
Neurocognitive outcomes in adolescents with and without four weeks of cannabis abstinence: a randomized clinical trial using contingency management
Abstract
Background:
As adolescent cannabis use becomes more common, questions remain about the potential for neurocognitive recovery after stopping cannabis use.
Method:
This study examined whether short-term abstinence from cannabis leads to cognitive improvements. A total of 238 adolescents (ages 13–19; 51% female; 55% White, 18% Black, 9% Asian, 18% other races) from Greater Boston participated, including 154 adolescents who regularly used cannabis (CB) and 84 adolescents with no cannabis use (NU). Participants who used cannabis were randomized to incentivized abstinence (CB-Abst) or a non-contingent monitoring control (CB-Mon). Non-users completed four weeks of monitoring (NU). Participants completed tests of executive function, memory, and attention weekly for four weeks.
Results:
At baseline, CB adolescents demonstrated worse verbal memory and processing speed than NU on (p <.006). CB-Abst performance was similar to that of the NU group at week 4. At week 4, those in the CB-Abst group showed greater improvements in inhibitory control compared to the CB-Mon group (β = -10.9, p = .037). There were no significant differences between CB groups in memory or attention task performance at week 4. Exploratory analyses revealed modest gains across all groups in some tasks.
Discussion:
Brief cannabis abstinence may be associated with improvements in executive function among adolescents, supporting the idea of neurocognitive recovery, which has important implications for treatment, prevention, and public health policies.
Article type: Research Article
Keywords: adolescence, cannabis, executive function, cognitive recovery, abstinence intervention, contingency management
Affiliations: Department of Psychiatry, Massachusetts General Hospital, Boston, MA, United States; Harvard Medical School, Boston, MA, United States; University of Miami Miller School of Medicine, Miami, FL, United States
License: Copyright © 2025 Schuster, Costello, Potter, Torquati, Gilman and Evins. CC BY 4.0 This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
Article links: DOI: 10.3389/fpsyt.2025.1723633 | PubMed: 41522481 | PMC: PMC12785183
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (1.6 MB)
Introduction
Cannabis is among the most widely used substances among adolescents, with nearly half reporting lifetime use by age 18 (ref. 1, ref. 2). Regular use is common, with 12% of 12th graders in 2023 reporting daily cannabis use for at least one month (ref. 3). Growing commercialization has increased youth access to cannabis products (ref. 4, ref. 5) and may lead to perceptions that cannabis is safe (ref. 6). Although adolescent cannabis use, especially early and frequent use, is linked to adverse outcomes (ref. 7), the impact of adolescent cannabis exposure on cognitive functioning remains unclear. As adolescence is a key period of brain development (ref. 8–ref. 11), understanding how cannabis affects neurocognitive functions, through controlled studies assessing the effect of ongoing cannabis exposure and abstinence in youth, is critically important (ref. 1).
Adolescent cannabis use has been linked to difficulties in verbal working memory (ref. 12–ref. 14), processing speed (ref. 15, ref. 16), and executive functioning (ref. 12, ref. 17–ref. 21). Much of this evidence comes from cross-sectional studies that generally demonstrate poorer neurocognitive performance amongst adolescents who use cannabis (CB) than their non-using peers (NU). Longitudinal studies suggest that early and frequent cannabis exposure predicts declines in cognitive functioning over time (ref. 22). Controlled trials are needed to assess whether the effect of cannabis is causal for cognitive deficits and rule in or out the common liability hypothesis, that preexisting vulnerabilities such as genetic risk, environmental adversity, or early cognitive weaknesses may contribute to both cannabis use and poorer neurocognitive performance.
Abstinence studies provide an important experimental approach to assess direct effects of cannabis exposure on cognition. Evidence from adults indicates the brain can recover: a meta-analysis of 45 studies found neural and functional improvements after stopping substance use, including improvement in executive functions (i.e., cognitive flexibility and decision-making as assessed by the Wisconsin Card Sorting and Iowa Gambling Tasks; ref. 23). Whether similar recovery occurs in adolescents is less clear. Adolescence is a developmental stage characterized by both increased neuroplasticity, which may help repair damage from harmful exposures (ref. 24), and greater vulnerability due to rapid neural changes (ref. 25). Early abstinence studies in youth offer cautious optimism. Non-randomized trials show improvements in sustained attention after two weeks of abstinence (ref. 26) and in memory after three weeks (ref. 27). In a trial of N-acetylcysteine, teens who achieved four to eight weeks of abstinence showed improvements in verbal memory and psychomotor speed (ref. 28). Our group reported improved verbal encoding after one week of cannabis abstinence in young adults (ref. 29). These findings highlight the potential of randomized adolescent abstinence trials to clarify the potential for neurocognitive recovery after stopping cannabis use in youth.
The current study
This longitudinal trial enrolled adolescents who used cannabis at least weekly (CB) and a comparison group of adolescents who reported no regular or current cannabis use (NU). CB adolescents were randomly assigned to four weeks of incentivized cannabis abstinence (CB-Abst) or monitoring with usual cannabis use (CB-Mon). We conducted weekly cognitive assessments over four weeks to compare the magnitude and timing of cognitive changes between adolescents assigned to incentivized cannabis abstinence and those monitored without an abstinence requirement. We hypothesized that CB-Abst would demonstrate greater improvements in memory, executive functioning, and attention than CB-Mon.
Methods
Participants
Study [NCT03276221] enrollment took place between August 2017 and September 2022. Participants (N = 238) were adolescents aged 13 to 19, recruited through community advertisements, direct outreach to middle and high schools in Greater Boston, and peer referrals. All participants spoke English, were medically healthy, endorsed no neurodevelopmental delays (including, but not limited to, Autism Spectrum Disorder, Intellectual Disability, and Down Syndrome), and were considered able to safely participate. CB adolescents (N = 154) reported at least weekly cannabis use, used cannabis within one week before screening, were willing to be randomized to 30 days of cannabis abstinence, and were not seeking assistance to or planning to stop regular cannabis use. NU adolescents (N = 84) reported no more than five cannabis use occasions lifetime and none in the prior year or before age 16.
Procedures
Procedures were approved by the Mass General Brigham Institutional Review Board. Written informed consent was obtained from participants aged 18 years or older, while those under age 18 provided written parental consent and participant assent. Participants then completed a baseline assessment over two visits. Participants reporting regular cannabis use were then randomly assigned to 4 weeks of incentivized abstinence using contingency management (CB-Abst; n=125) or 4 weeks of monitoring without incentives for abstinence (CB-Mon; n=94). Randomization was stratified by sex (male vs. female), age (13–16 years vs. ≥ 17 years), and average frequency of cannabis use (1 day per week vs. ≥ 1 day per week). All participants completed study visits, occurring approximately on study days 3, 5, 7, 14, 21, and 28 post-baseline.
Contingency management protocol
This study used a voucher-based contingency management (CM) procedure (ref. 29–ref. 32) for participants randomized to CB-Abst that offered escalating payments as incentives for biochemically verified cannabis abstinence over a 4-week period. At the baseline visit, all CB participants completed an abstinence contract with a study staff member, which outlined expected behavior changes over the 4-week period, the payment schedule, and contingencies if they were randomized to CB-Abst (ref. 32). At the end of the baseline visit, participants assigned to CB-Abst were asked to immediately stop cannabis use for four weeks. CB-Mon participants were not required to change their substance use habits. CB-Abst participants who resumed cannabis use within the first week of abstinence were given one opportunity to restart the abstinence protocol and remain in the study. Those who resumed cannabis after the first week of abstinence were excluded.
During the intervention phase, CB-Abst participants received incentives through a two-part system that included fixed payments for study visit attendance and increasing payments for biochemically verified ongoing cannabis abstinence. After completing the 4-week abstinence period, CB-Abst participants were no longer required to abstain from cannabis and were paid for attending a post-baseline follow-up visit (ref. 32). CB-Mon and NU participants were paid on an escalating schedule solely for study visit attendance. The payment schedule is shown in T1. Participants were paid via reloadable debit cards through Clinical Trials Payer (CT Payer), a secure web-based platform that ensures HIPAA and HITECH compliance for clinical trial payments. Payments were made on the day of the visit for attendance and after receipt of quantitative urinalysis results confirming abstinence, which typically occurred within 2–5 days after the study visit. Among participants assigned to the CB-Abst group, 6 resumed cannabis use. Post-hoc t-test analyses identified a trend toward higher CUDIT scores among CB-Abst participants who did not maintain abstinence compared to those who did (mean difference in scores = 4.5; p = 0.05), suggesting that higher cannabis dependence posed challenges in maintaining abstinence in the context of the contingency management protocol.
Table 1: Remuneration schedule for participants.
| Visit | Contingency management (cannabis users; CB-Abst) | Monitoring (cannabis users; CB-Mon) | Non-users (NU) | |||
|---|---|---|---|---|---|---|
| Attendance | Abstinence | Attendance | Abstinence | Attendance | ||
| 1 | Baseline part I | $10 | – | $10 | – | $10 |
| 2 | Baseline part II | $10 | – | $15 | N/A | $15 |
| 3 | 3 days | $10 | $15 | $20 | N/A | $20 |
| 4 | 4 days | $10 | $30 | $25 | N/A | $25 |
| 5 | 1 week | $10 | $45 | $30 | N/A | $30 |
| 6 | 2 weeks | $10 | $60 | $35 | N/A | $35 |
| 7 | 3 weeks | $10 | $75 | $40 | N/A | $40 |
| 8 | 4 weeks | $10 | $90 | $45 | N/A | $45 |
| 9 | 4-week follow-up | $10 +$15* | – | $50 | N/A | 50 |
| Max subtotal | $105 | $315 | $270 | N/A | $270 | |
| Max total | $420 | $270 | $270 | |||
*An additional $15 for completing study procedures.
Bio-verification of cannabis abstinence
Participants provided a urine sample at each study visit for 11-nor-9-carboxy-tetrahydrocannabinol (THCCOOH) concentration determination via liquid chromatography-tandem mass spectrometry, with a quantitation limit of 5 ng/mL and an upper linearity limit of 500 ng/mL (Dominion Diagnostics, Richmond VA). When necessary, samples were subjected to serial dilutions to ensure values fell within the assay’s linear range (5 ng/mL–500 ng/mL). THCCOOH concentrations were adjusted based on creatinine levels (measured in mg/dL), generating a THCCOOH to creatinine ratio for each time point (CN-THCCOOH; measured in ng/mg). To verify self-reported abstinence, CN-THCCOOH ratios for specimen pairs collected ≥48 hours apart were compared to an expected CN-THCCOOH ratio determined using a statistical model developed by Schwilke and colleagues (ref. 33). A specificity threshold of 95% was adopted, allowing for a false positive rate of 2.5%. Relevant to this algorithm, the sample reported days since last use prior to initiating abstinence. CB-Abst participants reported, on average, 1.4 days since last cannabis use when starting abstinence (SD = 1.5 days, median=1 day, range=0–7 days).
Cognitive functioning assessment
Cognitive functioning: executive functioning, memory, and attention
The Cambridge Neuropsychological Test Automated Battery (CANTAB) was used to assess cognition at baseline and weekly for four weeks. Eight modules evaluated executive function (Multitasking Test, One-Touch Stockings of Cambridge, Stop Signal Task, Spatial Working Memory), memory (Paired Associates Learning, Spatial Span, and Verbal Recognition Memory), and attention (Rapid Visual Information Processing; see Supplementary Table 1. for descriptions of all CANTAB modules used;).
Self-report measures
Demographic and background information
Baseline assessments included participant-reported age, sex, gender, and racial identity, Cannabis Use Disorder Identification Test–Revised (CUDIT-R: ref. 34), Alcohol Use Disorders Identification Test (AUDIT; ref. 35), 90-day Timeline Follow-back interview to approximate the quantity and frequency of cannabis and alcohol use, Adolescent Psychotic-Like Symptom Screener (APSS; ref. 36), Screener for Child Anxiety Related Disorders (SCARED; ref. 37), and the Mood and Anxiety Symptoms Questionnaire (MASQ; ref. 38).
Analytic plan
The initial implementation of analyses was analyst-blind (ref. 39). We examined all outcomes using regression models fitted with generalized estimating equations (GEE), a reliable alternative to maximum likelihood estimation for mixed effects models (ref. 40). We assumed data were clustered by subjects and that the observations within each study visit for a subject were uncorrelated (the GEE method is robust to misspecification of the correlation structure among a subject’s observations). Continuous outcomes, such as latencies and reaction times, were analyzed using linear regression. Bounded count outcomes, such as the number of errors or correct responses, were analyzed with binomial regression to address potential non-normality issues. Outcomes were examined across post-baseline study weeks 1 to 4. The primary confirmatory effect of interest for each outcome was a dummy-coded contrast between CB-Mon (the reference group, coded as 0) and CB-Abst (coded as 1), testing whether a constant effect of abstinence exists across all time points. A sensitivity analysis evaluated whether a group-by-time interaction term was necessary. Models included covariates for linear trends and baseline outcome score. Additional sensitivity analyses incorporated covariates for age (years), sex (male vs. female), and baseline CUDIT-R scores. P-values were adjusted for multiple comparisons using the Bonferroni method within each module. Clinical significance was assessed by computing standardized effect sizes, estimated by dividing the effect estimate (on the original measurement scale) by the pooled standard deviation of the outcome during the baseline visit.
Rates of missingness on all primary variables are presented in Supplementary Table 2 (range = 8.2-11.6%). Missing outcome data were imputed 48 times using chained equations (MICE; ref. 41; version 3.14.0; ref. 42).) with linear regression and predictive mean matching. Results were then pooled following Rubin’s rule. Participants were included in the analysis if they had data from at least one post-baseline visit and biochemically confirmed abstinence. Covariates for imputing missing values included baseline and non-missing post-baseline outcome scores, age in years, biological sex at birth, baseline CUDIT-R scores, and years of cannabis exposure. A sensitivity analysis was conducted including only participants with complete data. Analyses were performed using R (version 4.1.1; ref. 43) and RStudio (version 2020.9.0.351; ref. 44). Data were prepared with R packages ‘dplyr’ (version 1.0.7; ref. 45) and ‘tidyr’ (version 1.1.4; ref. 46). Models were fitted with the R package ‘geepack’ (version 1.3.4; ref. 47). Reproducible code and de-identified data were organized using the R package ‘targets’ (version 0.8.1; ref. 48).
Results
Sample descriptives
Of 238 participants screened, 201 participants were eligible and completed baseline measures, 132 (65.7%) used cannabis at least weekly (CB) (M = 4.2, SD = 2.2 days per week) and 69 (34.3%) did not use cannabis (NU). Groups differed significantly on age and alcohol use and no other baseline characteristics, (see T2, Supplementary Table 1).
Table 2: Descriptive statistics and group comparisons at baseline.
| Domain | Measure | CB-Abst | CB-Mon | NU | Significant group differences |
|---|---|---|---|---|---|
| Sample size | 54 | 66 | 69 | ||
| Completed intervention phase; % (n) | 83.3 (45) | 89.4 (59) | 92.8 (64) | ||
| Age; M (SD) | 18.3 (1.4) | 18.1 (1.5) | 17 (1.8) | CB-Mon > NU; CB-Abst > NU | |
| Biological sex; % (n) | |||||
| – Female | 48.1 (26) | 47 (31) | 58 (40) | ||
| – Male | 51.9 (28) | 53 (35) | 42 (29) | ||
| Race; % (n) | |||||
| – American Indian/Alaska Native | 1.9 (1) | 1.5 (1) | 0 (0) | ||
| – Asian | 7.4 (4) | 10.6 (7) | 8.7 (6) | ||
| – Black/African American | 18.5 (10) | 15.2 (10) | 20.3 (14) | ||
| – More than one race | 11.1 (6) | 16.7 (11) | 5.8 (4) | ||
| – White | 57.4 (31) | 51.5 (34) | 56.5 (39) | ||
| – Not listed | 3.7 (2) | 4.5 (3) | 8.7 (6) | ||
| Hispanic/Latino(a); % (n) | 9.3 (5) | 24.2 (16) | 13 (9) | ||
| Mental health symptoms | |||||
| – APSS; M (SD) | 0.1 (0.6) | 0.3 (0.8) | 0.1 (0.5) | ||
| – MASQ; M (SD) | 121.6 (26.4) | 122.1 (28.4) | 112.4 (28.3) | ||
| – SCARED GAD; M (SD) | 6 (4.4) | 5.9 (4.3) | 6.4 (4.6) | ||
| Substance use | |||||
| – Years w/cannabis use; M (SD) | 3.3 (1.3) | 3.4 (1.5) | |||
| – Days/wk cannabis use; M (SD) | 3.6 (2.8) | 3.3 (2.6) | |||
| – THCCOOH levels; M (SD) | 211.8 (338) | 389.6 (745) | |||
| – CUDIT-R; M (SD) | 13.7 (5.4) | 14.1 (5.5) | |||
| – Days/wk alcohol use; M (SD) | 0.7 (0.8) | 0.4 (0.8) | 0.1 (0.2) | CB-Abst > CB-Mon; CB-Mon > NU; CB-Abst > NU | |
| – AUDIT; M (SD) | 5.4 (4.8) | 5.9 (5) | 1.9 (2.5) | CB-Mon > NU; CB-Abst > NU | |
| Memory (PAL) | Total number of adjusted errors | 6.4 (6.3) | 5.9 (5.4) | 7.1 (6.0) | |
| First attempt memory score | 15.7 (2.8) | 15.6 (3.1) | 15.1 (3.4) | ||
| Memory (SSP) | Forward span length | 7.0 (1.5) | 7.3 (1.4) | 7.1 (1.3) | |
| Reverse span length | 6.8 (1.6) | 6.7 (1.4) | 6.7 (1.4) | ||
| Memory (VRM) | Immediate recall – total correct | 6.0 (2.4) | 6.7 (1.9) | 7.4 (2.2) | CB-Mon < NU; CB-Abst < NU |
| Delayed recall – total correct | 6.5 (2.8) | 6.9 (2.5) | 7.6 (2.3) | CB-Mon < NU; CB-Abst < NU | |
| Immediate recognition – total correct | 32.4 (3.8) | 33.2 (2.0) | 32.4 (2.6) | ||
| Delayed recognition – total correct | 32.4 (2.7) | 32.7 (2.5) | 32.2 (2.8) | ||
| Executive Functioning (MTT) | Total incorrect | 5.0 (5.5) | 6.0 (8.3) | 5.8 (5.9) | |
| Median response latency (ms) | 557 (87) | 548 (90) | 586 (85) | CB-Mon < NU; CB-Abst < NU | |
| Median incongruency cost (ms) | 40 (33) | 50 (32) | 55 (46) | ||
| Median multitasking cost (ms) | 159 (107) | 134 (75) | 163 (100) | ||
| Executive Functioning (OTS) | Problems solved on first choice | 11.9 (1.9) | 11.2 (2.2) | 11.3 (2.6) | |
| Median latency to first correct choice (ms) | 9714 (3032) | 9161 (3370) | 9682 (3454) | ||
| Executive Functioning (SST) | Stop signal reaction time (ms) | 224 (47) | 220 (45) | 232 (62) | |
| Executive Functioning (SWM) | Total number of between errors | 5.1 (6.2) | 6.0 (7.2) | 8.6 (8.3) | CB-Mon < NU; CB-Abst < NU |
| Strategy for 6–8 box conditions | 6.4 (2.6) | 6.1 (2.8) | 6.9 (2.3) | CB-Abst > CB-Mon; CB-Mon < NU; CB-Abst < NU | |
| Attention (RVP) | Discriminability – A’ | 0.92 (0.05) | 0.91 (0.05) | 0.89 (0.07) | CB-Mon > NU; CB-Abst > NU |
| Median response time for hits (ms) | 444 (55) | 434 (63) | 440 (54) |
APSS, Adolescent Psychotic-Like Symptom Screener; MASQ, Mood and Anxiety Symptoms Questionnaire, SCARED GAD, Screener for Child Anxiety Related Disorders – Generalized Anxiety Disorder; CUDIT, Cannabis Use Disorder Identification Test; AUDIT, Alcohol Use Disorder Identification Test; PAL, Paired Associates Learning; SSP, Spatial Span; VRM, Verbal Recognition Memory; MTT, Multitasking Test; OTS, One-Touch Stockings of Cambridge; SST, Stop Signal Task; SWM, Spatial Working Memory; RVP, Rapid Visual Information Processing.
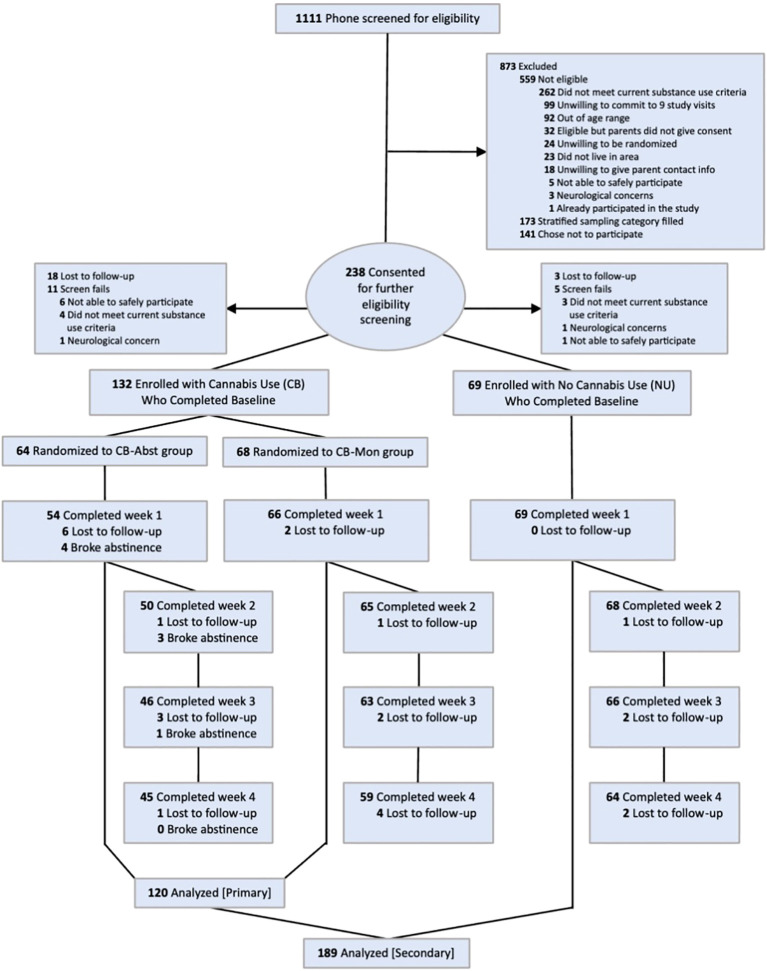
Among CB, 64 (48.5%) were randomized to CB-Abst and 68 (51.5%) to CB-Mon; 120 CB participants completed at least one post-baseline study visit and were included in the analyses (CB-Abst: 54, 84.4% of those randomized; CB-Mon: 66, 97.1% of those randomized). Among CB-Abst participants included in the analysis, 48 (88.9%) maintained biochemically-verified cannabis abstinence throughout the intervention period. Among NU 69 (100%) completed at least one post-baseline study visit and were included in analyses. See Consort Diagram, f1.
Baseline cognition
First, we note comparisons between baseline CB and NU groups because these groups were not randomly assigned. Comparing baseline NU and CB groups, NU had higher total correct for immediate recall (p = 0.001) and delayed recall (p = 0.006) on the VRM and faster median response times on the MTT (p = 0.012) and more errors (p = 0.004), yet better strategy on SWM (p = 0.007).
Second, we note comparisons between CB-Abst and CB-Mon, to characterize these randomly assigned groups. CB-Abst and CB-Mon were comparable across all baseline measures of memory (p’s > 0.16), attention (p’s > 0.35), and executive functioning (p’s > 0.06; see T2, Supplementary Table 1), except that CB-Abst had a better strategy on the SWM (p = 0.048).
Effects of abstinence
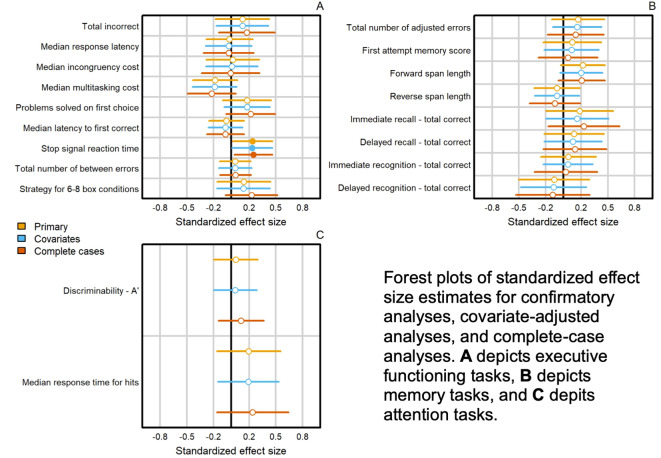
Our confirmatory contrast of interest was the average post-baseline difference between CB-Abst and CB-Mon. CB-Abst had significantly faster average reaction times on the SST module over the 4 post-baseline visits compared to CB-Mon (β = -10.9 [SE = 5.2], p = 0.037; ES = -0.24 [-0.46 to -0.01]; T3; f2). Analyses adjusted for age, sex, and baseline CUDIT-R scores (p = 0.045) and sensitivity analysis with complete cases (p = 0.02) confirmed the finding of faster reaction times on the SST among CB-Abst compared to CB-Mon. There were no other group differences in the remaining measures of executive functioning, memory, or attention (all p > 0.05).
Table 3: Confirmatory and sensitivity analysis results.
| Analysis | Module | Outcome | Test |
|---|---|---|---|
| Executive Functioning | |||
| MTT | Total incorrect | Primary | β = -0.12 [SE = 0.12]; p = 0.312 (α = 0.0125); ES = -0.12 [-0.43 to 0.18] |
| MTT | Sensitivity: Covariates | β = -0.13 [SE = 0.12]; p = 0.295 (α = 0.0125); ES = -0.12 [-0.42 to 0.17] | |
| MTT | Sensitivity: Complete cases | β = -0.18 [SE = 0.13]; p = 0.177 (α = 0.0125); ES = -0.17 [-0.49 to 0.14] | |
| MTT | Median response latency (ms) | Primary | β = 1.9 [SE = 9.3]; p = 0.836 (α = 0.0125); ES = 0.02 [-0.24 to 0.28] |
| MTT | Sensitivity: Covariates | β = 2.7 [SE = 9.1]; p = 0.769 (α = 0.0125); ES = 0.03 [-0.23 to 0.29] | |
| MTT | Sensitivity: Complete cases | β = 2.7 [SE = 10]; p = 0.789 (α = 0.0125); ES = 0.03 [-0.25 to 0.31] | |
| MTT | Median incongruency cost (ms) | Primary | β = -0.5 [SE = 3.9]; p = 0.898 (α = 0.0125); ES = -0.02 [-0.31 to 0.28] |
| MTT | Sensitivity: Covariates | β = -0.2 [SE = 3.8]; p = 0.966 (α = 0.0125); ES = -0.01 [-0.3 to 0.29] | |
| MTT | Sensitivity: Complete cases | β = 0.3 [SE = 4.2]; p = 0.949 (α = 0.0125); ES = 0.01 [-0.32 to 0.34] | |
| MTT | Median multitasking cost (ms) | Primary | β = 16.5 [SE = 9.1]; p = 0.068 (α = 0.0125); ES = 0.18 [-0.07 to 0.43] |
| MTT | Sensitivity: Covariates | β = 17.1 [SE = 9]; p = 0.059 (α = 0.0125); ES = 0.19 [-0.06 to 0.44] | |
| MTT | Sensitivity: Complete cases | β = 19.6 [SE = 9.6]; p = 0.042 (α = 0.0125); ES = 0.22 [-0.05 to 0.49] | |
| OTS | Problems solved on first choice | Primary | β = 0.15 [SE = 0.1]; p = 0.150 (α = 0.025); ES = 0.18 [-0.1 to 0.45] |
| OTS | Sensitivity: Covariates | β = 0.15 [SE = 0.1]; p = 0.121 (α = 0.025); ES = 0.18 [-0.08 to 0.44] | |
| OTS | Sensitivity: Complete cases | β = 0.19 [SE = 0.11]; p = 0.081 (α = 0.025); ES = 0.22 [-0.06 to 0.49] | |
| OTS | Median latency to first correct choice (ms) | Primary | β = 179.1 [SE = 281.8]; p = 0.525 (α = 0.025); ES = 0.06 [-0.14 to 0.25] |
| OTS | Sensitivity: Covariates | β = 212.9 [SE = 273.5]; p = 0.436 (α = 0.025); ES = 0.07 [-0.12 to 0.26] | |
| OTS | Sensitivity: Complete cases | β = 212.1 [SE = 295.1]; p = 0.472 (α = 0.025); ES = 0.07 [-0.14 to 0.28] | |
| SST | Stop signal reaction time (ms) | Primary | β = -10.9 [SE = 5.2]; p = 0.037 (α = 0.05); ES = -0.24 [-0.46 to -0.01] |
| SST | Sensitivity: Covariates | β = -10.7 [SE = 5.3]; p = 0.045 (α = 0.05); ES = -0.23 [-0.46 to -0.01] | |
| SST | Sensitivity: Complete cases | β = -10.7 [SE = 4.8]; p = 0.024 (α = 0.05); ES = -0.25 [-0.46 to -0.03] | |
| SWM | Total number of between errors | Primary | β = -0.1 [SE = 0.17]; p = 0.576 (α = 0.025); ES = -0.04 [-0.22 to 0.13] |
| SWM | Sensitivity: Covariates | β = -0.1 [SE = 0.19]; p = 0.603 (α = 0.025); ES = -0.04 [-0.23 to 0.14] | |
| SWM | Sensitivity: Complete cases | β = -0.12 [SE = 0.19]; p = 0.538 (α = 0.025); ES = -0.05 [-0.22 to 0.13] | |
| SWM | Strategy for 6–8 box conditions | Primary | β = -0.15 [SE = 0.15]; p = 0.296 (α = 0.025); ES = -0.14 [-0.44 to 0.16] |
| SWM | Sensitivity: Covariates | β = -0.15 [SE = 0.14]; p = 0.307 (α = 0.025); ES = -0.14 [-0.43 to 0.16] | |
| SWM | Sensitivity: Complete cases | β = -0.26 [SE = 0.15]; p = 0.088 (α = 0.025); ES = -0.23 [-0.52 to 0.07] | |
| Memory | |||
| PAL | Total number of adjusted errors | Primary | β = -0.19 [SE = 0.15]; p = 0.215 (α = 0.025); ES = -0.16 [-0.46 to 0.13] |
| PAL | Sensitivity: Covariates | β = -0.18 [SE = 0.14]; p = 0.206 (α = 0.025); ES = -0.16 [-0.43 to 0.12] | |
| PAL | Sensitivity: Complete cases | β = -0.16 [SE = 0.16]; p = 0.335 (α = 0.025); ES = -0.14 [-0.45 to 0.18] | |
| PAL | First attempt memory score | Primary | β = 0.1 [SE = 0.14]; p = 0.495 (α = 0.025); ES = 0.1 [-0.23 to 0.43] |
| PAL | Sensitivity: Covariates | β = 0.09 [SE = 0.13]; p = 0.507 (α = 0.025); ES = 0.09 [-0.22 to 0.4] | |
| PAL | Sensitivity: Complete cases | β = 0.05 [SE = 0.14]; p = 0.725 (α = 0.025); ES = 0.05 [-0.28 to 0.38] | |
| SSP | Forward span length | Primary | β = 0.28 [SE = 0.14]; p = 0.054 (α = 0.025); ES = 0.22 [-0.03 to 0.47] |
| SSP | Sensitivity: Covariates | β = 0.25 [SE = 0.14]; p = 0.062 (α = 0.025); ES = 0.2 [-0.04 to 0.44] | |
| SSP | Sensitivity: Complete cases | β = 0.25 [SE = 0.15]; p = 0.086 (α = 0.025); ES = 0.2 [-0.06 to 0.47] | |
| SSP | Reverse span length | Primary | β = -0.07 [SE = 0.12]; p = 0.532 (α = 0.025); ES = -0.07 [-0.33 to 0.19] |
| SSP | Sensitivity: Covariates | β = -0.07 [SE = 0.12]; p = 0.523 (α = 0.025); ES = -0.07 [-0.32 to 0.18] | |
| SSP | Sensitivity: Complete cases | β = -0.1 [SE = 0.13]; p = 0.451 (α = 0.025); ES = -0.1 [-0.38 to 0.19] | |
| VRM | Immediate recall – total correct | Primary | β = 0.09 [SE = 0.07]; p = 0.226 (α = 0.0125); ES = 0.18 [-0.19 to 0.56] |
| VRM | Sensitivity: Covariates | β = 0.08 [SE = 0.07]; p = 0.269 (α = 0.0125); ES = 0.16 [-0.2 to 0.51] | |
| VRM | Sensitivity: Complete cases | β = 0.11 [SE = 0.08]; p = 0.152 (α = 0.0125); ES = 0.23 [-0.17 to 0.63] | |
| VRM | Delayed recall – total correct | Primary | β = 0.08 [SE = 0.09]; p = 0.369 (α = 0.0125); ES = 0.12 [-0.21 to 0.46] |
| VRM | Sensitivity: Covariates | β = 0.07 [SE = 0.08]; p = 0.408 (α = 0.0125); ES = 0.11 [-0.22 to 0.43] | |
| VRM | Sensitivity: Complete cases | β = 0.08 [SE = 0.09]; p = 0.363 (α = 0.0125); ES = 0.13 [-0.23 to 0.48] | |
| VRM | Immediate recognition – total correct | Primary | β = 0.05 [SE = 0.11]; p = 0.647 (α = 0.0125); ES = 0.06 [-0.25 to 0.37] |
| VRM | Sensitivity: Covariates | β = 0.05 [SE = 0.1]; p = 0.635 (α = 0.0125); ES = 0.05 [-0.23 to 0.33] | |
| VRM | Sensitivity: Complete cases | β = 0.02 [SE = 0.12]; p = 0.839 (α = 0.0125); ES = 0.03 [-0.32 to 0.38] | |
| VRM | Delayed recognition – total correct | Primary | β = -0.06 [SE = 0.09]; p = 0.511 (α = 0.0125); ES = -0.1 [-0.5 to 0.29] |
| VRM | Sensitivity: Covariates | β = -0.07 [SE = 0.09]; p = 0.451 (α = 0.0125); ES = -0.11 [-0.48 to 0.26] | |
| VRM | Sensitivity: Complete cases | β = -0.07 [SE = 0.1]; p = 0.472 (α = 0.0125); ES = -0.12 [-0.54 to 0.3] | |
| Attention | |||
| RVP | Discriminability – A’ | Primary | β = 0.003 [SE = 0.006]; p = 0.650 (α = 0.025); ES = 0.05 [-0.2 to 0.3] |
| RVP | Sensitivity: Covariates | β = 0.002 [SE = 0.006]; p = 0.684 (α = 0.025); ES = 0.04 [-0.2 to 0.29] | |
| RVP | Sensitivity: Complete cases | β = 0.006 [SE = 0.006]; p = 0.337 (α = 0.025); ES = 0.11 [-0.15 to 0.37] | |
| RVP | Median response time for hits (ms) | Primary | β = -11.6 [SE = 9.5]; p = 0.223 (α = 0.025); ES = -0.19 [-0.55 to 0.16] |
| RVP | Sensitivity: Covariates | β = -11.4 [SE = 9.1]; p = 0.211 (α = 0.025); ES = -0.19 [-0.53 to 0.15] | |
| RVP | Sensitivity: Complete cases | β = -14.2 [SE = 10.6]; p = 0.182 (α = 0.025); ES = -0.24 [-0.64 to 0.16] | |
Highlighted rows indicate statistically significant outcomes. Adjusted alpha using Bonferroni correction shown to right of p-values.
Sensitivity analyses checked for main effects of time and group by time interactions for CB-Abst compared to CB-Mon. For memory, by week 4, participants on average had improved forward (p = 0.01) and reverse (p = 0.01) span for the SSP module but had worse immediate (p = 0.009) and delayed (p < 0.001) recognition for the VRM module. For executive functioning, participants by week 4 had on average worse error rates (p < 0.001) but improved response times (p < 0.001), incongruency costs (p < 0.001), and multitasking costs (p < 0.001) for the MTT module, and improved accuracy (p < 0.001) and response times (p < 0.001) for the OTS module. In the attention domain, by week 4, participants on average had improved discriminability (p = 0.003) for the RVP task. Across all cognitive domains, models with a group x time interaction term did not significantly outperform a simpler model with main effects only (p’s > 0.15; see Supplementary Table 3).
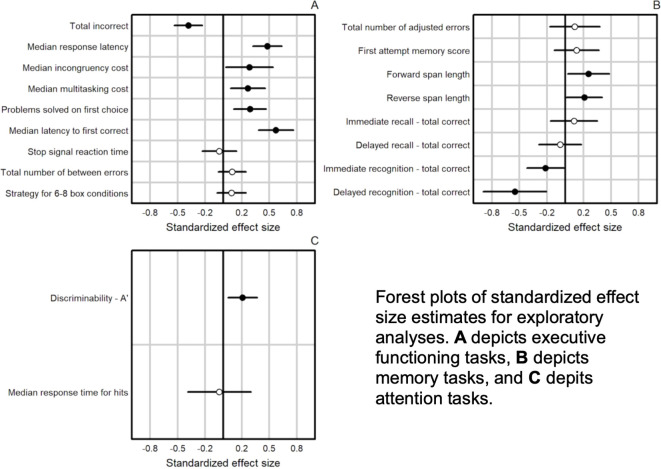
Exploratory analyses assessed whether there were differences across all outcomes for post-baseline time points among participants who used vs those who did not use cannabis. The planned contrast indicated that CB-Abst performed differently from CB-Mon on stop signal reaction time post-baseline (p = 0.038; see f3, Supplementary Tables 4.1-4.3). We did not find any significant differences between CB-Abst and NU (all p’s > 0.137) nor CB-Mon and NU (all p’s > 0.057) on any task post-baseline, implying that baseline differences between CB and NU resolved across the course of the study.
Discussion
This study offers modest evidence that cannabis abstinence improves inhibitory control. At baseline, participants who used cannabis performed worse than their non-cannabis using peers on verbal recall and processing speed tasks. Cannabis abstinence was associated with improved inhibitory control over continued cannabis use. Adolescents who abstained from cannabis use for 4 weeks performed similarly to participants who did not use cannabis across most cognitive domains tested. Improvements in some tasks of x across all groups, suggests likely practice effects.
This study suggests that inhibitory control, an aspect of executive functioning involving suppression of an automatic or prepotent response, may be sensitive to early recovery after cannabis abstinence. Prior work implicates cannabis exposure with worsened inhibitory control (ref. 49) and broader executive functioning deficits (ref. 50). Young adults who use cannabis show poorer cross-sectional inhibitory control on Go/No-Go tasks and more impulsive decision-making during gambling tasks (ref. 51), as well as altered neural activation and connectivity in frontal, parietal, and cerebellar regions during go/no-go inhibitory control tasks (ref. 52–ref. 55). THC also impairs inhibitory control in acute administration studies by increasing premature responses and commission errors on reaction-time, maze, Go/No-Go, and Stop Signal tasks (ref. 56–ref. 60). This is the first study to our knowledge to demonstrate improved executive functioning and inhibitory control during early cannabis abstinence in adolescents.
Reduced inhibitory control in adolescence may lead to risky decision-making, reduced driving safety, and may reduce an individual’s ability to regulate their own drug use. The dual-process model of addiction posits that sensitization of reward circuitry, coupled with diminished top-down control, may underpin continued drug use (ref. 61).
In exploratory analyses, participants who abstained from cannabis performed similarly to those with no cannabis use by week 4 of the study, while participants who continued their usual cannabis use performed significantly worse on tasks measuring verbal recall and processing speed, suggesting the potential for a return to cognitive baseline with cannabis abstinence among adolescents who use cannabis regularly. Other research has suggested cannabis abstinence may be associated with cognitive, structural, and neurochemical recovery (ref. 62). Future research is needed to investigate whether there are sensitive periods or turning points during adolescence that facilitate or hinder cognitive recovery with cannabis initiation and abstinence.
We also observe that all groups in the study showed improvements on several of the assessed tasks, likely due to practice effects. In this study, practice effects were evenly distributed across groups and thus do not interfere with interpretation. However, this is an important methodological point for future research aiming to identify acute changes in cognition through repeated measures over time. Investigating questions about the specific timing of abstinence effects and cognitive improvement may be challenging as a result.
This study did not find hypothesized improvements in verbal learning with cannabis abstinence as observed among older adolescents and young adults (ref. 29). This study was conducted in younger participants with a different test battery. These design differences limit direct comparison across studies. In particular, the CANTAB was designed for an older population and may lack sensitivity to detect subtle changes in cognitive functioning within this younger age group, a limitation that has been pointed out in other studies (ref. 63).
Limitations
Several limitations are worth considering. First, as noted above, the neurocognitive assessments used were not developed and age-normed for adolescents under age x which could have hampered sensitivity to detect performance changes with cannabis abstinence in this sample. Second, the 4-week window of cannabis abstinence evaluated here may be too brief to capture substantial changes in cognitive function. Additionally, NU participants were generally younger than the CB participants, reported less frequent alcohol use, and scored lower on the AUDIT at baseline. Although this might have been expected and may reflect patterns of age and symptoms among adolescents who do and do not use cannabis, it is possible that these differences contributed to variations in our cognitive variables of interest. Developmental differences between groups could have introduced residual confounds in between-group comparisons. We are also unable to account for other potential counfounds between cognitive functioning and cannabis use, for instance, education, grade level, GPA, or school engagement, which could presumably contribute to differences in cognitive functioning across groups and/or the impact of cannabis use on cognitive functioning. Additionally, although CB-Abst participants performed similarly to NU participants by Week 4, this improvement might reflect minimal change from baseline rather than true recovery. Baseline group differences and small within-group effect sizes suggest that this apparent “normalization” should be interpreted cautiously. Of note, the current study evaluates cannabis use along a binary (use versus no use), and does not account for the degree of use, which is becoming increasingly relevant as routes and doses of cannabis continue to change over time with development of new products and legalization. Differences in cannabis use frequency, route of administration, THC potency, and quantity of cannabis used during use sessions could influence changes in cognitive functioning, and future work would do well to consider these variables.
Conclusion
This longitudinal experimental study demonstrated modest improvements in inhibitory control among adolescents who abstained from regular cannabis use for one month, compared to those who did not abstain. Further research is needed to prospectively assess cognition before and after cannabis initiation as well as to evaluate the impact of cannabis abstinence in a broader age range and over a longer duration of cannabis abstinence and to understand developmental impacts in the relationship between cannabis use, discontinuation, and cognitive functioning. With increasing adolescent cannabis use amid commercialization with proliferation of product types and increasing THC potency, it is essential to deepen our understanding of the effect of cannabis exposure and abstinence in adolescence on neurocognitive performance in order to pinpoint sensitive periods when intervention might produce the greatest cognitive benefits, supporting targeted prevention and recovery-focused care for adolescents who use cannabis.
References
- AS Fischer, SF Tapert, DL Louie, AF Schatzberg, MK Singh. Cannabis and the developing adolescent brain.. Curr Treat Options Psychiatry. (, 2020. [DOI | PubMed]
- SL Godin, S Shehata. Adolescent cannabis use and later development of schizophrenia: An updated systematic review of longitudinal studies.. J Clin Psychol. (, 2022. [DOI | PubMed]
- RA Miech, LD Johnston, ME Patrick, PM O’Malley, JG Bachman, JE Schulenberg. Monitoring the Future National Survey Results on Drug Use 1975-2022: Secondary School Students., 2023
- DC D’Souza, M DiForti, S Ganesh, TP George, W Hall, C Hjorthøj. Consensus paper of the WFSBP task force on cannabis, cannabinoids and psychosis.. World J Biol Psychiatry. (, 2022. [DOI | PubMed]
- H Wilson, H Bodwitch, J Carah, KM Daane, CM Getz, TE Grantham. First known survey of cannabis production practices in California.. California Agric. (, 2019. [DOI]
- R Miech, SG Heeringa, S Molinaro, E Benedetti. Cannabis reduction among adolescents as spillover from successful tobacco control.. Int J Drug Policy. (, 2024. [DOI | PubMed]
- KH Karlsgodt. Cannabis use in adolescence: vulnerability to cognitive and psychological effects.. Biol Psychiatry Global Open Sci. (, 2023. [DOI | PubMed]
- JN Giedd, AC Vaituzis, SD Hamburger, N Lange, JC Rajapakse, D Kaysen. Quantitative MRI of the temporal lobe, amygdala, and hippocampus in normal human development: ages 4–18 years.. J Comp Neurol. (, 1996. [DOI | PubMed]
- TL Jernigan, DA Trauner, JR Hesselink, PA Tallal. Maturation of human cerebrum observed in vivo during adolescence.. Brain. (, 1991. [DOI | PubMed]
- ER Sowell, PM Thompson, SN Mattson, KD Tessner, TL Jernigan, EP Riley. Regional brain shape abnormalities persist into adolescence after heavy prenatal alcohol exposure.. Cereb Cortex. (, 2002. [DOI | PubMed]
- S Bava, SF Tapert. Adolescent brain development and the risk for alcohol and other drug problems.. Neuropsychol Review. (, 2010. [DOI | PubMed]
- KL Medina, KL Hanson, AD Schweinsburg, M Cohen-Zion, BJ Nagel, SF Tapert. Neuropsychological functioning in adolescent marijuana users: subtle deficits detectable after a month of abstinence.. J Int Neuropsychol Soc. (, 2007. [DOI | PubMed]
- N Solowij, KA Jones, ME Rozman, SM Davis, J Ciarrochi, PC Heaven. Verbal learning and memory in adolescent cannabis users, alcohol users and non-users.. Psychopharmacology. (, 2011. [DOI | PubMed]
- RJ Thoma, MA Monnig, PA Lysne, DA Ruhl, JA Pommy, M Bogenschutz. Adolescent substance abuse: the effects of alcohol and marijuana on neuropsychological performance.. Alcoholism: Clin Exp Res. (, 2011. [DOI | PubMed]
- MK Dahlgren, KA Sagar, MT Racine, MW Dremen, SA Gruber. Marijuana use predicts cognitive performance on tasks of executive function.. J Stud Alcohol Drugs. (, 2016. [DOI | PubMed]
- KM Lisdahl, JS Price. Increased marijuana use and gender predict poorer cognitive functioning in adolescents and emerging adults.. J Int Neuropsychol Soc. (, 2012. [DOI | PubMed]
- R Gonzalez, RM Schuster, RJ Mermelstein, J Vassileva, EM Martin, KR Diviak. Performance of young adult cannabis users on neurocognitive measures of impulsive behavior and their relationship to symptoms of cannabis use disorders.. J Clin Exp Neuropsychol. (, 2012. [DOI | PubMed]
- SA Gruber, KA Sagar, MK Dahlgren, MT Racine, RT Smith, SE Lukas. Splendor in the grass? A pilot study assessing the impact of medical marijuana on executive function.. Front Pharmacol. (, 2016. [DOI | PubMed]
- CW Mathias, TD Blumenthal, MA Dawes, A Liguori, DM Richard, B Bray. Failure to sustain prepulse inhibition in adolescent marijuana users.. Drug Alcohol Depend. (, 2011. [DOI | PubMed]
- NE Wade, AL Wallace, AM Swartz, KM Lisdahl. Aerobic fitness level moderates the association between cannabis use and executive functioning and psychomotor speed following abstinence in adolescents and young adults.. J Int Neuropsychol Soc. (, 2019. [DOI | PubMed]
- JM Cavalli, A Cservenka, DC Kerr, SS Tiberio, LD Owen. Ratings of executive function as a risk factor for adolescents’ frequent cannabis use: A prospective longitudinal study.. Psychol Addictive Behav. (, 2023. [DOI | PubMed]
- JC Scott, ST Slomiak, JD Jones, AFG Rosen, TM Moore, RC Gur. Association of cannabis with cognitive functioning in adolescents and young adults: A systematic review and meta-analysis.. JAMA Psychiatry. (, 2018. [DOI | PubMed]
- MA Parvaz, RA Rabin, F Adams, RZ Goldstein. Structural and functional brain recovery in individuals with substance use disorders during abstinence: a review of longitudinal neuroimaging studies.. Drug Alcohol Depend. (, 2022. [DOI | PubMed]
- LL Weyandt, CM Clarkin, EZ Holding, SE May, ME Marraccini, BG Gudmundsdottir. Neuroplasticity in children and adolescents in response to treatment intervention: A systematic review of the literature.. Clin Trans Neurosci. (, 2020. [DOI]
- JM Juraska. The last stage of development: The restructuring and plasticity of the cortex during adolescence especially at puberty.. Dev Psychobiol. (, 2024. [DOI | PubMed]
- AL Wallace, KE Maple, AT Barr, KM Lisdahl. BOLD responses to inhibition in cannabis-using adolescents and emerging adults after 2 weeks of monitored cannabis abstinence.. Psychopharmacology. (, 2020. [DOI | PubMed]
- KL Hanson, JL Winward, AD Schweinsburg, KL Medina, SA Brown, SF Tapert. Longitudinal study of cognition among adolescent marijuana users over three weeks of abstinence.. Addictive Behav. (, 2010. [DOI | PubMed]
- A Roten, NL Baker, KM Gray. Cognitive performance in a placebo-controlled pharmacotherapy trial for youth with marijuana dependence.. Addictive Behav. (, 2015. [DOI | PubMed]
- RM Schuster, J Gilman, D Schoenfeld, J Evenden, M Hareli, C Ulysse. One month of cannabis abstinence in adolescents and young adults is associated with improved memory.. J Clin Psychiatry. (, 2018. [DOI | PubMed]
- ME Cooke, SJ Knoll, JM Streck, K Potter, E Lamberth, N Rychik. Contingency management is associated with positive changes in attitudes and reductions in cannabis use even after discontinuation of incentives among non-treatment seeking youth.. Drug Alcohol Depend. (, 2024. [DOI | PubMed]
- ME Cooke, JM Gilman, E Lamberth, N Rychik, B Tervo-Clemmens, AE Evins. Assessing Changes in Symptoms of Depression and Anxiety During Four Weeks of Cannabis Abstinence Among Adolescents.. Front Psychiatry. (, 2021. [DOI | PubMed]
- RM Schuster, A Hanly, J Gilman, A Budney, R Vandrey, AE Evins. A contingency management method for 30-days abstinence in non-treatment seeking young adult cannabis users.. Drug Alcohol Depend. (, 2016. [DOI | PubMed]
- EW Schwilke, RG Gullberg, WD Darwin, CN Chiang, JL Cadet, DA Gorelick. Differentiating new cannabis use from residual urinary cannabinoid excretion in chronic, daily cannabis users.. Addiction. (, 2011. [DOI | PubMed]
- SJ Adamson, FJ Kay-Lambkin, AL Baker, TJ Lewin, L Thornton, BJ Kelly. An improved brief measure of cannabis misuse: the Cannabis Use Disorders Identification Test-Revised (CUDIT-R).. Drug Alcohol Depend. (, 2010. [DOI | PubMed]
- JB Saunders, OG Aasland, TF Babor, JR de la Fuente, M Grant. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II.. Addiction. (, 1993. [DOI | PubMed]
- I Kelleher, M Harley, A Murtagh, M Cannon. Are screening instruments valid for psychotic-like experiences? A validation study of screening questions for psychotic-like experiences using in-depth clinical interview.. Schizophr Bull. (, 2011. [DOI | PubMed]
- S Ahmed, TA Malik, A Naveed. Adaptation and concurrent validity of screen for children anxiety related emotional disorders (SCARED).. Nust J Soc Sci Humanities. (, 2020. [DOI | PubMed]
- D Watson, K Weber, JS Assenheimer, LA Clark, ME Strauss, RA McCormick. Testing a tripartite model: I. Evaluating the convergent and discriminant validity of anxiety and depression symptom scales.. J Abnormal Psychol. (, 1995. [DOI | PubMed]
- G Dutilh, J Annis, SD Brown, P Cassey, NJ Evans, RPPP Grasman. The Quality of Response Time Data Inference: A Blinded, Collaborative Assessment of the Validity of Cognitive Models.. Psychon Bull Rev. (, 2019. [DOI | PubMed]
- KY Liang, SL Zeger. Longitudinal data analysis using generalized linear models.. Biometrika. (, 1986. [DOI]
- MJ Azur, EA Stuart, C Frangakis, PJ Leaf. Multiple imputation by chained equations: What is it and how does it work?. Int J Methods Psychiatr Res. (, 2011. [DOI | PubMed]
- S Van Buuren, K Groothuis-Oudshoorn. mice: Multivariate imputation by chained equations in R.. J Stat Softw. (, 2011. [DOI]
- 43 R Core Team . R: A language and environment for statistical computing (version 4.1.1) [Computer software] (2021). R Foundation for Statistical Computing. Available online at: https://www.R-project.org. (Accessed November 11, 2022)
- 44 RStudio Team . RStudio: Integrated development environment for R (version 2020.9.0.351) [Computer software] (2021). RStudio, PBC. Available online at: http://www.rstudio.com. (Accessed November 11, 2022)
- H Wickham, R François, L Henry, K Müller. dplyr: A grammar of data manipulation (version 1.0.7). [Computer software] (, 2021
- H Wickham. tidyr: Tidy messy data (version 1.1.4). [Computer software] (, 2021
- S Hojsgaard, U Halekoh, J Yan. The R package geepack for generalized estimating equations.. J Stat Softw. (, 2006. [DOI]
- WM Landau. The targets R package: A dynamic Make-like function-oriented pipeline toolkit for reproducibility and high-performance computing.. J Open Source Softw. (, 2021. [DOI]
- KP Morie, MN Potenza. A mini-review of relationships between cannabis use and neural foundations of reward processing, inhibitory control and working memory.. Front Psychiatry. (, 2021. [DOI | PubMed]
- SG Coelho, CS Hendershot, ER Aston, AC Ruocco, LC Quilty, RF Tyndale. Executive functions and behavioral economic demand for cannabis among young adults: Indirect associations with cannabis consumption and cannabis use disorder.. Exp Clin Psychopharmacol. (, 2024. [DOI | PubMed]
- M Moreno, AF Estevez, F Zaldivar, JM Montes, VE Gutierrez-Ferre, L Esteban. Impulsivity differences in recreational cannabis users and binge drinkers in a University population.. Drug Alcohol Depend. (, 2012. [DOI | PubMed]
- B Behan, CG Connolly, S Datwani, M Doucet, J Ivanovic, R Morioka. Response inhibition and elevated parietal-cerebellar correlations in chronic adolescent cannabis users.. Neuropharmacology. (, 2014. [DOI | PubMed]
- AD Schweinsburg, SA Brown, SF Tapert. The influence of marijuana use on neurocognitive functioning in adolescents.. Curr Drug Abuse Rev. (, 2008. [DOI | PubMed]
- AM Smith, RAL Zunini, CD Anderson, CA Longo, I Cameron, MJ Hogan. Impact of marijuana on response inhibition: an fMRI study in young adults. Journal of Behavioral and Brain.. Science. (, 2011. [DOI]
- SF Tapert, AD Schweinsburg, SPA Drummond, MP Paulus, SA Brown, TT Yang. Functional MRI of inhibitory processing in abstinent adolescent marijuana users.. Psychopharmacology. (, 2007. [DOI | PubMed]
- C Hart, W van Gorp, M Haney, R Foltin, M Fischman. Effects of acute smoked marijuana on complex cognitive performance.. Neuropsychopharmacology. (, 2001. [DOI | PubMed]
- JG Ramaekers, G Kauert, P van Ruitenbeek, EL Theunissen, E Schneider, MR Moeller. High-potency marijuana impairs executive function and inhibitory motor control.. Neuropsychopharmacology. (, 2006. [DOI | PubMed]
- J Ramaekers, G Kauert, E Theunissen, S Toennes, M Moeller. Neurocognitive performance during acute THC intoxication in heavy and occasional cannabis users.. J Psychopharmacol. (, 2009. [DOI | PubMed]
- JHP van Wel, KPC Kuypers, EL Theunissen, SW Toennes, DB Spronk, RJ Verkes. Single doses of THC and cocaine decrease proficiency of impulse control in heavy cannabis users: single doses of THC and cocaine increase impulsivity.. Br J Pharmacol. (, 2013. [DOI | PubMed]
- A Weinstein, O Brickner, H Lerman, M Greemland, M Bloch, H Lester. A study investigating the acute dose— response effects of 13 mg and 17 mg Δ 9- tetrahydrocannabinol on cognitive—motor skills, subjective and autonomic measures in regular users of marijuana.. J Psychopharmacol. (, 2008. [DOI | PubMed]
- X Noel, D Brevers, A Bechara. A neurocognitive approach to understanding the neurobiology of addiction.. Curr Opin Neurobiol. (, 2013. [DOI | PubMed]
- C Meza, C Stefan, WR Staines, A Feinstein. The effects of cannabis abstinence on cognition and resting state network activity in people with multiple sclerosis: A preliminary study.. NeuroImage: Clin. (, 2024. [DOI | PubMed]
- HJ Syväoja, TH Tammelin, T Ahonen, P Räsänen, A Tolvanen, A Kankaanpää. Internal consistency and stability of the CANTAB neuropsychological test battery in children.. psychol Assess. (, 2015. [DOI | PubMed]