
Perceptions regarding the use of cannabis in orthopaedics for treating musculoskeletal joint pain: A survey of arthritis patients
Abstract
There is renewed interest in investigating the analgesic properties of cannabis for musculoskeletal joint pain; however, available data remain limited. This cross-sectional study was designed with the objective of evaluating patients’ perceptions regarding the effect of cannabis on arthritis pain. Patients with arthritis pain presenting at one of three orthopedic clinics were asked to complete the study questionnaire. Outcomes were the perceived effect of cannabis on arthritic pain (measured using the continuous visual analog scale, with scores ranging from 0% to 100%) and association between preferences, attitudes, and barriers to the clinical use of cannabis for arthritic pain (evaluated using multivariable linear regression analyses). Sample size was also calculated using multivariable regression analysis. The study included 406 patients, including 105 (26.3%) who had already previously used cannabis for medical purposes and 63 (15.8%) who had used it during the past year. Approximately one-third of the patients who were prescribed opioids (78/256, 30.5%) had used them in the last week. On an average, patients stated that cannabis could treat 53.6% ± 2.6% of their pain (95% confidence interval = 51.1%–56.1%) and helped them replace 50.4% ± 3.2% of their analgesic medications (95% confidence interval = 47.2%–53.6%). Additionally, 88.8% of the patients (135/152) believed that cannabis would aid pain management. Individuals who had used cannabis for medical purposes (odds ratio = 7.2, 95% confidence interval = 1.6–12.8, p = 0.001) and patients reporting more severe baseline pain (β = 0.2 per point, 95% confidence interval = 0.1–0.3, p = 0.012) were more likely to report meaningful pain improvement. A quarter of the patients with arthritis already used cannabis, and many patients regarded cannabis as an effective pain treatment option. Patient preferences regarding administration and distribution, timing, and indications may help inform clinicians regarding the optimal utilization of cannabis in patients with joint and arthritis pain.
Article type: Research Article
Keywords: Cannabis, analgesics, orthopedic surgery, postoperative pain, pain management
Affiliations: Division of Orthopaedic Surgery, Department of Surgery, Queen’s University, Canada; Department of Health Research Methods, 3710Evidence and Impact, McMaster University, Canada; Division of Orthopaedic Surgery, McMaster University, Canada; Royal College of Surgeons Ireland, Ireland; Department of Medical Imaging, 3710McMaster University, Canada; University of Toronto Institute of Medical Science, Canada; Department of Surgery, University of Calgary, Canada
License: © The Author(s) 2026 CC BY 4.0 Creative Commons CC BY: This article is distributed under the terms of the Creative Commons Attribution 4.0 License (https://creativecommons.org/licenses/by/4.0/) which permits any use, reproduction and distribution of the work without further permission provided the original work is attributed as specified on the SAGE and Open Access pages (https://us.sagepub.com/en-us/nam/open-access-at-sage).
Article links: DOI: 10.1177/03000605261438343 | PubMed: 42093160 | PMC: PMC13161620
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (522 KB)
Introduction
Approximately 600 million people in the world have arthritis,1,2 with one in every four individuals reporting severe joint pain. It is among the top causes of overall disability and reduced quality-of-life,3,4 causing limitations in daily activities in approximately 24 million adults.1 Annual medical care costs and lost earnings due to arthritis are also estimated to be over US$300 billion.1
Pain control following surgery is crucial as postoperative pain can limit early mobilization.5,6 One of the main treatments for patients with severe symptomatic osteoarthritis (OA) and significant quality-of-life limitations is total joint arthroplasty (TJA).7 Opioids are among the most commonly used pain medications for postoperative pain control,8bibr9-03000605261438343–10 with almost 8% of all opioid prescriptions in the USA coming from orthopedics.11,12 Considering that 20% of opioid-related deaths involve prescription medications,13,14 opioid prescribing has undoubtedly contributed to the current opioid crisis, particularly in Canada, the USA, the UK, and Australia.15bibr16-03000605261438343bibr17-03000605261438343bibr18-03000605261438343–19 In the USA, >90 opioid-related deaths are reported every day, and in Canada, opioid-related hospitalizations and emergency department visits have risen by more than 50% over the last decade, with the highest rise in the past 3 years.20bibr21-03000605261438343–22
Postoperative opioid overprescription seems to be a problem unique to North America as patients in other parts of the world consume opioids less frequently and in lower doses.23bibr24-03000605261438343–25 The USA is responsible for the consumption of 80% of the global opioids supply.26 Opioid prescriptions showed a decline between 2012 and 2017; however, the number of days per prescription continued to rise.27,28 This indicates that orthopedic surgeons in Canada and the USA still regard opioids as the primary mode of postoperative pain control; therefore, exploring nonopioid analgesic alternatives will serve a critical role in curbing this problem.
Although previously cannabis was often regarded as a substance with no medical benefits and high abuse potential, over the past several years, perceptions regarding its utilization have undergone a significant transformation, allowing a more permissive approach. Cannabis modulates pain primarily through the endocannabinoid system (ECS) and activation of cannabinoid receptors (CB1 and CB2), which inhibits painful signals and reduce inflammation as well as through interactions with noncannabinoid targets, with studies supporting the analgesic properties of cannabis.29 A living systematic review examined data primarily from randomized controlled trials (RCTs) and evaluated the benefits and harms of cannabinoids (including cannabis-related products) in adults with chronic pain; this review reported reduction in pain severity, particularly in case of neuropathic pain, compared with placebo.30 However, there is lack of robust data on the use of cannabis for pain management in orthopedic surgery, highlighting the need for further investigation.26,31 Considering that cannabis use is completely legal in Canada, investigating its potential use for arthritic pain presents a distinct research opportunity.32
The goals of this survey were to examine patients’ perceptions regarding cannabis use for treating arthritis pain. Evaluation of the perceived effects of cannabis on joint and arthritis pain was the primary objective, while exploration of patients’ views and preferences surrounding cannabis use in the orthopedic setting was the secondary objective. We hypothesized that patients would perceive cannabis to be an effective option for managing arthritis-related pain.
Methods
This cross-sectional study used a survey-based approach to determine orthopedic clinic patients’ perceptions, preferences, and insights regarding cannabis use for musculoskeletal (MSK) joint pain. Patients who presented at three participating orthopedic clinics in Canada from 24 January 2018 to 7 March 2018 were screened for inclusion. Eligibility criteria included English-speaking patients aged >18 years presenting with arthritis or joint pain. Cognitively impaired patients or those who were too ill or injured to participate were excluded. Our center also conducted separate studies using similar methods, examining patients with traumatic injury or back pain and their experiences with cannabis.33,34 All the included patients provided informed consent before study enrollment. The relevant Research Ethics Board provided approval for the study. This was a level of evidence III study.
We used a modified version of a questionnaire used in previous studies, which was created using inputs from existing research studies, patients, and a group of specialists, including orthopedic surgeons, anesthesiologists, rehabilitation professionals, and epidemiologists.33,34 The questionnaire included 50 questions (multiple-choice or Likert-scale format)35 regarding the following: (a) patient and injury characteristics; (b) pain severity and analgesics usage; (c) perceptions and positions concerning the medical use of cannabis; (d) perceived effectiveness of cannabis use for arthritis and joint pain; and (e) barriers to appropriate clinical use. We assessed pain severity using the continual visual analog scale (VAS), with scores ranging from 0 (for no pain) to 100 (indicating unbearable pain). A continuous scale ranging from 0% to 100% was used to measure the perceived effectiveness of cannabis use by asking patients to rate the level of pain they believed was being (or could be) treated using cannabis; this served as the primary outcome of the study. Secondary outcomes included preferences, attitudes, and barriers to the clinical use of cannabis for joint pain. Additionally, we added four items from the Patient-Reported Outcomes Measurement Information System Short Form version 1.0 (PROMIS SF v1.0)–Anxiety 4a and seven items from the Short Screening Scale version of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) post-traumatic stress disorder (PTSD) test to screen for anxiety and PTSD.36,37
Patients at a participating site were approached consecutively by the research team who screened them for eligibility. Patients who consented to participate were assigned a participant identity (ID), and their anonymized data were entered into a study-specific electronic data capture system using an electronic tablet. Multivariable linear regression analysis was performed to determine associations between patients’ perceived effectiveness of cannabis as the dependent variable and patient and injury characteristics, previous surgery for the pain, pain frequency and severity, and past experience with cannabis as independent variables.
The multivariable regression analysis directed the calculation of the sample size. A significance level of 0.05 was used (conservative estimated effect size of 0.06, powered for 80% and eight predictors), estimating that a sample of 257 patients would provide adequate power to assess the relationship with perceived effectiveness. Therefore, the study aimed to recruit at least 367 patients (presuming 30% incomplete data). The patient recruitment intentionally exceeded the a priori analysis to ensure a well-powered study and enhance the reliability of the statistical analyses.
Results
Patient and injury characteristics
The study included 406 patients, with a mean age of 58 (range 20–91) years; 250 (61.6%) were women and 156 (38.4%) were men. Most patients were college-educated (167/404, 41.3%) and had an annual income between CAD 25,000 and 75,000 (205/383, 53.5%). The average reported pain severity score, measured using the VAS, was 55.0 ± 22.7 (52.8–5.72). The majority of patients had chronic pain (375/404; 92.8%), described as pain lasting >6 months; 84.2% of them had experienced pain within the last week (342/406), and 238 (58.8%) had undergone surgery for their injury. Details of patient demographics and injury characteristics are presented in Table 1.
Table 1.: Patient demographics and injury characteristics.
| Variables | Number of patients (%) |
|---|---|
| Total number of patients | 406 (100) |
| Age (N = 405), mean (range) | 58.0 (20–91) |
| Sex (N = 406) | |
| Female | 250 (61.6) |
| Male | 156 (38.4) |
| Educational level (N = 440) | |
| Less than high school | 18 (4.5%) |
| High school | 121 (30.0) |
| College/Trade school | 167 (41.3) |
| Undergraduate degree | 71 (17.6) |
| Graduate degree | 27 (6.7) |
| Income (N = 424) | |
| <CAD 25,000 | 80 (20.9) |
| CAD 25,000–49,999 | 111 (29.0) |
| CAD 50,000–74,999 | 94 (24.5) |
| CAD 74,999–99,999 | 53 (13.8) |
| >CAD 99,999 | 45 (11.7) |
| Anxiety (N = 157) | |
| Yes | 38 (24.2) |
| No | 119 (75.8) |
| PTSD (N = 155) | |
| Yes | 40 (25.8) |
| No | 155 (74.2) |
| Duration of symptoms (N = 404) | |
| <6 months (acute) | 29 (7.2) |
| ≥6 months (chronic) | 375 (92.8) |
| Underwent surgery for musculoskeletal injury (N = 405) | |
| No | 167 (41.2) |
| Yes | 238 (58.8) |
| Within the last month | 48 (20.2) |
| During the last 1–12 months | 75 (31.5) |
| >1 year ago | 108 (45.5) |
| Unspecified | 7 (2.9) |
| Experienced musculoskeletal pain in the past week (N = 406) | |
| Yes | 342 (84.2) |
| No | 58 (14.3) |
| Unsure | 6 (1.5) |
| Pain severity based on VAS scores (N = 401), mean (SD) | 55.0 (22.7) |
| No pain (VAS 0–9) | 21 (5.2) |
| Minimal pain (VAS 10–39) | 78 (19.5) |
| Moderate pain (VAS 40–69) | 189 (47.1) |
| Severe pain (VAS 70–99) | 113 (28.2) |
| Extreme pain (VAS 100) | 0 (0.0%) |
VAS: visual analog scale; PTSD: post-traumatic stress disorder.
Analgesics use
Nearly two-third of the patients were prescribed analgesics (256/406, 63.1%); 64.5% (165/256) of them were prescribed opioids and 30.5% (78/256) had used opioids during the last week. Most patients reported oxycodone/oxycontin (64/256, 25.0%) as the most common opioid medication they used and fentanyl as the least common (2/256, 0.8%) (Table 2). Among nonopioid prescription analgesics, naproxen was most commonly used (62/256, 24.2%). Additionally, 315 (78.0%) patients stated that they used nonprescription medications for their arthritis or joint pain, with acetaminophen (208/315, 66.0%) and ibuprofen (158/315, 50.2%) being the most common choices (Table 2). More than a quarter of the patients (105/400, 26.3%) disclosed that they had already used cannabis for medical purposes, and 35.8% (143/400) reported using cannabis recreationally. Additionally, 63 (15.8%) patients reported having used cannabis in the last 12 months specifically for pain control.
Table 2.: Analgesics use.
| Variable | Number of patients (%) | |
|---|---|---|
| Use of prescription analgesics for current MSK pain (N = 406) | ||
| Yes | 256 (63.1) | |
| No | 150 (36.9) | |
| Prescription medications | Prescribed for MSK pain (N = 256) | Used during the past week |
| Opioids | 165 (64.5) | 78 (30.5) |
| Oxycodone/Oxycontin | 64 (38.8) | 25 (15.2) |
| Codeine | 60 (36.4) | 30 (18.2) |
| Hydromorphone | 56 (33.9) | 24 (14.5) |
| Morphine (oral) | 16 (9.7) | 6 (3.6) |
| Fentanyl (oral/patch) | 2 (1.2) | 0 (0.0) |
| NSAIDs | 130 (50.8) | 62 (24.2) |
| Naproxen | 62 (47.7) | 25 (19.2) |
| Celecoxib | 38 (29.2) | 17 (13.1) |
| Diclofenac (topical) | 16 (12.3) | 10 (7.7) |
| Toradol | 16 (12.3) | 3 (2.3) |
| Meloxicam | 14 (10.8) | 7 (5.4) |
| Diclofenac (oral) | 13 (10.0) | 4 (3.1) |
| Gabapentin/Pregabalin | 17 (6.6) | 7 (2.7) |
| Use of nonprescription/OTC analgesics for current MSK pain (N = 404) | ||
| Yes | 315 (78.0) | |
| No | 89 (22.0) | |
| Nonprescription/over-the-counter medications | Used for MSK pain (N = 315) | Used in the past week (N = 315) |
| NSAIDs | ||
| Ibuprofen | 158 (50.2) | 69 (21.9) |
| Naproxen | 100 (31.7) | 40 (12.7) |
| Diclofenac (topical) | 37 (11.7) | 12 (3.8) |
| Acetylsalicylic acid | 18 (5.7) | 7 (2.2) |
| Other | ||
| Acetaminophen | 208 (66.0) | 119 (37.8) |
| Miscellaneousb | 13 (4.1) | 10 (3.2) |
| Used cannabis, or know someone who has | Medically (N = 400) | Recreationally (N = 400) |
| No | 155 (61.3) | 120 (70.0) |
| Yes, | 245 (38.8) | 280 (30.0) |
| Used | 70 (17.5) | 68 (17.0) |
| Used and know someone | 35 (8.75) | 75 (18.6) |
| Know someone | 140 (35.0) | 137 (34.6) |
| Used cannabis in the past 12 months to control pain (N = 399) | ||
| No | 336 (84.2) | |
| Yes | 63 (15.8) | |
N: number; No: number; MSK: musculoskeletal; OTC: over-the-counter; NSAIDs: nonsteroidal anti-inflammatory drugs.
a Where data were missing or a study participant did not respond to a query, percentages were calculated considering the total number of responses, not the total number of study participants.
b Muscle relaxants, balms/rubs/cream, herbal medications (e.g. arnica and turmeric).
Perceived effects of cannabis on MSK pain
Overall, patients believed that cannabis was, or could be, used to treat over 50% of their pain (average reduction in VAS pain score = 53.6 ± 2.6, 95% (confidence interval) CI = 51.1%–56.1%) and replace nearly half of their analgesic medications (50.4 ± 3.2, 95% CI = 47.2%–53.6%) (Table 3). Most patients felt comfortable discussing cannabis use with their physicians (77.1 ± 2.7, 95% CI = 74.4–79.8). Our regression analysis showed that several factors were associated with greater reported pain relief with cannabis use. Individuals who had used cannabis for medical purposes (OR = 7.2, 95% CI = 1.6–12.8, p = 0.001) and individuals reporting more severe baseline pain (β = 0.2 per point, 95% CI = 0.1–0.3, p = 0.012) were more likely to report meaningful pain improvement (Table 4).
Table 3.: Perceptions regarding cannabis use following MSK injury.
| Variable (number of patients) | Mean value (95% CI) |
|---|---|
| Perceived pain relief/resolution with cannabis use (0% = none, 100% = all) (N = 382) | 53.6 (51.1–56.1) |
| Percentage of their pain medication regimen is made up by cannabis (0% = none, 100% = all) (N = 63) | 38.8 (30.4–47.2) |
| Percentage of analgesic medications that cannabis does/could replace (0% = none, 100% = all) (N = 319) | 50.4 (47.2–53.6) |
| Comfort in discussing cannabis use with provider (0% = not comfortable at all, 100% = completely comfortable) (N = 387) | 77.1 (74.4–79.8) |
MSK: musculoskeletal; CI: confidence interval.
Table 4.: Multivariable regression model for patients’ perception of their pain treated by cannabis.
| Covariate | OR/ß coefficient | 95% CI | p-value |
|---|---|---|---|
| Age | −0.5 | −0.3 to 0.1 | 0.341 |
| Sex | |||
| Male | 0.6 | −4.7 to 5.9 | 0.824 |
| Female | − | − | − |
| Duration of pain/symptoms | |||
| ≥6 months (chronic) | 3.5 | −6.6 to 13.6 | 0.492 |
| <6 months (acute) | − | − | − |
| Had surgery | −3.3 | −8.6 to 2.0 | 0.227 |
| Pain severity (VAS) | 0.2 | 0.1 to 0.3 | 0.001 |
| Used cannabis to manage pain in last year | 7.2 | 1.6 to 12.8 | 0.012 |
p-value <0.05
VAS: visual analog scale; OR: odds ratio; CI: confidence interval.
Statistics are based on cases with no missing values for any variable used (N = 375).
Knowledge, attitudes, and preferences regarding cannabis
Only 15.6% of patients (61/391) reported discussing cannabis use with their physicians (Table 5). The number one reason identified by patients for not discussing cannabis as a treatment choice was that they never considered using cannabis for medical purposes (172/330, 52.1%). Concerns about the adverse effects of cannabis and addiction were expressed by 16.4% (54/330) and 11.5% (38/330) of patients, respectively. When asked how they would prefer to obtain cannabis, private dispensaries (26/406, 6.4%) were the first choice, while pharmacies ranked second (23/406, 5.7%). Patients expressed more interest in oral formulations (pills (179/406, 44.1%) and edibles (99/406, 24.4%)) and topical creams (101/406, 24.9%). Inhaled formulations, such as that which could be smoked (69/406, 17.0%) and vaporized preparations (46/406, 11.3%), were less commonly preferred. Regarding the legalization of the recreational use of cannabis in Canada, half of the patients (194/382, 50.8%) either somewhat or strongly supported the legislation.
Table 5.: Barriers and considerations for clinical use and further investigation.
| Variable | Number of patients (%) |
|---|---|
| Have discussed medical use of cannabis with physician (N = 391) | |
| No | 330 (84.4) |
| Yes | 61 (15.6) |
| I never thought about using cannabis for medical purposesa | 172 (52.1) |
| I don’t need any more medications for pain controla | 62 (18.8) |
| I am concerned about adverse effectsa | 54 (16.4) |
| I am concerned about addiction with cannabisa | 38 (11.5) |
| I do not know how to access cannabisa | 26 (7.9) |
| I have a moral or religious objection to using cannabisa | 25 (7.6) |
| I can easily obtain cannabis through other physicians/sourcesa | 18 (5.5) |
| I don’t think it worksa | 17 (5.2) |
| My physician doesn’t think it worksa | 15 (4.5) |
| I prefer to use cannabis without discussing it with my physiciana | 4 (1.2) |
| Othera | 39 (11.8) |
| Was the discussion a positive experience (N = 61) | |
| Very positive | 24 (39.3) |
| Positive | 14 (23.0) |
| Mixed | 17 (27.9) |
| Somewhat negative | 3 (4.9) |
| Very negative | 3 (4.9) |
| Where patients obtained/preferred to obtain cannabis from | Preferred (N = 406) |
| Government | 40 (9.9) |
| Private dispensary | 26 (6.4) |
| Pharmacy | 23 (5.7) |
| Online | 23 (5.7) |
| Home grown | 19 (4.7) |
| Forms of cannabis patients preferred to use to treat their pain (N = 406) | |
| Oral pill/tablet | 179 (44.1) |
| Topical | 101 (24.9) |
| Edible | 99 (24.4) |
| Sublingual | 75 (18.5) |
| Inhaled smoke | 69 (17.0) |
| Inhaled vapor | 46 (11.3) |
| Liquid | 40 (9.9) |
| Transdermal | 38 (9.4) |
| Intra-articular | 17 (4.2) |
| Willingness to participate in a randomized clinical trial comparing cannabis to usual care for pain relief following an MSK injury (N = 381) | |
| Yes | 208 (54.6) |
| No | 80 (21.0) |
| Unsure | 93 (24.4) |
MSK: musculoskeletal.
a Denominator is 330 as 330 patients did not discuss cannabis with their providers.
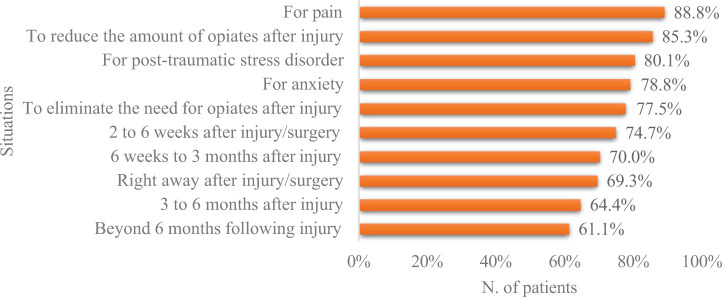
Patients identified the initial 3-month period after surgery/injury as the most appropriate period to use cannabis. However, the majority thought that using cannabis at multiple time points could also be beneficial (from immediately after the surgery/injury to beyond 6 months). Furthermore, patients also believed that cannabis may be useful for treating pain (135/152, 88.8%), reducing (128/150, 85.3%) or eliminating the need for opioids (117/151, 77.5%), and treating symptoms of PTSD (121/151, 80.1%) and anxiety (119/151, 78.8%) (Figure 1). More than half of the patients (208/381, 54.6%) expressed their willingness to participate in a randomized clinical trial comparing cannabis to standard treatments for MSK pain (Table 5).
Discussion
In this study, we investigated the perceptions and views of 406 arthritis patients attending orthopedic and rehabilitation clinics regarding the effectiveness of cannabis use in alleviating joint or arthritis pain. The patients in our study believed that cannabis could relieve 53.6% of their pain and replace at least half (50.4%) of their current pain medications. Furthermore, 26.3% of patients already used cannabis for medical purposes, and 15.8% had used cannabis during the last year, specifically for their joint pain. The other studies conducted at our center examining cannabis perceptions involving patients with a traumatic injury or back pain also support these findings.33,34 Studies on chronic and postoperative pain have shown that cannabis and cannabinoid products offer modest but measurable reductions in pain and may exert opioid-sparing effects. This aligns with the perceptions of the patients in the present study.38bibr39-03000605261438343–40
Moreover, our study revealed that 64.5% of pain prescriptions were for opioids, with oxycodone or oxycontin being the most frequently prescribed medications (25.0%). This aligns with findings from other studies, which suggest that, despite efforts to curb opioid prescriptions, opioids remain a common choice for managing chronic MSK pain, including arthritis.41bibr42-03000605261438343bibr43-03000605261438343–44 Eighty percent of respondents in the study believed that cannabis might lower their reliance on opioids or eliminate the need altogether. This is consistent with results from other studies, according to which, patients who use cannabis for medical reasons reported better pain relief and reported reduced reliance on opioids.45,46 In one study, 95% of patients who used cannabis for medical purposes reported improved pain control, and 87% reported using fewer analgesics, including opioids.47 Additionally, qualitative research has shown that for individuals with MSK pain (21% arthritis), cannabis is preferred over opioids and considered as the medium for reducing opioid consumption.48 These findings strongly suggest that cannabis play an important role in managing MSK joint pain.
With respect to our secondary goals, the most preferred methods of distribution and administration were private dispensaries and oral cannabis formulations, respectively. Although some patients expressed concerns about potential adverse effects and addiction, the primary reason for not discussing cannabis use with their healthcare providers was that they did not consider it as a treatment option for managing their pain. This could be owing to the limited existing literature on the use of cannabis for joint or arthritis-related pain. However, this gap in research highlights the need for high-quality studies, such as RCTs, comparing cannabis to standard pain management treatments for conditions such as arthritis. Currently, cannabis are approved for use in medical conditions such as neuropathic pain, palliative care, chemotherapy-induced nausea, and spasticity associated with multiple sclerosis or spinal cord injury.49 Our study indicates that patients are eager to participate in such trials, with over half (54.6%) of our participants expressing an interest in being randomized to either the cannabis or traditional pain management groups in a clinical trial.
Recall bias was a limitation of this study, considering that a survey was used for data collection. Additionally, because cannabis use has historically been associated with negative perceptions, such as concerns over addiction and its legality, concerns regarding social desirability may have also influenced the results. Nevertheless, the high response rate, focus on recent cannabis usage, and the fact that only 7% of participants cited moral or religious objections to cannabis use suggest that these issues had minimal impact on the findings. Moreover, we worked closely with a multidisciplinary team of experts and patients to develop the survey, ensuring that it was designed to meet the study’s objectives. As the study was conducted exclusively in Canada, the generalizability of the findings and methodology to other jurisdictions could be limited. Nevertheless, the timing of the study coincided with a major regulatory moment for cannabis in Canada when its recreational use was legalized, allowing a unique research opportunity. However, it is noteworthy that the dataset were generated in 2018, and perceptions and usage patterns may have changed since then.
With a focus on orthopedic surgery, based on these findings, orthopedic surgeons should proactively address cannabis use and perceptions as part of routine arthritis care. With one section of patients already using cannabis for medical purposes and some viewing it as a potential analgesic, informed discussions may support safer, multimodal pain management strategies. Additionally, educating orthopedic surgeons on appropriate formulations, administration routes, and adverse effects may improve clinical oversight and patient safety and present an opportunity for orthopedic practices to contribute to high-quality research aimed at defining the role of cannabis in evidence-based arthritis management.
Conclusions
Cannabis use among patients with arthritis and MSK joint pain is highly prevalent, and patients are generally open to discussing it with their healthcare providers. Many patients believe that cannabis is an effective pain management option, particularly during the postoperative recovery phase. Participants also believed that cannabis could address at least 50% of their pain and potentially reduce their reliance on opioids. Data on patient preferences, including preferred methods of administration, distribution, and perceived barriers, can help clinicians and researchers better understand the future use of cannabis for pain management. More research, particularly through RCTs, is essential to assess the safety and efficacy of cannabis use before it can be officially endorsed as a treatment option for this patient group.
References
- Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: a systematic analysis for the global burden of disease study 2021.. Lancet Rheumatol, 2023. [PubMed]
- Z Wang, Z Xiao, C Sun. Global, regional and national burden of osteoarthritis in 1990–2021: a systematic analysis of the global burden of disease study 2021.. BMC Musculoskelet Disord, 2024. [PubMed]
- TE McAlindon, C Cooper, JR Kirwan. Determinants of disability in osteoarthritis of the knee.. Ann Rheum Dis, 1993. [PubMed]
- KL Dominick, FM Ahern, CH Gold. Health-related quality of life and health service use among older adults with osteoarthritis.. Arthritis Rheum, 2004. [PubMed]
- RB Brokelman, CJ Van Loon, WJ. Rijnberg. Patient versus surgeon satisfaction after total hip arthroplasty.. J Bone Joint Surg Br, 2003. [PubMed]
- NA Trasolini, BM McKnight, LD. Dorr. The opioid crisis and the orthopedic surgeon.. J Arthroplasty, 2018. [PubMed]
- LA. Mandl. Determining who should be referred for total hip and knee replacements.. Nat Rev Rheumatol, 2013. [PubMed]
- CC Jørgensen, M Petersen, H Kehlet. Analgesic consumption trajectories in 8975 patients 1 year after fast-track total hip or knee arthroplasty.. Eur J Pain. Epub ahead of print 20 April, 2018
- T Blågestad, IH Nordhus, J Grønli. Prescription trajectories and effect of total hip arthroplasty on the use of analgesics, hypnotics, antidepressants, and anxiolytics: results from a population of total hip arthroplasty patients.. Pain, 2016. [PubMed]
- TJ Rajamäki, PA Puolakka, A Hietaharju. Use of prescription analgesic drugs before and after hip or knee replacement in patients with osteoarthritis.. BMC Musculoskelet Disord, 2019. [PubMed]
- BJ Morris, HR. Mir. The opioid epidemic: impact on orthopaedic surgery.. J Am Acad Orthop Surg, 2015. [PubMed]
- LD Delaney, DJ Clauw, JF. Waljee. The management of acute pain for musculoskeletal conditions: the challenges of opioids and opportunities for the future.. J Bone Joint Surg Am, 2020
- J. Katz. 2017
- 14National Institute on Drug Abuse. Drug Overdose Deaths: Facts and Figures, https://www.drugabuse.gov/drug-topics/trends-statistics/overdose-death-rates (2024, accessed 28 March 2026).
- MC Bicket, JJ Long, PJ Pronovost. Prescription opioid analgesics commonly unused after surgery: a systematic review.. JAMA Surg, 2017. [PubMed]
- S Berterame, J Erthal, J Thomas. Use of and barriers to access to opioid analgesics: a worldwide, regional, and national study.. Lancet, 2016. [PubMed]
- S. Okie. A flood of opioids, a rising tide of deaths.. N Engl J Med, 2010. [PubMed]
- B Fischer, E. Argento. Prescription opioid related misuse, harms, diversion and interventions in Canada: a review.. Pain Physician, 2012. [PubMed]
- B Larance, L Degenhardt, A Peacock. Pharmaceutical opioid use and harm in Australia: the need for proactive and preventative responses.. Drug Alcohol Rev, 2018. [PubMed]
- 20Public Health Agency of Canada. Opioid- and Stimulant-related Harms in Canada, https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/#fn2-0-rf (2026, accessed 28 March 2026).
- RA Rudd, P Seth, F David. Increases in drug and opioid-involved overdose deaths-United States, 2010–2015.. MMWR Morb Mortal Wkly Rep, 2016. [PubMed]
- JK Phillips, MA Ford, RJ Bonnie. Pain management and the opioid epidemic: balancing societal and individual benefits and risks of prescription opioid use., 2017
- KS Ladha, MD Neuman, G Broms. Opioid prescribing after surgery in the United States, Canada, and Sweden.. JAMA Netw Open, 2019. [PubMed]
- GT Helmerhorst, AL Lindenhovius, M Vrahas. Satisfaction with pain relief after operative treatment of an ankle fracture.. Injury, 2012. [PubMed]
- A Schuchat, D Houry, GP. Guy. New data on opioid use and prescribing in the United States.. JAMA, 2017. [PubMed]
- LT Kleeman-Forsthuber, DA Dennis, JM. Jennings. Medicinal cannabis in orthopaedic practice.. J Am Acad Orthop Surg, 2020. [PubMed]
- GP Guy, K Zhang, MK Bohm. Vital signs: changes in opioid prescribing in the United States, 2006–2015.. MMWR Morb Mortal Wkly Rep, 2017. [PubMed]
- 28Centers for Disease Control and prevention (CDC). 2018 Annual Surveillance Report of Drug-Related Risks and Outcomes, https://www.cdc.gov/overdose-prevention/media/pdfs/pubs/2018-cdc-drug-surveillance-report.pdf (2018, accessed 28 March 2026).
- G Donvito, SR Nass, JL Wilkerson. The endogenous cannabinoid system: a budding source of targets for treating inflammatory and neuropathic pain.. Neuropsychopharmacology, 2018. [PubMed]
- R Chou, AY Ahmed, T Dana. 2024
- K Madden, N Van der Hoek, S Chona. Cannabinoids in the management of musculoskeletal pain: a critical review of the evidence.. JBJS Rev, 2018
- 32Canada Minister of Justice. Cannabis Act/Loi sur Cannabis, https://laws-lois.justice.gc.ca/eng/acts/c-24.5/ (2018, accessed 31 March 2026).
- M Gjorgjievski, K Madden, C Bullen. Perceptions in orthopedic surgery on the use of cannabis in treating pain: a survey of musculoskeletal trauma patients-results from the Canadian POSIT study.. J Orthop Trauma, 2024. [PubMed]
- M Gjorgjievski, K Madden, C Bullen. Perceptions in orthopedic surgery on the use of cannabis in treating pain: a survey of patients with spine pain (POSIT Spine).. J Orthop Surg Res, 2024. [PubMed]
- LE Griffith, DJ Cook, GH Guyatt. Comparison of open and closed questionnaire formats in obtaining demographic information from Canadian general internists.. J Clin Epidemiol, 1999. [PubMed]
- N Breslau, EL Peterson, RC Kessler. Short screening scale for DSM-IV posttraumatic stress disorder.. Am J Psychiatry, 1999. [PubMed]
- PA Pilkonis, SW Choi, SP Reise. Item banks for measuring emotional distress from the Patient-Reported Outcomes Measurement Information System (PROMIS®): depression, anxiety, and anger.. Assessment, 2011. [PubMed]
- K Tran, K Odland, DWJ. Polly. Cannabis and cannabidiol for postoperative pain management in orthopedic surgery: a scoping review.. Pain Med, 2026. [PubMed]
- M Karst, W Meissner, S Sator. Full-spectrum extract from Cannabis sativa DKJ127 for chronic low back pain: a phase 3 randomized placebo-controlled trial.. Nat Med, 2025. [PubMed]
- DE Slawek, C Zhang, S Dahmer. Medical cannabis and opioid receipt among adults with chronic pain.. JAMA Intern Med, 2026. [PubMed]
- JW Busse, S Craigie, DN Juurlink. Guideline for opioid therapy and chronic noncancer pain.. CMAJ, 2017. [PubMed]
- 42Choosing Wisely Canada. Opioid Wisely, https://choosingwiselycanada.org/campaign/opioid-wisely/ (accessed 28 March 2026).
- J Bruneau, K Ahamad, MÈ Goyer. Management of opioid use disorders: a national clinical practice guideline.. CMAJ, 2018. [PubMed]
- CM Brummett, JF Waljee, J Goesling. New persistent opioid use after minor and major surgical procedures in US adults.. JAMA Surg, 2017. [PubMed]
- D Harris, RT Jones, R Shank. Self-reported marijuana effects and characteristics of 100 San Francisco medical marijuana club members.. J Addict Dis, 2000. [PubMed]
- T Nguyen, Y Li, D Greene. Changes in prescribed opioid dosages among patients receiving medical cannabis for chronic pain, New York State, 2017–2019.. JAMA Netw Open, 2023. [PubMed]
- JS Luque, AN Okere, CA Reyes-Ortiz. Mixed methods study of the potential therapeutic benefits from medical cannabis for patients in Florida.. Complement Ther Med, 2021. [PubMed]
- DC. Peters. Patients and caregivers report using medical marijuana to decrease prescription narcotics use.. Humboldt J Soc Relat, 2013
- GM Allan, J Ramji, D Perry. Simplified guideline for prescribing medical cannabinoids in primary care.. Can Fam Physician, 2018. [PubMed]