
Laparoscopy in management of appendicitis in high-, middle-, and low-income countries: a multicenter, prospective, cohort study
Abstract
Background:
Appendicitis is the most common abdominal surgical emergency worldwide. Differences between high- and low-income settings in the availability of laparoscopic appendectomy, alternative management choices, and outcomes are poorly described. The aim was to identify variation in surgical management and outcomes of appendicitis within low-, middle-, and high-Human Development Index (HDI) countries worldwide.
Methods:
This is a multicenter, international prospective cohort study. Consecutive sampling of patients undergoing emergency appendectomy over 6 months was conducted. Follow-up lasted 30 days.
Results:
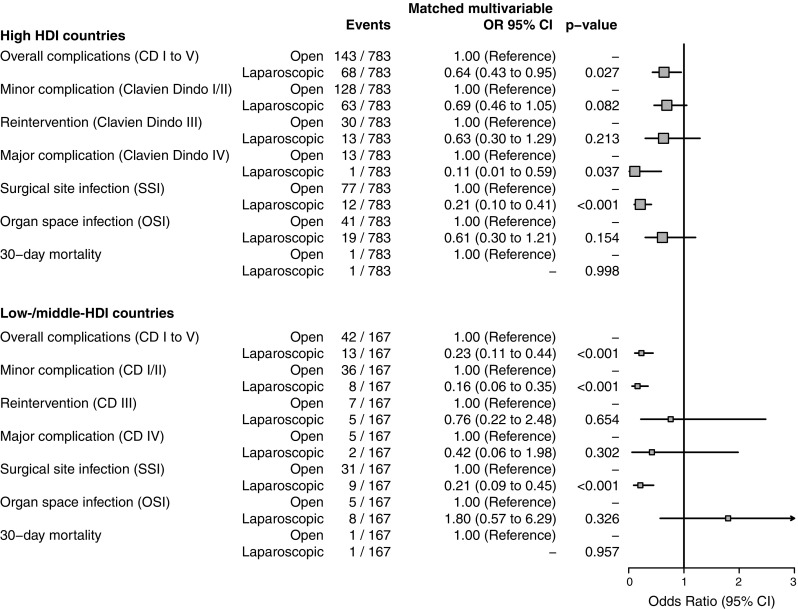
4546 patients from 52 countries underwent appendectomy (2499 high-, 1540 middle-, and 507 low-HDI groups). Surgical site infection (SSI) rates were higher in low-HDI (OR 2.57, 95% CI 1.33–4.99, p = 0.005) but not middle-HDI countries (OR 1.38, 95% CI 0.76–2.52, p = 0.291), compared with high-HDI countries after adjustment. A laparoscopic approach was common in high-HDI countries (1693/2499, 67.7%), but infrequent in low-HDI (41/507, 8.1%) and middle-HDI (132/1540, 8.6%) groups. After accounting for case-mix, laparoscopy was still associated with fewer overall complications (OR 0.55, 95% CI 0.42–0.71, p < 0.001) and SSIs (OR 0.22, 95% CI 0.14–0.33, p < 0.001). In propensity-score matched groups within low-/middle-HDI countries, laparoscopy was still associated with fewer overall complications (OR 0.23 95% CI 0.11–0.44) and SSI (OR 0.21 95% CI 0.09–0.45).
Conclusion:
A laparoscopic approach is associated with better outcomes and availability appears to differ by country HDI. Despite the profound clinical, operational, and financial barriers to its widespread introduction, laparoscopy could significantly improve outcomes for patients in low-resource environments.
Trial registration: NCT02179112.
Electronic supplementary material:
The online version of this article (10.1007/s00464-018-6064-9) contains supplementary material, which is available to authorized users.
Article type: Research Article
Keywords: Appendicitis, Appendectomy, Global surgery, Laparoscopic, Operative standards, Postoperative care, Postoperative complications, Surgical site infection
Affiliations: NIHR Unit on Global Surgery (Universities of Birmingham, Edinburgh and Warwick), University of Edinburgh, Royal Infirmary of Edinburgh, Edinburgh, EH16 4SA UK
License: © The Author(s) 2018 CC BY 4.0 Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Article links: DOI: 10.1007/s00464-018-6064-9 | PubMed: 29623470 | PMC: PMC6061087
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (894 KB)
The global burden of diseases requiring emergency surgery is poorly described and represents a significant health problem [ref. 1]. Most of the world’s population do not have access to safe, affordable and timely surgery, with access inequitably distributed in favor of high Human Development Index (HDI) countries [ref. 2]. It is estimated that in 2010, approximately 17 million deaths resulted from conditions requiring surgical care, far greater than the combined burden of HIV/AIDs, malaria, and tuberculosis [ref. 3]. There is an urgent need to increase access to surgical treatment across the world.
Appendicitis is one of the commonest diseases requiring emergency abdominal surgery, yet little data exist to allow comparison of management and outcomes at a patient level globally [ref. 4]. Recently published trends predict a significant increase in the prevalence of appendicitis in newly industrialized countries [ref. 5]. Data from the Global Burden of Disease Study (2016) show a higher prevalence of appendicitis in lower socio-economic countries, together with a greater proportion of years-of-life-lost as a result of the disease [ref. 6]. Appendicitis is usually treated with surgery, although management purely with antibiotics has been investigated [ref. 7]. Appendectomy can be performed by a traditional open procedure, but a laparoscopic approach has become common in many countries [ref. 8]. Significant variation in practice still exists in high-income settings [ref. 9].
The role of laparoscopy in low-resource healthcare settings has been debated [ref. 10]. Those arguing against its use suggest that the required initial financial and training investment, together with the on-going costs of equipment upkeep and consumables, make it unviable when compared to relatively straightforward open surgery. This argument has resonance: when a healthcare system is struggling to deliver basic surgical procedures, the introduction of a more complex intervention must be considered carefully. On the other hand, there are broad advantages to having laparoscopy available, particularly the ability to perform diagnostic laparoscopy in the absence of expensive CT imaging. Lower postoperative complication rates [ref. 9] and consequent healthcare costs are commonly reported to be associated with laparoscopic appendectomy. Whether laparoscopy has the same advantage in low-resource settings is unknown.
The GlobalSurg Collaborative has recently demonstrated the feasibility of conducting international data collection in low-resource settings [ref. 4, ref. 11]. Using these approaches, this study aimed to investigate the surgical management of appendectomy worldwide, including the use of laparoscopy, and to examine outcomes following surgery.
Methods
Study setting
A collaborative, international, multicenter, prospective, observational cohort study was conducted according to a pre-specified, published protocol (ClinicalTrials.gov identifier: NCT02179112) [ref. 12]. The collaborative network methodology has been described elsewhere [ref. 13]. Briefly, the study was conducted by teams of local investigators coordinated by a national lead investigator. Investigators were recruited via the GlobalSurg network and through dissemination on social media and other personal contacts. Consecutive sampling of patients undergoing emergency abdominal surgery was undertaken during 2-week periods within a 6-month study window. Investigators in a hospital could choose one or multiple 2-week periods. There was an absolute requirement for all cases in the chosen period(s) to be included, but no minimum number set to avoid bias against smaller centers. A UK National Health Service Research Ethics review considered this study exempt from formal research registration (South East Scotland Research Ethics Service, reference NR/1404AB12); individual centers obtained their own audit, ethical or institutional approval. This study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [ref. 14]. Pre-specified sub-group analyses included the examination of patients undergoing appendectomy as compared with other abdominal surgical procedures. At each participating center, data collection was performed by teams following the same standardized protocol [ref. 12].
Patients and procedures
The study inclusion period was 01 July 2014 to 31 December 2014. Consecutive patients undergoing emergency appendectomy were eligible for inclusion. No limits were placed on age or operative approach. Emergency surgery was defined as any unplanned, non-elective operation, including re-operation after a previous procedure. Elective (planned) or semi-elective procedures (where a patient initially admitted as an emergency was then discharged from hospital and re-admitted at later time for surgery) were excluded.
Data
Data were selected to be objective, standardized, easily transcribed and internationally relevant, to maximize record completion and accuracy. Patients were followed for 30 days after surgery or for the length of their inpatient stay where follow-up was not feasible. Records were uploaded by local investigators to a secure online website, provided using the Research Electronic Data Capture (REDCap) system [ref. 15]. The lead investigator at each site was responsible for “signing off” patient records. Data were checked with primary data sources if necessary. The local lead was responsible for ensuring consecutive sampling (i.e., no excluded cases) for each site. The submitted data were then checked centrally and where missing data were identified, the local lead investigator was contacted and asked to investigate. Once vetted, the record was accepted into the dataset for analysis.
Patient variables included age, gender, American Society of Anesthesiologists (ASA) physical status classification system, diabetes history, smoking and diagnostic category. Service variables included use of the WHO surgical safety checklist, the experience of surgeon/anesthetist, and compliance with selected evidence-based standards. Prophylactic antibiotic use was defined as antibiotics administered either at induction, or during surgery but before opening of a contaminated space.
Outcome variables
The primary outcome measure was overall complication rate, defined using the Clavien–Dindo grade occurring within 30 days of the index operation. The criteria required for each outcome were defined a priori in the protocol [ref. 12]. Major complication (Clavien–Dindo IV) was defined as a life-threatening illness requiring critical care management. In low-resource settings, investigators could report “complication requiring critical care, but facilities unavailable.”
The US Centre for Disease Control and Prevention (CDC) definitions for SSI and organ space infection (OSI) were used [ref. 16]. SSI: one of (1) purulent drainage from the incision; (2) at least two of following: pain or tenderness, localized swelling, redness, heat, fever, and the incision is opened deliberately to manage infection; (3) wound organisms AND pus cells from aspirate/swab. OSI: intra-abdominal/pelvic detected clinically/symptomatically, radiologically, or intra-operatively.
Power considerations
The sample size was limited by practical factors and estimation of power by uncertainty over critical quantities such as clustering and variation by diagnosis. An indicative calculation for overall complication rate showed that considerable precision was likely with 520 patients per HDI comparison group (a 6% point difference in overall complication rate; baseline rate 16% with alpha = 0.05, beta = 0.2, and accounting for missing data/loss to follow-up).
Statistical analysis
Variation across different international health settings was assessed by stratifying participating centers by country into three tertiles according to HDI rank. This is a composite statistic of life expectancy, education, and income indices published by the United Nations (http://hdr.undp.org/en/statistics). Differences between HDI tertiles were initially tested with the Pearson chi-squared and Kruskal–Wallis tests for categorical and continuous variables respectively.
Multivariable binary logistic regression models were constructed to adjust for case-mix and measures of hospital facilities and service, to explore the nature of differences in outcome. Subsequently, three-level hierarchical multivariable logistic regression models were made to account for hospital- and country-level variation (“hospital” and “country” as random effects with constrained gradients). Variable selection was incremental and accounted for both clinical and statistical significances. Model fit was guided log-likelihood methods including the Akaike Information Criterion (AIC). Discrimination was defined by the area-under-the receiver-operator-curve (c-statistic). Calibration across the range of observed probabilities was checked. All two-way interactions were investigated. Bayesian simulation methods are described in the supplementary digital content.
In a further propensity-score matched study, patients from low- and middle-HDI countries were analyzed separately to those from high-HDI countries. Patients who had undergone laparoscopic surgery were matched with those who underwent open surgery using a “nearest neighbor” approach, based on probabilities of group membership determined with multivariable logistic regression. The matching algorithm used age, gender, smoking status, ASA score, and perforation status. Pre- and post-matching balance was checked for all relevant variables.
All analyses were undertaken using the R Foundation Statistical Program (R 3.1.1, R Foundation for Statistical Computing) and Stan (Stan: A C++ Library for Probability and Sampling, Version 2.10.0. URL http://mc-stan.org/).
Results
4546 patients underwent laparoscopic or open appendectomy for acute appendicitis over the data collection period.
Demographics
Patients were from 52 countries with high-HDI (n = 2499), middle-HDI (n = 1540), and low-HDI (n = 507) groups (Table 1). Patients in low-HDI countries were younger (Pearson’s χ2 test, p < 0.001) and more likely to be male [low-HDI (295/507, 58%), middle-HDI (783/1540, 51%), high-HDI (1344/2499, 54%), p = 0.012]. There were numerically more patients considered to have severe systemic disease (ASA 3 or greater) in the low-HDI group (p = 0.021).
Table 1: Patient and operative characteristics
| Human development index (HDI) | p Value | |||
|---|---|---|---|---|
| High (n = 2499) | Middle (n = 1540) | Low (n = 507) | ||
| Age in completed years | ||||
| Mean (SD) | 31.2 (18.2) | 26.9 (14.6) | 24.1 (12.1) | < 0.001 |
| Gender | ||||
| Male | 1344 (53.8) | 783 (50.8) | 295 (58.2) | 0.012 |
| Female | 1155 (46.2) | 757 (49.2) | 212 (41.8) | |
| Diabetes history | ||||
| No | 2435 (97.4) | 1493 (96.9) | 489 (96.4) | 0.390 |
| Yes | 64 (2.6) | 47 (3.1) | 18 (3.6) | |
| Smoking currently | ||||
| No | 1977 (79.1) | 1295 (84.1) | 446 (88.0) | < 0.001 |
| Yes | 521 (20.8) | 244 (15.8) | 60 (11.8) | |
| Missing | 1 (0.0) | 1 (0.1) | 1 (0.2) | |
| ASA score | ||||
| 1 | 1724 (69.0) | 1098 (71.3) | 344 (67.9) | 0.021 |
| 2 | 613 (24.5) | 332 (21.6) | 102 (20.1) | |
| ≥ 3 | 104 (4.2) | 74 (4.8) | 33 (6.5) | |
| Missing | 58 (2.3) | 36 (2.3) | 28 (5.5) | |
| Procedure start time | ||||
| 0800–1800 (daytime) | 1345 (53.8) | 615 (39.9) | 188 (37.1) | < 0.001 |
| 1800–2200 (evening) | 616 (24.6) | 412 (26.8) | 137 (27.0) | |
| 2200–0800 (night-time) | 538 (21.5) | 513 (33.3) | 182 (35.9) | |
| Surgical safety checklist used | ||||
| No, not available in this hospital | 182 (7.3) | 570 (37.0) | 187 (36.9) | < 0.001 |
| No, but available in this hospital | 35 (1.4) | 103 (6.7) | 161 (31.8) | |
| Yes | 2282 (91.3) | 867 (56.3) | 159 (31.4) | |
| Prophylactic antibiotics | ||||
| No | 223 (8.9) | 205 (13.3) | 62 (12.2) | < 0.001 |
| Yes | 2276 (91.1) | 1335 (86.7) | 445 (87.8) | < 0.001 |
| Senior surgeon > 5 years training | ||||
| No | 108 (4.3) | 769 (49.9) | 210 (41.4) | < 0.001 |
| Yes | 2391 (95.7) | 770 (50.0) | 297 (58.6) | |
| Missing | 0 (0.0) | 1 (0.1) | 0 (0.0) | |
| Senior anesthetist > 5 years training | ||||
| No | 115 (4.6) | 789 (51.2) | 265 (52.3) | < 0.001 |
| Yes | 2384 (95.4) | 751 (48.8) | 242 (47.7) | |
| Laparoscopic approach | ||||
| No | 806 (32.3) | 1408 (91.4) | 466 (91.9) | < 0.001 |
| Yes | 1693 (67.7) | 132 (8.6) | 41 (8.1) | |
| Perforated viscus | ||||
| No | 2150 (86.0) | 1380 (89.6) | 394 (77.7) | < 0.001 |
| Yes | 348 (13.9) | 159 (10.3) | 109 (21.5) | |
| Missing | 1 (0.0) | 1 (0.1) | 4 (0.8) | |
Data are n (%) unless otherwise stated
SD standard deviation
Surgical characteristics
There were clear differences in management between HDI groups (Table 1). A laparoscopic approach was used in 67.7% of patients in the high-HDI group and in < 10% in the low- and middle-HDI groups (Pearson’s χ2 test, p < 0.001). There was more operating through the night in low- and middle-HDI groups (Pearson’s χ2 test, p < 0.001), while more patients were operated upon > 24 h after admission in high-HDI countries. Seniority of both the surgeon and anesthetist was higher in high-HDI countries. Prophylactic antibiotics and use of the WHO surgical safety checklist was less common in low- and middle-HDI groups.
Outcomes
In univariable analyses, associations were seen between HDI and overall and minor complications, as well as surgical site and OSIs (Table 2). There was no strong association between HDI and reintervention, major complication, or death.
Table 2: Outcomes
| Human development index (HDI) | ||||
|---|---|---|---|---|
| High (n = 2499) | Middle (n = 1540) | Low (n = 507) | p Value | |
| Overall complications (Clavien–Dindo I, II, III, IV, or V) | ||||
| No | 2182 (87.3) | 1303 (84.7) | 414 (81.7) | 0.001 |
| Yes | 317 (12.7) | 235 (15.3) | 93 (18.3) | |
| Missing | 0 (0.0) | 2 (0.1) | 0 (0.0) | |
| Minor complication (Clavien–Dindo I/II) | ||||
| No | 2219 (88.9) | 1314 (86.1) | 423 (84.1) | 0.002 |
| Yes | 278 (11.1) | 212 (13.9) | 80 (15.9) | |
| Missing | 2 (0.1) | 14 (0.9) | 4 (0.8) | |
| Reintervention (Clavien–Dindo III) | ||||
| No | 2431 (97.3) | 1501 (97.6) | 494 (97.4) | 0.828 |
| Yes | 68 (2.7) | 37 (2.4) | 13 (2.6) | |
| Missing | 0 (0.0) | 2 (0.1) | 0 (0.0) | |
| Major complication (Clavien–Dindo IV) | ||||
| No | 2474 (99.0) | 1520 (98.8) | 498 (98.2) | 0.325 |
| Yes | 25 (1.0) | 18 (1.2) | 9 (1.8) | |
| Missing | 0 (0.0) | 2 (0.1) | 0 (0.0) | |
| Surgical site infection (SSI) | ||||
| No | 2389 (95.6) | 1340 (88.0) | 432 (85.2) | < 0.001 |
| Yes | 109 (4.4) | 183 (12.0) | 75 (14.8) | |
| Missing | 1 (0.0) | 1 (0.1) | 0 (0.0) | |
| Organ/space infection (OSI) | ||||
| No | 2397 (96.0) | 1486 (96.4) | 494 (97.4) | 0.023 |
| Yes | 101 (4.0) | 39 (2.7) | 13 (2.6) | |
| Missing | 1 (0.0) | 15 (1.0) | 0 (0.0) | |
| Length of stay after surgery (days) | ||||
| Mean (SD) | 3 (3.4) | 2.9 (3.2) | 4.1 (4.7) | < 0.001 |
| 30-day mortality | ||||
| Alive | 2496 (99.9) | 1532 (99.5) | 504 (99.4) | 0.061 |
| Dead | 3 (0.1) | 2 (0.1) | 3 (0.6) | |
| Missing | 0 (0.0) | 6 (0.4) | 0 (0.0) | |
Data are n (%) unless otherwise stated
SD standard deviation
The overall complication rate was higher in low-HDI (odds ratio (OR) 1.55, 95% confidence interval (CI) 1.19–1.99, p = 0.001) and middle-HDI (OR 1.24, 95% CI 1.03–1.49, p = 0.020) countries compared with the high-HDI group (Tables 2, 3). When the analysis was adjusted in a multilevel model accounting for patient, disease, and hospital structural factors, there was no independent association between overall complications and HDI group.
Table 3: Overall complications
| Overall complications | ||||
|---|---|---|---|---|
| No | Yes | Univariable logistic regression OR (95% CI, p value) | Multilevel logistic regression OR (95% CI, p value) | |
| HDI tertile | ||||
| High | 2182 (56.0) | 317 (49.1) | ||
| Middle | 1303 (33.4) | 235 (36.4) | 1.24 (1.03–1.49, p = 0.020) | 0.91 (0.56–1.48, p = 0.701) |
| Low | 414 (10.6) | 93 (14.4) | 1.55 (1.19–1.99, p = 0.001) | 1.44 (0.82–2.54, p = 0.209) |
| Age in completed years | ||||
| Mean (SD) | 28.2 (16) | 33.3 (19.5) | 1.02 (1.01–1.02, p < 0.001) | 1.01 (1.01–1.02, p < 0.001) |
| Gender | ||||
| Male | 2069 (53.1) | 351 (54.4) | ||
| Female | 1830 (46.9) | 294 (45.6) | 0.95 (0.80–1.12, p = 0.523) | 0.98 (0.82–1.19, p = 0.873) |
| Diabetes history | ||||
| No | 3805 (97.6) | 610 (94.6) | ||
| Yes | 94 (2.4) | 35 (5.4) | 2.32 (1.54–3.42, p < 0.001) | 1.27 (0.80–2.01, p = 0.315) |
| Smoking currently | ||||
| No | 3208 (82.3) | 508 (78.8) | ||
| Yes | 688 (17.7) | 137 (21.2) | 1.26 (1.02–1.54, p = 0.029) | 0.96 (0.76–1.23, p = 0.770) |
| ASA score | ||||
| 1 | 2790 (73.6) | 375 (59.4) | ||
| 2 | 850 (22.4) | 196 (31.1) | 1.72 (1.42–2.07, p < 0.001) | 1.42 (1.13–1.78, p = 0.003) |
| ≥ 3 | 151 (4.0) | 60 (9.5) | 2.96 (2.14–4.04, p < 0.001) | 1.64 (1.10–2.46, p = 0.016) |
| Procedure start time | ||||
| 0800–1800 (daytime) | 1854 (47.6) | 292 (45.3) | ||
| 1800–2200 (evening) | 985 (25.3) | 180 (27.9) | 1.16 (0.95–1.42, p = 0.148) | |
| 2200–0800 (night-time) | 1060 (27.2) | 173 (26.8) | 1.04 (0.85–1.27, p = 0.730) | |
| Surgical safety checklist used | ||||
| No, not available in this hospital | 781 (20.0) | 157 (24.3) | ||
| No, but available in this hospital | 250 (6.4) | 48 (7.4) | 0.96 (0.67–1.35, p = 0.799) | 0.79 (0.48–1.30, p = 0.352) |
| Yes | 2868 (73.6) | 440 (68.2) | 0.76 (0.63–0.93, p = 0.008) | 0.84 (0.59–1.19, p = 0.327) |
| Prophylactic antibiotics | ||||
| No | 422 (10.8) | 67 (10.4) | ||
| Yes | 3477 (89.2) | 578 (89.6) | 1.05 (0.80–1.39, p = 0.741) | 0.99 (0.72–1.37, p = 0.974) |
| Senior surgeon > 5 years training | ||||
| No | 920 (23.6) | 167 (25.9) | ||
| Yes | 2978 (76.4) | 478 (74.1) | 0.88 (0.73–1.07, p = 0.207) | 1.05 (0.78–1.42, p = 0.745) |
| Senior anesthetist > 5 years training | ||||
| No | 980 (25.1) | 189 (29.3) | ||
| Yes | 2919 (74.9) | 456 (70.7) | 0.81 (0.67–0.98, p = 0.025) | 1.02 (0.75–1.39, p = 0.901) |
| Laparoscopic approach | ||||
| No | 2222 (57.0) | 457 (70.9) | ||
| Yes | 1677 (43.0) | 188 (29.1) | 0.55 (0.45–0.65, p < 0.001) | 0.55 (0.42–0.71, p < 0.001) |
| Perforated viscus | ||||
| No | 3474 (89.2) | 450 (69.8) | ||
| Yes | 419 (10.8) | 195 (30.2) | 3.59 (2.95–4.37, p < 0.001) | 3.66 (2.91–4.62, p < 0.001) |
Data are n (%) unless otherwise stated. Hospitals = 339, countries = 52. AIC = 3339.1. c-statistic = 0.790
OR odds ratio, CI confidence interval, HDI human development index, ASA American Association of Anesthesiologists risk score, SD standard deviation
A further prominent association was seen with more surgical site infection (SSI) in low-HDI (OR 3.81, 95% CI 2.78–5.19, p < 0.001) and middle-HDI (OR 2.99, 95% CI 2.34–3.84, p < 0.001) compared with high-HDI (Tables 2, 4). In the multilevel model, the association persisted in low-HDI (OR 2.57, 95% CI 1.33–4.99, p = 0.005) but not middle-HDI (OR 1.38, 95% CI 0.76–2.52, p = 0.291) countries.
Table 4: Surgical site infection
| Surgical site infection | ||||
|---|---|---|---|---|
| No | Yes | Univariable logistic regression OR (95% CI, p value) | Multilevel logistic regression OR (95% CI, p value) | |
| HDI tertile | ||||
| High | 2389 (57.4) | 109 (29.7) | ||
| Middle | 1340 (32.2) | 183 (49.9) | 2.99 (2.34–3.84, p < 0.001) | 1.38 (0.76–2.52, p = 0.291) |
| Low | 432 (10.4) | 75 (20.4) | 3.81 (2.78–5.19, p < 0.001) | 2.57 (1.33–4.99, p = 0.005) |
| Age in completed years | ||||
| Mean (SD) | 28.6 (16.4) | 32.8 (18.9) | 1.01 (1.01–1.02, p < 0.001) | 1.01 (1.01–1.02, p = 0.001) |
| Gender | ||||
| Male | 2205 (53.0) | 208 (56.7) | ||
| Female | 1956 (47.0) | 159 (43.3) | 0.86 (0.69–1.07, p = 0.175) | 0.95 (0.74–1.22, p = 0.666) |
| Diabetes history | ||||
| No | 4058 (97.5) | 341 (92.9) | ||
| Yes | 103 (2.5) | 26 (7.1) | 3.00 (1.89–4.61, p < 0.001) | 1.45 (0.83–2.52, p = 0.189) |
| Smoking currently | ||||
| No | 3415 (82.1) | 287 (78.2) | ||
| Yes | 743 (17.9) | 80 (21.8) | 1.28 (0.98–1.65, p = 0.062) | 1.05 (0.77–1.45, p = 0.751) |
| ASA score | ||||
| 1 | 2937 (72.6) | 213 (58.7) | ||
| 2 | 934 (23.1) | 111 (30.6) | 1.64 (1.28–2.08, p < 0.001) | 1.42 (1.05–1.94, p = 0.025) |
| ≥ 3 | 172 (4.3) | 39 (10.7) | 3.13 (2.13–4.50, p < 0.001) | 1.82 (1.10-3.00, p = 0.020) |
| Procedure start time | ||||
| 0800–1800 (daytime) | 1975 (47.5) | 162 (44.1) | ||
| 1800–2200 (evening) | 1057 (25.4) | 105 (28.6) | 1.21 (0.93–1.56, p = 0.144) | |
| 2200–0800 (night-time) | 1129 (27.1) | 100 (27.2) | 1.08 (0.83–1.40, p = 0.562) | |
| Surgical safety checklist used | ||||
| No, not available in this hospital | 826 (19.9) | 108 (29.4) | ||
| No, but available in this hospital | 253 (6.1) | 45 (12.3) | 1.36 (0.93–1.97, p = 0.108) | 0.92 (0.51–1.65, p = 0.771) |
| Yes | 3082 (74.1) | 214 (58.3) | 0.53 (0.42–0.68, p < 0.001) | 1.00 (0.64–1.54, p = 0.987) |
| Prophylactic antibiotics | ||||
| No | 445 (10.7) | 43 (11.7) | ||
| Yes | 3716 (89.3) | 324 (88.3) | 0.90 (0.65–1.27, p = 0.545) | 0.99 (0.66–1.50, p = 0.976) |
| Senior surgeon > 5 years training | ||||
| No | 943 (22.7) | 138 (37.6) | ||
| Yes | 3217 (77.3) | 229 (62.4) | 0.49 (0.39–0.61, p < 0.001) | 0.86 (0.60–1.23, p = 0.395) |
| Senior anesthetist > 5 years training | ||||
| No | 1006 (24.2) | 154 (42.0) | ||
| Yes | 3155 (75.8) | 213 (58.0) | 0.44 (0.35–0.55, p < 0.001) | 0.86 (0.60–1.24, p = 0.428) |
| Laparoscopic approach | ||||
| No | 2338 (56.2) | 326 (88.8) | ||
| Yes | 1823 (43.8) | 41 (11.2) | 0.16 (0.11–0.22, p < 0.001) | 0.22 (0.14–0.33, p < 0.001) |
| Perforated viscus | ||||
| No | 3654 (87.9) | 258 (70.5) | ||
| Yes | 502 (12.1) | 108 (29.5) | 3.05 (2.38–3.88, p < 0.001) | 3.36 (2.47–4.59, p < 0.001) |
Data are n (%) unless otherwise stated. Hospitals = 339, countries = 52. AIC = 2164. c-statistic = 0.849
OR odds ratio, CI confidence interval, HDI human development index, ASA American Association of Anesthesiologists risk score, SD standard deviation
There was no association in multilevel models between HDI and OSI (Table S1, Supplemental Digital Content).
Determining any influence of laparoscopy compared with an open approach is difficult given the inherent selection bias and the lower availability in low-HDI and middle-HDI countries. This is highlighted by the different populations undergoing laparoscopic compared with open procedures (Table S2, Supplemental Digital Content). Differences in the laparoscopic group included more females, lower ASA score, a greater likelihood of senior surgeon and anesthetist involvement, and lower perforation rates. Two approaches were taken to attempt to reduce the effect of this imbalance: multilevel logistic regression modeling and a propensity-score matched analysis.
After accounting for case-mix imbalance, laparoscopy was still associated with significantly fewer complications (OR 0.55, 95% CI 0.42–0.71, p < 0.001, Table 3) and SSIs (OR 0.22, 95% CI 0.14–0.33, p < 0.001, Table 4). To try and communicate these differences more meaningfully, a simple simulation was performed using different patient baseline characteristics (Table 5). This analysis shows an absolute risk reduction (ARR) in overall complication rate associated with laparoscopy of around 6% [number-needed-to-treat (NNT) = 16] in the absence of perforation and 17% (NNT = 8) when the appendix is perforated across HDI groups. For SSI, the analysis implies a greater potential benefit of laparoscopy in low-HDI (ARR 18.6%, 95% CI 11.4–27.7 with perforation) and middle-income countries (ARR 12.2%, 95% CI 6.6–19.6% with perforation), which is expected given the association of HDI and SSI seen in the multilevel model.
Table 5: Overall complications (top) and SSI (bottom) simulation
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| HDI groupPerforation | LowNo | LowYes | MiddleNo | MiddleYes | HighNo | HighYes |
| Overall complications | ||||||
| Complication (%) with open approach | 14.7 (9.7–20.9) | 37.0 (26.8–48.3) | 13.0 (9.1–17.7) | 33.7 (24.8–43.9) | 13.6 (9.6–18.3) | 35.0 (26.3–44.5) |
| Complication (%) with lap approach | 8.5 (5.1–12.8) | 24.0 (15.5–34.5) | 7.4 (4.7–10.9) | 21.5 (14.1–30.9) | 7.8 (5.3–10.7) | 22.4 (15.7–30.1) |
| Absolute risk reduction (%) open versus laparoscopic | 6.3 (3.5–9.6) | 13.0 (7.7–18.5) | 5.6 (3.3–8.2) | 12.3 (7.5–17.1) | 5.9 (3.3–8.8) | 12.6 (7.5–18.1) |
| Number-needed-to-treat | 16 (11–29) | 8 (6–13) | 18 (13–31) | 9 (6–14) | 17(12–31) | 8 (6–14) |
| Surgical site infection (SSI) | ||||||
| SSI (%) with open approach | 9.8 (5.5–15.9) | 26.1 (15.8–39.2) | 5.7 (2.9–9.7) | 16.6 (8.9–26.8) | 5.1 (2.8–8.0) | 15.0 (8.7–23.3) |
| SSI (%) with lap approach | 2.4 (1.1–4.5) | 7.5 (3.5–13.6) | 1.4 (0.6–2.6) | 4.4 (1.9–8.5) | 1.2 (0.6–2.1) | 3.9 (1.9–6.9) |
| Absolute risk reduction (%) open versus laparoscopic | 7.4 (4.1–12.1) | 18.6 (11.4–27.7) | 4.8 (2.2–7.4) | 12.2 (6.6–19.6) | 3.9 (2.1–6.4) | 11.2 (6.3–17.4) |
| Number-needed-to-treat | 14 (9–25) | 6 (4–9) | 21 (14–46) | 9 (6–16) | 26 (16–48) | 9 (6–16) |
The multilevel logistic regression models were simulated to convert model coefficients into real-world quantities of interest. The probabilities for different characteristics are shown, together with ARR for open versus laparoscopic. NNT with laparoscopic approach to save a complication. Data are proportion as a percentage (95% CI). Baseline covariate levels are age 29 years, gender male, ASA score 1, diabetes no, currently smoking no, checklist no, antibiotics yes, senior surgeon training > 5 years yes, anesthetics training > 5 years yes
To further explore these relationships, a propensity-score-based matching analysis was performed. Patients were first subset into low-/middle-HDI and high-HDI groups. Using all available independent baseline variables and a nearest neighbor approach, 167 patients in the laparoscopic group were matched to 167 in the open group in the low-/middle-HDI subset (Fig. 1, Tables S3 and S4, Supplemental Digital Content) and 783 matched in the high-HDI group. Balance was more easily achieved in the low-/middle-HDI group, with persistent imbalance only seen for seniority of anesthetist and surgical safety checklist use. Balance using nearest neighbor matching was difficult to achieve in the high-HDI group, reflecting de facto differences in the characteristics of patients offered laparoscopic compared with those undergoing open procedures in practice. Alternative matching procedures were successfully explored, but have not been included for space and clarity. Adjusted logistic regression models were applied to the matched sets to address any residual confounding. In the low-/middle-HDI group, a laparoscopic approach was still associated with fewer overall complications (OR 0.23 95% CI 0.11–0.44, p < 0.001), minor complications (OR 0.16 95% CI 0.06–0.35, p < 0.001), and episodes of SSI (OR 0.21 95% CI 0.09–0.45, p < 0.001) (Table S5, Supplemental Digital Content, Fig. 1). Similar results were observed within the matched high-HDI group (Table S6, Supplemental Digital Content).
Discussion
This is the first patient-level prospective study to describe the surgical approach to appendectomy and the frequency of postoperative complications on a global scale. Our findings reveal clear differences in the management of appendicitis and disparities in complication frequency between different HDI groups, with significantly more wound infections (SSI) in low-HDI versus high-HDI countries. A laparoscopic approach was common in the high-HDI group (1693/2499, 67.7%) but infrequent in low- (41/507, 8.1%) and middle-HDI (132/1540, 8.6%) groups. In analyses that attempted as far as it is possible to account for the inherent selection bias in these observational data, laparoscopy in low-/middle-HDI countries was significantly associated with fewer complications and lower SSI rates.
We have previously shown differences in outcomes after emergency surgery by HDI, with mortality found to be higher in low- and middle-HDI countries compared with high-HDI countries both in adults [ref. 4] and children [ref. 17]. In the present study, unadjusted analyses show a similar picture. However, in the multivariable analysis for overall complications, no persistent association was seen with HDI after accounting for case-mix and structural differences. There were persistent differences seen in SSI rates after adjustment. SSI is therefore a phenomenon in which factors not accounted for in our models play an important role. More studies are needed to understand how this can be intervened upon.
It is well established in high-income settings that laparoscopic appendectomy is associated with better outcomes; however, little information exists in low-resource settings [ref. 18–ref. 21]. Wei et al. undertook a randomized comparison of open and laparoscopic appendectomy and concluded that a laparoscopic approach was associated with lower SSI rates and fewer complications,[ref. 18] a finding similar to that observed in the current study. Further advantages include reduced postoperative stay, less postoperative pain, and lower oxidative stress [ref. 19, ref. 20]. In our study, the presence of a perforated appendix was associated with a 3- to 4-fold increase in adverse outcomes in multivariable models, including an increased surgical site and organ space (abscess) infection, findings similar to previous studies [ref. 21]. It has been debated whether a laparoscopic approach is always appropriate for patients with more advanced disease and peritonitis; however, evidence does exist supporting a laparoscopy even in complicated cases where reduced infection rates and postoperative length of stay can be achieved [ref. 22, ref. 23].
Appendicitis is common in low-resource settings but its incidence varies greatly by country. It is the fourth-most common procedure performed by training surgeons in the College of Surgeons of East, Central and Southern Africa (COSECSA) region [ref. 24]. Appendicitis also presents differently in the poorest countries,[ref. 25] which is supported in the current study by the higher perforation rate seen in the low-HDI group (21.5%) compared with high-HDI group (13.9%). Given traditional assumptions around treatment delay and progression to perforation, this may be due to the well-described first-delay in seeking medical attention in low-HDI settings, compounded by a second-delay in reaching a medical facility that may be many days’ travel away [ref. 3]. Alternatively, this may represent a pathophysiological distinction between perforated and non-perforated appendicitis,[ref. 26] with selection exaggerated in low-resource settings by delays in seeking medical attention arising from geographic barriers to access, cultural differences, and the potential out-of-pocket impoverishing or catastrophic costs of surgery discouraging all but the sickest in attending hospital [ref. 27, ref. 28].
The increased use of laparoscopy in low-income settings is controversial. In the poorest regions, the provision of any surgical service is extremely difficult and current high-technology, resource intensive laparoscopy is not feasible. However, our results raise the possibility of a benefit for patients and the healthcare system more widely. Given the higher rates of SSI in some low-income settings, the absolute benefit of laparoscopy is likely to be greater as shown by the simulation results [ARR of SSI in low-HDI countries (18.6%) compared with high-HDI countries (11.2%)]. This translates to a NNT with laparoscopic rather than open surgery of 6 to prevent one SSI in low-HDI countries managing perforated appendicitis. Moreover, in the absence of CT imaging, diagnostic laparoscopy can provide an effective way to investigate patients with acute abdominal pain short of the requirement for a full laparotomy.
The major strength of this study is the collection of patient-level prospective data from 52 countries. This unique dataset allows comparison across the HDI spectrum which is rarely possible. A published, detailed protocol translated into major languages ensured consistent data collection across varying regions without the burden of communication barriers. Local validation by leads ensured data accuracy and completeness was high. The interpretation of observational data is always difficult due to the inherent bias implicit in treatment allocation of patients. We have explored both multilevel models accounting for clustering patients in hospitals and countries, and propensity-score-matched models. In the latter, patients within low-/middle-HDI countries undergoing open or laparoscopic approaches were matched using available baseline variables, thus attempting to compare only “similar” patients who had undergone alternative treatments. Good balance was achieved and benefits of laparoscopy continue to be seen.
There are a number of weaknesses associated with our approach. Denominator data at a country level cannot easily be collected using this methodology. The “snapshot” may not accurately reflect overall practice, particularly where there are prominent seasonal effects [ref. 29]. We were not able to capture the degree of sepsis beyond the ASA and perforation rates, which may result in residual confounding. Within low-income, rural settings, collection of 30-day follow-up data can be challenging as patients are often discharged to remote regions and therefore cannot return to attend follow-up clinics. This was minimized by liberal use of telephone follow-up where feasible. A subsequent validation study of this methodology suggests that telephone follow-up is possible in upwards of one-third of included patients. Validation of data entry is challenging particularly where patient record keeping is limited. Collaborators frequently commented that the collected study data were of higher quality than existing hospital data. At each participating center, a lead was appointed to perform data validation and ensure accurate data-entry.
These results have significant implications for policy makers. Variation exists in outcomes after appendectomy across the world, but at least some of that variation may be explained by local surgical infrastructure such as the availability of laparoscopic surgery. Health services are faced with competing priorities and must balance a desire to improve surgical care with the costs of treating, say, malaria. The introduction of any new technology in a resource-poor setting must also be done with care. Recommendations include ensuring the existence of sufficient financial support and organizational systems to address staff training, including biomedical engineering staff to undertake equipment maintenance, and to establish robust, affordable, and sustainable supply chains [ref. 10]. A successful implementation of laparoscopic surgery has already been demonstrated at scale in low-resource settings [ref. 30].
Future research must focus on identifying innovative, affordable, and safe strategies to implement and scale laparoscopic surgery in low-resource settings. Such adaptive techniques may include gasless laparoscopy, room air insufflation, and development of affordable, reusable instrumentation. In addition, there is an ongoing need to establish robust systems for the continuous measurement of surgical outcomes across the world. High-quality clinical trials relevant to low-HDI countries must be performed to ensure the identification of the most effective treatments, such as how to reduce SSI. Outcomes in surgery will only improve with system-wide improvements across the pre-hospital, hospital, and post-hospital sectors.
This study has shown significant variation in the management and outcomes following appendectomy worldwide. The availability of laparoscopy differs by country HDI, and appears to be significantly associated with better outcomes. There are profound clinical, operational, and financial barriers to the introduction of laparoscopy that if overcome could result in significantly improved outcomes for patients and the wider health system in low-resource environments.
Supplementary Materials
References
- B Stewart, P Khanduri, C McCord, M Ohene-Yeboah, S Uranues, F Vega Rivera, C Mock. Global disease burden of conditions requiring emergency surgery. Br J Surg, 2014. [DOI | PubMed]
- BC Alkire, NP Raykar, MG Shrime, TG Weiser, SW Bickler, JA Rose, CT Nutt, SLM Greenberg, M Kotagal, JN Riesel, M Esquivel, T Uribe-Leitz, G Molina, N Roy, JG Meara, PE Farmer. Global access to surgical care: a modelling study. Lancet Glob Health, 2015. [DOI | PubMed]
- JG Meara, AJM Leather, L Hagander, BC Alkire, N Alonso, EA Ameh, SW Bickler, L Conteh, AJ Dare, J Davies, ED Mérisier, S El-Halabi, PE Farmer, A Gawande, R Gillies, SLM Greenberg, CE Grimes, RL Gruen, EA Ismail, TB Kamara, C Lavy, G Lundeg, NC Mkandawire, NP Raykar, JN Riesel, E Rodas, J Rose, N Roy, MG Shrime, R Sullivan, S Verguet, D Watters, TG Weiser, IH Wilson, G Yamey, W Yip. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet, 2015. [DOI | PubMed]
- Mortality of emergency abdominal surgery in high-, middle- and low-income countries. Br J Surg, 2016. [DOI | PubMed]
- M Ferris, S Quan, BS Kaplan, N Molodecky, CG Ball, GW Chernoff, N Bhala, S Ghosh, E Dixon, S Ng, GG Kaplan. The global incidence of appendicitis: a systematic review of population-based studies. Ann Surg, 2017. [PubMed]
- 6.GBD Results: Appendicitis by country sociodemographic index. http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2016-permalink/3c40df49b7377792f0fab1044d22d95e. Accessed 18 Oct 2017
- KK Varadhan, KR Neal, DN Lobo. Safety and efficacy of antibiotics compared with appendicectomy for treatment of uncomplicated acute appendicitis: meta-analysis of randomised controlled trials. BMJ, 2012. [DOI | PubMed]
- AC McCoy, E Gasevic, RE Szlabick, AE Sahmoun, RP Sticca. Are open abdominal procedures a thing of the past? An analysis of graduating general surgery residents’ case logs from 2000 to 2011. J Surg Educ, 2013. [DOI | PubMed]
- Multicentre observational study of performance variation in provision and outcome of emergency appendicectomy. Br J Surg, 2013. [DOI | PubMed]
- TE Chao, M Mandigo, J Opoku-Anane, R Maine. Systematic review of laparoscopic surgery in low- and middle-income countries: benefits, challenges, and strategies. Surg Endosc, 2016. [DOI | PubMed]
- 11.GlobalSurg Collaborative GlobalSurg 1 (2016) In: Globalsurg. http://globalsurg.org/projects/globalsurg-1/. Accessed 14 Dec 2016
- A Bhangu, JE Fitzgerald, S Fergusson, C Khatri, H Holmer, K Søreide, EM Harrison. Determining universal processes related to best outcome in emergency abdominal surgery: a multicentre, international, prospective cohort study. BMJ Open, 2014. [DOI | PubMed]
- A Bhangu, AG Kolias, T Pinkney, NJ Hall, JE Fitzgerald. Surgical research collaboratives in the UK. Lancet Lond Engl, 2013. [DOI]
- E von Elm, DG Altman, M Egger, SJ Pocock, PC Gøtzsche, JP Vandenbroucke. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet, 2007. [DOI | PubMed]
- PA Harris, R Taylor, R Thielke, J Payne, N Gonzalez, JG Conde. Research Electronic Data Capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform, 2009. [DOI | PubMed]
- TC Horan, M Andrus, MA Dudeck. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control, 2008. [DOI | PubMed]
- C GlobalSurg. Determinants of morbidity and mortality following emergency abdominal surgery in children in low-income and middle-income countries. BMJ Glob Health, 2016. [DOI]
- H-B Wei, J-L Huang, Z-H Zheng, B Wei, F Zheng, W-S Qiu, W-P Guo, T-F Chen, T-B Wang. Laparoscopic versus open appendectomy: a prospective randomized comparison. Surg Endosc, 2010. [DOI | PubMed]
- R Aktimur, AK Gokakin, K Deveci, M Atabey, O Topcu. Oxidative stress markers in laparoscopic vs. open appendectomy for acute appendicitis: a double-blind randomized study. J Minim Access Surg, 2016. [DOI | PubMed]
- X Li, J Zhang, L Sang, W Zhang, Z Chu, X Li, Y Liu. Laparoscopic versus conventional appendectomy—a meta-analysis of randomized controlled trials. BMC Gastroenterol, 2010. [DOI | PubMed]
- O Bat, H Kaya, HK Celik, NA Sahbaz. Clinical results of laparoscopic appendectomy in patients with complicated and uncomplicated appendicitis. Int J Clin Exp Med, 2014. [PubMed]
- P Horvath, J Lange, R Bachmann, F Struller, A Königsrainer, M Zdichavsky. Comparison of clinical outcome of laparoscopic versus open appendectomy for complicated appendicitis. Surg Endosc, 2016. [PubMed]
- Y Taguchi, S Komatsu, E Sakamoto, S Norimizu, Y Shingu, H Hasegawa. Laparoscopic versus open surgery for complicated appendicitis in adults: a randomized controlled trial. Surg Endosc, 2016. [DOI | PubMed]
- 24.E-Logbook | COSECSA. (2016) http://www.cosecsa.org/e-logbook-portal. Accessed 15 Dec 2016
- VY Kong, B Sartorius, DL Clarke. Acute appendicitis in the developing world is a morbid disease. Ann R Coll Surg Engl, 2015. [DOI | PubMed]
- EH Livingston, WA Woodward, GA Sarosi, RW Haley. Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management. Ann Surg, 2007. [DOI | PubMed]
- MG Shrime, A Dare, BC Alkire, JG Meara. A global country-level comparison of the financial burden of surgery. Br J Surg, 2016. [DOI | PubMed]
- NP Raykar, RR Yorlets, C Liu, R Goldman, SLM Greenberg, M Kotagal, PE Farmer, JG Meara, N Roy, RD Gillies. The how project: understanding contextual challenges to global surgical care provision in low-resource settings. BMJ Glob Health, 2016. [DOI | PubMed]
- P-L Wei, C-S Chen, JJ Keller, H-C Lin. Monthly variation in acute appendicitis incidence: A 10-year nationwide population-based study. J Surg Res, 2012. [DOI | PubMed]
- R Price, O Sergelen, C Unursaikhan. Improving surgical care in Mongolia: a model for sustainable development. World J Surg, 2013. [DOI | PubMed]