
Chemsex and uptake of HIV pre-exposure prophylaxis among adult cisgender gay, bisexual and other men who have sex with men worldwide: a systematic review with meta-analysis
Abstract
Background:
There is a lack of summarized information regarding the uptake of pre-exposure prophylaxis (PrEP) among HIV negative gay, bisexual and other men who have sex with men (GBMSM) who engage in chemsex. This systematic review and meta-analysis aimed to summarize, assess the quality of existing evidence, estimate the prevalence of PrEP uptake among GBMSM who engage in chemsex, based on available global evidence; and evaluate whether engagement in chemsex is associated with increased odds of PrEP uptake in this population.
Methods:
We searched Medline, Embase, Cochrane Reviews and CENTRAL, APA PsycInfo, Scopus, and LILACS. We included studies reporting chemsex practices among adult cisgender GBMSM and PrEP uptake until July 1, 2025. Evidence quality was assessed using the Newcastle–Ottawa Scale tool. Chemsex exposure was analyzed using two timeframe groups: recent (past 6 months) and ever (any longer or unspecified timeframe). Prevalence and associations -odds ratio (OR)- were pooled in meta-analyses using a random-effect model. Inconsistency, sensitivity, and publication bias analyses were conducted. PROSPERO registration: CRD42024573871.
Findings:
Among 3988 records screened, 28 studies comprising 36,339 participants across three world regions were included: Western and Central Europe and North America, Asia and the Pacific, and Latin America; all were rated low to moderate quality. The overall prevalence of PrEP use was 39% (95% CI: 29–49%) among GBMSM who engaged in chemsex, with no significant differences between recent and ever chemsex timeframe groups. Sensitivity analyses and meta-regressions showed no significant effect of study publication year, country income group or world region. Overall chemsex was associated with higher odds of PrEP use (OR = 3.44, 95% CI: 2.70–4.38), with a significantly stronger association for ever chemsex (OR = 4.74, 95% CI: 3.48–6.46) than for recent chemsex (OR = 2.84, 95% CI: 2.11–3.81p < 0.05). Meta-regressions indicated significantly lower odds of PrEP use in studies from low- and middle-income countries for both recent (OR = 0.54, 95% CI: 0.31–0.94; p = 0.031) and ever (OR = 0.46, 95% CI: 0.21–0.99; p = 0.046) chemsex timeframes. Heterogeneity remained moderate to high across all analyses.
Interpretation:
Our findings suggest that PrEP use is relatively common among GBMSM who engage in chemsex globally and chemsex is consistently and strongly associated with increased PrEP uptake in this population. The association between chemsex and PrEP use was significantly higher in studies from high-income settings, where chemsex practices are better described and PrEP is more widely available for this group. The lack of standardized definitions in the field contributes to the high heterogeneity and strongly influences the generation of global evidence. This first systematic review and metanalysis in the field highlights the need to expand and integrate chemsex harm reduction and PrEP services for GBMSM, especially in low- and middle-income settings, to improve health outcomes and advance towards the global HIV elimination goals.
Funding:
Publication fees were sponsored by the Research Group of the HIV Unit, Infectious Disease Division, Department of Medicine, Geneva University Hospitals, Geneva, Switzerland. The Covidence membership and the fees for an academic librarian developing a professional systematic search strategy were sponsored by the Research Group of the HIV Unit, Infectious Diseases Service, Hospital Clinic, and IDIBAPS, University of Barcelona, Barcelona, Spain. No further funding was received for this study.
Article type: Research Article
Keywords: Gay, Bisexual and other men who have sex with men, Chemsex, HIV pre-exposure prophylaxis, HIV prevention, Harm reduction
Affiliations: Faculty of Medicine, Institute of Global Health, University of Geneva, Chemin des Mines 9, 1202, Geneva, Switzerland; HIV Unit, Infectious Diseases Service, Hospital Clinic-IDIBAPS, University of Barcelona, Carrer de Villarroel 170, 08036, Barcelona, Spain; The Joint United Nations Program on HIV/AIDS (UNAIDS), Av. Appia 20, 1211, Geneva, Switzerland; Centro de Investigación Biomédica en Red de Enfermedades Infecciosas (CIBERINFEC), Instituto de Salud Carlos III, Madrid, Spain; HIV Unit, Infectious Disease Division, Department of Medicine, Geneva University Hospitals, Rue Gabrielle-Perret Gentil 6, 1205, Geneva, Switzerland; Department of Migrant Health, Global Tuberculosis Program. Baylor College of Medicine, 1102 Bates Avenue, FC 630, Houston, TX, 77030, USA
License: © 2026 The Author(s) CC BY 4.0 This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.1016/j.eclinm.2026.103804 | PubMed: 41938845 | PMC: PMC13043317
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (4.3 MB)
Research in context
Evidence before this study
Adult cisgender gay, bisexual, and other men who have sex with men (GBMSM) remain disproportionately affected by HIV globally and the use of HIV pre-exposure prophylaxis (PrEP) is recommended as a highly effective prevention strategy for this population. The intentional use of drugs to enhance sexual experiences in this group, referred as chemsex, is associated with increased sexual risk behaviors and HIV infection. Chemsex typically involves drugs such as methamphetamine, γ-hydroxybutyrate/γ-butyrolactone (GHB/GBL), or mephedrone.
Before this study, there was no systematic review of the literature or meta-analysis to synthesize the published evidence and examine the association of PrEP use among adult cisgender GBMSM who engage in chemsex. We searched Medline, Embase, Cochrane Reviews and CENTRAL, APA PsycInfo, Scopus, and LILACS from inception to Dec 4, 2024, and updated on July 1, 2025, without language or time restrictions. Searches combined indexing terms and free text for “men who have sex with men”, “chemsex”, and “pre-exposure prophylaxis”. Eligible studies reported prevalence or correlates of PrEP use among adult cisgender GBMSM engaging in chemsex.
Added value of this study
This is the first systematic review and meta-analysis to provide a global perspective on the relationship between chemsex and PrEP use among adult cisgender GBMSM. Across 28 studies from three world regions: Western and Central Europe and North America (WCENA); Asia and the Pacific (AP); and Latin America (LA), pooled estimates indicate more than threefold higher odds of PrEP use among this group. The association is stronger in the subgroup of adult cisgender GBMSM who reported engaging in chemsex at some point in their lifetime than among those who reported recent chemsex. Adult cisgender GBMSM who engaged in chemsex had lower odds of PrEP use in low- and middle-income countries (LMICs) compared with high-income settings. Chemsex practices may serve as a behavioral marker to identify individuals at higher risk of HIV infection and to support the incorporation of PrEP into HIV prevention services for this population.
Implications of all the available evidence
Evidence emanating from this study shows that engagement in chemsex among adult cisgender GBMSM is a global phenomenon and supports incorporating screening of sexualized substance use and harm reduction services into sexual health services for this population. Similarly, adult cisgender GBMSM who engage in chemsex have increased odds of using PrEP globally, however this intervention should be scaled up more widely to significantly decrease the risk of HIV infection in this group. Expanding culturally adapted HIV and harm reduction interventions related to chemsex for adult cisgender GBMSM would benefit from expanding existing evidence, especially in underrepresented regions including sub-Saharan Africa and Eastern Europe and Central Asia.
Introduction
Human immunodeficiency virus (HIV) remains a significant global public health concern, posing an important health risk to key populations.ref. bib1 According to the Joint United Nations Programme on HIV/AIDS (UNAIDS), gay, bisexual and other men who have sex with men (GBMSM) are particularly vulnerable to HIV and frequently experience human rights violations and lack adequate access to services.ref. bib2 In 2022, GBMSM were up to 23 times more likely to acquire HIV compared to the general adult population (15–49 years of age), with a reported global median HIV prevalence of 8% and rates reaching 11% in eastern and southern Africa. In the same year, GBMSM accounted for an estimated 20% of new infections globally, reaching up to 42% in Asia and the Pacific region and 45% in Latin America.ref. bib3,ref. bib4 Among the factors linked to HIV vulnerability in adult cisgender GBMSM, recent evidence has identified chemsex as a key contributor.ref. bib5
Despite the lack of a uniform definition, chemsex is a complex and culturally diverse global phenomenonref. bib6 that typically involves the intentional use of specific drugs, such as methamphetamine, mephedrone, γ-hydroxybutyrate/γ-butyrolactone (GHB/GBL), and, to a lesser extent, ketamine or cocaine, by GBMSM, to enhance or facilitate sexual experiences.ref. bib7 Chemsex can be characterized as a specific subset of sexualized drug use (SDU), distinguished by its intentionality for sex and prolonged duration of sex. This phenomenon has been primarily described within, and disproportionately affects, GBMSM community.ref. bib8 Chemsex is associated with high-risk sexual behaviors such as condomless sex, multiple partners, group sex, transactional sex, and polydrug use. When these practices occur in a poorly managed or unregulated context, they can lead to severe and multidimensional consequences including increased risk of HIV, hepatitis C and other sexually transmitted infections, as well as mental, physical, social and substance use-related health conditions,ref. bib9,ref. bib10 highlighting the urgent need for integrated and comprehensive health strategies to address chemsex-related risks.ref. bib11 Understanding the motivations behind chemsex is equally crucial to fully grasp the phenomenon and guide effective interventions. Reported reasons range from those perceived as positive, such as seeking pleasure and enhanced sexual experiences, to others linked to structural and psychosocial challenges, including HIV-related stigma, internalized homophobia, serophobia, and coping with emotional distress. These latter factors are more strongly associated with problematic patterns and adverse outcomes, emphasizing the need for approaches that address both behavioral and psychosocial dimensions.ref. 12, ref. 13, ref. 14 Despite its significant health implications, the timing, onset, and patterns of chemsex engagement across settings remain poorly defined, limiting the knowledge in the field, development of targeted interventions and evidence generation.ref. bib15
Given the heightened risk of HIV acquisition in adult cisgender GBMSM, this group is critical target for the scale-up of prevention strategies, including HIV pre-exposure prophylaxis (PrEP). The use of PrEP has demonstrated high efficacy in reducing the risk of HIV transmission among GBMSM and is currently widely recommended as a core component of HIV prevention packagesref. bib16 through oral and injectable options that offer flexibility to accommodate diverse needs and lifestyles. However, global scale up remains limited,ref. bib17 with a recent global meta-analysis estimating that only 11–16% of GBMSM had used PrEP according to available data,ref. bib18 and the 2025 UNAIDS Global AIDS Update likewise noting that PrEP coverage remains far below international targets.ref. bib19
With the global expansion of HIV prevention strategies, including PrEP,ref. bib20 targeting adult cisgender GBMSM, and the increasing use of chemsex,ref. bib21 a growing body of literature explores the intersection between chemsex engagement and PrEP uptake in this group. Because individuals who engage in chemsex frequently meet behavioral eligibility criteria for PrEP, an association between chemsex and PrEP use is plausible. However, to date, the field lacks a summary of the published evidence that offers a global perspective. Therefore, this systematic review and meta-analysis aim to synthesize available evidence on PrEP use among adult cisgender GBMSM who engage in chemsex, estimating the prevalence of PrEP use and assessing whether chemsex engagement is associated with higher odds of PrEP use compared to those who do not engage in chemsex.
Methods
Study design
This systematic review with meta-analysis followed the guidelines provided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (2020 PRISMA-P).ref. bib22 The review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration ID CRD42024573871.
Search strategy
The search strategy was co-designed with the assistance of a scientific information specialist librarian from the University of Zurich medical library. The electronic databases Medline (via Ovid), Embase (via Elsevier), Cochrane Reviews and CENTRAL (via Cochrane Library/Wiley), APA PsycInfo (via EBSCOhost), Scopus (via Elsevier), and LILACS (via VHL Regional Portal) were searched using a combination of medical indexing terms and free text terms for the concepts “men who have sex with men”, “chemsex”, and “pre-exposure prophylaxis” including related phrases and synonyms. For the concept “pre-exposure prophylaxis”, specific therapy names were tested but ultimately not included in the search strategy, to avoid bias. The concepts included in the PICO question and full search strategy are reported in eTable 1 and eTable 2. Literature search was initially performed on December 4th, 2024, and updated on July 1st, 2025, except for LILACS which was not accessible on that date. Search results from each database were exported, uploaded individually, and deduplicated using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia).ref. bib23 No dates, geography, or language restrictions were applied during the search or selection process. Additionally, backward and forward reference search was conducted.
Study selection criteria
The studies selection criteria followed the Population, Intervention, Comparison, and Outcome (PICO) design (eTable 1). We included cross-sectional studies involving HIV-negative adult cisgender GBMSM reporting at least once or current chemsex practices (self-reported) and PrEP use. Our comparator encompassed adult cisgender GBMSM who reported no engagement in chemsex practices and use PrEP. Only studies reporting quantitative data were included; studies without quantitative outcomes relevant to the review were excluded at full-text screening. Reviews, case reports, randomized controlled trials, and editorials were excluded. Gray literature sources, such as preprints or conference abstracts, were also excluded. Before formal screening, a pilot calibration exercise was conducted in which all reviewers independently screened a sample of studies to test, redefine, and align on the eligibility criteria. Two independent reviewers screened titles and abstracts, and performed full text review (JGM, SAG). Discrepancies were solved through discussion involving a third reviewer (JGM, SAG, LGF).
Definition of exposure and outcome
The studies included different definitions for chemsex practices (exposure) and PrEP use (outcome). The definitions of chemsex have evolved over time and vary considerably across studies, reflecting differences in drug use patterns, sexual contexts, and regional terminology. The growing role of digital platforms in facilitating encounters has also contributed to the evolving nature of chemsex.ref. bib24 Broadly, chemsex refers to the intentional use of specific non-prescription substances, most commonly methamphetamine, GHB/GBL, and mephedrone, to initiate, enhance, or prolong sexual encounters. However, the scope of the term expanded in recent years to include a wider range of substances and behaviors. In different settings, various terms are used to describe similar practices, for instance, party and play (PnP) in the United States, ice parties or high fun in Southeast Asia, chills in Spain or festinha in Brazil and fiesta química in some parts of Latin America and the Caribbean. Given the lack of a standardized definition across the literature, for this review, we included studies that used different definitions of chemsex, provided that the core components were present: intentional drug use of typical chemsex drugs for the purpose to enhance sexual encounters among GBMSM and clearly were differentiated from other patterns of substance use. As such, we included studies that explicitly described chemsex practices and studies that referred to chemsex implicitly, where the term chemsex was not alluded to, however, they reported the use of drugs typically associated within sexual contexts. Regarding the timeframe of chemsex, participants self-reported their last engagement over heterogeneous periods of time, ranging from the previous 3 months to at some point in their lifetime, or without a specified period. For the purpose of this review, chemsex engagement was classified as either recent chemsex (reported within the past 6 months) or ever engaged in chemsex (hereafter referred to as “ever chemsex”), which included all other reported periods such as 12 months, 18 months, lifetime, or unspecified timing. This latter category may also include individuals who engaged in chemsex more recently, although this could not be distinguished based on the available data. PrEP use was typically described as the use of oral Tenofovir-based PrEP or long-acting injectable PrEP (cabotegravir). The studies differed in how PrEP use was reported, including daily oral, on-demand, injectable, or even informal use. For the purpose of this review, PrEP uptake was recorded when the participants self-reported use of any modality of PrEP. Continuation, adherence, or re-initiation of PrEP was not analyzed.
Data extraction
A standardized data extraction form was used to collect information from the included studies. Study data were collected and managed using REDCap electronic data capture tools hosted at Hospital Clínic Barcelona.ref. bib25 One reviewer (SAG) conducted the data extraction, and a second reviewer (JGM) cross-verified all extracted data. None of the included studies required translation. We collected the following information: first author, publication year and journal, study design, country, setting, study population, study period, definition and timeframe for chemsex exposure, definition of PrEP and timeframe of use when available, and study primary endpoint. We extracted the number of participants that reported using chemsex and PrEP, and those who did not report using chemsex or PrEP when participants answered both questions. Where available, we extracted unadjusted effect measures using odds ratios (OR), along with their 95% confidence intervals. If OR was not reported, we used extracted data and calculated the unadjusted OR. Additionally, we documented covariates included in adjustments. For studies that presented only p-values without corresponding OR, we computed unadjusted effect measures when sufficient data were available. If key data were missing or unclear, study authors were contacted. In cases where no response was received, the limitation was documented, and the study was excluded from the quantitative synthesis.
Quality assessment of studies
We assessed study quality using the Newcastle–Ottawa Scale (NOS) quality assessment tool adapted for observational, cross-sectional studies.ref. bib26 Studies were evaluated based on three broad criteria: selection of study groups (up to 5 points), comparability of groups (up to 1 point) and ascertainment of exposure or outcomes (up to 3 points) with a maximum possible score of 9 (eTable 3). Two reviewers independently evaluated each study, and discrepancies were resolved with a third reviewer (JGM, SAG, LGF). Based on the NOS point system, we assigned an overall quality rating as low = 0–3, moderate = 4–6 or high = 7–9.
Statistical analysis and meta-analyses
A meta-analysis of prevalence estimates of PrEP use among individuals engaged in chemsex was first conducted using a logistic-normal random-effects model to account for between-study heterogeneity. The Freeman-Tukey double arcsine transformation was applied to stabilize variance, and pooled prevalence estimates with 95% Clopper-Pearson exact confidence intervals were back-transformed for interpretation. Statistical heterogeneity was tested using the I2 statistic, which describes the percentage of total variation in the effect sizes across studies due to heterogeneity rather than chance. I2 values up to 25% indicate no heterogeneity; 25%–50%, low; 50%–75%, moderate and 75%–100%, high heterogeneity.ref. bib27 Potential publication bias in the prevalence meta-analysis was evaluated using a DOI plot and the Luis Furuya-Kanamori (LFK) index.ref. bib28 The DOI plot provides a visual assessment of asymmetry, while the LFK index quantifies the degree of asymmetry: an LFK index < ±1 indicates no asymmetry and suggests no evidence of publication bias; values between ±1 and ±2 reflect minor asymmetry, indicating possible minor publication bias; values greater than ±2 denote major asymmetry, suggesting substantial publication bias may be present. Subsequently, a meta-analysis of ORs for PrEP use among individuals engaged in chemsex versus those not engaged was performed using a random-effects model based on restricted maximum likelihood. Results were displayed in a forest plot. Publication bias was assessed using a funnel plot and Harbord’s test for small-study effects. To explore potential sources of heterogeneity, meta-regression analysis was conducted using selected study-level covariates: study publication year, country income group, world region and timeframe of chemsex exposure (recent versus ever), as moderators.
Subgroup analyses were also performed by timeframe of chemsex exposure to compare prevalence and associations across these groups. The study year refers to the year of publication. The world region where the study was undertaken was defined following UNAIDS classificationref. bib29: Asia and the Pacific, eastern and southern Africa, eastern Europe and central Asia, Latin America and the Caribbean, Middle East and North Africa, western and central Africa and, western and central Europe and North America. Country income groups were defined according to the World Bank classificationref. bib30 as high-income countries (HICs) and low- and middle-income countries (LMICs). The model included both within- and between-study variability, and heterogeneity explained was assessed using the adjusted R2. A test of residual heterogeneity was also performed. Additionally, a leave-one-out sensitivity analysis was conducted to identify influential studies. All tests were two-tailed, and statistical significance was set at p < 0.05. Statistical analyses were performed using Stata version 19.ref. bib31
Ethics statement
This study is a systematic review and meta-analysis of previously published, anonymized data. As no primary data were collected and no individual-level identifiable information was accessed, ethics approval was not required.
Informed consent
Informed consent was not required for this study because it involved secondary analysis of data from published studies only.
Role of the funding source
This study received financial support for publication fees from the Research Group of the HIV Unit, Infectious Diseases Division, Department of Medicine, Geneva University Hospitals, Geneva, Switzerland. The Covidence membership and the fees for the academic librarian who developed the systematic search strategy were sponsored by the Research Group of the HIV Unit, Infectious Diseases Service, Hospital Clínic, and IDIBAPS, University of Barcelona, Barcelona, Spain. No additional funding was received for this study. The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
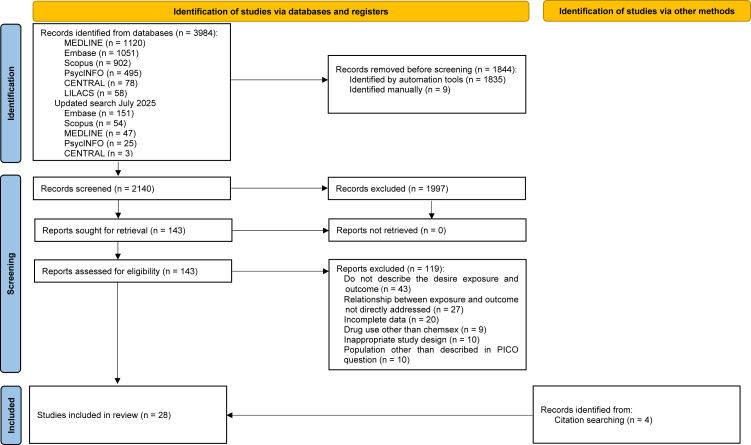
The search strategy identified 3984 records from electronic databases. Following the removal of 1844 duplicates, a total of 2140 records were screened by titles and abstracts. Of these, 1997 were excluded. The remaining 143 full-text articles were reviewed, of which 119 did not meet the eligibility criteria. A total of 42 authors were contacted; 12 provided the requested data, of which 10 met the inclusion criteria. An additional 4 articles were identified via citation searching. A total of 28 studies were finally included in this review, as outlined in the PRISMA flow diagram (Fig. 1). Reasons for exclusion are presented in eTable 4.
Characteristics of included studies, participants and quality of studies
Table 1 provides a summary of the 28 included studies, all (100%)ref. 32, ref. 33, ref. 34, ref. 35, ref. 36, ref. 37, ref. 38, ref. 39, ref. 40, ref. 41, ref. 42, ref. 43, ref. 44, ref. 45, ref. 46, ref. 47, ref. 48, ref. 49, ref. 50, ref. 51, ref. 52, ref. 53, ref. 54, ref. 55, ref. 56, ref. 57, ref. 58, ref. 59 were observational and cross-sectional, in the form of surveys. 14 studies (50%)ref. bib32,ref. bib33,ref. bib35,ref. bib36,ref. 39, ref. 40, ref. 41, ref. 42, ref. 43,ref. bib45,ref. bib49,ref. bib53,ref. bib54,ref. bib58 were conducted in Western and Central Europe and North America (WCENA): Spain (n = 4)ref. bib33,ref. bib45,ref. bib53,ref. bib54, Netherlands (n = 3)ref. bib32,ref. bib40,ref. bib43, United Kingdom (n = 3),ref. bib35,ref. bib41,ref. bib49 France (n = 1),ref. bib42 Italy (n = 1),ref. bib58 Portugal (n = 1),ref. bib39 and United States (n = 1).ref. bib36 12 studies (43%)ref. bib25,ref. bib28,ref. bib35,ref. bib38,ref. bib39,ref. 41, ref. 42, ref. 43,ref. 46, ref. 47, ref. 48,ref. bib50 were held in Asia and the Pacific (AP): China, Hongkong,ref. bib37,ref. bib59 Mainland,ref. bib55 and Taiwanref. bib57 (n = 4), Australia (n = 2),ref. bib34,ref. bib47 Malaysia (n = 2),ref. bib44,ref. bib48 India (n = 1),ref. bib51 New Zealand (n = 1),ref. bib52 Pakistan (n = 1),ref. bib50 and Thailand (n = 1).ref. bib56 Only two studies (7%) occurred in Latin America (LA), both in Brazil (n = 2).ref. bib38,ref. bib46 Of the 28 included studies, 20 (71%) were conducted in high-income settings,ref. 32, ref. 33, ref. 34, ref. 35, ref. 36, ref. 37,ref. 39, ref. 40, ref. 41, ref. 42, ref. 43,ref. bib45,ref. bib47,ref. bib49,ref. 52, ref. 53, ref. 54,ref. 57, ref. 58, ref. 59 and 8 (29%) in low- and middle-income settings.ref. bib38,ref. bib44,ref. bib46,ref. bib48,ref. bib50,ref. bib51,ref. bib55,ref. bib56
Table 1: Characteristics of the included studies.
| Study | Country | Study setting and participants | Study primary endpoint | Study period | Exposure engagement in chemsex | Outcomea PrEP uptake | Sample size | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| First author | Publication year | Definition | Drug reported | Time frame | Definition in study | Time frame | |||||
| Coyer L. | 2018 | Netherlands | Prospective cohort study.HIV-negative MSM participating in Amsterdam Cohort Studies | Trends in PrEP use, PrEP eligibility, and intention to use PrEP | 2015–2017 | Use of drugs during sex with casual partners | GHB/GBL, mephedrone, methamphetamine | 6 months | Daily or event-driven PrEP (self-obtained or via studies) | 6 months and lifetime PrEP use | 687 |
| Valencia J. | 2018 | Spain | Cross-sectional study.HIV-negative MSM who attended ‘Orgullo Gay Madrid 2016″ | Prevalence of drug use and chemsex-related drug use, and associated factors, including PrEP | 2016 | Use of drugs associated with chemsex | GHB/GBL, mephedrone, methamphetamine | 12 months | PrEP use history | Lifetime PrEP use | 666 |
| Hammoud MA. | 2019 | Australia | Prospective cohort study.MSM recruited online participating in the Flux study | Incidence of PrEP uptake, initiation predictors, and characteristics associated with non-uptake | 2014–2017 | Recent drug use to enhance sex | Methamphetamine | 6 months | Daily, “every other day” or event-driven PrEP | Daily, every other day, or before and after sex | 1257 |
| Hanum N. | 2020 | UK | Prospective cohort study.HIV-negative or of unknown HIV status MSM participating in the AURAH2 study | PrEP and PEP awareness and use among HIV-negative MSM and predictors of PrEP initiation | 2013–2018 | Use of at least one chemsex-related drug | Crystal methamphetamine, γ-hydroxybutyrate (GHB), γ-butyro- lactone (GBL), or mephedrone | 3 months | PrEP use history | 12 months | 1162 |
| Okafor CN. | 2020 | United States | Observational subanalysis within a randomized clinical trial.Black MSM participating in the HPTN 073 randomized clinical trail | PrEP adherence and initiation in relation to substance use | 2013–2014 | Self-reported use of different drugs before/during CAS | Alcohol, marijuana, inhaled nitrates, cocaine, and methamphetamine | 3 months | Tenofovir-based daily PrEP initiation or continuation | Not specifically reported | 226 |
| Wang Z. | 2020 | China (Hong Kong) | Cross-sectional study.MSM self-reported as HIV-negative or of unknown HIV status | PrEP uptake and willingness among sexualized drug users | April–December 2018 | Sexualized drug use in the last year (types of drugs used, poly-drug use, time since first episode, CAS, frequency, use of drug rehabilitation service) | Ketamine, methamphetamine, cocaine, cannabis, ecstasy, dormicum, Halcion, Erimin 5, hypnotic drugs (non- prescription), heroin, cough suppressant, amyl nitrite GHB/GBL methoxy-N, N-diisopropyltryptamine (Foxy), mephedrone | 12 months | Current use of PrEP, sources of PrEP and methods of PrEP use | Not specifically reported | 580 |
| Blair K. | 2021 | Brazil | Cross-sectional.PrEP-eligible MSM | Current PrEP uptake, and key predictors: HIV knowledge, and internalized homonegativity | February–March 2020 | Illicit substance use before or during sex | Cocaine, crack, basic paste, or oxy; marijuana, hashish, or skank; ecstasy or MD, methamphetamines (crystal or speed); GHB or GBL; poppers; other inhalants; mephedrone; hallucinogens (LSD, mushroom tea) | 6 months | Current use of PrEP | Not specifically reported | 2398 |
| Chone JS. | 2021 | Portugal | Prospective cohort study.MSM recruited online during COVID-19 pandemic | Prevalence and factors associated with chemsex, including PrEP use, during the COVID-19 social distancing | May 2020 | Drug use immediately before and/or during sex | Alcohol, opioids, cannabis, sedatives, cocaine, stimulants, hallucinogens, and poppers | 3 months | Tenofovir-based oral PrEP | Not specifically reported | 1301 |
| Hulstein SH. | 2021 | Netherlands | Cross-sectional study.MSM reporting informal PrEP use | Eligibility for PrEP, intention to use PrEP, informal use of PrEP, chemsex and STI | 2017–2018 | Self-reported use of at least one of the following substances in the context of sex | GHB, methamphetamine, and/or mephedrone | 6 months | Informally obtained Tenofovir-based oral PrEP obtained via acquaintance, online, buyers’ club, on travel, or other options. Used daily and event-driven | 3 months | 5120 |
| Hyndman I. | 2021 | UK | Cross-sectional study.Online survey of HIV-negative MSM attending Dean Street clinic during COVID-19 | Impact of COVID-19 on sexual behavior, and mental well-being. Variables compared by PrEP use | March–June 2020 | Sexualized recreational drug use | Not specifically reported | 3 months | Self-reported PrEP use during lockdown | Not specifically reported | 814 |
| Rollet D. | 2021 | France | Cross-sectional study.MSM attending 6 STI clinics in Paris. | Number of general practitioner visits reported by patients (compared chemsex users and controls). Evaluated PrEP follow-up. | October–December 2018 | Drug use in a sexual context (excluding alcohol, poppers and cannabis) | Tobacco, cocaine, MDMA, crystal, methamphetamine, Cathinones, GHB/GBL, ketamine, opiates, hallucinogens | 12 months | PrEP use history and PrEP follow-up | Not specifically reported | 364 |
| Coyer L. | 2022 | Netherlands | Prospective cohort study. HIV-negative MSM after PrEP-initiation with controls not initiating PrEP | Number of casual partners, proportion engaging in CAS and receptive CAS with casual partners, sexualized drug use, any STI, and anal STI | 2015–2019 | Use of drugs during sex | Mephedrone, methamphetamine, GHB/GBL, ketamine, amphetamine, cocaine, ecstasy/MDMA | 6 months | PrEP initiation, including study contexts and outside the ACS, informal or prescribed PrEP. Used daily and event-driven | Not specifically reported | 858 |
| Eger WH. | 2022 | Malaysia | Cross-sectional study. MSM recruited online | PrEP use and associated factors influencing its uptake | June–July 2020 | Drug use before sexual intercourse | Crystal, methamphetamine, ketamine, ecstasy, and gamma-hydroxybutyrate “G” | 6 months | History of PrEP use, as “Yes” or “No” | Not specifically reported | 355 |
| García-Pérez JN. | 2022 | Spain | Cross-sectional study. MSM who attended a sexual health clinic in Barcelona | Illicit drug and chemsex use, sexual behavior, and STI prevalence; associations between drug use, PrEP use, and STI | January–June 2019 | Any recreational drug use with a sexual purpose independently of the drug type or number of drugs used | Poppers, cannabis, MDMA, cocaine, GHB, amphetamines, ketamine, methamphetamine, mephedrone, LSD | 12 months | PrEP use history | 12 months | 514 |
| Jalil EM. | 2022 | Brazil | Cross-sectional study. HIV-negative MSM recruited online/on-site | Prevalence and predictors of sexualized drug use, including PrEP use, among gender minorities | October–December 2020 | Any use of drug before or during sex | Tobacco, marijuana, cocaine, crack, ecstasy, amphetamines, ketamine, meth, GHB, poppers, other inhalants | 6 months | History or current PrEP use. Daily, event-driven or injectable PrEP (cabotegravir). | Not specifically reported | 3553 |
| MacGibbon J. | 2022 | Australia | Cross-sectional study. HIV-negative MSM recruited online | Factors associated with PrEP use among men in relationships | April–June 2021 | Any recreational drug use with a sexual purpose | MDMA, GHB, Crystal | 6 months | Daily or event-driven current PrEP use | Not specifically reported | 1185 |
| Maviglia F. | 2022 | Malaysia | Cross-sectional study. MSM recruited online | Prevalence and associated factors with chemsex, including PrEP use | August–September 2021 | Any use of drug before or during sex | Ecstasy, crystal, methamphetamine/ice, GHB/GBL, Foxy | 6 months | PrEP knowledge and current, ever use history | Not specifically reported | 870 |
| Ogaz D. | 2022 | UK | Cross-sectional study. HIV-negative/unknown MSM recruited from London commercial venues | PrEP usage patterns and unmet needs | June–August 2019 | Any use of drug before or during sex | Ketamine, GHB/GBL, mephedrone, methamphetamine | 12 months | Self-reported PrEP use | 12 monthsb | 1408 |
| Ali U. | 2023 | Pakistan | Cross-sectional study. HIV-negative MSM recruited online | Knowledge, willingness and history of PrEP use | September–November 2021 | Sex with use of drugs | Amphetamine-type stimulants | 6 months | Knowledge, willingness and history of PrEP use | Not specifically reported | 347 |
| Agarwal H. | 2024 | India | Cross-sectional study. Individuals who reported sex with men recruited via app | PrEP use and awareness | May–June 2022 | Use of “party drugs” | Not specifically reported | Not specified | History or current PrEP use | Not specifically reported | 3116 |
| Andrews S. | 2024 | New Zealand | Cross-sectional study. MSM recruited online | Sexual practice, drug use and sociodemographic, social milieu and behavioral predictors of sexualized drug use | December 2018–February 2019 | Illicit drug use motivated by ‘better sex’ and/or ‘party and play session’ | Cannabis, alkyl nitrite,MDMA, methamphetamine, cocaine, LSD, GHB, amphetamine, other hallucinogen, ketamine, synthetic cannabis, heroin, mephedrone | 6 months | Current use of PrEP | Not specifically reported | 836 |
| Íncera-Fernández D. | 2024 | Spain | Cross-sectional study. MSM recruited via networks and apps | Prevalence and association of sexualized drug use with sexual behaviors, prevention measures for HIV, and STI | Not specified | Intentional use of drugs for sexual purposes | Alcohol, cannabis, cocaine, poppers, ecstasy, erectile dysfunction medication, MDMA, GHB/GBL, meth, mephedrone, ketamine, heroin, benzodiazepines | 18 months | History of PrEP use. Either prescribed or without prescription | 18 months | 493 |
| Moreno-García S. | 2024 | Spain | Cross-sectional study. HIV-negative MSM recruited online. | Daily PrEP prevalence and associated factors | May–July 2020 | Use of drugs within the 6 h prior to or during anal sex | Mephedrone, methamphetamine, GHB, ketamine | Lifetime | Current daily oral PrEP | Not specifically reported | 4692 |
| Sun J. | 2024 | China | Cross-sectional study. MSM recruited online via gay service groups. | Impact of SDU, particularly chemsex, on sexual behavior, HIV/STI infection risk, and the use PrEP among MSM | March–April 2022 | Use of drugs for sexual purposes or in conjunction with sexual activities | Poppers, methamphetamine, ketamine, ecstasy, GHB/GBL | Lifetime | History of PrEP use (type not specified) and willingness to use PrEP. | Lifetimeb | 796 |
| Boonruang J. | 2025 | Thailand | Longitudinal study. MSM in Bangkok, recruited from healthcare setting | Prevalence and patterns of amphetamine-type stimulant use among MSM, and associated factors (including PrEP use) | January 2018–May 2019 | Sex with use of drugs | Amphetamine-type stimulants use | 6 months | History and willingness to use PrEP | 6 months | 1375 |
| Mayo D. | 2025 | China (Taiwan only) | Cross-sectional study. HIV-negative/unknown MSM recruited online | PrEP engagement and its predictors, including chemsex | April–May 2023 | Use of drugs immediately before or during sex | Methamphetamine, poppers, GHB/GBL, ketamine, methcathinone/mephedrone | 6 months | PrEP use and continuation | 12 months | 284 |
| Pessina R. | 2025 | Italy | Cross-sectional study. MSM recruited online via LGBT + community settings and sexual health services in Italy. | Epidemiological profile of chemsex and related psychological and health factors | March–June 2023 | Use of psychoactive substances, typically through oral or inhalation routes, during sexual activity | Mephedrone, GHB/GBL, methamphetamine | Lifetime | History of PrEP use | Not specifically reported | 841 |
| Wong N. | 2025 | China (Hong Kong only) | Cross-sectional study. PrEP-naïve and PrEP-experienced MSM recruited online through NGOs. | Interrelationship between chemsex engagement and PrEP use | February 2022–January 2024 | Use of drugs with or without other sexualized drugs before or during sex | Methamphetamine and/or GHB | Lifetime | History of PrEP use | Lifetime or recent | 338 |
HIV: human immunodeficiency virus; GBMSM: gay, bisexual and other men who have sex with men; GHB: gamma hydroxybutyrate; GBL: gamma butyrolactone; PrEP: Pre-exposure prophylaxis; PEP: post-exposure prophylaxis; CAS: condomless anal sex; STI: sexually transmitted infections; MDMA or MD: methylenedioxy-methylamphetamine. LSD: Lysergic Acid Diethylamide.
Transgender and non-binary people were excluded from this study, according to exclusion and inclusion criteria of the present study.
With regards to the chemsex practices, a total of 17 (61%) studiesref. bib32,ref. bib33,ref. bib35,ref. 39, ref. 40, ref. 41, ref. 42,ref. 44, ref. 45, ref. 46, ref. 47, ref. 48,ref. bib50,ref. bib54,ref. 57, ref. 58, ref. 59 explicitly described the use of chemsex; and 11 (39%) studiesref. bib34,ref. 36, ref. 37, ref. 38,ref. bib43,ref. bib49,ref. 51, ref. 52, ref. 53,ref. bib55,ref. bib56 referred to it implicitly. Studies also captured the timeframe of chemsex: 17 (61%) studies reported recent chemsexref. bib32,ref. 34, ref. 35, ref. 36,ref. 38, ref. 39, ref. 40, ref. 41,ref. bib43,ref. bib44,ref. 46, ref. 47, ref. 48,ref. bib50,ref. bib52,ref. bib56,ref. bib57, among these: 4 (14%)ref. bib35,ref. bib36,ref. bib39,ref. bib41 and 13 (46%)ref. bib32,ref. bib34,ref. bib38,ref. bib40,ref. bib43,ref. bib44,ref. 46, ref. 47, ref. 48,ref. bib50,ref. bib52,ref. bib56,ref. bib57 included participants who engaged in chemsex in the previous 3 and 6 months, respectively. 11 studies reported ever chemsex timeframesref. bib33,ref. bib37,ref. bib42,ref. bib45,ref. bib49,ref. bib51,ref. 53, ref. 54, ref. 55,ref. bib58,ref. bib59: 5 (18%)ref. bib33,ref. bib37,ref. bib42,ref. bib45,ref. bib49 and one (4%)ref. bib53 studies included participants who engaged in chemsex in the previous 12 and 18 months, respectively. Also, one (4%) studyref. bib51 included participants who engaged in chemsex in a non-specified period, and 4 studies (14%)ref. bib54,ref. bib55,ref. bib58,ref. bib59 included participants that reported use of chemsex in their lifetime (unspecified). All studies (100%) reported oral Tenofovir-based PrEP use, and one (4%) studyref. bib46 also referred to long-acting injectable PrEP (cabotegravir). None of the studies explicitly reported frequency, dosage, or patterns of chemsex use.
In total, 36,339 HIV-negative adult cisgender GBMSM were included across all the studies. The studies where participants reported recent chemsex contributed with 22,531 individuals while the studies where participants reported ever chemsex timeframes contributed with 13,808 individuals. A total of 5690 of the total 36,339 (16%) participants reported chemsex, and 5881 out of 36,339 (16%) participants reported the use of PrEP.
With regards to the quality of the evidence, of the 28 studies, 9 (32%) were rated as low quality,ref. bib36,ref. bib38,ref. bib41,ref. bib44,ref. 50, ref. 51, ref. 52,ref. bib57,ref. bib59 19 (68%) as medium quality.ref. 32, ref. 33, ref. 34, ref. 35,ref. bib37,ref. bib39,ref. bib40,ref. bib42,ref. bib43,ref. 45, ref. 46, ref. 47, ref. 48, ref. 49,ref. 53, ref. 54, ref. 55, ref. 56,ref. bib58 Overall scores ranged from 1 to 6, with a median of 4.5. The most frequent methodological limitations were observed in the Selection domain, particularly regarding response rates, which were satisfactory in only 2 studies (7%)ref. bib33,ref. bib56 and, to a lesser extent, concerns about the representativeness of cases, which was adequate in 13 studies (46%).ref. bib32,ref. bib33,ref. 35, ref. 36, ref. 37,ref. bib40,ref. bib42,ref. bib43,ref. bib45,ref. bib46,ref. bib49,ref. bib55,ref. bib56 In the Comparability domain, only 10 studies (36%)ref. bib37,ref. bib39,ref. bib42,ref. bib45,ref. bib46,ref. bib48,ref. bib52,ref. bib53,ref. bib55,ref. bib59 adequately controlled potential confounders. In the Outcome domain, scores were generally higher (median 2, range 1–2), particularly for outcome assessment, although all studies 28 (100%) relied exclusively on self-reported measures; reporting of statistical tests was clearly described and appropriate in most studies 22 (79%).ref. 32, ref. 33, ref. 34, ref. 35,ref. 37, ref. 38, ref. 39, ref. 40, ref. 41, ref. 42, ref. 43, ref. 44, ref. 45, ref. 46, ref. 47, ref. 48,ref. 53, ref. 54, ref. 55, ref. 56, ref. 57, ref. 58 Study quality assessments are summarized in eTable 3.
Prevalence of PrEP use among adult cisgender GBMSM engaging in chemsex
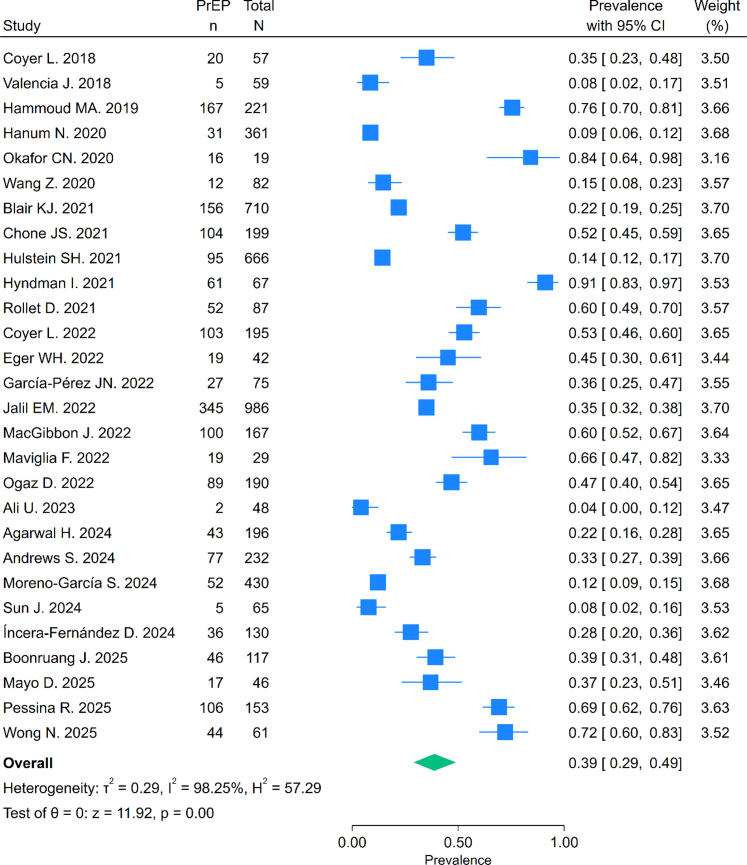
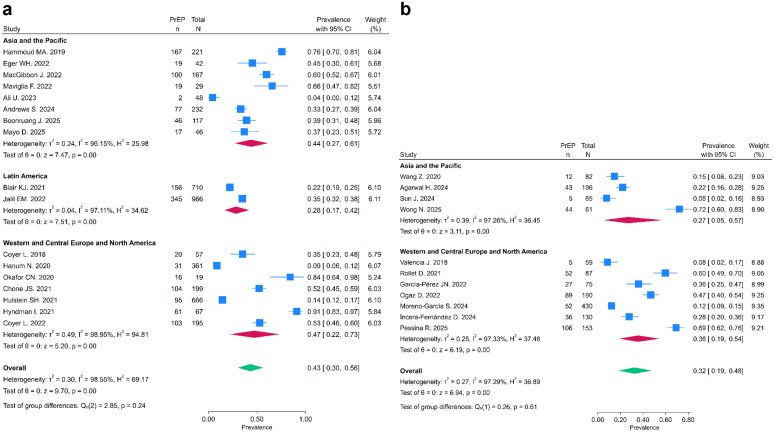
The pooled prevalence of PrEP use was 39% (95% CI: 29–49%) (Fig. 2). We found no statistically significant difference between recent chemsex engagement with ever timeframes of engagement (Fig. 3). The leave-one-out sensitivity analysis indicated that no single study substantially influenced the pooled prevalence estimates (eFig. 1). Meta-regression analyses for recent and ever chemsex exposure timeframes and study year, country income group, or world region found no statistical difference in the prevalence of PrEP use (p > 0.05), and these covariates explained very little of the between-study variance. Heterogeneity remained high (I2 > 97%) across all analyses (eTable 5 and eTable 6).
Chemsex and odds of PrEP use among adult cisgender GBMSM
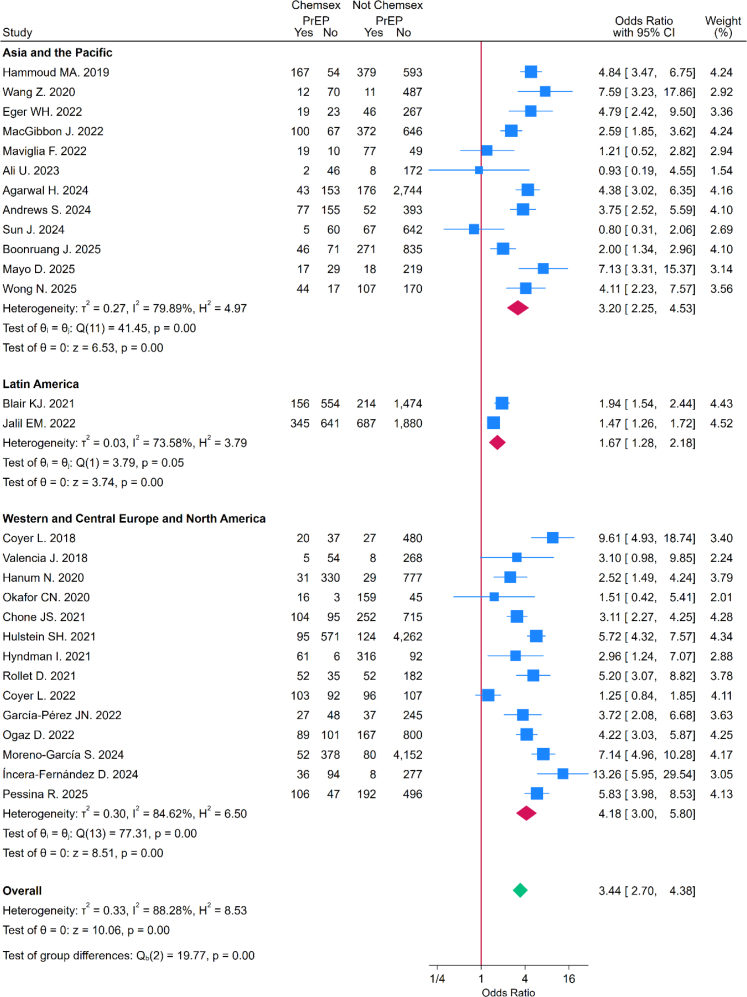
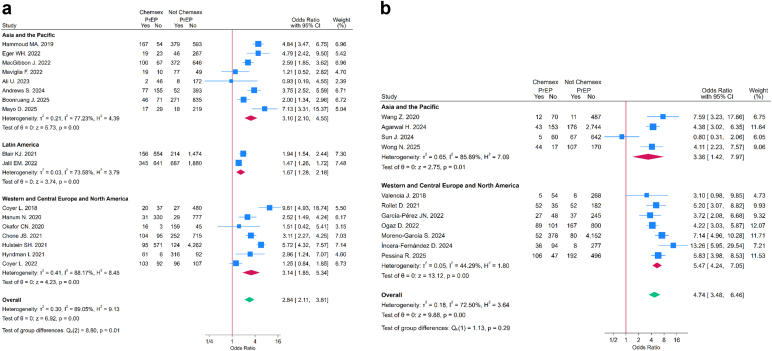
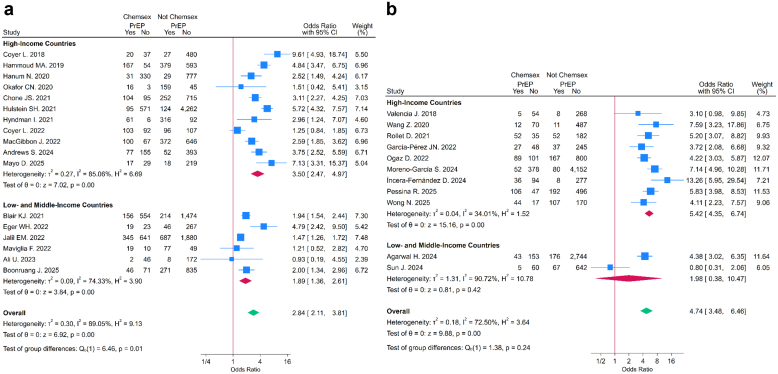
The pooled OR indicated that chemsex exposure was associated with higher odds of PrEP use (OR = 3.44, 95% CI: 2.70–4.38) (Fig. 4). In subgroup analyses by timing of chemsex engagement, the association with PrEP use was greater among those reporting ever chemsex (OR = 4.74, 95% CI: 3.48–6.46) compared with those reporting recent chemsex (OR = 2.84, 95% CI: 2.11–3.81). This difference was statistically significant (test for subgroup differences: p = 0.019) (Fig. 5), (eTable 7). The leave-one-out analysis indicated that no single study substantially influenced the pooled ORs (eFig. 2). The meta-regressions with country income group as moderator were statistically significant for both recent (OR = 0.54, 95% CI: 0.31–0.94; p = 0.031) and ever chemsex timeframes (OR = 0.46, 95% CI: 0.21–0.99; p = 0.046), indicating that in LMICs, the association between chemsex and PrEP uptake was weaker compared to HICs (Fig. 6) (eTable 8 and eTable 9). None of the other moderators were statistically significant in either group (p > 0.05), and they explained little of the between-study variance. Heterogeneity remained moderate to high (I2 > 70%) across all analyses.
Small-study effects and publication bias
The PrEP use prevalence meta-analyses showed minor asymmetry for the overall estimate (eFig. 3) and major asymmetry for both recent and ever chemsex engagement (eFig. 4), suggesting possible small-study effects or selective publication bias, particularly in the time-specific subgroups. In contrast, the chemsex–PrEP association meta-analyses showed no evidence of small-study effects or publication bias, either in the overall analysis (eFig. 5) or in the time-specific subgroups (eFig. 6).
Discussion
This is the first systematic review and meta-analysis to provide a global summary of the interplay between chemsex practice and PrEP use in adult cisgender GBMSM, addressing a critical gap in the literature to optimize HIV prevention in this population. A total of 28 studies, including 36,339 participants, from three world regions were collated. Across all studies, 39% of GBMSM who engaged in chemsex reported the use of PrEP. This estimate is higher than the 11–16% PrEP use reported in a previous global meta-analysisref. bib60 of MSM, although differences in study populations, definitions, and lack of disaggregated data in earlier studies limit direct comparison, as that review did not specifically evaluate adult cisgender GBMSM who engage in chemsex. GBMSM who reported engagement in chemsex were over three times more likely to report the use of PrEP compared to those who did not engage in chemsex. Additionally, studies conducted in LMICs reported significantly lower odds of PrEP use in this group compared with those in HICs.
With respect to chemsex timeframes, the association with PrEP use was stronger among individuals reporting ever chemsex than recent engagement, which may partly reflect the longer exposure window captured by ever chemsex. A number of factors may play a role in this result, determining a shift in the risk perception or access to PrEP services. Individuals with past or unspecified chemsex engagement may have had more opportunities to initiate PrEP or may represent a subgroup with more sustained engagement in healthcare. This association may also reflect contextual factors, including greater health-seeking behavior among some individuals who engage in chemsex and the wider availability of PrEP in urban sexual health services where chemsex is more frequently reported, although the cross-sectional evidence does not allow these influences to be disentangled. Conversely, those reporting recent chemsex may face more acute barriers to PrEP access, or less perception of risk. Despite the robust association observed, the published studies are limited to local surveys with high heterogeneity across them, such as differences in study design, population characteristics, definitions of chemsex, and healthcare systems. These results therefore need to be interpreted with caution, as they reflect studies published between 2018 and July 2025, a period during which PrEP availability and access varied substantially across countries and regions and remained below global targets.ref. bib19 Similarly, the lower odds of PrEP use in GBMSM observed in studies from LMICs may be a result by legal restrictions, health system challenges, and social barriers.ref. bib61 In settings where laws criminalize same–sex relations or drug use can discourage individuals from seeking care, limiting access to PrEP, and obscuring the reach of these practices. Chemsex is associated with high-risk sexual behaviors and drug use patterns, that can lead to severe sexual and mental health and social consequences. Studies among GBMSM living with HIVref. bib62,ref. bib63 report poorer treatment adherence among individuals engaging in chemsex or SDU. Although these findings concern HIV treatment rather than prevention, they highlight behavioral and psychosocial factors that may similarly impede consistent PrEP use. Motivations described for the practice range from pleasure-seeking to coping with stigma and emotional distress, with psychosocial factors strongly linked to problematic patterns and adverse outcomes.ref. 12, ref. 13, ref. 14 In this regard, the conceptual framework proposed in The problematic chemsex journey (2019)ref. bib64 describes a six-stage progression from feelings of loneliness and emptiness to problematic chemsex. This model emphasizes the importance of addressing both behavioral and psychosocial dimensions to prevent escalation and guide effective interventions highlighting the importance of interventions addressing both behavioral and psychosocial dimensions. Providing services to GBMSM who engage in chemsex practices remains a global challenge that needs addressing stigma, cultural sensitivities, financial and structural barriers, strengthening health workers’ capacity, infectious disease prevention (including hepatitis C), harm reduction, and mental health care,ref. bib65 especially in LMICs. Conventional drug services, largely designed for opioid or alcohol dependence, often lack cultural competence and relevance for GBMSM, underscoring the importance of multidisciplinary approaches in partnership with community organizations and peers. A recent systematic review of harm reduction strategiesref. bib66 revealed that interventions for chemsex among MSM include a web-based programs, peer-led support, and mobile health services. Digital interventions, such as mindfulness-based cognitive approaches and harm reduction platforms, improve self-efficacy and promote safer practices, while peer-led programs, particularly those facilitated by individuals with lived experience, demonstrate greater engagement and abstinence rates. Mobile health initiatives, such as distributing safer sex and drug use kits, have also proven beneficial. While some GBMSM engaging in chemsex may use PrEP as part of proactive health-seeking behavior, PrEP alone does not address the broader physical, psychological, and social harms associated with chemsex. In addition, a recent studyref. bib67 describes the implementation of a multidisciplinary approach for people living with HIV who engage in chemsex, showing a positive impact on substance use and enabling the identification of unmet needs and vulnerable subgroups, such as migrants, individuals who practice slam, and sex workers, who still require targeted interventions. HIV, sexual health, and harm reduction services should routinely incorporate PrEP and chemsex care. In this context, the 2025 WHO guidelines expanding the HIV prevention toolkit with long-acting injectable lenacapavir, administered only twice yearly, represent a transformative step for GBMSM at risk of HIV, particularly those facing challenges with daily adherence, stigma, or limited healthcare access.ref. bib68 Despite the overall variability, our findings were consistent across settings and world regions, suggesting that the association between chemsex and PrEP uptake among adult cisgender GBMSM is not context-specific but a global phenomenon.
Studies lacked detailed descriptions of chemsex use and behavioral patterns, such as frequency, dose, or mode of administration (e.g., intravenous use or slamsex).ref. bib58 The timeframe of the use of chemsex was often loosely categorized and was reported by the study participants. Similarly, the definitions of PrEP use across included studies were also heterogeneous, ranging from current reported use to ever PrEP use, and, in some cases, informalref. bib40 or off-prescription use.ref. bib53 All studies reported oral PrEP use, and only one study reported injectable PrEP with cabotegravir.ref. bib46 This reflects the evolution of clinical guidelines and the historical availability of PrEP formulations for this group.ref. bib16 The lack of standardized definitions and variability across studies limit the ability to fully understand the interplay between chemsex and PrEP use in GBMSM,ref. bib69 considering that different chemsex patterns may shape prevention needs and affect PrEP uptake and continuation in this group.ref. bib70
This review has several strengths, including a comprehensive search across major databases without language or time restrictions, systematic literature quality assessment, and the use of subgroup, sensitivity, and meta-regression analyses. However, important limitations should be considered. Although the search was comprehensive, relevant studies may have been missing if not indexed or unpublished. All included studies were observational, cross-sectional reports, which preclude establishing causality or temporality, and their overall methodological quality was low to moderate. Reliance on self-reported information regarding use of chemsex or PrEP in participants introduces risks of recall error and social desirability bias. Variability in measurement of chemsex and PrEP definitions reduced comparability across studies and likely contributed to the heterogeneity observed. In addition, evidence of possible small-study effects or publication bias was detected in the prevalence analyses, which may have led to overestimation of pooled prevalence. In many reports, the odds of PrEP use among chemsex-engaged GBMSM were presented as secondary findings, increasing the risk of selective reporting. Because the included studies span multiple years and a limited number of countries, our pooled prevalence should not be interpreted as reflecting current global PrEP uptake, and temporal and regional variability further limits generalizability. Geographic representation was uneven, with greater weight from high-income settings and no studies from regions with a high HIV burden, such as sub-Saharan Africa, limiting the generalizability, and highlighting the need to generate global evidence in the field. In particular, estimates for LA and for AP were derived from a small number of studies, and should therefore be interpreted with caution. More fundamentally, the number of studies that report both chemsex and PrEP uptake remains very limited globally, which reflects a structural evidence gap rather than a search limitation, as relevant information may exist only in gray literature, which was excluded. Moreover, our review focused on estimating prevalence and associations rather than characterizing individual profiles of GBMSM engaging in chemsex, as most included studies provided limited disaggregated data beyond exposure and outcome measures. While these limitations warrant caution, in a context where randomized trials are not feasible, this synthesis of standardized observational evidence becomes essential to inform practice and global policy recommendations.
Important evidence gaps remain.ref. bib71 Future studies should adopt standardized definitions of chemsex and PrEP to improve comparability, with consensus on a core set of indicators including standard terminology, substance descriptions, frequency, patterns, and timeframe of chemsex exposure, as well as standardized reporting of PrEP options, including initiation and continuation of PrEP use.ref. bib72 Additionally, future research should prioritize prospective longitudinal studies to clarify the temporal relationship between chemsex and PrEP initiation and continuation. Qualitative and mixed-methods research is needed to capture lived experiences, motivations, and barriers that may explain heterogeneity across settings and will be critical to strengthen the evidence base in the field. Research should also move beyond prevalence estimates to better characterize GBMSM engaging in chemsex, considering age, migration status, and socioeconomic position. Age-stratified analyses, in particular, would be valuable to capture differences in patterns of chemsex practice and prevention needs across the course of life. Other populations with distinct vulnerabilities, patterns of chemsex practice, and different barriers or facilitators to prevention, such as transgender people and minor GBMSM, also warrant dedicated investigation.ref. bib73 Finally, geographic coverage for evidence generation must be extended to underrepresented regions, as current evidence comes predominantly from high-income settings, with significant areas missing, such as sub-Saharan Africa and the Middle East and North Africa.ref. bib74 Scaling up integrated PrEP provision with comprehensive harm reduction and broader health promotion efforts for GBMSM across settings and cultures, with particular attention to LMICs, can significantly improve health outcomes for this population and contribute to the global HIV elimination goals.
Contributors
JGM and LGF conceived the idea for the review, designed and coordinated the study. JGM, SAG, and LGF acquired data, screened records, extracted data, and assessed the quality of the evidence. EDL conducted data analysis. JGM, SAG, and LGF wrote the first draft of the manuscript. EDL, FJMC, LM, ML, JM, MMR, and AC gave crucial intellectual input and provided critical revisions in the manuscript. JGM, SAG and LGF have verified the underlying data and had the final responsibility for the decision to submit for publication. All authors had full access to all the data in the study and approved the final version of the manuscript. JGM and LGF managed the project timelines and coordinated tasks among the research team.
Data sharing statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of interests
ML has received institutional research funding and speaker honoraria from ViiV Healthcare, Gilead Sciences, and Janssen, and has participated in advisory boards for Janssen and Gilead Sciences.
JM has received payments for expert testimony from MSD, ViiV Healthcare, Gilead Sciences, and Janssen, and the HIV Unit in which he works has received institutional research funding from these companies.
AC works in an HIV Unit that receives institutional funding for industry-sponsored trials from ViiV Healthcare, MSD, and Gilead Sciences.
All other authors declare no competing interests.
References
- 1The Urgency of Now: AIDS at a Crossroads. Geneva: Joint United Nations Programme on HIV/AIDS2024Licence: CC BY-NC-SA 3.0 IGO
- 2UNAIDS Key Population Groups, Including Gay Men and Other Men Who Have Sex With Men, Sex Workers, Transgender People, People Who Inject Drugs and Prisoners and Other Incarcerated People2024Joint United Nations Programme on HIV/AIDS (UNAIDS)Geneva, Switzerland
- E.L. Korenromp, K. Sabin, J. Stover. New HIV infections among key populations and their partners in 2010 and 2022, by world region: a multisources estimation. J Acquir Immune Defic Syndr, 2024. [PubMed]
- Global AIDS monitoring, 2020–2024
- Y.J. Evers, G.A.F.S. Van Liere, C.J.P.A. Hoebe, N.H.T.M. Dukers-Muijrers. Chemsex among men who have sex with men living outside major cities and associations with sexually transmitted infections: a cross-sectional study in the Netherlands. PLoS One, 2019. [DOI]
- E. Mundy, A. Carter, T. Nadarzynski, C. Whiteley, R.O. de Visser, C.D. Llewellyn. The complex social, cultural and psychological drivers of the ‘chemsex’ experiences of men who have sex with men: a systematic review and conceptual thematic synthesis of qualitative studies. Front Public Health, 2025
- S. Maxwell, M. Shahmanesh, M. Gafos. Chemsex behaviours among men who have sex with men: a systematic review of the literature. Int J Drug Policy, 2019. [PubMed]
- A. Bourne, D. Reid, F. Hickson, S. Torres-Rueda, P. Weatherburn. Illicit drug use in sexual settings (‘chemsex’) and HIV/STI transmission risk behaviour among gay men in South London: findings from a qualitative study. Sex Transm Infect, 2015. [PubMed]
- M. Pakianathan, W. Whittaker, M.J. Lee. Sexualised drug use (chemsex) and its association with health outcomes in men who have sex with men: a cross-sectional study in South London clinics. BMJ Open, 2020. [DOI]
- M.P. Hibbert, A. Hillis, C.E. Brett, L.A. Porcellato, V.D. Hope. A narrative systematic review of sexualised drug use and sexual health outcomes among LGBT people. Int J Drug Policy, 2021
- D. Íncera-Fernández, M. Gámez-Guadix, S. Moreno-Guillén. Mental health symptoms associated with sexualized drug use (Chemsex) among men who have sex with men: a systematic review. Int J Environ Res Publ Health, 2021
- C. Protiere, A. Sow, V. Estellon. Diversity of chemsex experiences among men who have sex with men: results from the French ANRS PaacX Study using Q-Methodology. Arch Sex Behav, 2025 Mar 1. [PubMed]
- P. Weatherburn, F. Hickson, D. Reid, S. Torres-Rueda, A. Bourne. Motivations and values associated with combining sex and illicit drugs (chemsex) among gay men in South London: findings from a qualitative study. Sex Transm Infect, 2017. [PubMed]
- N. Georgiadis, A. Katsimpris, M.A. Vatmanidou, T. Vassilakou, A. Beloukas, T.N. Sergentanis. Prevalence of chemsex and sexualized drug use among men who have sex with men: a systematic review and meta-analysis. Drug Alcohol Depend, 2025
- M. Coronado-Muñoz, E. García-Cabrera, A. Quintero-Flórez, E. Román, Á. Vilches-Arenas. Sexualized drug use and chemsex among men who have sex with men in Europe: a systematic review and meta-analysis. J Clin Med, 2024
- 16World Health OrganizationConsolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring: recommendations for a public health approach2021World Health OrganizationGeneva
- 17World Health OrganizationGuidelines on long-acting injectable cabotegravir for HIV prevention2022World Health OrganizationGeneva
- Y. Huang, R. Tian, Z. Zhou. HIV pre-exposure prophylaxis use on a global Scale among men who have sex with men: a systematic review and meta-analysis. AIDS Patient Care STDS, 2023 Apr 1. [PubMed]
- 19UNAIDSGlobal AIDS Update 2025: delivering on the 2025 targets2025Joint United Nations Programme on HIV/AIDS (UNAIDS)Geneva
- 20UNAIDSThe Path that ends AIDS: global AIDS Update 20232023Joint United Nations Programme on HIV/AIDS (UNAIDS)Geneva
- N. Georgiadis, A. Katsimpris, M.A. Vatmanidou, T. Vassilakou, A. Beloukas, T.N. Sergentanis. Prevalence of chemsex and sexualized drug use among men who have sex with men: a systematic review and meta-analysis. Drug Alcohol Depend, 2025
- M.J. Page, J.E. McKenzie, P.M. Bossuyt. PRISMA 2020 Checklist. BMJ, 2021
- 23Veritas Health InnovationCovidence Systematic Review Software2020Veritas Health InnovationMelbourne, AustraliaAvailable at:www.covidence.orgMelbourne Australia. 2023
- Z. Wang, X. Yang, P.K.H. Mo, Y. Fang, T.K.M. Ip, J.T.F. Lau. Influence of social media on sexualized drug use and chemsex among Chinese men who have sex with men: observational prospective cohort study. J Med Internet Res, 2020
- P.A. Harris, R. Taylor, B.L. Minor. The REDCap consortium: building an international community of software platform partners. J Biomed Inform, 2019
- J. Peterson, V. Welch, M. Losos, P. Tugwell. The Newcastle–Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hosp Res Inst, 2011
- J.P.T. Higgins, S.G. Thompson, J.J. Deeks, D.G. Altman. Measuring inconsistency in meta-analyses. Br Med J, 2003. [PubMed]
- L. Furuya-Kanamori, J.J. Barendregt, S.A.R. Doi. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int J Evid Based Healthc, 2018. [PubMed]
- Regions. UNAIDS
- 30World BankWorld Bank Country and Lending Groups2025World BankWashington, DC[cited 2025 Aug 20]. Available from:https://datahelpdesk.worldbank.org/knowledgebase/articles/906519
- 31StataCorpStata Statistical Software: Release 192025StataCorp LLCCollege Station, TX
- L. Coyer, W. Van Bilsen, J. Bil. Pre-exposure prophylaxis among men who have sex with men in the Amsterdam Cohort Studies: use, eligibility, and intention to use. PLoS One, 2018
- Valencia Jorge GJTJGBADHGRP. Consumption of Sexualized and Recreational Drugs in HIV Negative Males: Survey of a Community HIV Screening, 2018
- M.A. Hammoud, S. Vaccher, F. Jin. HIV pre-exposure prophylaxis (PrEP) uptake among gay and bisexual men in Australia and factors associated with the nonuse of PrEP among eligible men: results from a prospective cohort Study. 2019
- N. Hanum, V. Cambiano, J. Sewell. Articles Use of HIV pre-exposure prophylaxis among men who have sex with men in England: data from the AURAH2 prospective study. 2020
- C.N. Okafor, C. Hucks-Ortiz, L.B. Hightow-Weidman. 2020
- Z. Wang, P.K.H. Mo, M. Ip, Y. Fang, J.T.F. Lau. Uptake and willingness to use PrEP among Chinese gay, bisexual and other men who have sex with men with experience of sexualized drug use in the past year. BMC Infect Dis, 2020
- K.J. Blair, T.S. Torres, B. Hoagland. Pre-exposure prophylaxis use, HIV knowledge, and internalized homonegativity among men who have sex with men in Brazil: a cross-sectional study. Lancet Reg Health Am, 2022. [DOI]
- J.S. Chone, S.V.M.A. Lima, I. Fronteira. Factors associated with chemsex in Portugal during the COVID-19 pandemic. Rev Lat Am Enfermagem, 2021
- S.H. Hulstein, A. Matser, M.F.S. Van Der Loeff, E. Hoornenborg, M. Prins, H.J.C. De Vries. Eligibility for HIV preexposure prophylaxis, intention to use preexposure prophylaxis, and informal use of preexposure prophylaxis among men who have sex with men in Amsterdam, the Netherlands. Sex Transm Dis, 2021. [PubMed]
- I. Hyndman, D. Nugent, G.G. Whitlock, A. McOwan, N. Girometti. COVID-19 restrictions and changing sexual behaviours in HIV-negative MSM at high risk of HIV infection in London, UK. Sex Transm Infect, 2021. [PubMed]
- D. Rollet, V. Clergue-Duval, S. Fouéré. Chemgen study: assessing the consumption of care in general practice of men with sexual relationships with men users of psychoactive products in a sexual context. Sex Res Social Policy, 2022
- L. Coyer, M. Prins, U. Davidovich. Trends in sexual behavior and sexually transmitted infections after initiating human immunodeficiency virus pre-exposure prophylaxis in men who have sex with men from Amsterdam, the Netherlands: a longitudinal exposure-matched study. AIDS Patient Care STDS, 2022. [PubMed]
- W.H. Eger, A. Adaralegbe, A. Khati. Exploring drivers of pre-exposure prophylaxis uptake among gay, bisexual, and other men who have sex with men in Malaysia. Int J STD AIDS, 2022. [PubMed]
- J.N. García-Pérez, E. Cañas-Ruano, J. Navarro. Sexual behavior and drug use impact in gay, bisexual, and other men who have sex with men. Med Clin, 2022
- E.M. Jalil, T.S. Torres, C.C.D.A. Pereira. High rates of sexualized drug use or chemsex among Brazilian transgender women and young sexual and gender minorities. Int J Environ Res Public Health, 2022
- J. MacGibbon, B.R. Bavinton, K. Drysdale. Explicit relationship agreements and HIV pre-exposure prophylaxis use by gay and bisexual men in relationships. Arch Sex Behav, 2023. [PubMed]
- F. Maviglia, J.A. Wickersham, I. Azwa. Engagement in chemsex among men who have sex with men (MSM) in Malaysia: prevalence and associated factors from an online national survey. Int J Environ Res Public Health, 2022
- D. Ogaz, L. Logan, T.J. Curtis. PrEP use and unmet PrEP-need among men who have sex with men in London prior to the implementation of a national PrEP programme, a cross-sectional study from June to August 2019. BMC Public Health, 2022
- U. Ali, S.K. Pasha, R. Patel, H.M. Schmidt, A. Altaf. Assessment of acceptability of pre-exposure prophylaxis for HIV prevention among men who sex with men and transgender community in Pakistan. J Coll Physicians Surg Pak, 2023. [PubMed]
- H. Agarwal, K. Yeatts, S.R. Chung, J. Harrison-Quintana, T.S. Torres. Social disparities on PrEP use and awareness among sexual and gender minorities using smartphones in India. Ther Adv Infect Dis, 2024
- S. Andrews, M. Hammoud, G. Prestage, D. Newcombe, P. Saxton. Sexualised drug use among gay and bisexual men in New Zealand: findings from a national cross-sectional study. Drug Alcohol Rev, 2024. [PubMed]
- D. Íncera-Fernández, F.J. Román-González, S. Moreno-Guillén, M. Gámez-Guadix. Sexualized drug use, risky sexual behaviors, and prevention strategies among gay, bisexual, and other men who have sex with men. Drugs Educ Prev Pol, 2024
- S. Moreno-García, M.J. Belza, C. Iniesta. Daily use of HIV pre-exposure prophylaxis among gay, bisexual and other men who have sex with men in Spain: prevalence and associated factors. Med Clínica, 2024
- J. Sun, B. She, P.M. Latt. Comparing the impact of sexualised drug use with and without chemsex on sexual behaviours among men who have sex with men in China: a national multi-site cross-sectional study. Sex Health, 2024
- J. Boonruang, D. Colby, S. Nonenoy. Amphetamine-type stimulant use and associated factors among men who have sex with men in Bangkok. AIDS Behav, 2025. [PubMed]
- D. Mayo, P. Huang. Pre-exposure prophylaxis engagement among sexual minority men in Taiwan: a behavioral health perspective. J Behav Med, 2025. [PubMed]
- R. Pessina, S. Pavanello Decaro, C. Torri, A. Prunas. Chemsex and psychosexual health in a large Italian sample of men who have sex with men (MSM). Sex Cult, 2025
- N.S. Wong, S.L. Chung, K.C.K. Lee, S.S. Lee. Interrelationship between chemsex engagement and PrEP (pre-exposure prophylaxis) experience in men who have sex with men: a community-based cross-sectional study. Sex Transm Infect, 2025. [PubMed]
- Y. Huang, R. Tian, Z. Zhou. HIV pre-exposure prophylaxis use on a global scale among men who have sex with men: a systematic review and meta-analysis. AIDS Patient Care STDS, 2023. [PubMed]
- M. Antonini, I.E.D. Silva, H.C. Elias, L. Gerin, A.C. Oliveira, R.K. Reis. Barriers to pre-exposure prophylaxis (Prep) use for hiv: an integrative review. Rev Bras Enferm, 2023
- G.G. Whitlock, K. Protopapas, J.I. Bernardino. Chems4EU: chemsex use and its impacts across four European countries in HIV-positive men who have sex with men attending HIV services. HIV Med, 2021. [PubMed]
- A.R. Howarth, V. Apea, S. Michie. The association between use of chemsex drugs and HIV clinic attendance among gay and bisexual men living with HIV in London. HIV Med, 2021. [PubMed]
- T. Platteau, R. Pebody, N. Dunbar, T. Lebacq, B. Collins. The problematic chemsex journey: a resource for prevention and harm reduction. Drugs Alcohol Today, 2019
- B.R. Bavinton, A.E. Grulich. HIV pre-exposure prophylaxis: scaling up for impact now and in the future. Lancet Public Health, 2021. [PubMed]
- P.D. Pozo-Herce, A. Martínez-Sabater, P. Sanchez-Palomares. Effectiveness of harm reduction interventions in chemsex: a systematic review. Healthcare (Switzerland), 2024
- L. De La Mora, M. Laguno, B. Torres. Long-term health outcomes of people with HIV engaged in chemsex: a prospective cohort study on drug use, sexual behaviour, sexually-transmitted infections and vulnerability. Infect Dis Ther, 2025. [PubMed]
- 68World Health OrganizationGuidelines on lenacapavir for HIV prevention and testing strategies for long-acting injectable pre-exposure prophylaxis (PrEP)2025World Health OrganizationGeneva
- A. Tomkins, R. George, M. Kliner. Sexualised drug taking among men who have sex with men: a systematic review. Perspect Public Health, 2019
- M. Viamonte, D. Ghanooni, J.M. Reynolds, C. Grov, A.W. Carrico. Running with scissors: a systematic review of substance use and the pre-exposure prophylaxis care continuum among sexual minority men. Curr HIV AIDS Rep, 2022. [PubMed]
- L. Muschialli, J.C. Yang, T. Engstrom. Sexualized drug use and chemsex: a bibliometric and content analysis of published literature. J Psychoactive Drugs, 2025. [DOI | PubMed]
- P.D. Pozo-Herce, A. Martínez-Sabater, P. Sanchez-Palomares. Effectiveness of harm reduction interventions in chemsex: a systematic review. Healthcare, 2024. [DOI | PubMed]
- L. Muschialli, J.C. Yang, T. Engstrom. Sexualized drug use and chemsex: a bibliometric and content analysis of published literature. J Psychoactive Drugs, 2025. [DOI | PubMed]
- P.C. Eustaquio, J. Smyth, J.A. Salisi. The risks for HIV and sexually transmitted infections among men who have sex with men who engage in chemsex in Low- and middle-income countries: a mixed methods systematic review and meta-analysis. AIDS Behav, 2024. [PubMed]