
Cannabis Use Disorder and Risk of Pancreatic Cancer in Patients with Chronic Pancreatitis: a Multicenter Retrospective Cohort Study
Abstract
Background:
Cannabis use is increasing globally, with a parallel rise in Cannabis Use Disorder (CUD). Chronic pancreatitis (CP), a progressive inflammatory condition, is associated with acute pancreatitis (AP) flares and an elevated risk of pancreatic cancer (PC). Although cannabis is often used for pain management in CP, its impact on PC risk and AP flare frequency is unclear.
Methods:
We conducted a retrospective cohort study using TriNetX to identify adults with CP, stratified by CUD status. Patients with pre-existing PC were excluded. Propensity score matching (1:1) was applied for demographics, behavioral factors, and comorbidities. The primary outcome was PC incidence; the secondary was AP flare frequency. Hazard ratios (HR) were calculated using Cox proportional hazards regression. Sensitivity analysis adjusted for opioid use disorder.
Results:
Before matching, the CUD cohort (n = 10,864) had higher rates of alcohol and nicotine use than controls (n = 42,160). After matching, 6,858 patients per group remained with balanced covariates (SMD < 0.1). Mean follow-up was shorter in the CUD cohort (736 ± 422 vs. 896 ± 368 days). CUD was associated with a significantly reduced risk of PC (67 vs. 274 cases; HR: 0.263, 95% CI: 0.202–0.344; p < 0.001) but a modest increase in AP flare risk (HR: 1.102, 95% CI: 1.043–1.166; p = 0.001). Results were consistent in the sensitivity analysis.
Conclusions:
Among patients with CP, CUD was associated with lower rates of PC detection during available follow-up, but a slightly increased risk of AP flares. These findings warrant further prospective and mechanistic studies to clarify cannabis’s role in pancreatic disease.
Article type: Research Article
Keywords: Cannabis use disorder, Chronic pancreatitis, Pancreatic cancer, Acute pancreatitis, Cannabinoids
Affiliations: https://ror.org/014ye12580000 0000 8936 2606Department of Medicine, Rutgers New Jersey Medical School, Newark, NJ 07103 USA; https://ror.org/011vxgd24grid.268154.c0000 0001 2156 6140Department of Medicine, Division of Gastroenterology & Hepatology, West Virginia University, Morgantown, West Virginia USA; https://ror.org/0358b9334grid.417348.d0000 0000 9687 8141Pakistan Institute of Medical Sciences, Islamabad, Pakistan; https://ror.org/04hbpw172grid.415422.40000 0004 0607 131XPunjab Medical College, Faisalabad, Pakistan; https://ror.org/014ye12580000 0000 8936 2606Department of Medicine, Division of Gastroenterology & Hepatology, Rutgers New Jersey Medical School, New Jersey, Newark USA
License: © The Author(s) 2026 CC BY 4.0 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Article links: DOI: 10.1007/s12029-025-01383-w | PubMed: 41533288 | PMC: PMC12804313
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (799 KB)
Introduction
Cannabis use is reported in about 2.5% of the world’s population, and about 45% of individuals in the US report lifetime cannabis use. The prevalence is gradually rising with the widespread legalization of its medical and recreational use and is associated with a simultaneous increase in cannabis use disorder (CUD) [ref. 1]. This growing prevalence underscores the importance of understanding the potential health effects of cannabis use, particularly in individuals with preexisting conditions. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) characterizes cannabis use disorder by a problematic cannabis use pattern leading to clinically significant impairment or distress. This requires meeting 2 out of 11 criteria within a 1-year period, including social impairment, risky use, impaired control over use, tolerance, and withdrawal [ref. 2, ref. 3].
Chronic pancreatitis (CP) is progressive pancreatic inflammation leading to irreversible damage and persistent abdominal pain. CP is associated with an elevated risk of pancreatic cancer (PC), a malignancy with one of the highest mortality rates among cancers [ref. 4].
CP patients may use cannabis as an alternative or adjunct therapy for pain management. While clinical efficacy data in CP specifically remain limited, medical cannabis has been studied for chronic pain conditions more broadly [ref. 5–ref. 7]. Despite the known association between CP and PC, a paucity of data explores the relationship between CUD and PC in individuals with CP. This study aims to address this by conducting a retrospective cohort study.
Methods
We conducted a retrospective cohort study utilizing TriNetX, a research network that provides real-time access to electronic health records from participating healthcare organizations. Most of these organizations are in the United States. Since it only provides de-identified data, TriNetX is compliant with the Health Insurance Portability and Accountability Act (HIPAA) and has received a waiver of review and informed consent from the Western Institutional Review Board. We identified patients using International Classification of Diseases, Tenth Revision (ICD-10) diagnostic codes available within the TriNetX research network.
Study Design and Participants
Patients aged 18 years or older with a CP, defined by ICD-10 codes K86.0 and K86.1, were included in the study. Patients were stratified into two cohorts: those with CUD, identified using ICD-10 codes F12.1 and F12.2, and a control cohort without cannabis-related disorders (F12). Patients with pre-existing PC (ICD-10 C25) were excluded. Follow-up was completed through December 2024.
Study Definitions and Outcomes
The primary outcome was the development of PC. The secondary outcome was the occurrence of AP flares, identified using ICD-10 codes K85 and K85.92.
Statistical Analysis
We used TriNetX’s in-built capabilities to conduct our analyses. To control for confounding, we performed 1:1 propensity score matching for demographic factors (age, sex, race, ethnicity), behavioral factors (alcohol use, nicotine dependence), and comorbidities (cholelithiasis, obesity, type 2 diabetes, hypertension, hyperlipidemia, chronic kidney disease, and systemic connective tissue disorders). Covariate balance between the two groups was evaluated using standardized mean difference (SMD), with a value < 0.1 indicating adequate balance.
After matching, Cox proportional hazards model (a time-to-event survival analysis which inherently accounts for differences in follow-up time by estimating the relative risk of the event occurring at any given point during the follow-up period) was used to calculate hazard ratios (HR) and 95% confidence intervals (CIs) (R’s Survival package v3.2-3; R Foundation for Statistical Computing). Kaplan-Meier analysis was also conducted with log-rank tests to compare outcomes between the cohorts.
Sensitivity Analysis
Opioid use disorder (OUD), identified by ICD-10 F11, is a common CUD-associated comorbidity that can potentially impact outcomes. Hence, to test the robustness of our findings, we conducted a sensitivity analysis after including opioid use disorder in the covariates used for propensity matching.
Results
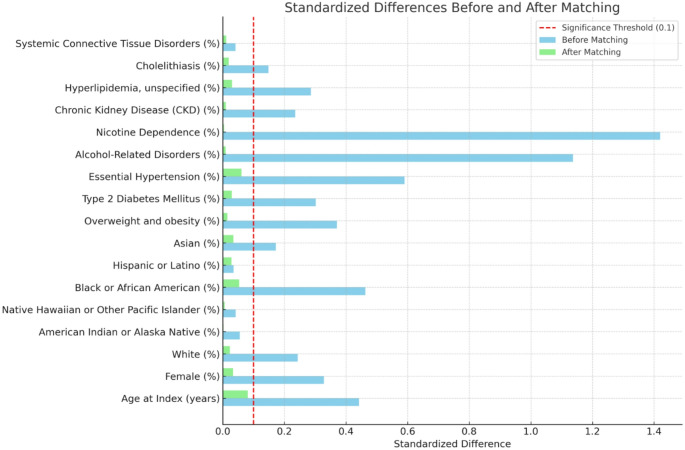
The CUD cohort had 10,864 patients and the control cohort had 42,160 patients. The CUD cohort was a younger population (46.4 ± 13.0 years vs. 53.3 ± 18.1 years, SMD: 0.045) and had a higher proportion of females (50.9% vs. 34.9%, SMD: 0.501) and African American individuals (30.6% vs. 12.1%, SMD: 0.538). On the other hand, the proportion of white (52.9% vs. 64.8%, SMD: 0.324) and Asian individuals (1.0% vs. 3.5%, SMD: 0.114) was significantly lower in the CUD cohort. Prevalence of comorbid conditions such as cholelithiasis (12.1% vs. 7.7%, SMD: 0.393), type 2 diabetes (30.7% vs. 17.8%, SMD: 0.619), hypertension (56.8% vs. 28.9%, SMD: 0.883), hyperlipidemia (26.7% vs. 15.2%, SMD: 0.478), alcohol-related disorders (53.7% vs. 8.0%, SMD: 1.153), and nicotine dependence (64.9% vs. 9.0%, SMD: 1.337) were also significantly higher in the CUD cohort. Similarly, chronic kidney disease (13.8% vs. 6.7%, SMD: 0.422) and overweight/obesity (18.3% vs. 6.3%, SMD: 0.399) were significantly more prevalent in the CUD cohort. (Table 1)
Table 1: Cohort characteristics before and after propensity score matching
| Characteristic | Before matching: CUD cohort (n = 10,894) | Before matching: control cohort (n = 42,160) | P-value (Before) | Std. Diff. (Before) | After matching: CUD cohort (n = 6,858) | After matching: control cohort (n = 6,858) | P-value (After) | Std. Diff. (After) |
|---|---|---|---|---|---|---|---|---|
| Demographics | ||||||||
| Age at Index (years) | 46.4 ± 13.0 | 53.3 ± 18.1 | < 0.001 | 0.442 | 47.0 ± 13.4 | 48.1 ± 14.6 | < 0.001 | 0.081 |
| Female (%) | 34.9% | 50.9% | < 0.001 | 0.328 | 38.6% | 37.0% | 0.055 | 0.033 |
| White (%) | 52.9% | 64.8% | < 0.001 | 0.243 | 56.9% | 55.8% | 0.185 | 0.023 |
| American Indian or Alaska Native (%) | 0.6% | 0.2% | < 0.001 | 0.055 | 0.5% | 0.5% | 0.903 | 0.002 |
| Native Hawaiian or Other Pacific Islander (%) | 0.6% | 0.3% | < 0.001 | 0.042 | 0.5% | 0.6% | 0.728 | 0.006 |
| Black or African American (%) | 30.6% | 12.1% | < 0.001 | 0.463 | 24.5% | 26.8% | 0.002 | 0.053 |
| Hispanic or Latino (%) | 6.4% | 5.6% | 0.001 | 0.035 | 6.6% | 5.9% | 0.097 | 0.028 |
| Asian (%) | 1.0% | 3.5% | < 0.001 | 0.172 | 1.2% | 0.9% | 0.046 | 0.034 |
| Diagnoses | ||||||||
| Overweight and Obesity (%) | 18.3% | 6.3% | < 0.001 | 0.370 | 14.4% | 14.9% | 0.385 | 0.015 |
| Type 2 Diabetes Mellitus (%) | 30.7% | 17.8% | < 0.001 | 0.302 | 28.2% | 29.5% | 0.093 | 0.029 |
| Essential Hypertension (%) | 56.8% | 28.9% | < 0.001 | 0.590 | 48.5% | 51.5% | < 0.001 | 0.061 |
| Alcohol-Related Disorders (%) | 53.7% | 8.0% | < 0.001 | 1.137 | 36.4% | 36.0% | 0.606 | 0.009 |
| Nicotine Dependence (%) | 64.9% | 9.0% | < 0.001 | 1.420 | 45.9% | 45.7% | 0.824 | 0.004 |
| Chronic Kidney Disease (%) | 13.8% | 6.7% | < 0.001 | 0.235 | 11.9% | 12.2% | 0.564 | 0.010 |
| Hyperlipidemia, Unspecified (%) | 26.7% | 15.2% | < 0.001 | 0.286 | 23.8% | 25.1% | 0.077 | 0.030 |
| Cholelithiasis (%) | 12.1% | 7.7% | < 0.001 | 0.148 | 10.4% | 11.0% | 0.270 | 0.019 |
| Systemic Connective Tissue Disorders (%) | 2.8% | 2.1% | < 0.001 | 0.041 | 2.8% | 2.9% | 0.538 | 0.011 |
Following matching, both cohorts included 6,858 patients, with appropriate balancing of all covariates (SMD < 0.1). (Fig. 1) The mean follow-up was 736 ± 422 days for the CUD cohort and 896 ± 368 days for the control cohort. Given the non-normal distribution of follow-up duration, medians are also reported: 642 days (IQR 381–1,012) in the CUD cohort vs. 811 days (IQR 501–1,219) in the control cohort.
Outcomes
The CUD cohort showed significantly lower rates of PC detection (67 vs. 274; HR 0.263, 95% CI: 0.202–0.344, log-rank p-value: <0.001). (Table 2) Conversely, the risk of AP flares was higher in the CUD cohort vs. controls (2,487 vs. 2,446; HR 1.102, 95% CI: 1.043–1.166, log-rank p-value: 0.001). In sensitivity analysis adjusting for opioid use disorder, results remained consistent with the primary analysis (PC: 62 vs. 328 h 0.281, 95% CI: 0.213–0.372, p < 0.001), demonstrating robustness of our findings.
Table 2: Comparison of outcomes between CUD cohort and control cohort
| Outcome | Patients with outcome in CUD cohort (n) | Patients with outcome in control cohort (n) | Hazard ratio (95% CI) | Log rank p-value |
|---|---|---|---|---|
| Pancreatic Cancer | 67 | 274 | 0.263 (0.202–0.344) | < 0.001 |
| Acute Pancreatitis Flare | 2,487 | 2,446 | 1.102 (1.043–1.166) | 0.001 |
Discussion
The relationship between CUD and cancer risk remains complex and not fully established. With the growing prevalence of cannabis use, understanding its health implications is increasingly critical. Cannabis use has been associated with both an increased risk of some cancers, such as particular testicular cancers, and a decreased risk of others, such as bladder cancer [ref. 8, ref. 9]. This variation in outcomes is often influenced by the type of cannabinoid being used and the mode of consumption. For instance, smoking cannabis is believed to increase the risk of cancers in the throat and respiratory tract due to the presence of carcinogens in cannabis smoke, which resemble those found in cigarette smoke [ref. 8, ref. 10].
The relationship between cannabis use and cancer risk remains incompletely understood. Preclinical studies demonstrate that certain cannabinoids can inhibit tumor growth, induce apoptosis, and reduce angiogenesis in pancreatic cancer cell lines and animal models. However, several important caveats limit the interpretation of these findings. Most anti-cancer studies have been conducted in vitro or in animal xenograft models rather than clinical trials [ref. 11–ref. 14]. Cannabinoid receptors (CB1 and CB2) are expressed ubiquitously throughout the body and bind endocannabinoids, phytocannabinoids (such as THC and CBD), and synthetic cannabinoids—each with potentially different biological effects [ref. 15]. Studies demonstrating synergistic effects with chemotherapy have predominantly used synthetic cannabinoids rather than the cannabis products consumed by patients with CUD [ref. 16]. The cannabis used by patients in our cohort likely differs substantially from purified compounds studied in laboratory settings in terms of cannabinoid composition, THC: CBD ratios, route of administration, and dose.
We also found a modestly increased risk of AP flares in CP in the CUD. Whereas growing evidence suggests that cannabis use may contribute to idiopathic acute pancreatitis (AP), our study is unique in demonstrating an increased risk of AP flares, specifically within the CP population [ref. 17]. This is a pertinent novelty, as CP patients are inherently at higher risk for recurrent pancreatic inflammation, with a pressing need for the identification of modifiable risk factors in this vulnerable group.
Despite these mechanistic uncertainties, our study provides novel real-world epidemiological evidence from a large clinical population, addressing a critical knowledge gap. While preclinical data cannot be directly extrapolated to clinical outcomes, our findings generate important hypotheses that warrant prospective investigation through well-designed clinical studies and mechanistic research to clarify the relationship between cannabis use and pancreatic cancer risk in patients with chronic pancreatitis.
Our study’s strengths include the large sample size, propensity score matching to minimize confounding bias, and implementation of sensitivity analysis. The differential follow-up time between cohorts warrants consideration, with the shorter follow-up time in the CUD cohort being a potential factor for lower PC case detection. However, Cox proportional hazards regression inherently accounts for differential follow-up by estimating the instantaneous hazard at any given time point among those still at risk, rather than relying on cumulative event counts [ref. 18]. However, the study is limited by its observational nature, which means that only associations, not causal relationships, can be inferred. TriNetX relies on coded diagnostic data from electronic health records, which may be subject to coding inaccuracies and incomplete capture of clinical information. Moreover, the lack of detailed information on the frequency, duration, or type of cannabis use restricts the ability to determine dose-response relationships. Cannabinoid pharmacokinetics are influenced by numerous variables, and product labeling is often inaccurate, making the quantification of exposure particularly challenging [ref. 19–ref. 21]. Future studies incorporating more granular data on healthcare utilization patterns, socioeconomic variables, and provider-level factors would be valuable in clarifying the influence of potential unmeasured confounders on our findings.
In conclusion, these exploratory findings suggest an association between CUD and reduced PC detection during available follow-up in patients with CP. CUD was also associated with a modestly increased risk of AP flares, which aligns with emerging evidence linking cannabis use to acute pancreatitis episodes. Given the limitations of our retrospective observational study, these associations require validation in prospective studies with longer, standardized follow-up and comprehensive ascertainment of cancer outcomes before clinical implications can be determined. Future research should also investigate potential mechanisms and determine whether the observed differences reflect true biological effects or detection bias.
References
- KN Farrelly, JD Wardell, E Marsden, ML Scarfe, P Najdzionek, J Turna, J MacKillop. The impact of recreational cannabis legalization on cannabis use and associated outcomes: a systematic review. Subst Abuse: Res Treat, 2023
- DA Gorelick. Cannabis-related disorders and toxic effects. N Engl J Med, 2023. [DOI | PubMed]
- 3.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed., text rev. Washington, DC: American Psychiatric Association; 2022. 10.1176/appi.books.9780890425787
- G Le Cosquer, C Maulat, B Bournet, P Cordelier, E Buscail, L Buscail. Pancreatic cancer in chronic pancreatitis: pathogenesis and diagnostic approach. Cancers, 2023. [DOI | PubMed]
- TS Barlowe, JL Koliani-Pace, KD Smith, SR Gordon, TB Gardner. Effects of medical cannabis on use of opioids and hospital visits by patients with painful chronic pancreatitis. Clin Gastroenterol Hepatol, 2019. [DOI | PubMed]
- M de Vries, DC Van Rijckevorsel, KC Vissers, OH Wilder-Smith, H Van Goor. Single dose delta‐9‐tetrahydrocannabinol in chronic pancreatitis patients: analgesic efficacy, pharmacokinetics and tolerability. Br J Clin Pharmacol, 2016. [DOI | PubMed]
- 7.Wang L, Hong PJ, May C, Rehman Y, Oparin Y, Hong CJ, Hong BY, AminiLari M, Gallo L, Kaushal A, Craigie S, Couban RJ, Kum E, Shanthanna H, Price I, Upadhye S, Ware MA, Campbell F, Buchbinder R, Agoritsas T, Busse JW. Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: a systematic review and meta-analysis of randomised clinical trials. BMJ. 2021;374:n1034.
- M Ghasemiesfe, B Barrow, S Leonard, S Keyhani, D Korenstein. Association between marijuana use and risk of cancer: a systematic review and meta-analysis. JAMA Netw Open, 2019. [DOI | PubMed]
- AA Thomas, LP Wallner, VP Quinn, J Slezak, SK Van Den Eeden, GW Chien, SJ Jacobsen. Association between cannabis use and the risk of bladder cancer: results from the California men’s health study. Urology, 2015. [DOI | PubMed]
- D Moir, WS Rickert, G Levasseur, Y Larose, R Maertens, P White, S Desjardins. A comparison of mainstream and sidestream marijuana and tobacco cigarette smoke produced under two machine smoking conditions. Chem Res Toxicol, 2008. [DOI | PubMed]
- TQ Le, N Meesiripan, S Sanggrajang, N Suwanpidokkul, P Prayakprom, C Bodhibukkana, V Khaowroongrueng, K Suriyachan, S Thanasitthichai, A Srisubat, P Surawongsin. Anti-proliferative and apoptotic effect of cannabinoids on human pancreatic ductal adenocarcinoma xenograft in BALB/c nude mice model. Sci Rep, 2024. [DOI | PubMed]
- Y Yang, N Huynh, C Dumesny, K Wang, H He, M Nikfarjam. Cannabinoids inhibited pancreatic cancer via P-21 activated kinase 1 mediated pathway. Int J Mol Sci, 2020. [DOI | PubMed]
- P Malhotra, R Palanisamy, A Panda, I Casari, JE Tirnitz-Parker, F O’Gara, R Trengove, K Ragunath, JA Caparros-Martin, M Falasca. Cannabidiol is associated with improved survival in pancreatic cancer and modulation of bile acids and gut microbiota. Int J Mol Sci, 2025. [DOI | PubMed]
- A Carracedo, M Gironella, M Lorente, S Garcia, M Guzmán, G Velasco, JL Iovanna. Cannabinoids induce apoptosis of pancreatic tumor cells via Endoplasmic reticulum stress–related genes. Cancer Res, 2006. [DOI | PubMed]
- AI Fraguas-Sánchez, A Fernández-Carballido, A Torres-Suárez. Phyto-, endo-and synthetic cannabinoids: promising chemotherapeutic agents in the treatment of breast and prostate carcinomas. Expert Opin Investig Drugs, 2016. [DOI | PubMed]
- B Hinz, R Ramer. Cannabinoids as anticancer drugs: current status of preclinical research. Br J Cancer, 2022. [DOI | PubMed]
- JA Barkin, Z Nemeth, AK Saluja, JS Barkin. Cannabis-induced acute pancreatitis: a systematic review. Pancreas, 2017. [DOI | PubMed]
- 18.Abd ElHafeez S, D’Arrigo G, Leonardis D, Fusaro M, Tripepi G, Roumeliotis S. Methods to analyze time‐to‐event data: the Cox regression analysis. Oxidative medicine and cellular longevity. 2021;2021(1):1302811.
- M Liyanage, M Nikanjam, EV Capparelli, RT Suhandynata, RL Fitzgerald, TD Marcotte, I Grant, JD Momper. Variable delta-9-tetrahydrocannabinol pharmacokinetics and pharmacodynamics after cannabis smoking in regular users. Ther Drug Monit, 2023. [DOI | PubMed]
- EL Karschner, MJ Swortwood-Gates, MA Huestis. Identifying and quantifying cannabinoids in biological matrices in the medical and legal cannabis era. Clin Chem, 2020. [DOI | PubMed]
- R Vandrey, ES Herrmann, JM Mitchell, GE Bigelow, R Flegel, C LoDico, EJ Cone. Pharmacokinetic profile of oral cannabis in humans: blood and oral fluid disposition and relation to pharmacodynamic outcomes. J Anal Toxicol, 2017. [DOI | PubMed]