
RETRACTED: Effect Comparison of E-Cigarette and Traditional Smoking and Association with Stroke—A Cross-Sectional Study of NHANES
Abstract
Introduction: Tobacco use is one of the most significant risk factors for stroke. Besides traditional cigarettes and combustible products, the use of e-cigarettes and electronic nicotine delivery products has been widespread among young adults in the recent era. Furthermore, the trend of vaping has increased over the last decade. However, the relationship between e-cigarettes and stroke is largely unknown. The aim of this study was to evaluate the prevalence and identify the relationship between e-cigarette smoking and stroke. Methods: A cross-sectional study was performed using the NHANES database of the US population. Adults with a history of smoking were considered in our study and divided into three groups, e-cigarette users, traditional, and dual smokers. The Chi-squared test, Wilcoxon rank-sum test, and multivariable logistic regression analysis were used to identify the prevalence and association of e-cigarette consumption and stroke. Results: Out of a total of 266,058 respondents from 2015 to 2018, we found 79,825 respondents who smoked e-cigarettes (9.72%) or traditional (29.37%) or dual smoking (60.91%). Stroke prevalence among e-cigarette smokers was 1.57%. Stroke was more prevalent among traditional smokers than among e-cigarette smokers. (6.75% vs. 1.09%; p < 0.0001) E-cigarette smokers had early onset of stroke in comparison with traditional smokers. (median age: 48 vs. 59 years; p < 0.0001). Among females with stroke, the prevalence of e-cigarette use was higher in comparison with traditional smoking (36.36% vs. 33.91%; p < 0.0001). Among the stroke population, the prevalence of e-cigarette use was higher among Mexican-Americans (21.21% vs. 6.02%) and other Hispanics (24.24% vs. 7.70%) compared with traditional smoking (p < 0.0001). The regression analysis found higher odds of stroke history among e-cigarette users than traditional smokers [aOR: 1.15; 95% CI: 1.15–1.16)]. Conclusion: Though stroke was more prevalent in traditional smokers, the incidence of stroke was early-in-onset and was strongly associated with e-cigarette use compared to traditional smokers. We have also identified vascular effects of e-cigarettes components as possible triggers for the stroke.
Article type: Research Article
Keywords: e-cigarette, vaping, ENDS, e-cigs, smoking, ischemic stroke, cerebrovascular disorders, stroke risk factors, NHANES
Affiliations: Department of Public Health, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA; neel4ahm@gmail.com; Department of Public Health, University of California, Berkeley, CA 92093, USA; mahika_khurana@berkeley.edu; Department of Biology, York University, Toronto, ON M3J 1P3, Canada; akshadapar@gmail.com; Department of Public Health, Milken Institute School of Public Health, George Washington University, Washington, DC 20052, USA; patelamrapali428@gmail.com; Department of Neurology, Larkin Community Hospital, Miami, FL 33143, USA; sumjuanfer41@gmail.com; Department of Internal Medicine, Texas Tech University Health Sciences Center, Transmountain Campus, El Paso, TX 79430, USA; rutul.patel@ttuhsc.edu (R.P.); anumistr@ttuhsc.edu (A.M.); Department of Internal Medicine, Hudson Regional Hosp, Secaucus, NJ 07094, USA; eseosaurhoghide@gmail.com; Department of Child Neurology, Jersey Shore University Medical Center, Neptune City, NJ 07753, USA; bhriguva@gmail.com; Department of Internal Medicine, Geisinger Med Center, Danville, PA 17822, USA; mhdaliabdulqader@gmail.com; Department of Epidemiology and Biostatistics, Boston University School of Public Health, Boston, MA 02118, USA; neev.n.mehta@gmail.com; Department of Neurology, Mayo Clinic, Albert Lea, MN 56007, USA; dockogul26@gmail.com; Department of Neurology, Stormont Vail Health, Topeka, KS 66604, USA; drshahshamik@gmail.com
License: © 2022 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.3390/neurolint14020037 | PubMed: 35736618 | PMC: PMC9227824
Relevance: Moderate: mentioned 3+ times in text
1. Introduction
The prevalence, mortality, and disability-adjusted life years (DALYs) associated with stroke have steadily increased globally, from 1990 to 2019, reaching approximately 101 million (95% UI: 93.2 to 111 million); death from stroke has decreased over the past decade in the USA [ref. 1,ref. 2]. Stroke continues to be the fifth-leading cause of death [ref. 1]. Tobacco consumption is a major modifiable risk factor associated with stroke, CVD, and silent infarction [ref. 2,ref. 3] Globally, smoking is the second-leading cause of death and the leading cause of DALYs [ref. 2]. There are various forms of tobacco consumption [ref. 4], of which vaping is very popular among adolescents [ref. 5]. The popularity of vaping has sharply increased over the last two decades [2011: 1.5% to 2018: 20.8%] [ref. 2], and the most recent data shows that 20% of students in grades 7–12 are current vapers, and 34% have tried it at least once. Another study found a 112% increase in the rate of vaping among youth from 2017 to 2019 [ref. 6].
The few studies that have shown a positive association between the use of e-cigarettes and combustible cigarettes with vascular disorders were limited either by choosing specific target populations [ref. 5,ref. 7] or being not specific to stroke [ref. 7]. Parekh et al. showed that dual use of e-cigarettes and combustible cigarettes was associated with 2.9 times higher odds of stroke but no association between isolated e-cigarette use with stroke (0.69; 95% CI: 0.3–1.4) among the population of 18–44-year-olds [ref. 5]. Kaiser et al. showed that the use of nicotine and/or vaping leads to worsening outcomes in stroke, secondary to a state of glucose deprivation in the neurovascular unit, which augments neuronal damage and enhances ischemic brain injury [ref. 8]. The limited information on long-term health effects of e-cigarettes on CVD is one of the reasons why AHA maintains its stand on e-cigarette regulation and health care screening precisely like other forms of tobacco [ref. 9].
Hence, we aim to investigate the association of e-cigarettes and traditional smoking with ischemic stroke using the National Health and Nutrition Examination Survey (NHANES) among the general population of the USA. The risk of stroke incidence and hospitalizations due to tobacco consumption has increased among adults. However, the association between e-cigarette smoking and stroke development in this population remains unknown. This study aims to examine the effect of e-cigarettes and traditional smoking on stroke.
2. Methods
2.1. Details of Data
The National Health and Nutrition Examination Survey (NHANES) is a population-based cross-sectional survey study program designed to assess the health and nutritional status of adults and children in the United States. NHANES is a part of the National Center for Health Statistics (NCHS) and the Centers for Disease Control and Prevention (CDC). The NHANES includes socio-demographic, dietary, examination, lab findings, and health-related questions. The dataset is available at the CDC website https://www.cdc.gov/nchs/nhanes/about_nhanes.htm, accessed on 30 August 2021, and details of the respondents are de-identified, so institutional IRB was not required.
2.2. Demographic Characteristics of the Study Population
A cross-sectional retrospective population-based study was performed using the NHANES database 2015–2018 of the US. Participants 18 or older with a history of smoking were considered in our study and divided into three groups, exclusive e-cigarette users, traditional smokers, and dual (e-cigarette + traditional) smokers. The confirmed history of stroke among all three groups was extracted.
Exclusive e-cigarettes, vaping, or electronic nicotine delivery systems (ENDS) use was defined by “SMQ900” (Ever used an e-cigarette?) and “SMQ905” (During the past 30 days, how many days have you used an e-cigarette?). Exclusive traditional smoking was defined by either “SMQ020” (Smoked at least 100 cigarettes in life) or “SMQ040” (Do you now smoke cigarettes?). Dual smokers were defined by respondents who responded “yes” to both e-cigarettes and traditional smoking. Stroke was defined by “MCQ160f” (Has a doctor or other health professional ever told you had a stroke?) and “MCQ180f”—(Age when told you had a stroke?).
We have included socio-demographic variables like age, race, annual household income, and comorbidities like diabetes, cholesterol, hypertension, depression, obesity, cancer, substance abuse (marijuana, cocaine/heroin/methamphetamine, illegal injectable drug), alcohol use (median average # of drinks/day and binge drinking (women: 4 or more and men: 5 or more drinks/day in past 12 months), and preventive aspirin use. We have collected data on high blood pressure on two occasions, recent systolic and diastolic blood pressure, body mass index (BMI), S. cholesterol, S. LDL, S. TG, and HbA1C.
2.3. Outcomes
The primary aim of this study is to evaluate the prevalence of e-cigarette, traditional, and dual smokers among respondents with a history of stroke. The secondary aim of this study is to evaluate the odds of different methods of nicotine consumption among respondents with a history of stroke. We have also evaluated the odds of e-cigarette use in the past 30 days among the population having a history of stroke.
2.4. Statistical Analysis
We analyzed the data using SAS software (Version 9.4, SAS Institute Inc., Cary, NC, USA). We performed univariate analysis to find out socio-demographic characteristics of the respondents with different methods of nicotine consumption among the stroke population, using Chi-square for categorical variables and a t-test and Wilcoxon ransom test for continuous variables. Multivariable logistic regression models were generated to calculate the odds of e-cigarettes among the stroke population in comparison with traditional smokers after adjusting for confounding variables. There was no pre-decided sample size calculation. p-value < 0.05 was considered significant, and an adjusted odds ratio (aOR) with a 95% confidence interval (95% CI) was calculated.
In regression analysis, the models were adjusted with socio-demographic variables, like age, gender, and annual household income, and comorbidities, like diabetes, cholesterol, hypertension, depression, cancer, substance abuse (marijuana, cocaine/heroin/methamphetamine, illegal injectable drug), alcohol use (median average # of drinks/day and binge drinking (women: 4 or more and men: 5 or more drinks/day in past 12 months), and preventive aspirin use. We collected data on high blood pressure on two occasions, recent systolic and diastolic blood pressure, and body mass index (BMI).
3. Results
Out of 266,058 respondents from 2015 to 2018 in the NHANES survey, we found 79,825 respondents who smoked e-cigarettes or traditional smoking or dual smoking, after excluding patients with age < 18 years and admissions with missing data for age, gender, or ethnicity. Out of 79,825 respondents, 7756 (9.72%) were e-cigarette smokers, 23,444 (29.37%) were dual smokers, and 48,625 (60.91%) were traditional smokers. The overall prevalence of stroke was 5.41% (n = 4194) among various types of smokers. The overall prevalence of stroke among e-cigarette smokers was 1.57%, among traditional smokers was 78.04%, and among dual smokers was 20.39%. Stroke was more prevalent among traditional smokers than e-cigarette and dual smokers (6.75% vs. 1.09% vs. 3.72% p < 0.0001). E-cigarette smokers have an early onset of stroke compared to dual and traditional smokers, respectively (median age in years: 48 vs. 50 vs. 59; p < 0.0001) (Table 1).
Table 1: Prevalence of stroke among various smoking habits among NHANES respondents 2015–2018 (n = 79,825).
| E-Cigarette Smokersn = 7756 (9.72%) | Dual E-Cigarette + Traditional Smokersn = 23,444 (29.37) | Traditional Smokers n = 48,625 (60.91%) | Totaln = 79,825 (100) | p Values | |
|---|---|---|---|---|---|
| Stroke (n)(Prevalence %)(Column % comparison between different smoking habits) | 66(1.57)(1.09) | 855(20.39)(3.72) | 3273(78.04)(6.75) | 4194(100)(5.41) | <0.0001 |
| Age of onset of stroke in years(Median + IQR) | 48 (42–58) | 50 (40–58) | 59 (50–69) | <0.0001 |
3.1. Socio-Demographic Characteristics and Comorbidities
Among 4194 respondents with a history of stroke, males had higher use of e-cigarettes in comparison to females (1.61% vs. 1.52%; p < 0.0001). Among females with stroke, the prevalence of e-cigarette use was higher than traditional smoking (36.36% vs. 33.91%; p < 0.0001) Among Mexican-Americans (21.21% vs. 6.02%) and other Hispanics (24.24% vs. 7.70%), the prevalence of e-cigarette use was higher than traditional smoking. (p < 0.0001) Overall, e-cigarette use was higher among other Hispanics than among Mexican-Americans and among other races. (5.13% vs. 4.52% vs. 1.37% vs. 2.82%; p < 0.0001) (Table 2).
Table 2: Socio-demographics characteristics of various smoking habits among respondents with history of stroke (n = 4194).
| E-Cigarette Smokers with History of Stroken = 66(1.57%) | Dual E-Cigarette + Traditional Smokers with History of Stroken = 855 (20.39%) | Traditional Smokers with History of Stroke n = 3273 (78.04%) | Totaln = 4194 (100) | p Value | |
|---|---|---|---|---|---|
| Age in years at screening(Median + IQR) | 50 (45–63) | 55 (47–64) | 69 (62–80) | <0.0001 | |
| Sex (%) | <0.0001 | ||||
| Female | 36.36 | 51.93 | 33.91 | 37.63 | |
| Male | 63.64 | 48.07 | 66.09 | 62.37 | |
| Race (%) | <0.0001 | ||||
| Mexican-American | 21.21 | 11.58 | 6.02 | 7.39 | |
| Other Hispanic | 24.24 | 5.15 | 7.70 | 7.44 | |
| Non-Hispanic White | 37.88 | 47.13 | 42.77 | 43.59 | |
| Non-Hispanic Black | 0.00 | 24.09 | 31.29 | 29.33 | |
| Non-Hispanic Asian | 0.00 | 0.00 | 3.79 | 2.96 | |
| Other Race—Including Multi-Racial | 16.67 | 12.05 | 8.43 | 9.30 | |
| Annual Household Income (%) | <0.0001 | ||||
| $0–$25,000 | 57.58 | 59.15 | 50.67 | 52.44 | |
| $25,000–$65,000 | 16.67 | 32.18 | 32.49 | 32.16 | |
| $65,000–$100,000 | 25.76 | 4.27 | 7.99 | 7.57 | |
| >$100,000 | 0.00 | 4.41 | 8.85 | 7.83 | |
| Comorbidities (%) | |||||
| Coronary Heart Disease (%) | 25.76 | 15.32 | 27.62 | 25.08 | <0.0001 |
| Congestive Heart Failure (%) | 25.76 | 21.75 | 16.59 | 17.79 | <0.0001 |
| High Blood Pressure—2+ Times (%) | 60.98 | 98.02 | 80.91 | 84.11 | <0.0001 |
| Recent Systolic Blood Pressure in mmHg(Median) * | 118 | 120 | 134 | <0.0001 | |
| Recent Diastolic Blood Pressure in mmHg(Median) * | 70 | 80 | 80 | <0.0001 | |
| Taking Prescribed Medicine For HBP (%) | 100.00 | 81.66 | 89.33 | 87.89 | <0.0001 |
| High Cholesterol Level (%) | 25.76 | 60.58 | 58.11 | 58.11 | <0.0001 |
| Taking Prescribed Medicine High Cholesterol (%) | 100.00 | 82.52 | 84.39 | 81.83 | 0.2876 |
| LDL-Cholesterol, NIH Equation 2 (mg/dL) (Median) * | 112 | 101 | 110 | <0.0001 | |
| Diabetes (%) | 50.00 | 19.06 | 36.63 | 33.26 | <0.0001 |
| Last Hb A1C Level (Median) * | 5.7 | 7.2 | 7.9 | <0.0001 | |
| Feeling Down, Depressed, Or Hopeless (%) | <0.0001 | ||||
| Several Days | 12.12 | 17.56 | 18.24 | 17.99 | |
| More Than Half The Days | 0.00 | 13.59 | 8.91 | 9.73 | |
| Nearly Every Day | 21.21 | 19.87 | 7.46 | 10.29 | |
| Liver Disorders (%) | 21.21 | 6.43 | 9.84 | 9.32 | <0.0001 |
| Cancer Or Malignancy (%) | 25.76 | 17.19 | 24.35 | 22.91 | <0.0001 |
| Alcohol use disorder—Heavy drinking (%) † | 30.91 | 41.97 | 61.24 | 56.03 | <0.0001 |
| Marijuana or Hashish (%) | 100.00 | 92.15 | 66.20 | 78.61 | <0.0001 |
| Cocaine/Heroin/Methamphetamin (%) | 71.21 | 38.85 | 31.64 | 34.93 | <0.0001 |
| Inject Illegal Drug (%) | 21.21 | 1.77 | 4.63 | 4.63 | <0.0001 |
Percentage in brackets are column %, indicating a direct comparison between e-cigarette users vs. dual smokers vs. traditional smokers. * Due to positive skewed data and absence of 75th percentile (Q3) value, IQR for the median was not mentioned † Heavy drinking: for women, 8 or more drinks per week, and for men, 15 or more drinks per week.
Among stroke respondents with congestive heart failure, the prevalence of e-cigarette utilization (25.76%) was higher compared to that of traditional smokers (16.59%) and dual smokers (21.75%). (p < 0.0001). Among respondents with high blood pressure, the prevalence of dual smoking was higher in comparison to traditional smoking. (98.02% vs. 80.91%; p < 0.0001). The prevalence of dual smokers was higher among people with high cholesterol levels than traditional smoking. (60.58% vs. 58.11%, p < 0.0001) E-cigarette smokers had a higher percentage of diabetes in comparison to traditional smokers. (50.0% vs. 36.63%; p < 0.0001) E-cigarette use was higher in people who had depression nearly every day than in traditional smokers (21.21% vs. 7.46%, p < 0.0001). Similarly, we found higher e-cigarette utilization with liver disorders (21.21% vs. 9.84%, p < 0.0001). Among substance users with a history of stroke, the prevalence of marijuana or hashish (100.00% vs. 66.20%), cocaine/heroin/methamphetamine (71.21% vs. 31.64%), and injectable illegal drug abuse (21.21% vs. 4.63%) were higher among e-cigarette users compared to traditional smoking. (p < 0.0001) (Table 2).
3.2. Multivariable Logistic Regression Showing Association between Stroke and Smoking Habits
In multivariable logistic regression analysis, after adjusting for socio-demographic characteristics and comorbidities, the odds of having a history of stroke was higher among e-cigarette in comparison with traditional smokers (adjusted odds ratio (aOR): 1.15; 95% CI: 1.15–1.16; p < 0.0001). Dual smoker respondents had 14% higher odds of stroke history in comparison with traditional smokers (aOR: 1.14; 95% CI: 1.14–1.15; p < 0.0001). Respondents who smoked e-cigarettes in the last 30 days were also associated with higher odds of stroke prevalence in comparison to non-e-cigarette smokers in the last 30 days (aOR: 1.14; 95% CI: 1.14–1.15; p < 0.0001) (Table 3).
Table 3: Regression analysis showing relationship between various types of tobacco consumption and stroke.
| Variable | Multivariable Analysis *Odds Ratio (95% Confidence Interval); p Value | c-Value (Area under ROC) |
|---|---|---|
| Possibility of having history of stroke = 1 | ||
| Non-smokers | Reference | |
| E-cigarette smokers vs. Traditional smokers | 1.15 (1.15–1.16); p < 0.0001 | 0.733 |
| Dual smokers vs. Traditional smokers | 1.14 (1.14–1.15); p < 0.0001 | |
| E-cigarette smoking in last 30-days vs. no-E-cigarette smoking in last 30-days | 1.60 (1.60–1.61); p < 0.0001 | 0.894 |
* Model for multivariable regression analysis was adjusted with sociodemographic variables like age, gender, race, annual household income, and comorbidities.
4. Discussion
Although stroke was more prevalent in traditional smokers, our cross-sectional study found that e-cigarette smokers had an early onset of stroke compared to traditional and dual smokers. Furthermore, the odds of having a history of stroke was 1.15 times higher among e-cigarette and 1.14 times higher in dual smokers compared to traditional smokers. These findings have clear implications in helping physicians, healthcare policymakers, and tobacco product regulatory authorities to call for strict new regulations on e-cigarette access, sales, and marketing.
Tobacco consumption, a known modifiable risk factor, is associated with stroke and cardiovascular disease, including myocardial infarction [ref. 10,ref. 11]. Although death from stroke has decreased in the last decade, the use of tobacco products such as e-cigarettes and vaping has trended upward in the last two decades [ref. 12]. According to the World Health Organization 2018, vaping has increased from around 7 million users in 2011 to 41 million in 2018, with a projection of more than 55 million by 2021 [ref. 13]. Globally, tobacco consumption is worth an estimated $19.3 billion, up from around $7 billion five years ago, of which the US is one of the biggest markets [ref. 14]. Prior studies have shown that e-cigarettes are less harmful than tobacco cigarettes and can help smokers quit or reduce tobacco use [ref. 15,ref. 16,ref. 17,ref. 18,ref. 19]. But our study reveals that e-cigarette users had higher odds of stroke than traditional smokers. In addition, we found that dual smokers (e-cigarette plus traditional) had 14% higher odds of stroke than traditional smokers alone. The higher odds of stroke in dual smokers suggest that e-cigarettes may have an additive effect on traditional smokers. The additive effect may be attributed to e-cigarette ingredients other than nicotine, like carbonyls, including aldehydes such as formaldehyde, acetaldehyde, and acrolein; fine and ultrafine particulate matter (PMs); benzene; toluene; ethylbenzene; and xylenes (BTEX) [ref. 8,ref. 20,ref. 21,ref. 22,ref. 23]. Parekh et al. also found higher odds of stroke among the young adult population (18–44 years) secondary to the additive effect of e-cigarettes (aOR: 2.91) on current or former traditional smokers (sole combustible cigarette OR: 1.83), without establishing a relationship between sole e-cigarette use and stroke [ref. 5].
Long-term exposure to higher nicotine levels is known to increase the risk of atherosclerosis and further promote stroke risk [ref. 11,ref. 24]. According to Kaiser et al., e-cigarettes, like traditional smoking, can cause a loss of blood–brain barrier (BBB) integrity and vascular inflammation [ref. 25]. Several studies have documented the detrimental effect of non-nicotinic ingredients of e-cigarettes on cerebral and cardiovascular systems (Table 4). Acrolein and PM inhalation from smoking and ambient air pollution have previously been reported to have various deleterious effects on the vascular system, including increasing blood pressure; increasing vascular injury by impairing vascular repair capacity; and increasing the risk of thrombosis and atherosclerosis due to endothelial dysfunction, dyslipidemia, and platelet activation [ref. 11,ref. 26,ref. 27,ref. 28,ref. 29,ref. 30,ref. 31,ref. 32,ref. 33,ref. 34]. Kuntic et al. found that E-cigarette vapor exposure increases vascular, cerebral, and pulmonary oxidative stress through toxic aldehyde(acrolein)-mediated NOX-2-dependent mechanisms [ref. 35].
Table 4: Potential vascular effects of e-cigarette components.
| Component Potentially Involved | Effect [ref. 11,ref. 26,ref. 27,ref. 28,ref. 29,ref. 30,ref. 31,ref. 32,ref. 33,ref. 34] |
|---|---|
| Acrolein, PMs, nicotine | Increased blood pressure |
| Acrolein | Myocardial dysfunction and cardiomyopathy, impaired vascular repair, and vascular injury |
| Acrolein, PMs | Reduced cardiac contractility, Increased risk of thrombosis, increased risk of ventricular arrhythmias |
| PMs, nicotine | Coronary artery disease and myocardial infarction |
PMs: fine and ultrafine particulate matters.
A few studies have reported that e-cigarette use negatively impacts heart rate and blood pressure [ref. 36,ref. 37,ref. 38,ref. 39]. In addition, E-cigarettes cause endothelial cell dysfunction, vascular injury, and oxidative stress, which play important roles in the pathogenesis of stroke [ref. 40,ref. 41]. Furthermore, e-cigarette vapor extracts (toxic chemical, fine particulate matter: 2.5 μm and smaller, and nicotine) were found to enhance platelets’ activation (aggregation-adhesion-inflammation), which potentiates the atherosclerosis process [ref. 42]. S. Hom et al. found that e-vapor extracts have the same effect on the vascular system as traditional tobacco products, including myocardial infarction and stroke, and they noticed that it is fine particulate matter (PMs), not nicotine or toxic combustion products, that activates the hemostatic system/platelet activation. Thus, it is plausible that just reducing exposure to the fine particulate matter may reduce some of the risks associated with CVD development [ref. 42]. Acute and chronic effects of e-cigarette extract as a possible risk factor and trigger for the stroke were summarized in Figure 1 and described in detail in Table 5.
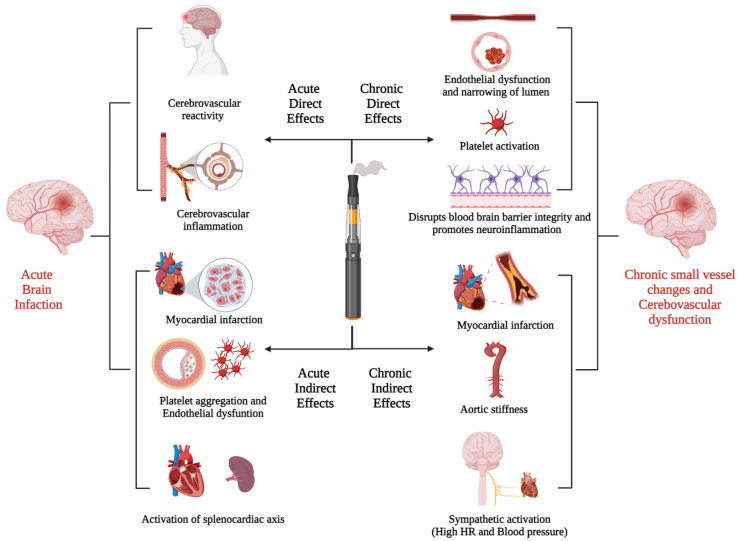
Table 5: Acute and chronic effects of e-cigarettes as a possible risk factor and trigger for stroke.
| Acute Direct Effect | |
| Kuntic et al. [ref. 35] | E-cigarette product acrolein (reactive aldehydes) mediated NOX-2-driven oxidative stress and cerebrovascular inflammation |
| Caporale et al. [ref. 43] | Transient impairment of cerebrovascular reactivity and endothelial function |
| Sifat et al. [ref. 8] | Induces a state of glucose deprivation at the neurovascular unit, leading to enhanced ischemic brain injury and/or stroke risk |
| Acute Indirect Effect | |
| Antoniewicz et al.,Mitchelle et al. [ref. 44,ref. 45] | Increased HR; increased arterial stiffness is an independent risk factor for cardio and cerebrovascular events such as myocardial infarctions and stroke |
| Nocella et al. [ref. 46] | Increase the soluble CD40L and P-selectin; enhance platelet aggregation |
| Boas et al. [ref. 47] | Activation of splenocardiac axis (increase oxidative stress and increase sympathetic activity) |
| Carnevale et al. [ref. 40] | Increase oxidative stress and endothelial dysfunction by increasing soluble NOX-mediated peptides and decreasing NO bioavailability and vitamin E |
| Chronic Direct Effect | |
| Kuntic et al. [ref. 35] | Endothelial dysfunction and narrowing of vessels |
| Kaisar et al. [ref. 25] | Alter blood-brain barrier (BBB) permeability and vascular inflammation |
| Qasim et al. [ref. 48] | In mice, alter physiological hemostasis and increase the risk of thrombogenic events; platelet activation |
| Chronic Indirect Effect | |
| Alzahrani et al. [ref. 49] | Increased odds of having myocardial infarction (OR = 1.79, 95% CI = 1.20, 2.66, p = 0.004) |
| Moheimani et al. [ref. 50] | Increases in cardiac sympathetic activity and oxidative stress, both of which increase the risk of vascular disease |
| Frederik Franzen et al. [ref. 51] | Increase peripheral and central blood pressure and pulse wave velocity |
| Vlachopoulos et al. [ref. 52] | Increase aortic stiffness and increase blood pressure |
In our study, among respondents with a history of stroke, males had higher use of e-cigarettes in comparison to females. However, among females with stroke, the prevalence of e-cigarette use was higher in comparison with traditional smoking. This study reveals that the stroke population with coexisting conditions like congestive heart failure, depression, and hypertension had higher odds of e-cigarette utilization compared to traditional smoking. Previous studies have also reported a strong association between e-cigarette use and level of stress, depression, CHF, and hypertension [ref. 26,ref. 28,ref. 31,ref. 53]. Our study also reports that the prevalence of marijuana or hashish, cocaine, heroin, methamphetamine, and injectable illegal drug abuse was higher among e-cigarette users than traditional smoking.
Secondly, we have also evaluated the odds of e-cigarette use in the last 30 days in stroke population. In the VESUVIUS study, George et al. reported short-term beneficial effects from switching to e-cigarette smoking on vascular function and found a significant improvement in endothelial function and vascular stiffness in e-cigarette smokers who had switched from traditional smoking to e-cigarette smoking within the last 30 days [ref. 54]. However, in contrast, we found higher odds of stroke prevalence compared to non-e-cigarette smokers in respondents who smoked e-cigarettes in the previous 30 days. This results from the acute harmful effects of e-cigarettes on vascular function, including high blood pressure and heart rate, increased arterial stiffness, endothelial dysfunction, and increased cerebrovascular oxidative stress [ref. 40,ref. 43,ref. 44,ref. 45]. This finding of our study is limited by the fact that ‘non-e-cigarette smokers in the last 30 days’ could have smoked e-cigarettes outside the last 30 days of the time frame, and stroke could occur before smokers switch from traditional smoking.
5. Strength and Limitations
Our study has several limitations. First, because of the study’s cross-sectional design, causal inferences may be limited, with the possibility of reverse temporality, as we considered isolated e-cigarettes smokers separate from traditional and dual smokers (history of traditional and e-cigarette smoking at least once). We have assumed that isolated e-cigarette smokers, as mentioned in the survey, never had a history of traditional smoking. So if they had a stroke, they would not start or switch their form of smoking. Thus, this stroke episode happened after e-cigarettes had started. Secondly, the study cannot determine the amount or type of e-cigarette use, timing, frequency, nature of stroke, stroke severity, or timing. We could not evaluate the role of e-cigarettes as a trigger of stroke. This survey study also has respondents and recall bias due to limited responses from survey respondents. Despite major limitations, NHANES data represent a diverse sample of the US population, covering populations of all ages, sex, race, and socioeconomic status from all geographic distributions.
6. Future Directions
We propose more studies to evaluate the short- and long-term effects of e-cigarette ingredients, including but not limited to acetaldehyde, acrolein, fine and ultrafine PMs, and BTEX on cardio and cerebrovascular systems. The use of e-cigarettes might be more harmful to the female and Hispanic population, so more awareness should be created among these sub-groups of the population. Future guidelines for the quantification of e-cigarettes in regards to cardio and cerebrovascular risk stratification may provide additional insight to mitigate the burden.
7. Conclusions
Stroke is more prevalent in traditional smokers than among e-cigarette users, but we found that the incidence of stroke was early in onset in e-cigarette smokers compared to traditional smokers. There were higher odds of stroke prevalence for those who smoked e-cigarettes in the last 30 days compared to non-e-cigarette smokers in the last 30 days. More prospective studies are needed to evaluate the long-term effects and safety of e-cigarettes to mitigate the risk of cardio and cerebrovascular disorders.
References
- G.A. Roth, G.A. Mensah, C.O. Johnson, G. Addolorato, E. Ammirati, L.M. Baddour, N.C. Barengo, A. Beaton, E.J. Benjamin, C.P. Benziger. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol., 2020. [DOI | PubMed]
- S.S. Virani, A. Alonso, E.J. Benjamin, M.S. Bittencourt, C.W. Callaway, A.P. Carson, A.M. Chamberlain, A.R. Chang, S. Cheng, F.N. Delling. Heart Disease and Stroke Statistics—2020 Update: A Report From the American Heart Association. Circulation, 2020. [DOI | PubMed]
- W.N. Kernan, B. Ovbiagele, H.R. Black, D.M. Bravata, M.I. Chimowitz, M.D. Ezekowitz, M.C. Fang, M. Fisher, K.L. Furie, D.V. Heck. Guidelines for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke, 2014. [DOI | PubMed]
- Cigarettes and Other Tobacco Products DrugFacts
- T. Parekh, S. Pemmasani, R. Desai. Risk of Stroke With E-Cigarette and Combustible Cigarette Use in Young Adults. Am. J. Prev. Med., 2020. [DOI | PubMed]
- Vaping What You Need to Know
- H. Yatsuya, A.R. Folsom. Risk of Incident Cardiovascular Disease among Users of Smokeless Tobacco in the Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Epidemiol., 2010. [DOI | PubMed]
- A.E. Sifat, B. Vaidya, M.A. Kaisar, L. Cucullo, T.J. Abbruscato. Nicotine and Electronic Cigarette (E-Cig) Exposure Decreases Brain Glucose Utilization in Ischemic Stroke. J. Neurochem., 2018. [DOI | PubMed]
- A. Bhatnagar, L.P. Whitsel, K.M. Ribisl, C. Bullen, F. Chaloupka, M.R. Piano, R.M. Robertson, T. McAuley, D. Goff, N. Benowitz. Electronic Cigarettes: A Policy Statement from the American Heart Association. Circulation, 2014. [DOI | PubMed]
- P.M. Ndunda, T.M. Muutu. Abstract 9: Electronic Cigarette Use Is Associated with a Higher Risk of Stroke. Stroke, 2019. [DOI]
- H. Qasim, Z.A. Karim, J.O. Rivera, F.T. Khasawneh, F.Z. Alshbool. Impact of Electronic Cigarettes on the Cardiovascular System. J. Am. Heart Assoc., 2017. [DOI | PubMed]
- 2018 NYTS Data: A Startling Rise in Youth E-Cigarette Use
- Euromonitor.com. Growth in Vapour Products
- A.S. Gentzke, M. Creamer, K.A. Cullen, B.K. Ambrose, G. Willis, A. Jamal, B.A. King. Vital Signs: Tobacco Product Use Among Middle and High School Students—United States, 2011–2018. MMWR. Morb. Mortal. Wkly. Rep., 2019. [DOI | PubMed]
- C. Bullen, C. Howe, M. Laugesen, H. McRobbie, V. Parag, J. Williman, N. Walker. Electronic Cigarettes for Smoking Cessation: A Randomised Controlled Trial. Lancet, 2013. [DOI | PubMed]
- P.T. Harrell, V.N. Simmons, J. Correa, T.A. Padhya, T.H. Brandon. Electronic Nicotine Delivery Systems (“e-Cigarettes”): Review of Safety and Smoking Cessation Efficacy. Otolaryngol. Head Neck Surg., 2014. [DOI | PubMed]
- K.E. Farsalinos, A. Spyrou, K. Tsimopoulou, C. Stefopoulos, G. Romagna, V. Voudris. Nicotine Absorption from Electronic Cigarette Use: Comparison between First and New-Generation Devices. Sci. Rep., 2014. [DOI | PubMed]
- C. Vardavas, F.T. Filippidis, I.T. Agaku. Determinants and Prevalence of E-Cigarette Use throughout the European Union: A Secondary Analysis of 26 566 Youth and Adults from 27 Countries. Tob. Control, 2015. [DOI | PubMed]
- S. Lee, R.A. Grana, S.A. Glantz. Electronic Cigarette Use among Korean Adolescents: A Cross-Sectional Study of Market Penetration, Dual Use, and Relationship to Quit Attempts and Former Smoking. J. Adolesc. Health, 2014. [DOI | PubMed]
- H.-W. Lee, S.-H. Park, M. Weng, H.-T. Wang, W.C. Huang, H. Lepor, X.-R. Wu, L.-C. Chen, M. Tang. E-Cigarette Smoke Damages DNA and Reduces Repair Activity in Mouse Lung, Heart, and Bladder as Well as in Human Lung and Bladder Cells. Proc. Natl. Acad. Sci. USA, 2018. [DOI | PubMed]
- C. Hutzler, M. Paschke, S. Kruschinski, F. Henkler, J. Hahn, A. Luch. Chemical Hazards Present in Liquids and Vapors of Electronic Cigarettes. Arch. Toxicol., 2014. [DOI | PubMed]
- M.L. Goniewicz, J. Knysak, M. Gawron, L. Kosmider, A. Sobczak, J. Kurek, A. Prokopowicz, M. Jablonska-Czapla, C. Rosik-Dulewska, C. Havel. Levels of Selected Carcinogens and Toxicants in Vapour from Electronic Cigarettes. Tob. Control, 2014. [DOI | PubMed]
- J. Palmisani, C. Abenavoli, M. Famele, A.D. Gilio, L. Palmieri, G.d. Gennaro, R. Draisci. Chemical Characterization of Electronic Cigarette (e-Cigs) Refill Liquids Prior to EU Tobacco Product Directive Adoption: Evaluation of BTEX Contamination by HS-SPME-GC-MS and Identification of Flavoring Additives by GC-MS-O. Atmosphere, 2020. [DOI]
- S. Bradford, S.M. Stamatovic, R.S. Dondeti, R. Keep, A.V. Andjelkovic. Nicotine Aggravates the Brain Postischemic Inflammatory Response. Am. J. Physiol. Heart Circ. Physiol., 2011. [DOI | PubMed]
- M.A. Kaisar, H. Villalba, S. Prasad, T. Liles, A.E. Sifat, R.K. Sajja, T.J. Abbruscato, L. Cucullo. Offsetting the Impact of Smoking and E-Cigarette Vaping on the Cerebrovascular System and Stroke Injury: Is Metformin a Viable Countermeasure?. Redox Biol., 2017. [DOI | PubMed]
- C.M. Perez, M.S. Hazari, A.D. Ledbetter, N. Haykal-Coates, A.P. Carll, W.E. Cascio, D.W. Winsett, D.L. Costa, A.K. Farraj. Acrolein Inhalation Alters Arterial Blood Gases and Triggers Carotid Body-Mediated Cardiovascular Responses in Hypertensive Rats. Inhal. Toxicol., 2015. [DOI | PubMed]
- M.S. Hazari, N. Haykal-Coates, D.W. Winsett, Q.T. Krantz, C. King, D.L. Costa, A.K. Farraj. TRPA1 and Sympathetic Activation Contribute to Increased Risk of Triggered Cardiac Arrhythmias in Hypertensive Rats Exposed to Diesel Exhaust. Environ. Health Perspect., 2011. [DOI | PubMed]
- L.A. Wheat, P. Haberzettl, J. Hellmann, S.P. Baba, M. Bertke, J. Lee, J. McCracken, T.E. O’Toole, A. Bhatnagar, D.J. Conklin. Acrolein Inhalation Prevents Vascular Endothelial Growth Factor-Induced Mobilization of Flk-1+/Sca-1+ Cells in Mice. Arterioscler. Thromb. Vasc. Biol., 2011. [DOI | PubMed]
- S.D. Sithu, S. Srivastava, M.A. Siddiqui, E. Vladykovskaya, D. Riggs, D.J. Conklin, P. Haberzettl, T.E. O’Toole, A. Bhatnagar, S.E. D’Souza. Exposure to Acrolein by Inhalation Causes Platelet Activation. Toxicol. Appl. Pharmacol., 2010. [DOI | PubMed]
- A. Peters, D.W. Dockery, J.E. Muller, M.A. Mittleman. Increased Particulate Air Pollution and the Triggering of Myocardial Infarction. Circulation, 2001. [DOI | PubMed]
- J. Sullivan, L. Sheppard, A. Schreuder, N. Ishikawa, D. Siscovick, J. Kaufman. Relation between Short-Term Fine-Particulate Matter Exposure and Onset of Myocardial Infarction. Epidemiology, 2005. [DOI | PubMed]
- T. Wang, G.D. Lang, L. Moreno-Vinasco, Y. Huang, S.N. Goonewardena, Y.J. Peng, E.C. Svensson, V. Natarajan, R.M. Lang, J.D. Linares. Particulate Matter Induces Cardiac Arrhythmias via Dysregulation of Carotid Body Sensitivity and Cardiac Sodium Channels. Am. J. Respir. Cell Mol. Biol., 2012. [DOI | PubMed]
- D.J. Conklin, O.A. Barski, J.-F. Lesgards, P. Juvan, T. Rezen, D. Rozman, R.A. Prough, E. Vladykovskaya, S. Liu, S. Srivastava. Acrolein Consumption Induces Systemic Dyslipidemia and Lipoprotein Modification. Toxicol. Appl. Pharmacol., 2009. [DOI | PubMed]
- S. Srivastava, S.D. Sithu, E. Vladykovskaya, P. Haberzettl, D.J. Hoetker, M.A. Siddiqui, D.J. Conklin, S.E. D’Souza, A. Bhatnagar. Oral exposure to acrolein exacerbates atherosclerosis in apoE-null mice. Atherosclerosis, 2011. [DOI | PubMed]
- M. Kuntic, M. Oelze, S. Steven, S. Kröller-Schön, P. Stamm, S. Kalinovic, K. Frenis, K. Vujacic-Mirski, M.T. Bayo Jimenez, M. Kvandova. Short-Term e-Cigarette Vapour Exposure Causes Vascular Oxidative Stress and Dysfunction: Evidence for a Close Connection to Brain Damage and a Key Role of the Phagocytic NADPH Oxidase (NOX-2). Eur. Heart J., 2020. [DOI | PubMed]
- A.R. Vansickel, T. Eissenberg. Electronic Cigarettes: Effective Nicotine Delivery After Acute Administration. Nicotine Tob. Res., 2013. [DOI | PubMed]
- M.A. Nides, S.J. Leischow, M. Bhatter, M. Simmons. Nicotine Blood Levels and Short-Term Smoking Reduction with an Electronic Nicotine Delivery System. Am. J. Health Behav., 2014. [DOI | PubMed]
- X.S. Yan, C. D’Ruiz. Effects of Using Electronic Cigarettes on Nicotine Delivery and Cardiovascular Function in Comparison with Regular Cigarettes. Regul. Toxicol. Pharmacol., 2015. [DOI | PubMed]
- C. Vlachopoulos, N. Ioakeimidis, M. Abdelrasoul, D. Terentes-Printzios, C. Georgakopoulos, P. Pietri, C. Stefanadis, D. Tousoulis. Electronic Cigarette Smoking Increases Aortic Stiffness and Blood Pressure in Young Smokers. J. Am. Coll. Cardiol., 2016. [DOI | PubMed]
- R. Carnevale, S. Sciarretta, F. Violi, C. Nocella, L. Loffredo, L. Perri, M. Peruzzi, A.G. Marullo, E. De Falco, I. Chimenti. Acute Impact of Tobacco vs Electronic Cigarette Smoking on Oxidative Stress and Vascular Function. Chest, 2016. [DOI | PubMed]
- L. Antoniewicz, J.A. Bosson, J. Kuhl, S.M. Abdel-Halim, A. Kiessling, F. Mobarrez, M. Lundbäck. Electronic Cigarettes Increase Endothelial Progenitor Cells in the Blood of Healthy Volunteers. Atherosclerosis, 2016. [DOI | PubMed]
- S. Hom, L. Chen, T. Wang, B. Ghebrehiwet, W. Yin, D.A. Rubenstein. Platelet Activation, Adhesion, Inflammation, and Aggregation Potential Are Altered in the Presence of Electronic Cigarette Extracts of Variable Nicotine Concentrations. Platelets, 2016. [DOI | PubMed]
- A. Caporale, M.C. Langham, W. Guo, A. Johncola, S. Chatterjee, F.W. Wehrli. Acute Effects of Electronic Cigarette Aerosol Inhalation on Vascular Function Detected at Quantitative MRI. Radiology, 2019. [DOI | PubMed]
- L. Antoniewicz, A. Brynedal, L. Hedman, M. Lundbäck, J.A. Bosson. Acute Effects of Electronic Cigarette Inhalation on the Vasculature and the Conducting Airways. Cardiovasc. Toxicol., 2019. [DOI | PubMed]
- G.F. Mitchell, S.-J. Hwang, R.S. Vasan, M.G. Larson, M.J. Pencina, N.M. Hamburg, J.A. Vita, D. Levy, E.J. Benjamin. Arterial Stiffness and Cardiovascular Events: The Framingham Heart Study. Circulation, 2010. [DOI | PubMed]
- C. Nocella, G. Biondi-Zoccai, S. Sciarretta, M. Peruzzi, F. Pagano, L. Loffredo, P. Pignatelli, C. Bullen, G. Frati, R. Carnevale. Impact of Tobacco Versus Electronic Cigarette Smoking on Platelet Function. Am. J. Cardiol., 2018. [DOI | PubMed]
- Z. Boas, P. Gupta, R.S. Moheimani, M. Bhetraratana, F. Yin, K.M. Peters, J. Gornbein, J.A. Araujo, J. Czernin, H.R. Middlekauff. Activation of the “Splenocardiac Axis” by Electronic and Tobacco Cigarettes in Otherwise Healthy Young Adults. Physiol. Rep., 2017. [DOI | PubMed]
- H. Qasim, Z.A. Karim, J.C. Silva-Espinoza, F.T. Khasawneh, J.O. Rivera, C.C. Ellis, S.L. Bauer, I.C. Almeida, F.Z. Alshbool. Short-Term E-Cigarette Exposure Increases the Risk of Thrombogenesis and Enhances Platelet Function in Mice. J. Am. Heart Assoc., 2018. [DOI | PubMed]
- T. Alzahrani, I. Pena, N. Temesgen, S.A. Glantz. Association between Electronic Cigarette Use and Myocardial Infarction. Am. J. Prev. Med., 2018. [DOI | PubMed]
- R.S. Moheimani, M. Bhetraratana, F. Yin, K.M. Peters, J. Gornbein, J.A. Araujo, H.R. Middlekauff. Increased Cardiac Sympathetic Activity and Oxidative Stress in Habitual Electronic Cigarette Users: Implications for Cardiovascular Risk. JAMA Cardiol., 2017. [DOI | PubMed]
- K.F. Franzen, J. Willig, S.C. Talavera, M. Meusel, F. Sayk, M. Reppel, K. Dalhoff, K. Mortensen, D. Droemann. E-Cigarettes and Cigarettes Worsen Peripheral and Central Hemodynamics as Well as Arterial Stiffness: A Randomized, Double-Blinded Pilot Study. Vasc. Med., 2018. [DOI | PubMed]
- C. Vlachopoulos, F. Kosmopoulou, D. Panagiotakos, N. Ioakeimidis, N. Alexopoulos, C. Pitsavos, C. Stefanadis. Smoking and Caffeine Have a Synergistic Detrimental Effect on Aortic Stiffness and Wave Reflections. J. Am. Coll. Cardiol., 2004. [DOI | PubMed]
- A. Besaratinia, S. Tommasi. Vaping: A Growing Global Health Concern. EClinicalMedicine, 2019. [DOI | PubMed]
- J. George, M. Hussain, T. Vadiveloo, S. Ireland, P. Hopkinson, A.D. Struthers, P.T. Donnan, F. Khan, C.C. Lang. Cardiovascular Effects of Switching from Tobacco Cigarettes to Electronic Cigarettes. J. Am. Coll. Cardiol., 2019. [DOI | PubMed]