
Does Cannabinoid Use Reduce Opioid Utilization Among Patients with Gastrointestinal Cancer? Evidence from Epic COSMOS
Abstract
Patients with gastrointestinal (GI) cancers receiving chemotherapy often experience difficult symptoms such as pain, nausea, reduced appetite, and fatigue. As cannabis use has expanded across the United States, many have questioned whether it could help to manage these symptoms while also reducing reliance on opioid medications, which carry risks of dependence and overdose. Despite increasing interest, it remains unclear whether cannabis use leads to lower opioid use in cancer care. This study examined real-world prescribing patterns of cannabinoids and opioids in a large national database of patients starting chemotherapy. We aimed to understand which patients receive cannabis, how prescribing varies by region or patient characteristics, and whether cannabis use is associated with reduced opioid use early in treatment. Our findings show that cannabis prescribing remains relatively uncommon and was not linked to lower opioid use. These results underscore the need for additional research to guide safe, effective, and equitable symptom management for people undergoing cancer treatment.
Article type: Research Article
Keywords: cannabis, cannabinoids, opioids, GI cancer, chemotherapy, COSMOS
License: © 2026 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Article links: DOI: 10.3390/cancers18071110 | PubMed: 41976333 | PMC: PMC13072402
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (715 KB)
1. Introduction
Over the past two decades, cannabis use in the United States has increased substantially, driven by state-level medical and recreational legalization and growing public acceptance [ref. 1,ref. 2,ref. 3,ref. 4]. As of 31 December 2025, medicinal cannabis is permitted in 47 states and Washington, DC, and recreational use is legal in 24 states [ref. 5]. Concurrently, cannabis is increasingly considered for symptom management (pain, nausea, vomiting, appetite loss, sleep disturbances and anxiety) [ref. 6,ref. 7]. Of note, federal deliberations in late 2025 regarding potential rescheduling from Schedule I to Schedule III further reflect the evolving recognition of possible medical utility [ref. 8]. Cannabis has also gained traction in public and clinical discourse as a potential adjunct or alternative to opioids for symptom control [ref. 9,ref. 10].
Despite these trends, opioid-related harm remains substantial [ref. 11,ref. 12]. In 2022, approximately 110,900 opioid overdose deaths were reported nationally, with synthetic opioids (e.g., fentanyl) accounting for the majority [ref. 8,ref. 9]. Whether cannabis meaningfully reduces opioid utilization, or opioid-related harms, among medically complex populations such as patients undergoing chemotherapy remains an unresolved question at the intersection of clinical care, public health policy, and drug regulation. This uncertainty underscores the need to evaluate the broader implications of medical cannabis for clinical practice, public health, and policy and regulation.
Evidence on the medical benefits of cannabis is mixed. Randomized trials and observational studies generally demonstrate modest, often clinically marginal effects across many indications [ref. 13,ref. 14,ref. 15]. Meta-analyses related to chronic pain and sleep have noted small, short-term improvements, with higher rates of nonserious adverse events such as dizziness and somnolence [ref. 15]. One Cochrane review reported that there was no consistent superiority of THC-dominant, CBD-dominant, or balanced formulations over a placebo for neuropathic pain [ref. 14]. Evidence for an opioid-sparing effect is also limited, with randomized trials demonstrating little benefit and observational estimates being inconsistent with low certainty [ref. 16]. In oncology, cannabinoids demonstrate a modest benefit for refractory chemotherapy-induced nausea and vomiting, although tolerability constrains routine use; evidence is strongest (yet heterogeneous) for spasticity in multiple sclerosis [ref. 4,ref. 17,ref. 18].
Patients with GI cancers undergoing chemotherapy often require multimodal treatment for pain, nausea, and fatigue [ref. 19]. Despite increasing cannabis availability, the prevalence of cannabis use in this population and its association with opioid utilization after chemotherapy initiation remain poorly characterized. We therefore characterized patterns of cannabis prescribing patterns at chemotherapy initiation and its association with short-term opioid utilization among patients with GI cancers, using multisite electronic health record (EHR) data.
2. Methods
2.1. Study Design, Study Population, and Data Sources
Patients with GI (colon, biliary, liver, pancreas, and rectum) cancer diagnosed between 1 January 2016 and 30 September 2025 were identified from the Epic COSMOS database [ref. 20]. COSMOS is a nationwide, multisite electronic health record (EHR) research network that aggregates de-identified patient-level data from participating Epic health systems across the United States, capturing longitudinal demographics, diagnoses, medications, procedures, and geographic characteristics to support real-world evidence generation [ref. 20]. GI cancers were defined using the International Classification of Diseases (ICD-9/10) codes and include esophagus, stomach, small intestine, colon, rectum, liver, gallbladder, biliary tract, and pancreas [ref. 21,ref. 22].
The index date was the date of chemotherapy initiation. To capture new exposure, patients with any documented cannabis (cannabinoid) or opioid prescriptions from 1 year to 15 days before the index date were excluded. Patients who died within 90 days of the index date or had incomplete medication records during follow-up were also excluded. The Ohio State University Institutional Review Board approved the study and waived informed consent because COSMOS provides de-identified, limited datasets for research.
2.2. Exposure
“Cannabis use” was defined as receipt of an FDA-approved cannabinoid (dronabinol, nabilone, or cannabidiol) documented on EHR medication lists or prescription fills totaling >2 days within 90 days after the index date. Exposure was binary (yes/no). Cannabis obtained via dispensaries or recreational markets is not captured in COSMOS and was therefore not included in the exposure definition.
2.3. Covariates
Patient-level factors included age, sex, race/ethnicity (White, Black, Hispanic, or Other [i.e., Asian, American Indian, and Alaska Native]), cancer type, U.S. Census region (Midwest, Northeast, South, West), rural versus metropolitan residence, marital status, and index year. Clinical factors included GI cancer site, treatment phase (active chemotherapy vs. postoperative), and Charlson Comorbidity Index (CCI), categorized as low (≤2) or high (>2) [ref. 23]. The social vulnerability index (SVI), a county-level composite measure of socioeconomic vulnerability linked by patient residence, was categorized as low, medium, or high, based on national tertiles [ref. 24]. The cannabis and opioid measures were derived from EHR medication lists and prescription fills within prespecified windows.
2.4. Outcome of Interest and Measures
The primary outcome was receipt of any opioid prescription during the same 90-day post-chemotherapy period. Among opioid recipients, cumulative opioid exposure was quantified as the total number of prescription days supplied during the follow-up period. Secondary outcomes included (1) opioid discontinuation (cessation of opioid prescriptions within 90 days after cannabis initiation) and (2) ≥50% reduction in the mean daily dose compared with the baseline. Temporal trends in cannabis prescribing were examined by calendar year, and geographic variation was described at the state level (Supplementary Table S2). Counts <11 were censored per COSMOS reporting.
2.5. Statistical Analysis
Continuous variables are reported as medians with interquartile ranges (IQRs), and categorical variables are reported as frequencies and percentages. Baseline differences between cannabinoid recipients and nonrecipients were assessed using the Kruskal–Wallis test for continuous variables and chi-square or Fisher’s exact tests for categorical variables. Within-person pre–post comparisons were evaluated using paired t tests or Wilcoxon signed-rank tests.
Multivariable logistic regression examined factors associated with early cannabis prescribing. Model 1 adjusted for patient-level and clinical covariates (age, sex, race/ethnicity, CCI, cancer type, index year). Model 2 additionally adjusted for region. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were reported. Temporal trends were evaluated using index-year indicators (reference = 2017).
3. Results
3.1. Baseline Characteristics of Patients in the Cohort
Among 144,981 adults with a GI cancer, colon: n = 49,285, 34.0%; rectum: n = 35,094, 24.2%; pancreas: n = 34,280, 23.6%; liver: n = 23,643, 16.3%; and biliary: n = 2679, 1.8%. Most individuals were male (n = 83,534, 57.6%) and White (n = 100,262, 78.7%); the median age was 69 years (IQR, 60–77). The majority resided in metropolitan areas (n = 115,033, 80.6%), with the largest proportions living in the South (n = 53,960; 37.8%) and Midwest (n = 35,406, 24.8%). Within 90 days of chemotherapy initiation, 3390 patients (2.4%) received an FDA-approved cannabinoid prescription of >2 days; 141,591 (97.6%) individuals did not. During the same period, 46,141 (31.8%) patients received ≥1 opioid prescriptions (Table 1).
Table 1: Baseline characteristics of patients.
| Characteristics | Total (n = 144,981) | No Cannabis Prescription (n = 141,591; 97.6%) | Cannabis Prescription ≥2 Days (n = 3390; 2.4%) | p-Value |
|---|---|---|---|---|
| Age in years | 69 (60, 77) | 69 (60, 77) | 70 (62, 77) | <0.001 |
| Sex | <0.001 | |||
| Male | 83,534 (57.6%) | 81,714 (57.7%) | 1820 (53.7%) | |
| CCI | <0.001 | |||
| >2 | 141,162 (97.4%) | 137,898 (97.4%) | 3264 (96.3%) | |
| Race | <0.001 | |||
| White | 100,262 (78.7%) | 98,128 (78.8%) | 2134 (75.1%) | |
| Black | 15,368 (12.1%) | 14,878 (11.9%) | 490 (17.2%) | |
| Hispanic | 6160 (4.8%) | 6037 (4.8%) | 123 (4.3%) | |
| Other | 5647 (4.4%) | 5551 (4.5%) | 96 (3.4%) | |
| Missing | 17,544 (12.1%) | 16,997 (12%) | 547(16.1%) | |
| Region | <0.001 | |||
| Midwest | 35,406 (24.8%) | 34,689 (24.9%) | 717 (21.4%) | |
| Northeast | 29,843 (20.9%) | 29,181 (20.9%) | 662 (19.7%) | |
| South | 53,960 (37.8%) | 52,320 (37.5%) | 1640 (48.9%) | |
| West | 23,693 (16.6%) | 23,358 (16.7%) | 335 (10.0%) | |
| Missing | 2079(1.4%) | 2043(1.44%) | 36(1%) | |
| Area | 0.018 | |||
| Urban | 115,033 (80.6%) | 112,279 (80.6%) | 2754 (82.2%) | |
| Rural | 27,676 (19.4%) | 27,080 (19.4%) | 596 (17.8%) | |
| Missing | 2272 (1.6%) | 2232 (1.6%) | 40 (1.2%) | |
| Married | 0.293 | |||
| No | 57,852 (40.6%) | 56,525 (40.6%) | 1327 (39.7%) | |
| Yes | 84,635 (59.4%) | 82,621 (59.4%) | 2014 (60.3%) | |
| Missing | 2494(1.7%) | 2445(1.7%) | 49 (1.4%) | |
| SVI | 0.01 | |||
| Low | 48,162 (33.8%) | 47,096 (33.9%) | 1066 (31.9%) | |
| Medium | 48,068 (33.8%) | 46,949 (33.8%) | 1119 (33.5%) | |
| High | 46,099 (32.4%) | 44,942 (32.3%) | 1157 (34.6%) | |
| Missing | 2652(1.8%) | 2604 (1.8%) | 48(1.4%) | |
| Cancer site | <0.001 | |||
| Biliary | 2679 (1.8%) | 2604 (1.8%) | 75 (2.2%) | |
| Colon | 49,285 (34.0%) | 48,495 (34.3%) | 790 (23.3%) | |
| Liver | 23,643 (16.3%) | 23,184 (16.4%) | 459 (13.5%) | |
| Pancreas | 34,280 (23.6%) | 32,616 (23.0%) | 1664 (49.1%) | |
| Rectum | 35,094 (24.2%) | 34,692 (24.5%) | 402 (11.9%) | |
| Any opioid | <0.001 | |||
| No | 98,840 (68.2%) | 97,506 (68.9%) | 1334 (39.4%) | |
| Yes | 46,141 (31.8%) | 44,085 (31.1%) | 2056 (60.6%) | |
| Total opioid prescription days among opioid users (Median; IQR) | 16 (4–62) | 15 (4–61) | 35 (8–76) | <0.001 |
| Total cannabis prescription days (Median; IQR) | 0 (0–0) | 0 (0–0) | 31 (31–49) | <0.001 |
| Index Year | <0.001 | |||
| 2017 | 11,680 (8.1%) | 11,372 (8.0%) | 308 (9.1%) | |
| 2018 | 13,442 (9.3%) | 13,069 (9.2%) | 373 (11.0%) | |
| 2019 | 14,058 (9.7%) | 13,626 (9.6%) | 432 (12.7%) | |
| 2020 | 14,231 (9.8%) | 13,866 (9.8%) | 365 (10.8%) | |
| 2021 | 16,619 (11.5%) | 16,197 (11.4%) | 422 (12.4%) | |
| 2022 | 17,732 (12.2%) | 17,301 (12.2%) | 431 (12.7%) | |
| 2023 | 18,284 (12.6%) | 17,791 (12.6%) | 493 (14.5%) | |
| 2024 | 20,626 (14.2%) | 20,258 (14.3%) | 368 (10.9%) | |
| 2025 | 18,309 (12.6%) | 18,111 (12.8%) | 198 (5.8%) |
Variables with >5% missingness; complete-case analyses were conducted as sensitivity analyses. Analyses were performed using SAS 9.4; two-sided α = 0.05.
3.2. Opioid Utilization by Cannabis Exposure
Early prescribed cannabinoid exposure was not associated with reduced opioid use. Compared with nonrecipients, cannabinoid recipients were more likely to receive opioids (60.6% vs. 31.1%; p < 0.001). Among patients who received opioids, cannabinoid recipients had longer total opioid prescription days (median 35 [IQR, 8–76] vs. 15 [IQR, 4–61] days; p < 0.001). Compared with nonrecipients, cannabinoid recipients were more often Black (17.2% vs. 11.9%) and less likely to be White (75.1% vs. 78.8%), more likely to reside in the South (48.9% vs. 37.5%), more likely to have pancreatic cancer (49.1% vs. 23.0%), and less likely to have colon cancer (23.3% vs. 34.3%) (all p < 0.001). Residence in high-SVI counties was also modestly more common among recipients, compared with nonrecipients (34.6% vs. 32.3%; p = 0.01) (Table 1).
3.3. Factors Associated with Early Cannabis Prescribing
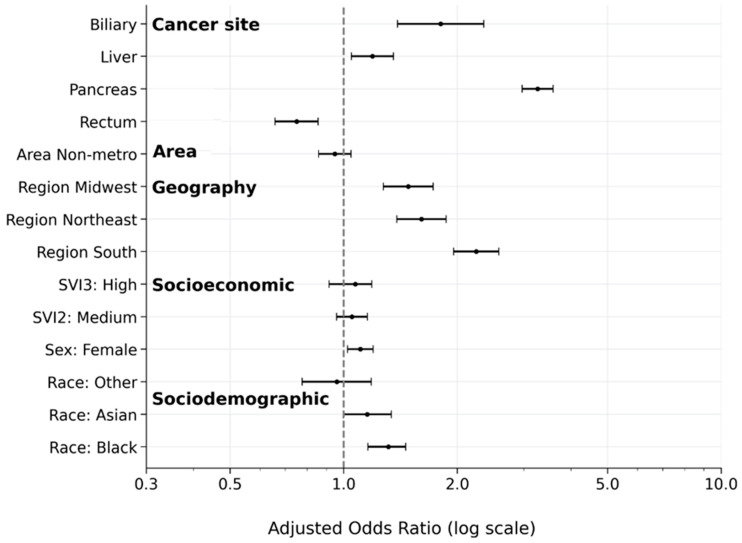
In a multivariable analysis (Model 1), Black race was independently associated with higher odds of early cannabis prescribing in a model adjusted for patient-level characteristics (Model 1: aOR 1.45, 95%CI 1.30–1.61; p < 0.001), an association that persisted with additional regional adjustment (Model 2, including region: aOR 1.31, 95%CI 1.18–1.46; p < 0.001) (Table 2 and Table 3). Female sex was also modestly associated with higher odds of cannabis use (aOR 1.11, 95%CI 1.03–1.19; p = 0.018). High SVI was associated with greater cannabis use in Model 1 (aOR 1.16, 95%CI 1.05–1.28; p = 0.009), but the effect was attenuated after adjusting for region in Model 2 (aOR 1.07, 95%CI 0.97–1.89; p = 0.249). Interestingly, the cancer site was the strongest determinant of early cannabis use. Compared with colon cancer, the adjusted odds were substantially higher for pancreatic cancer (aOR, 3.23; 95%CI, 2.96–3.57), modestly higher for liver cancer (aOR, 1.19; 95%CI, 1.05–1.35), and lower for rectal cancer (aOR, 0.75; 95%CI, 0.66–0.86) (all p < 0.001 or p < 0.02) (Table 2; Figure 1).
Table 2: Multivariable model—factors associated with cannabis use (Model 1; region excluded, p-values adjusted for multiple comparisons).
| Variable | aOR | 95%CI | Adj p-Value |
|---|---|---|---|
| Age | 1.12 | 0.99–1.21 | 0.158 |
| Sex (male ref) | |||
| Female | 1.11 | 1.03–1.19 | 0.020 |
| CCI (CCI ≤ 2 ref) | |||
| CCI > 2 | 0.82 | 0.67–1.02 | 0.137 |
| Race (white ref) | |||
| Black | 1.45 | 1.30–1.61 | <0.001 |
| Asian | 0.98 | 0.82–1.18 | 0.881 |
| Other | 0.84 | 0.68–1.04 | 0.161 |
| SVI (low ref) | |||
| Medium | 1.06 | 0.98–1.19 | 0.146 |
| High | 1.16 | 1.05–1.28 | 0.009 |
| Area (Metro ref) | |||
| Non-metro | 0.97 | 0.88–1.08 | 0.619 |
| Cancer site (Colon ref) | |||
| Biliary | 1.77 | 1.37–2.31 | <0.001 |
| Liver | 1.19 | 1.05–1.35 | 0.020 |
| Pancreas | 3.23 | 2.96–3.57 | <0.001 |
| Rectum | 0.75 | 0.66–0.86 | <0.001 |
| Index Year (2017 ref) | |||
| 2018 | 1.05 | 0.89–1.24 | 0.648 |
| 2019 | 1.11 | 0.95–1.31 | 0.278 |
| 2020 | 0.95 | 0.81–1.13 | 0.648 |
| 2021 | 0.91 | 0.77–1.07 | 0.326 |
| 2022 | 0.85 | 0.72–1.02 | 0.115 |
| 2023 | 1.02 | 0.85–1.17 | 0.994 |
| 2024 | 0.68 | 0.58–0.80 | <0.001 |
| 2025 | 0.40 | 0.33–0.48 | <0.001 |
Abbreviations: CI: confidence interval, Adj p-value: adjusted p-value, CCI: Charlson Comorbidity Index, and SVI: Social Vulnerability Index.
Table 3: Multivariable model (Model 2: Region included p-values adjusted for multiple comparisons).
| Variable | aOR | 95%CI | Adj p-Value |
|---|---|---|---|
| Age | 1.02 | 0.99–1.04 | 0.173 |
| Sex (Male ref) | |||
| Female | 1.11 | 1.03–1.19 | 0.018 |
| CCI (CCI ≤ 2 ref) | |||
| CCI > 2 | 0.87 | 0.70–1.07 | 0.267 |
| Race (White ref) | |||
| Black | 1.31 | 1.18–1.46 | <0.001 |
| Asian | 1.15 | 0.96–1.38 | 0.228 |
| Other | 0.96 | 0.78–1.18 | 0.720 |
| SVI (SVI low ref) | |||
| Medium | 1.05 | 0.96–1.15 | 0.364 |
| High | 1.07 | 0.97–1.89 | 0.249 |
| Region | |||
| Midwest | 1.48 | 1.27–1.72 | <0.001 |
| Northeast | 1.61 | 1.39–1.96 | <0.001 |
| South | 1.22 | 1.95–2.57 | <0.001 |
| Area (Metro ref) | |||
| Non-metro | 0.95 | 0.86–1.05 | 0.354 |
| Cancer site (Colon ref) | |||
| Biliary | 1.83 | 1.39–2.35 | <0.001 |
| Liver | 1.19 | 1.05–1.35 | 0.018 |
| Pancreas | 3.26 | 2.97–3.58 | <0.001 |
| Rectum | 0.75 | 0.66–0.85 | <0.001 |
| Index Year (2017 ref) | |||
| 2018 | 1.05 | 0.89–1.24 | 0.635 |
| 2019 | 1.11 | 0.94–1.30 | 0.287 |
| 2020 | 0.95 | 0.81–1.23 | 0.635 |
| 2021 | 0.89 | 0.75–1.04 | 0.223 |
| 2022 | 0.83 | 0.70–0.97 | 0.044 |
| 2023 | 0.99 | 0.84 -1.17 | 0.882 |
| 2024 | 0.66 | 0.56–0.78 | <0.001 |
| 2025 | 0.39 | 0.32–0.48 | <0.001 |
Abbreviations: CI: Confidence interval, Adj p-value: Adjusted p-value, CCI: Charlson Comorbidity Index, SVI: Social Vulnerability Index.
Adjusted odds ratios (aORs) and 95%CI are from a multivariable logistic regression model, including demographic characteristics, cancer site, social vulnerability, geographic region, and area of residence (Model 2). The reference categories were male sex, White race, low Social Vulnerability Index score, metropolitan residence, West region, and colon cancer. Odds ratios greater than one indicated higher odds of cannabis prescribing.
3.4. Geographic and Temporal Patterns
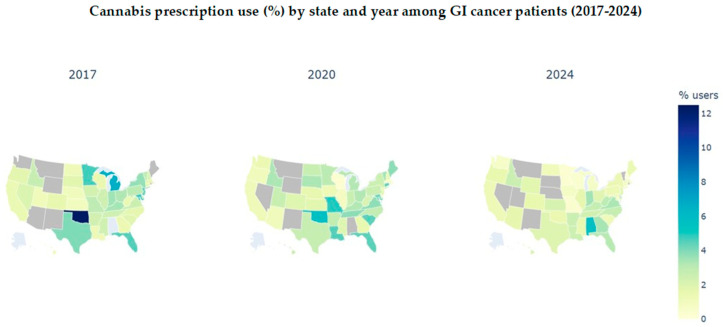
After adjustment (Model 2), substantial regional variation was observed (Table 3). Compared with the West (reference), patients in the Midwest (aOR, 1.48; 95%CI, 1.27–1.72) and Northeast (aOR, 1.61; 95%CI, 1.39–1.96) had higher odds of cannabinoid prescribing; the South also had modestly elevated odds (aOR, 1.22; p < 0.001; 95%CI provided in Table 3). State-level prescribing proportions varied widely (states with <11 cases were suppressed per COSMOS disclosure policies) (Supplementary Table S2; Figure 2). Relative to 2017, the odds of early cannabinoid prescribing declined over time, with lower odds by 2024 (aOR 0.66; 95%CI, 0.56–0.78) and 2025 (aOR 0.39; 95%CI, 0.32–0.48) (Table 3; Supplementary Table S3).
4. Discussion
Over the past two decades, the availability of medical cannabis in the United States has expanded substantially, alongside growing expectations that it may mitigate chemotherapy-related symptoms such as nausea, sleep disturbance, and appetite loss [ref. 4,ref. 25,ref. 26]. Despite extensive investigation, evidence regarding its effectiveness for cancer pain and its potential opioid-sparing role has remained mixed and inconclusive [ref. 5,ref. 12,ref. 25,ref. 26]. Notably, patient-level data evaluating prescription cannabinoids and opioid substitution during the critical period of chemotherapy initiation have been limited. Using multisite Epic COSMOS electronic health record data, the current study examined short-term opioid utilization associated with cannabinoids prescribing at chemotherapy initiation among patients with GI cancers. In this analysis, early cannabis use was not associated with reduced opioid use within 90 days; instead, THC cannabis prescribing was clustered among patients with more aggressive cancers (particularly pancreatic cancer) and varied by race and geographic region, underscoring the heterogeneity in supportive care practices and the influence of differential policy and clinical environments.
In this large, multisite EHR cohort of adults initiating chemotherapy for GI cancers, early cannabinoid prescribing was not associated with reduced short-term opioid utilization. Instead, cannabinoid recipients were more likely to receive opioids and, among opioid recipients, had a longer cumulative prescription over 90 days. These patient-level findings suggest limited short-term opioid substitution in routine GI cancer care, and align with randomized trials and meta-analyses demonstrating small or inconsistent analgesic benefits and no reliable opioid-sparing effect when cannabinoids are added to standard regimens [ref. 22,ref. 27]. Professional society guidance generally supports cannabinoids for chemotherapy-induced nausea and vomiting, with insufficient evidence for routine use in cancer-related pain or to reduce opioid exposure [ref. 28,ref. 29]. In contrast to ecological/policy-level analyses reporting declines in opioid dispensing after cannabis legalization in some populations [ref. 16,ref. 25], data in the current study indicated that such population-level associations may not reflect individual-level clinical effects during chemotherapy initiation. Collectively, these findings suggest that early cannabinoid prescribing may identify patients with greater symptom burden, rather than function as an early opioid substitute.
Cannabinoid prescribing varied by cancer site and clustered among patients with pancreatic and biliary-adjacent cancers, and it was less common in colon/rectal cancers, which is consistent with clinical triage toward patients with more severe or refractory symptoms [ref. 12,ref. 25,ref. 30]. Other observational oncology data has similarly suggested that patients with higher pain, sleep disturbance, or anxiety are more likely to seek adjunctive options, including cannabinoids, early in treatment [ref. 31,ref. 32,ref. 33,ref. 34]. Meta-analyses of randomized trials, including cancer-pain populations, have generally failed to note any meaningful incremental analgesia compared with a placebo when cannabinoids were added to opioids, alongside a higher risk of nonserious adverse events [ref. 35,ref. 36]. Within a learning health system, this pattern underscores the need for patient-level evidence and careful expectation-setting when considering cannabinoids during chemotherapy initiation.
Racial differences in prescribing persisted after adjustment, with higher odds among Black patients. These patterns mirror well-documented inequities in cancer pain management and access to supportive care [ref. 37,ref. 38,ref. 39]. Structural barriers (out-of-pocket costs, coverage exclusions, certification and travel requirements, dispensary density), clinician-level factors (implicit bias, differential risk perceptions), and patient-level determinants (stigma, prior criminalization exposure, varying beliefs about effectiveness) likely contribute to heterogeneous uptake and sourcing [ref. 18,ref. 40,ref. 41,ref. 42,ref. 43,ref. 44]. Without equity-focused implementation, legalization may yield uneven clinical and social benefits [ref. 38,ref. 45,ref. 46,ref. 47]. Oncology pathways should include coverage support, training in balanced counseling (including candid discussion of limited analgesic/opioid-sparing evidence), standardized education on safe sourcing and product labeling/potency, and social-equity provisions to mitigate disparities. Regionally, adjusted prescribing was also higher in the Midwest and Northeast, relative to the West, and the odds of cannabis prescription declined markedly after 2017. Regional heterogeneity likely reflected differences in program design and implementation (certification criteria, fees, product limits, labeling standards, dispensary density), payer coverage, and concurrent opioid policies (e.g., PDMPs, prior authorization, dose limits), rather than pharmacologic substitution alone [ref. 12,ref. 16,ref. 47]. Policy-aware oncology research should move beyond ecological inference and incorporate granular exposure measures (program features, access constraints, formulation/dose/route), patient-level outcomes, and quasi-experimental designs that account for staggered policy adoption and co-occurring regulations. Collectively, these patterns indicate that early cannabinoid prescribing is unlikely to function as an opioid-sparing strategy in routine GI cancer care and more likely reflects underlying symptom burden, underscoring the need for equitable, evidence-based supportive care interventions.
5. Strengths and Limitations
The current study leveraged a large, multisite EHR dataset (COSMOS), enabling the comprehensive capture of prescribing cannabinoid patterns across diverse geographic regions, racial groups, and gastrointestinal cancer types. This breadth allowed for a detailed evaluation of variation in cannabinoid use across the clinical and demographic subpopulations. In addition, robust multivariable adjustment strengthened the internal validity by addressing a wide range of potential confounders that are available within the EHR. However, despite these strengths, interpretations of the current study findings should consider several limitations. First, because COSMOS captures only FDA-approved cannabinoid prescriptions documented in the EHR, nonprescription cannabis obtained through dispensaries or state cannabis programs could not be measured, potentially leading to exposure misclassification. Second, residual confounding was likely despite exclusions and multivariable adjustment, particularly due to unmeasured symptom severity, palliative intent, and clinician prescribing preferences. Cannabinoid prescribing may function as a proxy for greater symptom burden, such as uncontrolled pain, nausea, or cachexia, rather than acting as a causal driver of opioid utilization. Third, the absence of standardized symptom-severity scores in COSMOS limited the ability to directly adjust for confounding by indication. Additionally, key contextual determinants—including state cannabis policy, insurance coverage, and product availability—were not directly linkable to patient-level records, limiting inference regarding structural drivers of use. The retrospective design precluded causal interpretation of observed associations. Regional and temporal heterogeneity further suggested evolving practice patterns within dynamic policy environments. Future studies should integrate policy and payer data, standardize cannabinoid exposure measures (dose, route, THC:CBD ratio), and examine longer-term outcomes such as opioid dose trajectories, pain interference, and functional recovery. Adoption of common data elements and learning health system approaches may accelerate evidence generation, as substantial geographic variation indicates that legalization alone is insufficient; rather, local implementation within oncology supportive care pathways likely determines the real-world impact.
6. Conclusions
In this large multisite EHR study of patients with GI cancers, early cannabis use at the start of chemotherapy was not associated with reduced short-term opioid utilization. Instead, cannabinoid prescribing appeared more common among patients with greater symptom burden or more aggressive disease. These patterns suggest that early cannabis use is unlikely to function as an opioid-sparing strategy in routine GI cancer care and may primarily reflect an underlying clinical need. Racial and regional differences in prescribing highlight persistent inequities and the influence of policy and practice environments, rather than true pharmacologic substitution. Overall, cannabis should be considered, when used as an adjunct for selected symptoms, rather than a replacement for opioids. Guideline-concordant multimodal analgesia, early supportive care, and equity-focused implementation remain central to effective cancer pain management.
References
- G.W. Neeley, L.E. Richardson. Influences on cannabis policy design and adaptation in the American states. Policy Stud. J., 2025. [DOI]
- D.M. Anderson, D.I. Rees. The Public Health Effects of Legalizing Marijuana. J. Econ. Lit., 2023. [DOI]
- 3.Available online: https://news.uga.edu/cannabis-dispensaries-reduce-opioid-prescriptions/(accessed on 12 December 2025)
- J.C. Hu, K. Karan, H. Zhang, R. Portenoy, W.E. Rosa, Y. Zhang, M.C. Reid, R.M. Tamimi, F. Zhang, E. Bruera. Medical marijuana policies, opioid prescriptions, and adverse events among patients undergoing cancer resection surgery. Cancer, 2025. [DOI | PubMed]
- D.E. Slawek, C. Zhang, S. Dahmer, N. Sohler, Y. Zolotov, J.L. Starrels, Y. Deng, G. Calderon DiFrancesca, F.R. Levin, J. Ross. Medical Cannabis and Opioid Receipt Among Adults With Chronic Pain. JAMA Intern. Med., 2026. [DOI | PubMed]
- R. Snijders, L. Brom, M. Theunissen, M. Van Den Beuken-van Everdingen. Update on Prevalence of Pain in Patients with Cancer 2022: A Systematic Literature Review and Meta-Analysis. Cancers, 2023. [DOI | PubMed]
- 7.Available online: https://www.cancer.gov/about-cancer/treatment/side-effects/nausea/nausea-hp-pdq(accessed on 12 December 2025)
- A.K. Kropp Lopez, S.D. Nichols, D.Y. Chung, D.E. Kaufman, K.L. McCall, B.J. Piper. Prescription Opioid Distribution after the Legalization of Recreational Marijuana in Colorado. Int. J. Environ. Res. Public Health, 2020. [DOI | PubMed]
- A. Alam, D.N. Juurlink. The prescription opioid epidemic: An overview for anesthesiologists. Can. J. Anesth./J. Can. Anesth., 2016. [DOI]
- M. Meldrum. Opioids’ Long Shadow. AMA J. Ethics, 2020. [DOI | PubMed]
- M. Cerdá, K. Wheeler-Martin, E. Bruzelius, C.M. Mauro, S. Crystal, C.S. Davis, S. Adhikari, J. Santaella-Tenorio, K.M. Keyes, S.S. Martins. The role of prescription opioid and cannabis supply policies on opioid overdose deaths. Am. J. Epidemiol., 2025. [DOI | PubMed]
- H.V. Nguyen, E.E. McGinty, S. Mital, G.C. Alexander. Recreational and Medical Cannabis Legalization and Opioid Prescriptions and Mortality. JAMA Health Forum, 2024. [DOI | PubMed]
- P. Grimison, A. Mersiades, A. Kirby, A. Tognela, I. Olver, R.L. Morton, P. Haber, A. Walsh, Y. Lee, E. Abdi. Oral Cannabis Extract for Secondary Prevention of Chemotherapy-Induced Nausea and Vomiting: Final Results of a Randomized, Placebo-Controlled, Phase II/III Trial. J. Clin. Oncol., 2024. [DOI | PubMed]
- R. Chow, A. Basu, J. Kaur, D. Hui, J. Im, E. Prsic, G. Boldt, M. Lock, L. Eng, T.L. Ng. Efficacy of cannabinoids for the prophylaxis of chemotherapy-induced nausea and vomiting-a systematic review and meta-analysis. Support. Care Cancer, 2025. [DOI | PubMed]
- S.F. Kemmner, J. Dörfler, J. Huebner. Cannabinoids for the prevention of chemotherapy-induced nausea and vomiting in oncological therapy: A systematic review. J. Cancer Surviv., 2025. [DOI]
- F. Lozano-Rojas, V. Bethel, S. Gupta, S.R. Steuart, W.D. Bradford, A.J. Abraham. Cannabis Laws and Opioid Use Among Commercially Insured Patients With Cancer Diagnoses. JAMA Health Forum, 2025. [DOI | PubMed]
- T.M. Brasky, S. Lee, B. McBride, A.M. Newton, R.D. Baltic, T.L. Wagener, S. Conroy, J.L. Hays, E.E. Stevens, A. Adib. Prevalence of cannabis and medication use by indices of residential urbanicity and deprivation among Ohio cancer patients. Cancer Causes Control, 2025. [DOI | PubMed]
- R.L. Ashare, B. Worster, S.M. Nugent, D.M. Smith, B.J. Morasco, A.E. Leader, A.A. Case, S.H. Meghani. Cannabis and opioid perceptions, co-use, and substitution among patients across 4 NCI-Designated Cancer Centers. J. Natl. Cancer Inst. Monogr., 2024. [DOI | PubMed]
- S. Pourebrahim, T. Ahmad, E. Rottmann, J. Schulze, B. Scheller. Does Cannabis Use Contribute to Schizophrenia? A Causation Analysis Based on Epidemiological Evidence. Biomolecules, 2025. [DOI | PubMed]
- Epic Cosmos
- ICD-10-CM Code Range C15–C26: Malignant Neoplasms of Digestive Organs. RxReasoner
- 22. Centers for Disease Control and Prevention CDC Social Vulnerability Index (SVI) [Internet]Centers for Disease Control and PreventionAtlanta, GA, USA2025Available online: https://www.atsdr.cdc.gov/place-health/php/svi/?CDC_AAref_Val=https://www.atsdr.cdc.gov/placeandhealth/svi/index.html/(accessed on 12 December 2025)
- M.E. Charlson, P. Pompei, K.L. Ales, C.R. MacKenzie. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis., 1987. [DOI | PubMed]
- B.E. Flanagan, E.W. Gregory, E.J. Hallisey, J.L. Heitgerd, B. Lewis. A Social Vulnerability Index for Disaster Management. J. Homel. Secur. Emerg. Manag., 2011. [DOI]
- Y. Bao, H. Zhang, E. Bruera, R. Portenoy, W.E. Rosa, M.C. Reid, H. Wen. Medical Marijuana Legalization and Opioid- and Pain-Related Outcomes Among Patients Newly Diagnosed With Cancer Receiving Anticancer Treatment. JAMA Oncol., 2023. [DOI | PubMed]
- P.F. Whiting, R.F. Wolff, S. Deshpande, M. Di Nisio, S. Duffy, A.V. Hernandez, J.C. Keurentjes, S. Lang, K. Misso, S. Ryder. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA, 2015. [DOI | PubMed]
- L. Wang, P.J. Hong, C. May, Y. Rehman, Y. Oparin, C.J. Hong, B.Y. Hong, M. AminiLari, L. Gallo, A. Kaushal. Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: A systematic review and meta-analysis of randomised clinical trials. BMJ, 2021. [DOI | PubMed]
- L. Coscia, P. Causa, E. Giuliani, A. Nunziata. Pharmacological properties of new neuroleptic compounds. Arzneimittelforschung, 1975. [PubMed]
- J. Janke, A. Fleckenstein, B. Hein, O. Leder, H. Sigel. Prevention of myocardial Ca overload and necrotization by Mg and K salts or acidosis. Recent Adv. Stud. Card. Struct. Metab., 1975. [PubMed]
- A. Noori, A. Miroshnychenko, Y. Shergill, V. Ashoorion, Y. Rehman, R.J. Couban, D.N. Buckley, L. Thabane, M. Bhandari, G.H. Guyatt. Opioid-sparing effects of medical cannabis or cannabinoids for chronic pain: A systematic review and meta-analysis of randomised and observational studies. BMJ Open, 2021. [DOI | PubMed]
- S. Amin, S.W. Chae, C.T. Kawamoto, K.T. Phillips, P. Pokhrel. Cannabis use among cancer patients and survivors in the United States: A systematic review. JNCI Cancer Spectr., 2024. [DOI | PubMed]
- J.M. Powers, L.R. LaRowe, D. Rubenstein, J.A. Paice, B. Hitsman, C.M. Rini. Relationship between pain and nonopioid substance use in two national samples of cancer survivors. Cancer, 2025. [DOI | PubMed]
- M. Chwistek. Cancer, Cannabis, and the Search for Relief. J. Natl. Compr. Cancer Netw., 2019. [DOI]
- S.A. Pergam, M.C. Woodfield, C.M. Lee, G.S. Cheng, K.K. Baker, S.R. Marquis, J.R. Fann. Cannabis use among patients at a comprehensive cancer center in a state with legalized medicinal and recreational use. Cancer, 2017. [DOI | PubMed]
- S. Nielsen, P. Sabioni, J.M. Trigo, M.A. Ware, B.D. Betz-Stablein, B. Murnion, N. Lintzeris, K.E. Khor, M. Farrell, A. Smith. Opioid-Sparing Effect of Cannabinoids: A Systematic Review and Meta-Analysis. Neuropsychopharmacology, 2017. [DOI | PubMed]
- M. Mücke, T. Phillips, L. Radbruch, F. Petzke, W. Häuser. Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database Syst. Rev., 2018. [DOI]
- A. Schoenthaler, N. Williams. Looking Beneath the Surface: Racial Bias in the Treatment and Management of Pain. JAMA Netw. Open, 2022. [DOI | PubMed]
- G. Himmelstein, P.A. Ganz. Distribution of Cancer Care Resources Across US Hospitals by Patient Race and Ethnicity. JAMA Oncol., 2024. [DOI | PubMed]
- R.A. Rodin, C.B. Smith. Examining Racial and Ethnic Inequities in Opioid Prescribing and Risk Screening Among Patients With Advanced Cancer. J. Clin. Oncol., 2023. [DOI | PubMed]
- L.P. Gibson, R.A. Ferrer, S.H. Meghani, A.M. Acevedo. Potential role of cannabis in ameliorating observed racialized disparities in cancer pain management. JNCI J. Natl. Cancer Inst., 2024. [DOI | PubMed]
- B. Worster, S.H. Meghani, A.E. Leader, S.M. Nugent, K.F. Jones, K.A. Yeager, K. Liou, R.L. Ashare. Toward reducing racialized pain care disparities: Approaching cannabis research and access through the lens of equity and inclusion. Cancer, 2024. [DOI | PubMed]
- J.L. Mego. Further evidence for a proton pump in mouse kidney phagolysosomes: Effect of nigericin and 2,4-dinitrophenol on the stimulation of intralysosomal proteolysis by ATP. Biochem. Biophys. Res. Commun., 1975. [DOI | PubMed]
- K. Turner, O.T. Nguyen, J.Y. Islam, S. Rajasekhara, Y.C. Martinez, A.A. Tabriz, B.D. Gonzalez, H.S.L. Jim, K.M. Egan. Patient-provider communication about the use of medical cannabis for cancer symptoms: A cross-sectional study. J. Natl. Cancer Inst. Monogr., 2024. [DOI | PubMed]
- J.G. Cannon, J.P. O’Donnell, T. Lee, C.R. Hoppin, J.P. Long, M. Ilhan, B. Costall, R.J. Naylor. N-Isopropyl derivatives of dopamine and 5,6-dihydroxy-2-aminotetralin. J. Med. Chem., 1975. [DOI | PubMed]
- M. Hsu, A. Shah, A. Jordan, M.S. Gold, K.P. Hill. Therapeutic Use of Cannabis and Cannabinoids: A Review. JAMA, 2026. [DOI | PubMed]
- S.S. Martins, L.E. Segura, N.S. Levy, P.M. Mauro, C.M. Mauro, M.M. Philbin, D.S. Hasin. Racial and Ethnic Differences in Cannabis Use Following Legalization in US States With Medical Cannabis Laws. JAMA Netw. Open, 2021. [DOI | PubMed]
- B.E. Sheehan, R.A. Grucza, A.D. Plunk. Association of Racial Disparity of Cannabis Possession Arrests Among Adults and Youths With Statewide Cannabis Decriminalization and Legalization. JAMA Health Forum, 2021. [DOI | PubMed]