ruba Sam et al. ref. 2023; Weintraub et al. ref. 2016, ref. 2020).
Anxiety, tension, lack of compassion, disconnection, bad coping skills, and general negative attitudes are common symptoms of CF among healthcare providers (Milligan and Almomani ref. 2020). CF was found as a mediator between resilience and both anxiety and depression (Jo et al. ref. 2020). Strong positive correlations were found between nursing sensitive indicators (CAUTI, CLABSI and pressure injuries) and CF (Anglade ref. 2014; Maiden et al. ref. 2011). Two mixed method studies found that nurses who intended to leave or resign have higher CF scores in comparison to their colleagues who chose to stay (Christianson et al. ref. 2023; Maiden et al. ref. 2011).
Theme 4: CF Management
Coping strategies positively predict CS and negatively predict CF (Abou Hashish and Ghanem Atalla ref. 2023; Al Barmawi et al. ref. 2019; Calegari et al. ref. 2022; Weintraub et al. ref. 2020). As well, Level of resilience significantly predicted the rating of CS, BO, and STS. Regression model indicated that resilience as a predictor explained 66% of the CS, 26% of the BO and 15.4% of the STS variance (Alharbi et al. ref. 2019). On the other hand, two studies showed a significant relationship between Spiritual wellbeing and CF, with spiritual well‐being significantly predict CF among nurses and critical care nurses specifically (Ariapooran and Abdolmaleki ref. 2023; Unlugedik and Akbas ref. 2023). Moreover, Cumulative Stress Debriefing attendance demonstrates a correlation and reduction in symptoms related to CF (Arbios et al. ref. 2022). Furthermore, two RCTs were done to test the effect of emotional regulation training sessions and short‐ and long‐term Compassion Fatigue Resilience Program CFRP on nurses’ ProQOL score (Kharatzadeh et al. ref. 2020; Pehlivan Saribudak et al. ref. 2023). Both, program and sessions, positively affected CS, however, show no effect on CF.
Theme 5: Nurses’ Perspective on CF
Nurses recognised that CF could be handled with self‐care although they were unsure how to do so in their everyday working lives. Permission from themselves and others, namely nursing culture; organisation; managers, appeared to be the key for enabling nurses to continue providing the compassionate care to patients. Nurses described CF as “bruises in the soul” that fade away but leave scares that may affect patients later on if not treated (Andrews et al. ref. 2020; Gustafsson and Hemberg ref. 2022; Jakimowicz et al. ref. 2018). Furthermore, a mixed method study highlighted that critical care nurses don’t deliver compassionate care but competent care (Milligan and Almomani ref. 2020).
Discussion
This review provides a comprehensive review of the available literature on CF among healthcare providers working in critical care settings. Of the 47 empirical studies, almost 80% of the studies (n = 38), were conducted in the past 5 years, post COVID, reflecting the growing attention of to CF in critical care. This interest is paralleled by evidence of serious consequences, including increased rates of emotional exhaustion, reduced empathy, and compromised patient care outcomes (Alharbi et al. ref. 2020b; Peters ref. 2018). Unaddressed CF contribute to higher turnover intentions, absenteeism, and long‐term psychological distress threatening the healthcare systems stability and the patient care quality (Zhang et al. ref. 2022).
A substantial proportion of studies were conducted in the Arab countries and the MENA region, providing a more globally representative perspective than Western‐centric research. Furthermore, studies spanned countries with varying income levels, offering insights across diverse demographic and professional groups. However, all studies were in English language, which poses a risk of excluding relevant non‐English research.
CF manifest in critical care nurses as difficulty focusing, poor judgement, disturbing imagery, desperation, tiredness, anger, and irritability (Devilly et al. ref. 2009; Negash and Sahin ref. 2011), yet, no consensus exists on a single definition for CF. Some studies considered CF as distinct concept, others overlapping with STS and BO. This definitional inconsistency limits research mostly to cross‐sectional descriptive and correlational designs. Only a few experiments including randomised controlled trials, quasi‐experimental studies, and longitudinal studies have examined interventions (Kharatzadeh et al. ref. 2020; Arbios et al. ref. 2022; Pehlivan Saribudak et al. ref. 2023; Asadollah et al. ref. 2023; Egami and Farrar Highfield ref. 2023).
Methodological limitations were widespread, lack of interventional research methods, lack of standardised questionnaires to assess for CF, using a non‐validated questionnaire, self‐reported questionnaire, low response rate, cluster randomisation, potentially led to biased findings and exaggerated responses and low statistical power. Furthermore, despite extensive research on BO among physicians, CF among doctors remains under explored.
Regional and cultural factors shape CF experiences in the MENA region. Levantine countries (Jordan, Lebanon) and Egypt differ from Gulf countries in cultural norms, education systems, nurse–patient interactions, and resources, influencing CF. Local nurses often embody community‐centered care, emphasising family engagement (Elbarazi et al. ref. 2017). Conversely, foreign nurses in the face dual pressures of acculturation and maintaining cultural identity which complicates acculturation and contributes to emotional strain (El‐Jardali et al. ref. 2011).
Also, educational and systemic disparities exacerbate CF. Nursing programs in the Levant and Egypt while culturally contextualised, lack resources and international linkages present in Gulf programs (Aiken et al. ref. 2014). Gulf systems prioritise evidence‐based practice with significant funding (Alshammari et al. ref. 2019) creating a mismatch of demands and capabilities across regions.
Nurse–patient ratios emphasise CF burden. The American Association of Critical‐Care Nurses (AACN ref. 2024) recommends a 1:2 ratio in geriatric critical care wards to assure excellent treatment while reducing BO. However, Levantine ratios are higher. In Jordan, ICUs ratios fluctuate between 1:4 at university medical centers to 1:5–1:8 in Governmental institutions (Shuriquie et al. ref. 2008), while Lebanon face critical care nurses shortages (Alameddine et al. ref. 2020). These circumstances increase workloads, burnout, and CF prevalence.
Furthermore, support networks for nurses vary across regions. Levantine hospitals adequate resources, resulting in BO and high attrition (Alharbi et al. ref. 2020b) while Gulf nations are investing in nurse psychological wellness initiatives, social support, and professional growth (Alosaimi et al. ref. 2013). Cultural stigmas in the Levant and Egypt, where CF is seen as weakness further hinder obtaining the necessary care (Hamdan Mansour et al. ref. 2020).
Finally, professional status differences affect CF. In Egypt and the Levant, nurses may have limited recognition, hiring and retention opportunities as well. Expat nurses in Gulf, are often valued, yet this might reinforce hierarchies and local marginalisation among native nurses (Almutairi et al. ref. 2015).
Although no formal quality appraisal was performed, consistent with scoping review methodology, a critical reflection on the included studies revealed notable variability in methodological rigour. Overall, definitional inconsistencies, methodological limitations, and regional disparities hinder the development of evidence‐based interventions. Methodological challenges additionally restrict the generalisability of the findings. Limitations are summarised in the table below (Table 1). Future research should use participatory action research (PAR), engaging bedside staff to co‐develop interventions reflecting lived experiences. In addition, healthcare organisations should implement standardised staffing, anti‐stigma initiative, and equitable resources distribution. A multifaceted, frontline‐centered approach in policy, practice, and research is critical to protect healthcare workers’ mental health, building resilience, and ensuring high‐quality patient care worldwide.
TABLE 1: Analytical integration across reviewed studies.
| Theme | Key findings | Contradictions/variations | Research gaps/limitations |
|---|---|---|---|
| Definition of CF | |||
| Study designs | |||
| Measurement tools | |||
| Population and region | |||
| Impact on staff and patients | |||
| Organisational and cultural factors | |||
| Interventions | Some experimental studies show positive effects (Kharatzadeh et al. ref. 2020; Arbios et al. ref. 2022) |
Conclusion
This paper has identified several theoretical and empirical gaps in the study of CF, that warrant further investigation. Despite increased recognition of CF within the medical field, understanding its underlying effects, impacts on related factors, and effective interventions to mitigate its impact remains limited.
Theoretical gaps are evident in the absence of consensus regarding the conceptualisation of CF. The interchangeable and indiscriminate use of CF alongside concepts such as STS, Vicarious Traumatization, and BO reflects conceptual ambiguity and the interrelated nature of these phenomena.
Empirically, although extensive, a notable gap persists in interventional and preventive studies aimed at addressing CF. Moreover, the employment of multiple assessment tools with varying dimensions complicates the comparison of findings across studies. While numerous predictors of CF have been explored, results are frequently contradictory and lack replication. Methodological limitations have also been noted in the reviewed studies, particularly in the few that employ interventional designs. Finally, while numerous studies have focused on CF among nurses, studies among physicians are relatively limited.
In conclusion, addressing these theoretical and empirical gaps is crucial for advancing our understanding of this phenomenon and developing effective strategies for its prevention and management. Future research should aim to clarify conceptual boundaries, standardise measurement tools, and design robust interventional studies to enhance healthcare professionals’ well‐being and prevent declines in the quality of patient care.
Funding
The authors have nothing to report.
Clinical Resources
PRISMA for Scoping Reviews: http://www.prisma‐statement.org/Extensions/ScopingReviews; Professional Quality of Life version V ProQOL‐V manual: https://proqol.org/proqol‐manual.
Conflicts of Interest
The authors declare no conflicts of interest.
Supplementary Materials
References
- “Healthy Work Environment Assessment Tool (HWEAT) Team Sample Report.”. 2024
- The Relationship Between Coping Strategies, Compassion Satisfaction, and Compassion Fatigue During the COVID‐19 Pandemic.”. SAGE Open Nursing, 2023. [DOI | PubMed]
- Assessment of Professional Quality of Life Among Critical Care Nurses During the COVID‐19 Pandemic in Saudi Arabia.”. Journal of Healthcare Leadership, 2022. [DOI | PubMed]
- Nurse Staffing and Education and Hospital Mortality in Nine European Countries: A Retrospective Observational Study.”. Lancet, 2014. [PubMed]
- Coping Strategies as Moderating Factors to Compassion Fatigue Among Critical Care Nurses.”. Brain and Behavior, 2019. [DOI | PubMed]
- What Made Lebanese Emigrant Nurses Leave and What Would Bring Them Back? A Cross‐Sectional Survey.”. International Journal of Nursing Studies, 2020. [PubMed]
- Compassion Fatigue in Critical Care Nurses. An Integrative Review of the Literature [Systematic Review].”. Saudi Medical Journal, 2019. [PubMed]
- Personal Characteristics, Coping Strategies, and Resilience Impact on Compassion Fatigue in Critical Care Nurses: A Cross‐Sectional Study.”. Nursing & Health Sciences, 2020a. [DOI | PubMed]
- The Potential for COVID‐19 to Contribute to Compassion Fatigue in Critical Care Nurses.”. Journal of Clinical Nursing, 2020b. [DOI | PubMed]
- Understanding Cultural Competence in a Multicultural Nursing Workforce: Registered Nurses’ Experience in Saudi Arabia.”. Journal of Transcultural Nursing, 2015. [PubMed]
- A Phenomenological Study of Non‐Muslim Nurses Experiences of Caring for Muslim Patients in Saudi Arabia.”. International Journal of Arts & Sciences, 2013
- Barriers to Nurse–Patient Communication in Saudi Arabia: An Integrative Review.”. BMC Nursing, 2019. [DOI | PubMed]
- Perceived Stress and Professional Quality of Life in Neonatal Intensive Care Unit Nurses in Gujarat, India [Multicenter Study].”. Indian Journal of Pediatrics, 2015. [DOI | PubMed]
- Needing Permission: The Experience of Self‐Care and Self‐Compassion in Nursing: A Constructivist Grounded Theory Study.”. International Journal of Nursing Studies, 2020. [DOI | PubMed]
- Anglade, D. 2014. Patient Safety Culture, Compassion Fatigue, Compassion Satisfaction: Impact on Nurse‐Sensitive Patient Outcomes. University of Miami.
- Cumulative Stress Debriefings to Combat Compassion Fatigue in a Pediatric Intensive Care Unit.”. American Journal of Critical Care, 2022. [DOI | PubMed]
- Compassion Fatigue in Nurses: The Role of Spiritual Well‐Being, Emotion Regulation and Time Perspective.”. Iranian Journal of Nursing and Midwifery Research, 2023. [DOI | PubMed]
- Scoping Studies: Towards a Methodological Framework.”. International Journal of Social Research Methodology, 2005. [DOI]
- Relationship Between Compassion Fatigue in Nurses, and Work‐Related Stress and the Meaning of Life.”. Journal of Religion and Health, 2022. [DOI | PubMed]
- The Impact of Loving‐Kindness Meditation on Compassion Fatigue of Nurses Working in the Neonatal Intensive Care Unit: A Randomized Clinical Trial Study.”. Holistic Nursing Practice, 2023. [PubMed]
- Pediatric Resident Burnout and Attitudes Toward Patients.”. Pediatrics, 2017. [DOI | PubMed]
- Stress and Burnout Among Surgeons: Understanding and Managing the Syndrome and Avoiding the Adverse Consequences.”. Archives of Surgery, 2009. [DOI | PubMed]
- Occupational Determinants of Compassion Satisfaction and Compassion Fatigue Among Filipino Registered Nurses.”. Journal of Clinical Nursing, 2020. [DOI | PubMed]
- Association Between Coping Strategies and Professional Quality of Life in Nurses and Physicians During COVID‐19: A Cross‐Sectional Study.”. Journal of Nursing Management, 2022. [DOI | PubMed]
- Work‐Related Burnout, Compassion Fatigue, and Nurse Intention to Leave the Profession During COVID‐19.”. Nurse Leader, 2023. [DOI | PubMed]
- Do Nurses’ Personality Traits Affect the Level of Compassion Fatigue?”. International Nursing Review, 2023. [DOI | PubMed]
- Compassion Fatigue Within Nursing Practice: A Concept Analysis.”. Nursing & Health Sciences, 2010. [PubMed]
- The Importance of Word Choice in the Care of Critically Ill Patients and Their Families.”. Intensive Care Medicine, 2014. [PubMed]
- Exploring the Concept of Nurse‐Physician Communication Within the Context of Health Care Outcomes Using the Evolutionary Method of Concept Analysis.”. Dimensions of Critical Care Nursing, 2011. [DOI | PubMed]
- What Are Scoping Studies? A Review of the Nursing Literature.”. International Journal of Nursing Studies, 2009. [DOI | PubMed]
- Differences in the Long‐Term Impact of the COVID‐19 Pandemic on the Mental Health and Professional Quality of Life of Resident and Specialist Physicians.”. Medicina del Lavoro, 2023. [DOI | PubMed]
- Vicarious Trauma, Secondary Traumatic Stress or Simply Burnout? Effect of Trauma Therapy on Mental Health Professionals.”. Australian and New Zealand Journal of Psychiatry, 2009. [PubMed]
- The Effect of a Mindfulness Phone Application on NICU Nurses’ Professional Quality of Life.”. Advances in Neonatal Care: Official Journal of the National Association of Neonatal Nurses, 2023
- Prevalence of and Factors Associated With Burnout Among Health Care Professionals in Arab Countries: A Systematic Review.”. BMC Health Services Research, 2017. [DOI | PubMed]
- Nurses’ Work Environment and Intent to Leave in Lebanese Hospitals: Implications for Policy and Practice.”. International Journal of Nursing Studies, 2011. [PubMed]
- Burnout in Critical Care Nurses: A Literature Review.”. Dynamics (Pembroke), 2012
- Figley, C. 1995. “Compassion Fatigue as Secondary Traumatic Stress Disorder: An Overview.” In Compassion Fatigue: Coping With Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized, edited by C. R. Figley , 1–20. Routledge.
- Prevalence of Burnout in Pediatric Intensivists: An Observational Comparison With General Pediatricians.”. Pediatric Critical Care Medicine, 2014. [DOI | PubMed]
- A Cross‐Sectional Analysis of Compassion Fatigue, Burnout, and Compassion Satisfaction in Pediatric Critical Care Physicians in the United States.”. Pediatric Critical Care Medicine, 2019. [DOI | PubMed]
- Compassion Fatigue as Bruises in the Soul: A Qualitative Study on Nurses.”. Nursing Ethics, 2022. [DOI | PubMed]
- Health‐Care Workers’ Knowledge and Management Skills of Psychosocial and Mental Health Needs and Priorities of Individuals With COVID‐19.”. Mental Health and Social Inclusion, 2020
- Compassion Fatigue, Compassion Satisfaction, Burnout and Its Associated Factors Among Nurses Working in Critical Care Area of Tertiary Care Hospital, Karachi, Pakistan.”. Liaquat National Journal of Primary Care, 2022
- Compassion Satisfaction, Compassion Fatigue, Anxiety, Depression and Stress in Registered Nurses in Australia: Study 1 Results.”. Journal of Nursing Management, 2014. [DOI | PubMed]
- Compassion Satisfaction and Fatigue: A Cross‐Sectional Survey of Australian Intensive Care Nurses.”. Australian Critical Care, 2018. [DOI | PubMed]
- Concept Analysis: Compassion Fatigue and Effects Upon Critical Care Nurses.”. Critical Care Nursing Quarterly, 2012. [PubMed]
- The Relationship Between Secondary Traumatic Stress and Burnout in Critical Care Nurses: The Mediating Effect of Resilience.”. Intensive & Critical Care Nursing, 2023. [DOI | PubMed]
- Prevalence and Factors of Compassion Fatigue Among Nurse in China: A Protocol for Systematic Review and Meta‐Analysis.”. Medicine (Baltimore), 2021. [DOI | PubMed]
- Mediation Effects of Compassion Satisfaction and Compassion Fatigue in the Relationships Between Resilience and Anxiety or Depression Among Hospice Volunteers.”. Journal of Hospice and Palliative Nursing, 2020. [DOI | PubMed]
- Coping With Compassion Fatigue.”. Nursing, 1992
- Nurses’ Self‐Compassion and Professional Quality of Life During COVID‐19 Pandemic: A Cross‐Sectional Study.”. Jurnal Keperawatan Padjadjaran, 2023. [DOI]
- Effect of Meaningful Recognition on Critical Care Nurses’ Compassion Fatigue.”. American Journal of Critical Care, 2017. [DOI | PubMed]
- Emotional Regulation Training for Intensive and Critical Care Nurses.”. Nursing & Health Sciences, 2020. [DOI | PubMed]
- Cross‐Sectional Analysis of Burnout, Secondary Traumatic Stress, and Compassion Satisfaction Among Emergency Nurses in Southern California Working Through the COVID‐19 Pandemic.”. Journal of Emergency Nursing, 2022. [DOI | PubMed]
- Compassion Fatigue, Burnout, Compassion Satisfaction and Depression Among Emergency Department Physicians and Nurses: A Cross‐Sectional Study.”. BMJ Open, 2022. [DOI]
- Moral Distress, Compassion Fatigue, and Perceptions About Medication Errors in Certified Critical Care Nurses.”. Dimensions of Critical Care Nursing, 2011. [DOI | PubMed]
- Maslach, C. , and S. E. Jackson . 1981. Maslach Burnout Inventory (MBI): Educators Survey (ES) manual. Consulting Psychologists Press.
- Compassion Fatigue and Secondary Traumatization: Provider Self Care on Intensive Care Units for Children.”. Journal of Pediatric Health Care, 2008. [DOI | PubMed]
- Secondary Traumatization in Pediatric Healthcare Providers: Compassion Fatigue, Burnout, and Secondary Traumatic Stress.”. Omega (Westport), 2009. [DOI | PubMed]
- Death Anxiety and Compassion Fatigue in Critical Care Nurses.”. British Journal of Nursing, 2020. [PubMed]
- The Relationship Between Critical Care Work Environment and Professional Quality of Life.”. American Journal of Critical Care, 2020. [PubMed]
- A Preliminary Analysis of Compassion Satisfaction and Compassion Fatigue With Considerations for Nursing Unit Specialization and Demographic Factors.”. Journal of Trauma Nursing, 2017. [DOI | PubMed]
- Relationship Between Compassion Satisfaction, Compassion Fatigue and Peritraumatic Psychological Distress Among Nurses Caring for COVID‐19 Patients.”. Minia Scientific Nursing Journal, 2022
- Professional Quality of Life of Nurses in Critical Care Units: Influence of Demographic Characteristics.”. Southern African Journal of Critical Care, 2022. [DOI]
- Compassion Fatigue in Marriage and Family Therapy: Implications for Therapists and Clients.”. Journal of Marital and Family Therapy, 2011. [PubMed]
- Compassion Fatigue and Compassion Satisfaction in Pediatric Intensive Care Professionals.”. Materia Socio‐Medica, 2023. [DOI | PubMed]
- Effect of a Compassion Fatigue Resiliency Program on Nurse Managers’ Professional Quality of Life, Stress, and Resilience: A Mixed‐Methods Study.”. Journal of Nursing Care Quality, 2023. [DOI | PubMed]
- Combating Compassion Fatigue.”. Nursing, 2019. [DOI]
- Compassion Fatigue in Nursing: A Concept Analysis.”. Nursing Forum, 2018. [DOI | PubMed]
- Compassion Fatigue and Compassion Satisfaction Among Family Physicians in the Republic of Srpska, Bosnia and Herzegovina.”. International Journal of Occupational Safety and Ergonomics, 2019. [DOI | PubMed]
- Impact of Exposure to Patient Death or Near Death on Compassion Fatigue in Pediatric Intensive Care Nurses.”. American Journal of Critical Care, 2020. [DOI | PubMed]
- Prevalence of Compassion Fatigue Among Nursing Staffs Working in High Acuity Clinical Settings, Within Dubai Health Authority Hospitals, UAE.”. Eatsern Journal of Healthcare, 2023. [DOI]
- Rudolph, J. , B. H. Stamm , and H. Stamm . 1997. “Compassion Fatigue: A Concern for Mental Health Policy, Providers, and Administration.” In Poster at the 13th Annual Meeting of the International Society for Traumatic Stress Studies, Montreal, Quebec, Canada.
- Compassion Fatigue, Burnout, Compassion Satisfaction and Perceived Stress in Healthcare Professionals During the COVID‐19 Health Crisis in Spain.”. Journal of Clinical Nursing, 2020. [DOI | PubMed]
- Compassion Satisfaction, Burnout, and Secondary Traumatic Stress Among Critical Care Nurses in Iran [Research Support, Non‐U.S. Gov’t].”. Journal of Transcultural Nursing, 2020. [DOI | PubMed]
- Oncologist Burnout: Causes, Consequences, and Responses.”. Journal of Clinical Oncology, 2012. [DOI | PubMed]
- Burnout and Medical Errors Among American Surgeons.”. Annals of Surgery, 2010. [DOI | PubMed]
- Burnout and Psychological Distress Among Pediatric Critical Care Physicians in the United States.”. Critical Care Medicine, 2018. [DOI | PubMed]
- Nursing Work in Jordan: An Example of Nursing Work in the Middle East.”. Journal of Clinical Nursing, 2008. [PubMed]
- An Evolutionary Concept Analysis of Compassion Fatigue.”. Journal of Nursing Scholarship, 2017. [DOI | PubMed]
- Stamm, B. 2010. The Concise Manual for the Professional Quality of Life Scale. Eastwoods, LLC.
- Stamm, B. H. 2002. “Measuring Compassion Satisfaction as Well as Fatigue: Developmental History of the Compassion Satisfaction and Fatigue Test.” In Treating Compassion Fatigue, edited by C. R. Figley , 107–119. Brunner‐Routledge.
- Stamm, B. H. 2005. “The Professional Quality of Life Scale.” In Compassion Satisfaction, Burnout & Compassion Fatigue/Secondary Trauma Scales, edited by Institute of Rural Health . Sidran Press.
- Stamm, B. H. 2012. “Helping the Helpers: Compassion Satisfaction and Compassion Fatigue in Self‐Care, Management, and Policy.” In Resources for Community Suicide Prevention. [CD], edited by I. A. D. Kirkwood and B. H. Stamm . Idaho State University.
- The Relationships Among Alarm Fatigue, Compassion Fatigue, Burnout and Compassion Satisfaction in Critical Care and Step‐Down Nurses.”. Journal of Clinical Nursing, 2021. [DOI | PubMed]
- Evaluation of Compassion Fatigue and Compassion Satisfaction Among Emergency Nurses in Jordan: A Cross‐Sectional Study.”. International Emergency Nursing, 2023. [DOI | PubMed]
- Addressing the Indirect Trauma of Social Work Students in Intimate Partner Violence (IPV) Field Placements: A Framework for Supervision.”. Clinical Social Work Journal, 2019. [DOI]
- Issues and Controversies in the Understanding and Diagnosis of Compassion Fatigue, Vicarious Traumatization, and Secondary Traumatic Stress Disorder.”. International Journal of Emergency Mental Health, 2004. [PubMed]
- Critical Care Nurses’ Perceptions of Preparedness and Ability to Care for the Dying and Their Professional Quality of Life.”. Dimensions of Critical Care Nursing, 2013. [DOI | PubMed]
- PRISMA Extension for Scoping Reviews (PRISMA‐ScR): Checklist and Explanation.”. Annals of Internal Medicine, 2018. [DOI | PubMed]
- Trzeciak, S. , A. Mazzarelli , and C. Booker . 2019. Compassionomics: The Revolutionary Scientific Evidence That Caring Makes a Difference. Studer Group.
- The Effect of Spiritual Well‐Being on Compassion Fatigue Among Intensive Care Nurses: A Descriptive Study.”. Intensive & Critical Care Nursing, 2023. [DOI | PubMed]
- The Comparison of Healthcare Personnel’s Life Qualities in Intensive Care Units Following and Unfollowing Covid‐19 Patient.”. Haydarpasa Numune Training and Research Hospital Medical Journal, 2022. [DOI]
- Diagnosis and Treatment of Helper Stresses, Traumas, and Illnesses.”. Treating Compassion Fatigue, 2002
- The Prevalence of Compassion Fatigue and Burnout Among Healthcare Professionals in Intensive Care Units: A Systematic Review.”. PLoS One, 2015. [DOI | PubMed]
- Compassion Fatigue, Burnout and Compassion Satisfaction in Neonatologists in the US.”. Journal of Perinatology, 2016. [DOI | PubMed]
- A Cross‐Sectional Analysis of Compassion Fatigue, Burnout, and Compassion Satisfaction in Pediatric Hematology‐Oncology Physicians in the United States.”. Journal of Pediatric Hematology/Oncology, 2020. [PubMed]
- Secondary Traumatic Stress and Compassion Fatigue: A Guide for Childbirth Professionals When the Infant Dies.”. International Journal of Childbirth Education, 2018
- Compassion Fatigue, Burnout, and Compassion Satisfaction Among Oncology Nurses in the United States and Canada.”. Oncology Nursing Forum, 2016. [DOI | PubMed]
- Compassion Satisfaction, Burnout, and Secondary Traumatic Stress in Heart and Vascular Nurses.”. Critical Care Nursing Quarterly, 2011. [DOI | PubMed]
- The Moderating Effect of Occupational Burnout on the Link Between Career Competencies and Career Sustainability amid the COVID‐19 Pandemic: A Mixed‐Method Study.”. Frontiers in Psychology, 2022. [PubMed]
- The Levels and Influencing Factors of Compassion Fatigue Among New Nurses During the COVID‐19 Pandemic.”. Journal of Nursing Management, 2023. [DOI]