
Behavioral phenotypes associated with cannabis and alcohol substitution
Abstract
Objective:
Alcohol and cannabis co-use is the most common form of polysubstance use in the U.S. Some evidence suggests that there is an association between cannabis use and reduced alcohol consumption, however data on this topic are mixed. Further research is needed to elucidate the individual factors that determine whether cannabis substitutes for alcohol.
Method:
This study is an exploratory analysis of data from a within-subjects, crossover laboratory study on alcohol and cannabis co-administration. Participants completed two sessions: one in which they self-administered alcohol after using cannabis, and one in which they self-administered alcohol but did not use cannabis. We aim to compare behavioral phenotypes of individuals who self-administered less alcohol after cannabis (“substituters”; n = 23), more alcohol after cannabis (“complementers”; n = 7), or the same amount of alcohol regardless of whether cannabis was used (“non-substituters”; n = 16). We utilized Welch’s ANOVAs and Kruskal-Wallis tests to compare baseline group differences, drawing on domains from the Addictions Neuroclinical Assessment (ANA) framework. Wilcoxon tests were employed to test differences in laboratory self-administration measures between sessions for each group.
Results:
Substituters had significantly lower scores on measures corresponding to ANA domains of negative emotionality (BDI-II, DASS-Depression) and executive function (UPPS-P Lack of Premeditation) than non-substituters. Substituters endorsed higher positive cannabis expectancies than non-substituters, though expectancy differences did not reach significance.
Conclusions:
Individuals who use cannabis and alcohol and have lower levels of negative emotionality and impulsivity may be more likely to substitute cannabis for alcohol. Future research is needed to explore long-term outcomes of cannabis substitution.
Clinical trials registration number:
NCT04998006.
Supplementary Information:
The online version contains supplementary material available at 10.1186/s12954-026-01432-y.
Article type: Research Article
Keywords: Alcohol, Cannabis, Substitution, Simultaneous use, Behavioral phenotyping
Affiliations: https://ror.org/03k1gpj17grid.47894.360000 0004 1936 8083Department of Psychology, Colorado State University, Fort Collins, CO USA; https://ror.org/02ttsq026grid.266190.a0000 0000 9621 4564Department of Psychology and Neuroscience, University of Colorado Boulder, Boulder, CO USA; https://ror.org/03wmf1y16grid.430503.10000 0001 0703 675XDepartment of Psychiatry, University of Colorado Anschutz Medical Campus, Aurora, CO USA; https://ror.org/03k1gpj17grid.47894.360000 0004 1936 8083Department of Environmental and Radiological Health Sciences, Colorado State University, CO Fort Collins, USA
License: © The Author(s) 2026 CC BY 4.0 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Article links: DOI: 10.1186/s12954-026-01432-y | PubMed: 41792806 | PMC: PMC13078031
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (2.1 MB)
Introduction
Widespread legalization of cannabis in recent years has contributed to a steady increase in co-use of cannabis and alcohol in the U.S. [ref. 16], with recent estimates of 8.4% of adults aged 30–80 reporting current co-use [ref. 58]. Co-use of alcohol and cannabis includes use that occurs simultaneously (such that intoxicating effects overlap), as well non-overlapping (concurrent) use [ref. 55]. Co-use (particularly simultaneous co-use) has been associated with increased risk of poorer mental health and academic outcomes, engagement in risky behavior, and other harmful experiences, especially among young people [ref. 8, ref. 28, ref. 39, ref. 47, ref. 56]. Individuals often engage in simultaneous use for the “complementary” effects of the substances [ref. 7], which may lead to increased alcohol consumption during simultaneous use relative to alcohol-only use events [ref. 39, ref. 55]. Conversely, there is also considerable evidence suggesting that for some individuals, using cannabis and alcohol at the same time, particularly when cannabis is used first, results in decreased alcohol consumption (i.e., “substitution”) and reduced craving [ref. 34, ref. 41]. Further research is needed to elucidate individual factors associated with different patterns of alcohol and cannabis co-use.
The Addictions Neuroclinical Assessment (ANA) framework may offer insight into behavioral phenotypes that may be associated with specific alcohol-cannabis co-use patterns. The ANA framework has been proposed as a tool for developing precision medicine approaches to treating alcohol and substance use disorders (ASUDs), consisting of 3 functional domains that map onto the 3 stages of the addiction cycle [ref. 25, ref. 27]. The Incentive Salience domain encapsulates processes such as attentional bias and cue-induced craving in response to drug-related stimuli, corresponding with the Binge-Intoxication stage of the addiction cycle [ref. 25, ref. 27]. The Negative Emotionality domain reflects negative emotional states associated with addictive disorders, including withdrawal, reflecting the Withdrawal-Negative affect stage [ref. 25, ref. 27]. Lastly, the Executive Function domain reflects dysfunction in processes related to planning and organizing goal-directed behaviors, which involves attention inhibition, working memory, and behavioral and cognitive adaptation, which maps onto the Preoccupation-Anticipation stage [ref. 27]. This framework allows deep phenotyping across these theory-derived functional domains, with the goal of identifying subgroups within a population who are most likely to respond to a given intervention [ref. 27]. While this framework was designed for use in clinical populations, a prior study validated a 4-factor structure in a sample of “problem drinkers” with and without AUD diagnoses, comprised of the three neurofunctional domains and an additional factor representing alcohol-related problems [ref. 36]. We propose that this framework may therefore offer utility in identifying behavioral phenotypes associated with cannabis and alcohol co-use patterns (e.g., substitution) in at-risk populations who do not necessarily have clinical diagnoses.
For example, a recent laboratory study employed a controlled-dose, parallel design to investigate the effect of smoked cannabis (< 0.3% placebo vs. 3.1%, 7.2% active THC) on alcohol consumption and craving in individuals who engage in heavy episodic drinking [ref. 34]. The 7.2% THC dose was associated with a significant reduction in alcohol urge after smoking (ANA incentive salience domain) compared to placebo and both active doses were associated with a significant reduction in alcohol consumed in an alcohol self-administration task compared to placebo [ref. 34]. This is consistent with findings from our crossover laboratory study wherein a subset of individuals experienced reductions in alcohol craving and consumption when cannabis was self-administered ad libitum before alcohol compared to when alcohol was self-administered without cannabis [ref. 41].
Several studies have also found associations between cannabis and alcohol co-use (both concurrent and simultaneous) and dimensions relevant to executive functioning, namely impulsivity [ref. 11, ref. 43, ref. 64, ref. 66, ref. 67] and challenges with emotion regulation [ref. 30, ref. 35]. One study found that lower levels of positive urgency and lack of perseverance were associated with reduced alcohol consumption on co-use days relative to alcohol-only days (consistent with substitution) in a sample of veterans [ref. 66]. Daros et al. [ref. 11] also found there was a stronger positive relationship between grams of cannabis used and number of standard drinks consumed on a given day for young adults high in negative urgency and behavioral disinhibition [ref. 11]. Higher levels of impulsivity may therefore increase risk of alcohol-related harms in the context of simultaneous use. However, the relationship between grams of cannabis and any same day drinking was higher for individuals low in negative urgency and disinhibition, which the authors speculated may reflect planned, context-specific substance use (e.g., weekend social events) [ref. 11].
In terms of the ANA negative emotionality domain, prior studies have found associations between anxiety and depression symptoms and increased alcohol consequences and odds of AUD diagnosis for both concurrent and simultaneous alcohol and cannabis use [ref. 15, ref. 33, ref. 62, ref. 63]. This suggests that greater negative emotionality may be a risk factor for greater alcohol related harms. Moreover, in an EMA study, Wycoff and Trull, [ref. 72] found that higher coping motives for drinking were associated with increases in anxious and depressed mood from the last moment, but this association was attenuated in simultaneous use relative to alcohol-only use moments [ref. 72]. This study did not explicitly show that lower negative emotionality is linked to substitution, but we hypothesize that the effect of simultaneous cannabis use on coping-motivated drinking could facilitate increased alcohol consumption in individuals with higher levels of negative affect via negative reinforcement mechanisms, based on these prior data. No prior study to date has explicitly examined how ANA phenotypes relate to substitution behavior during simultaneous use events in the laboratory.
To fill gaps in the literature and build upon prior data, the present secondary analysis is focused on linking ANA-derived behavioral phenotypes to alcohol and cannabis self-administration behavior in the lab. We leverage data from our aforementioned crossover laboratory study [ref. 41], involving two lab sessions: one “alcohol only” self-administration session and one session in which participants self-administered cannabis prior to alcohol self-administration (NCT04998006). Three groups (“substituters” who drank less during the Cannabis+Alcohol [CA] lab session compared to the Alcohol only [AO] lab session, “non-substituters”, who drank the same amount at both sessions, and “complementers”, who drank more at the CA session than the AO session) were derived from our data post hoc, based on observed drinking behavior during the CA and AO lab sessions [ref. 41]. Given emerging evidence from the ANA literature linking negative emotionality [ref. 15, ref. 33, ref. 62, ref. 63, ref. 72], impulsivity [ref. 60, ref. 64, ref. 66–ref. 68] and incentive salience [ref. 34, ref. 65] to alcohol and cannabis co-use behavior, we hypothesized that substituters would have significantly lower scores across measures of trait impulsivity, negative emotionality, and incentive salience administered at baseline, compared to non-substituters and complementers.
Methods
All methods were approved by Colorado State University’s Institutional Review Board. Data were collected as part of a larger study [ref. 41].
Participants
Participants were recruited from the community using flyers, outreach at community events, and online advertisements. They met NIAAA heavy-drinking criteria (> 4 drinks on any day or > 14 drinks per week for males; > 3 drinks on any day or > 7 drinks per week for women) [ref. 38], endorsed using flower cannabis > = 3 times/week for at least three months, had not been diagnosed with an alcohol or substance use disorder (AUD/SUD) and were not currently seeking treatment. Exclusion criteria are described in the Supplementary Materials.
Procedure
Eligible participants completed three appointments: one baseline session conducted in our on-campus lab and two sessions in our mobile laboratory, which travels to the participant’s residence and parks outside their home for the duration of the visit (Alcohol only session = AO, Cannabis + Alcohol session = CA). The mobile laboratory methodology allows for the study of legal market cannabis self-administration while complying with state and federal laws that prohibit researchers from bringing legal-market cannabis onto a university campus. Study appointments were separated by 2-weeks and the order of mobile laboratory visits was counterbalanced across participants.
Baseline appointment
At the baseline appointment, participants underwent informed consent and eligibility verification procedures, including drug urinalysis (and pregnancy test when applicable) and a breathalyzer test. Eligible participants completed a series of surveys capturing demographics, substance use and psychological functioning, and medical and mental health history. Participants also completed an online timeline follow back documenting their substance use over the past 60 days (OTLFB; [ref. 32]). Participants were then provided with instructions for their mobile laboratory appointments. For the purposes of a separate study aim, participants were asked to try to abstain from cannabis use but to drink alcohol as they normally would up in the 2 weeks prior to session AO, up until 24 h before the mobile lab session. In the two weeks preceding session CA, participants were asked to use alcohol and cannabis as they normally would up until 24 h before the mobile lab session. Participants were asked not to use any drugs (including cannabis) or alcohol in the 24 h leading up to each mobile lab sessions.
Mobile laboratory sessions
At both laboratory visits, participants completed a blood draw and were then given an alcohol priming drink (prepared using the Widmark formula targeting breath alcohol concentration [BrAC] of 0.03 g/dL). Next, (for both AO and CA) participants completed an alcohol self-administration task, wherein they had the opportunity to receive 4 drinks of their preferred alcohol (e.g. beer, wine, liquor) over the course of one hour (1 drink was offered every 15 minutes, with each drink targeting a 0.015 g/dL increase in BrAC), or alternatively receive an additional $1 per drink refused1, consistent with typical bar-lab procedures which offer small monetary incentives for not consuming drinks, to create a decisional balance between drinking and abstaining [ref. 45, ref. 46]. Participants also completed questionnaires assessing alcohol craving throughout the self-administration period, for which the results are presented in Pince et al. [ref. 41]. All procedures were identical at sessions AO and CA up until the first blood draw, after which participants self-administered their own legal-market flower cannabis product inside their residence prior to receiving the priming drink.
There were three venous blood draws to assess levels of blood cannabinoids over the course of the study; one blood draw occurred before the priming drink at session AO and two occurred at session CA (one before cannabis self-administration and one immediately upon returning to the mobile lab after self-administering cannabis). The second blood draw post-cannabis use at session CA is used to verify that participants used cannabis during the session. Plasma was extracted from blood samples and stored at −80 °C until being assayed for THC and metabolites (11-OH-THC, THC-COOH) using High Performance Liquid Chromatography-Tandem Mass Spectrometry [ref. 9, ref. 12, ref. 23]. A detailed description of blood cannabinoid assay methods are included in Supplementary Materials. For further information on study procedures, see NCT04998006 and our prior publication [ref. 41].
Measures
At the baseline visit, participants completed a series of surveys related to demographic characteristics, substance use, personality, and psychological functioning, which mapped onto ANA domains. Consistent with previous studies [ref. 18, ref. 36, ref. 37], we utilized the Penn Alcohol Craving Scale (PACS) [ref. 14] and the Alcohol Use Disorders Identification Test (AUDIT) [ref. 44] to capture the incentive salience domain. As the majority of research on ANA has focused on alcohol, we use comparable measures to capture cannabis-related incentive salience, including The Marijuana Dependence Scale (MDS) [ref. 52] and Marijuana Craving Questionnaire (MCQ) [ref. 22]. The AUDIT and MDS were also employed to screen for AUD and CUD symptomatology. For the negative emotionality domain, we used The Beck Depression Inventory II (BDI-II) [ref. 5] and Beck Anxiety Inventory II (BAI) [ref. 4], which have been employed in prior studies [ref. 27, ref. 61]. We also included the Depression-Anxiety-Stress-Scale (DASS) to capture a wider range of negative affective states [ref. 29]. For the executive function domain, we used the Urgency, Premeditation, Perseverance, Sensation Seeking, and Positive urgency Impulsive Behavior Scale (UPPS-P) [ref. 10, ref. 70], the Impaired Control Scale (ICS) [ref. 21 ], and Barratt Impulsiveness Scale (BIS-15) short-form [ref. 40, ref. 48], which have been represented in prior ANA literature [ref. 18, ref. 26, ref. 36, ref. 37, ref. 50]. We also included the Impulsive Sensation Seeking Scale (ImpSS) [ref. 73], as impulsivity and sensation seeking personality traits represent potential risk and maintaining factors for SUDs relevant to the executive function ANA domain [ref. 57]. The ImpSS has been shown to predict substance use amongst undergraduates as well as relapse amongst individuals with SUDs [ref. 1, ref. 20]. We also included the Difficulties in Emotion Regulation Scale (DERS) [ref. 6, ref. 17], as emotion regulation engages cognitive control dimensions of executive functioning, which are thought to be disrupted in individuals with SUDs [ref. 31, ref. 71]. A recent meta-analysis revealed that individuals with SUDs lower on the DERS, specifically in the strategies and impulse subscales [ref. 51]. A detailed description of each measure is included in the Supplementary Materials.
Data analysis
Participants who completed both mobile laboratory sessions were categorized as either “substituters” (self-administered fewer drinks after using cannabis compared to alcohol alone), “complementers” (self-administered more drinks after using cannabis compared to alcohol alone), or “non-substituters” (self-administered the same number of drinks after using cannabis + alcohol compared to alcohol alone), as described in our prior publication [ref. 41]. Individuals who did not self-administer any alcohol during either laboratory session were excluded from the present analyses. We assessed group differences in baseline substance use, mobile laboratory measures, and measures of personality and psychological functioning, using Welch’s ANOVAs and Kruskal-Wallis non-parametric tests depending on variable distributions. Group differences in demographics were also evaluated using Fisher’s exact tests. When significant group differences were observed, post-hoc pairwise comparisons were conducted with a Bonferroni correction. Within-subject differences for mobile laboratory measures (e.g., blood THC, number of drinks self-administered) for each group were evaluated using pairwise Wilcoxon signed-rank tests. When statistically significant group differences in behavioral phenotyping measures were found, data were visualized with boxplots (non-significant statistics are reported in Supplementary Materials). Descriptive statistics for behavioral phenotyping measures for each group are included in the Supplementary Materials. All statistical analyses were performed using RStudio statistical software [ref. 42].
Results
Group characteristics
Sixty-one participants completed both mobile laboratory appointments. Participants who chose not to self-administer any alcohol at either appointment (n = 15) were excluded from analyses, resulting in a final sample of 46, 50% of which were classified as substituters (self-administered at least one more drink at session AO compared to CA; n = 23), 34.7% as non-substituters (self-administered the same number of drinks at session AO and CA; n = 16), and 15.3% as complementers (self-administered at least one more drink at session CA compared to AO; n = 7). Based on clinical cutoffs from the Alcohol Use Disorders Identification Test and Marijuana Dependence Scale, a majority of our final sample (64.7%) met criteria for at least mild AUD (AUDIT > = 8) and almost half (43.5%) met criteria for CUD (MDS > = 3) at baseline, nearly a third of which met criteria for both AUD and CUD (28.2%). Only 8 individuals (17.4%) didn’t meet criteria for either diagnosis based on AUDIT and MDS scores.
Regarding baseline substance use, Kruskal-Wallis tests revealed significant group differences in typical drinks per drinking day in the past 2 months (χ2(2) = 7.63, p <.05). There were trends towards non-substituters consuming more drinks per drinking day compared to complementers (Z = 2.36, p =.06) and substituters (Z = 2.31, p =.06). There were no other significant group differences in baseline alcohol use frequency or cannabis use frequency and quantity, nor did Fisher’s tests reflect significant demographic differences between groups (Table 1). In the mobile laboratory, substituters self-administered an average of 2.96 (SD = 1.19) drinks at session AO and 1 drink (SD = 1.21) at session CA, with a Wilcoxon test revealing a statistically significant difference (Z = −4.18, p <.001) with a large effect size (r =.87). Non-substituters self-administered an average of 3.19 drinks (SD = 1.22) at both sessions. Complementers self-administered an average of 0.71 drinks (SD = 0.76) at session AO and 2.71 drinks (SD = 1.38) at session CA, which was a statistically significant difference (Z = −2.28, p <.001) with a large effect size (r =.86). Kruskal-Wallis tests revealed significant group differences in drinks self-administered at session AO (χ2(2) = 14.61, p <.001) and session CA (χ2(2) = 20.55, p <.001). Complementers self-administered significantly fewer drinks at session AO compared to non-substituters (Z = −3.67, p <.001) and substituters (Z = −3.41, p =.001), but there were no significant differences between non-substituters and substituters (Z = 0.60, p =.55). In contrast, substituters self-administered significantly fewer drinks at session CA compared to non-substituters (Z = −4.44, p <.001) and complementers (Z = −2.59, p =.02) (Table 2).
Table 1: Group demographics and baseline substance use
| Substituter(n = 23) | Non-substituter(n = 16) | Complementer(n = 7) | |
|---|---|---|---|
| Demographics | |||
| Gender, n (%) | |||
| Cisgender Man | 16 (69.6%) | 9 (56.25%) | 2 (28.6%) |
| Cisgender Woman | 6 (26.1%) | 7 (43.75%) | 4 (57.1%) |
| Non-binary | 1 (4.3%) | 0 (0%) | 1 (14.3%) |
| Sex assigned at birth,Male, n (%) | 16 (69.6%) | 9 (56.3%) | 3 (42.8%) |
| Age, mean (S.D.) | 31.9 (11.2) | 30.3 (9.0) | 27.6 (7.0) |
| Race/Ethnicity, n (%) | |||
| Asian | 1 (4.3%) | 0 (0%) | 0 (0%) |
| Black or African American | 1 (4.3%) | 0 (0%) | 0 (0%) |
| Hispanic/Latino | 4 (17.4%) | 0 (0%) | 1 (14.3%) |
| Multiracial/ethnic | 3 (13%) | 0 (0%) | 0 (0%) |
| White | 14 (61%) | 16 (100%) | 6 (85.7%) |
| Education, n (%) | |||
| High School | 1 (4.3%) | 3 (18.75%) | 0 (0%) |
| Some college | 5 (21.8%) | 4 (25.0%) | 4 (57.1%) |
| Associates/Technical degree | 5 (21.8%) | 2 (12.5%) | 0 (0%) |
| Bachelor’s degree | 10 (43.5%) | 5 (31.25%) | 3 (42.8%) |
| Master’s degree | 1 (4.3%) | 2 (12.5%) | 0 (0%) |
| Doctoral degree | 1 (4.3%) | 0 (0%) | 0 (0%) |
| Employment, n (%) | |||
| Full-time | 9 (39.1%) | 7 (43.75%) | 3 (42.8%) |
| Part-time | 6 (26.1%) | 3 (18.75%) | 1 (14.3%) |
| Unemployed, disabled, orretired | 4 (17.4%) | 2 (12.5%) | 1 (14.3%) |
| Student full-time | 3 (13%) | 3 (18.75%) | 2 (28.6%) |
| Stay-at-home parent | 1 (4.4%) | 1 (6.25%) | 0 (0%) |
| Annual Income, n (%) | |||
| Less than $10,000 | 5 (21.75%) | 5 (31.25%) | 1 (14.3%) |
| $10,000–20,000 | 2 (8.7%) | 1 (6.25%) | 0 (0%) |
| $20,000–30,000 | 5 (21.75%) | 4 (25.0%) | 1 (14.3%) |
| $30,000–40,000 | 2 (8.7%) | 0 (0%) | 1 (14.3%) |
| $40,000–50,000 | 1 (6.25%) | 1 (6.25%) | 1 (14.3%) |
| $50,000–60,000 | 6 (26.1%) | 3 (18.75%) | 3 (42.8%) |
| Greater than $60,000 | 2 (6.25%) | 1 (6.25%) | 0 (0%) |
| Baseline substance use characteristics | |||
| Alcohol use days in past 60 days(O-TLFB), mean (S.D.) | 21.70 (17.20) | 25.62 (15.18) | 31.43 (14.52) |
| Drinks per drinking day (O-TLFB), mean (S.D.)1 | 3.60 (1.27) 1 | 5.20 (2.02) 1 | 3.41 (1.91) |
| Flower cannabis days in past 60days (O-TLFB), mean (S.D.) 1 | 31.3 (22.3)1 | 31.44 (21.39) | 25.14 (24.60) |
| Grams flower cannabis used perday (O-TLFB), mean (S.D.) 1 | 0.65 (0.70) | 0.53 (0.47) | 0.27 (0.10) |
1data missing for one participant; 2data missing from two participants
Table 2: Group mobile laboratory self-administration descriptives
| Substituter(n = 23) | Non-substituter(n = 16) | Complementer(n = 7) | ||
|---|---|---|---|---|
| Alcohol self-administration | ||||
| Drinks self-administered | ||||
| Session AO, mean (S.D.) | 2.96 (1.19) | 3.19 (1.22)### | 0.71 (0.76)### | |
| Session CA, mean (S.D.) | 1.00 (1.21) | 3.19 (1.22)### | 2.71 (1.38)# | |
| Session CA vs. AO, mean difference | 1.96 (1.11)*** | 0 (0.00) | −2.00 (1.29)** | |
| Cannabis self-administration | ||||
| Grams flower cannabis, mean (S.D.) | 0.46 (0.61) | 0.42 (0.58) | 0.25 (0.17) | |
| THC percentage, mean (S.D.) | 23.2 (5.05) | 23.1 (4.71) | 20.1 (2.98) | |
| Flower cannabis strain. n (%)1 | ||||
| Sativa | 9 (45%) | 5 (31.25%) | 2 (28.6%) | |
| Indica | 4 (25%) | 2 (12.5%) | 3 (42.8%) | |
| Hybrid | 7 (35%) | 9 (56.25%) | 2 (28.6%) | |
| Blood cannabinoid concentrations (ng/mL)2 | ||||
| Blood THC concentration, mean (S.D.) | ||||
| Baseline AO | 9.65 (19.0) | 5.78 (7.99) | 12.01 (15.45) | |
| Baseline CA | 11.72 (23.03) | 4.34 (5.16) | 7.30 (14.16) | |
| Post-use CA | 193.26 (229.16) | 140.39 (159.70) | 129.84 (135.25) | |
| Baseline CA vs. AO difference | 2.47 (6.63)* | −0.90 (3.75) | 0.15 (11.31) | |
| Baseline CA vs. Post-use difference | 190.59 (216.61)*** | 126.20 (157.09)*** | 117.68 (123.52)* | |
| Blood 11-OH-THC concentration, mean (S.D.) | ||||
| Baseline AO | 3.43 (5.16) | 2.42 (3.58) | 4.94 (7.15) | |
| Baseline CA | 3.62 (4.95) | 1.87 (2.25) | 6.41 (7.30) | |
| Post-use CA | 11.08 (11.09) | 16.01 (17.67) | 20.07 (21.50) | |
| Baseline CA vs. AO difference | 0.52 (1.52) | −0.38 (1.55) | 1.47 (6.31) | |
| Baseline CA vs. Post-use difference | 7.58 (8.47)*** | 12.62 (15.72)*** | 13.65 (15.49)* | |
| Blood THC-COOH concentration, mean (S.D.) | ||||
| Baseline AO | 78.23 (111.29) | 69.03 (102.62) | 96.98 (153.07) | |
| Baseline CA | 86.88 (115.61) | 65.74 (104.87) | 86.76 (101.12) | |
| Post-use CA | 128.81 (138.04) | 135.75 (166.44) | 119.67 (130.49) | |
| Baseline CA vs. AO difference | 17.30 (45.70) | 2.24 (35.04) | −10.23 (60.71) | |
| Baseline CA vs. Post-use difference | 39.19 (73.36)** | 54.18 (58.38)*** | 32.92 (31.52)* | |
1n = 43, missing strain information for 3 substituters; 27 individuals had one missing blood timepoint, 2 had two missing timepoints and 3 had three, due to difficulty with blood draws. #p <.05, ### p <.001, between-group, within-timepoint comparison; *p <.05, ** p <.01, ***p <.001, within-group, between-timepoint comparison
Regarding cannabis self-administration, Kruskal-Wallis tests indicated no significant group differences in the amount or potency of flower cannabis used during session CA. On average, participants self-administered an average of 0.37 g (SD = 0.48) of flower cannabis with a THC content of 22.82% (SD = 22.48). All groups experienced a significant increase in blood THC concentrations between baseline and post-cannabis use (p <.05). On average, baseline blood THC concentration was 8.61 ng/mL (SD = 15.15) at session AO and 9.02 ng/mL (SD = 17.13) at CA, with an average post-use concentration of 165.24 ng/mL (SD = 193.00). While there were no significant group differences in blood THC or metabolites at any timepoint, Wilcoxon tests revealed that only substituters had significantly higher baseline blood THC concentrations at session CA compared to AO (Z = 2.25, p =.02), with a medium effect size (r =.47) (Table 2).
Incentive salience measures
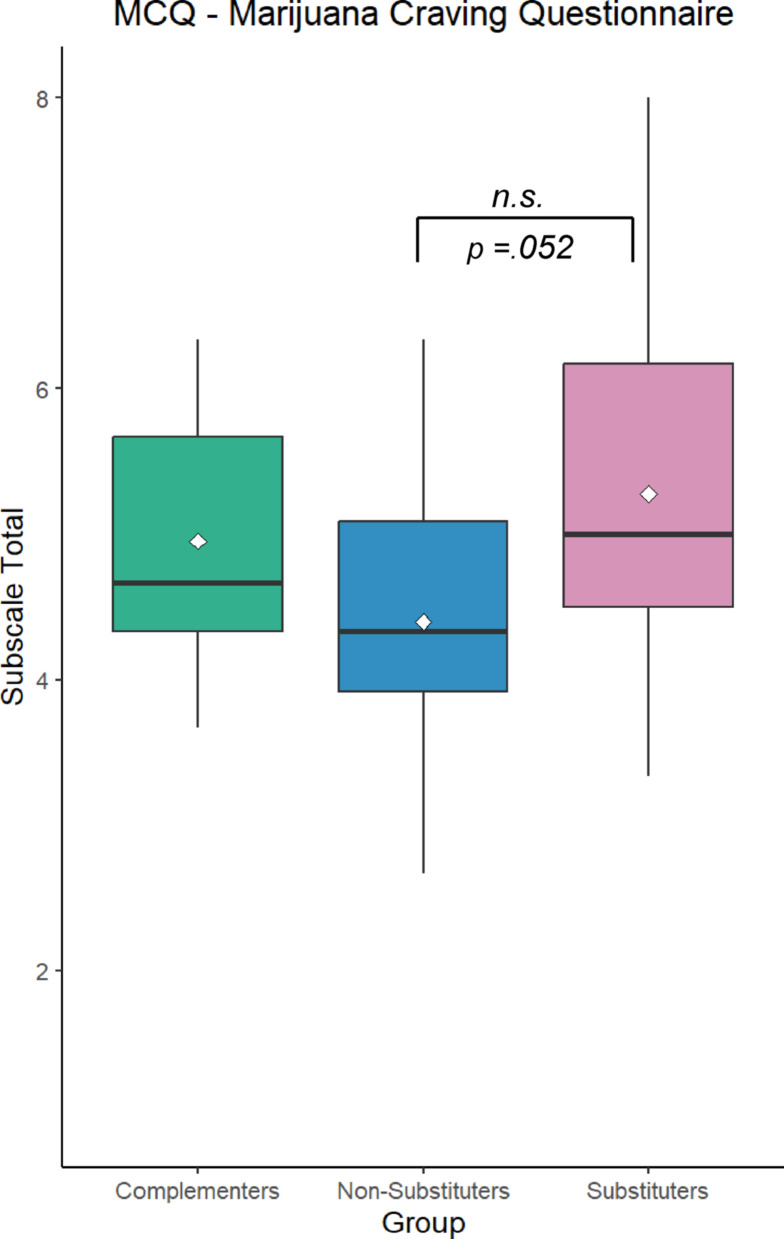
A Welch’s ANOVA revealed a trend towards a significant group difference for the Expectancy subscale of the MCQ (Fw(17.8,2) = 2.87, p =.08), with post-hoc analyses indicating a trend towards substituters scoring higher than non-substituters (p =.052) (Fig. 1). There were no significant group differences for any other subscales of the MCQ nor the PACS, MDS, or AUDIT (Supplementary Materials).
Negative emotionality measures
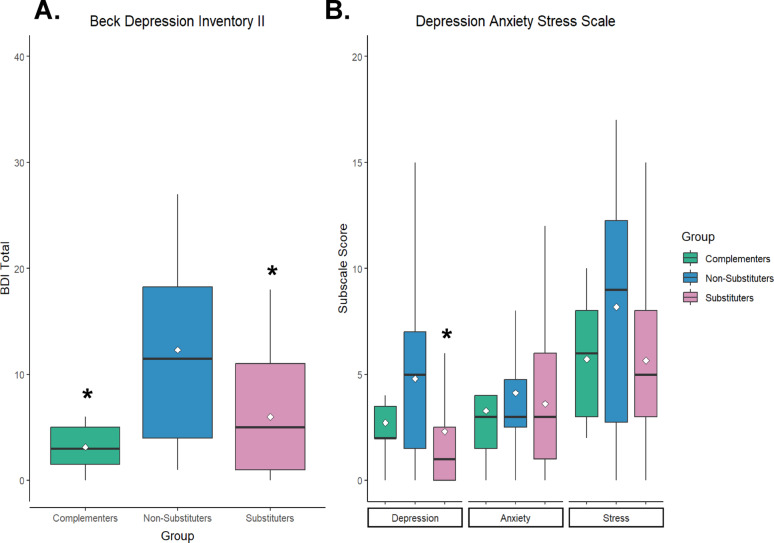
A Kruskal-Wallis test indicated significant group differences in scores on the BDI-II (χ2(2) = 8.79, p =.01), with a large effect size (η2 = 0.16). Post-hoc analyses revealing that substituters (Z = −2.44, p =.04) and complementers (Z = −2.55, p =.03) scored significantly lower than non-substituters. There were also significant group differences in DASS Depression subscale scores (χ2(2) = 6.60, p =.04), with a medium effect size (η2 = 0.11). Post-hoc analyses indicated substituters scored significantly lower than non-substituters (Z = −2.56, p =.03) (Fig. 2). There were no significant group differences in BAI scores or DASS Stress or Anxiety subscales (Supplementary Materials).
Executive function measures
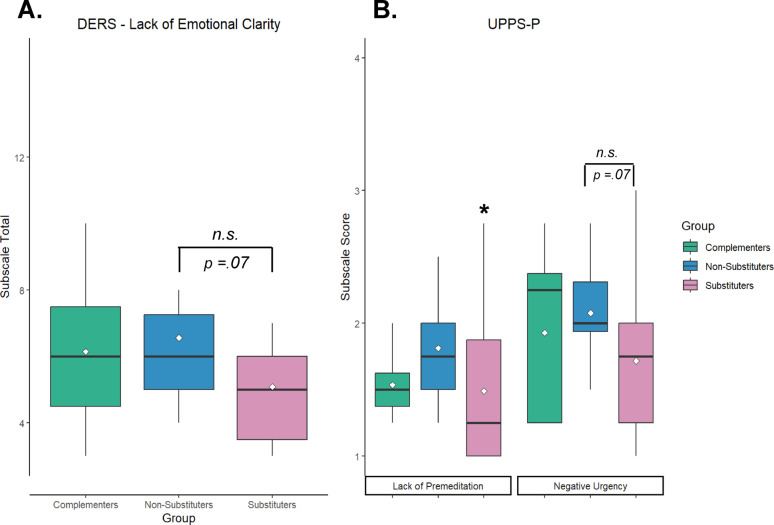
A Kruskal-Wallis test revealed significant group differences in UPPS-P Lack of Premeditation subscale scores (χ2(2) = 6.06, p = .048), with a medium effect size (η2 = 0.09). Post-hoc analyses showed that substituters scored significantly lower than non-substituters (Z = −2.45, p =.04). There was also a trend towards group differences in UPPS-P Negative Urgency subscale scores (χ2(2) = 5.32, p =.07), with post-hoc tests indicating substituters scored lower than non-substituters (Z = −2.25, p =.07). There were no significant differences between complementers and substituters or non-substituters on either of these subscales. A Kruskal-Wallis test demonstrated a trend towards a difference in the Lack of Emotional Clarity subscale of the DERS (χ2(2) = 5.55, p =.06), whereby substituters scored lower than non-substituters (Z = 2.26, p =.07) (Fig. 3). There were no significant group differences in scores on any other DERS subscales, nor ImpSS, ICS, or BIS subscales (Supplementary Materials).
Discussion
In this novel laboratory study, we used the ANA framework [ref. 27] to characterize behavioral phenotypes associated with alcohol and cannabis self-administration behavior, as no studies to date have examined how ANA phenotypes relate to co-use behavior during simultaneous use events in the laboratory. We hypothesized that substituters would have significantly lower scores across measures of impulsivity, negative emotionality, and incentive salience administered at baseline, compared to non-substituters and complementers. Findings partially supported hypotheses, as both substituters and complementers reported significantly lower levels of depression compared to non-substituters. Substituters also endorsed significantly lower lack of premeditation than non-substituters.
Higher scores on lack of premeditation and depression among non-substituters in the present study may reflect a behavioral pattern of impulsive drinking during co-use to alleviate negative affect [ref. 2, ref. 49, ref. 59, ref. 66, ref. 72], whereas lower depression and greater premeditation among substituters may contribute to more conscientious drinking choices [ref. 11]. In recent work, the simultaneous use of cannabis with alcohol has been shown to attenuate increases in negative affect associated with coping-motivated drinking, which may reflect an underlying negative reinforcement mechanism unique to simultaneous use [ref. 72]. Further, recent work by Wardell and colleagues [ref. 69] showed a within-person association between internalizing symptoms (i.e., depression, anxiety, and stress) and number of heavy drinking simultaneous use days via reward/enhancement motives [ref. 69]. However, at the between-person level, greater average internalizing symptoms were associated with more light drinking simultaneous use days and fewer heavy drinking simultaneous use days via coping motives [ref. 69], highlighting the importance of distinguishing between use motives, trait-level emotional vulnerability vs. state-dependent use patterns, and potential behavioral differences across substance use contexts (i.e., self-report vs. laboratory). It is notable that both substituters and complementers demonstrated significantly lower levels of depression than non-substituters in the present analysis. While lower negative emotionality among complementers compared to non-substituters may reflect drinking motives aimed at enhancing positive mood during simultaneous use events [ref. 54], we are hesitant to draw conclusions about this finding give the small (n = 7) subset of participants in the complementers group.
Prior studies have found associations between trait impulsivity and quantity of alcohol consumed on co-use days [ref. 11, ref. 66], though our study was the first to investigate the association between trait impulsivity and substitution in the laboratory. We did not observe significant group differences in positive urgency and lack of perseverance, which have been shown to predict alcohol consumption on cannabis use days (i.e., substitution) among veterans [ref. 66]. Instead, we found that substituters had lower lack of premeditation and a trend towards lower negative urgency. Consistent with our findings, negative urgency has previously been shown to moderate the association between grams of cannabis used and number of drinks consumed in a given day for young adults, with higher negative urgency corresponding to greater quantities of cannabis and alcohol use [ref. 11]. However, Rothstein and Stamates, [ref. 43] found that lack of premeditation was associated with lower co-use frequency in college students [ref. 43]. There is also evidence to suggest planned simultaneous use is associated with greater alcohol consumption and intoxication [ref. 13, ref. 53], emphasizing a need for further research on the role of premeditation in co-use behavior in naturalistic settings.
Within the ANA incentive salience domain, no significant group differences emerged, potentially reflecting homogeneity introduced by study inclusion criteria related to alcohol and cannabis use characteristics (i.e., participants were not recruited on the basis of being a clinical sample and had relatively low levels of craving and dependence symptoms for both alcohol and cannabis) [ref. 41]. Thus, incentive salience may be less relevant than other ANA domains for this specific population. Overall, findings support the ANA’s emphasis on negative emotionality and executive function as core domains in addiction phenotyping, underscoring the importance of individual differences when considering cannabis as a potential substitute for alcohol. In addition, our study extends prior work by applying the ANA framework in a non-clinical sample of individuals engaged in alcohol and cannabis co-use in the laboratory and provides further support for the potential utility of the ANA in non-clinical samples [ref. 36].
Limitations and future directions
Demographic diversity within our sample was limited, and we did not explicitly recruit a clinical sample for this study. However, many of these individuals are likely to meet criteria for AUD and CUD based on their scores on baseline screening measures. Replication in a clinical sample with greater diversity is necessary to extend the generalizability of findings. We were also limited in our ability to draw conclusions regarding the complementer group due to the small sample size. Due to federal restrictions, participants consumed commercial flower cannabis products ad libitum during the cannabis and alcohol co-administration session, thus we lacked experimental control over cannabis dosage, strain, and mode of administration. Future studies should employ stricter dosing controls and could also explore co-administration of alcohol alongside other forms of legal-market cannabis, such as cannabis concentrates [ref. 24]. We also only employed one order of co-administration (cannabis before alcohol), limiting our ability to investigate order effects. Participants were also asked to abstain from cannabis use prior to session AO and therefore may have self-administered more alcohol due to cannabis withdrawal. Additionally, while we used behavior during a single simultaneous use event in the laboratory to categorize participants, engagement in substitutive vs. complementary use of cannabis and alcohol may vary within person at the momentary level [ref. 19], which should be further examined using ecological momentary assessment (EMA) or other experience sampling methods in combination with laboratory assessments. Such a design would allow for the assessment of contextual factors and consequences associated with substitution and co-use. Future research may also benefit from assessing state-level affect (e.g., depression, anxiety) prior to drug administration and including a measure of co-use expectancies at baseline [ref. 3]. Finally, we acknowledge that our participants were only offered $1 per drink not consumed, which is slightly lower than the amount offered in recent bar-lab studies (e.g., $2 per drink) [ref. 45, ref. 46]. This could have promoted greater alcohol consumption during the sessions. However, given that the same $1 incentive was used at both lab sessions, this does not meaningfully impact our interpretation of substitution effects in the present study.
Conclusions
The present findings offer preliminary evidence that individual differences in negative emotionality and impulsivity may meaningfully shape alcohol and cannabis co-use behavior. Notably, substitution of cannabis for alcohol in the laboratory was associated with lower levels of negative emotionality and impulsivity. These results, while preliminary, underscore the potential utility of the ANA framework to identify individuals who may be more or less likely to acutely reduce their alcohol intake while using cannabis, with possible implications for tailoring interventions or harm-reduction strategies for people who co-use alcohol and cannabis. However, given that we did not link the present findings to real-world alcohol or cannabis related consequences, additional longitudinal research is needed to establish whether these results extend to real-world use patterns and consequences over time, and to determine whether substitution may be a reasonable harm-reduction strategy for some individuals who wish to reduce their alcohol use.
Supplementary Materials
References
- EA Abdelhamid, HA-H Hammad, OMI Morsy. The interplay of cognitive distortions, impulsive sensation seeking, and relapse probability among clients with substance use disorders. Tanta Sci Nurs J, 2024. [DOI]
- ZW Adams, AJ Kaiser, DR Lynam, RJ Charnigo, R Milich. Drinking motives as mediators of the impulsivity-substance use relation: pathways for negative urgency, lack of premeditation, and sensation seeking. Addict Behav, 2012. [DOI | PubMed]
- SS Barnwell, M Earleywine. Simultaneous alcohol and cannabis expectancies predict simultaneous use. Subst Abuse Treat Prev Policy, 2006. [DOI | PubMed]
- 4.Beck AT, Epstein N, Brown G, Steer R. Beck anxiety inventory. 1988. 10.1037/t02025-000
- 5.Beck AT, Steer RA, Brown G. Beck Depression Inventory–II. 1996. 10.1037/t00742-000
- J Bjureberg, B Ljótsson, MT Tull, E Hedman, H Sahlin, L-G Lundh, J Bjärehed, D DiLillo, T Messman-Moore, CH Gumpert, KL Gratz. Development and validation of a brief version of the difficulties in emotion regulation scale: the DERS-16. J Psychopathol Behav Assess, 2016. [DOI | PubMed]
- HK Boyle, RL Gunn, G López, OS Fox, JE Merrill. Qualitative examination of simultaneous alcohol and cannabis use reasons, evaluations, and patterns among heavy drinking young adults. Psychol Addict Behav, 2021. [DOI | PubMed]
- AJ Bravo, MA Prince, A Pilatti, L Mezquita, MT Keough, L Hogarth. Young adult concurrent use and simultaneous use of alcohol and marijuana: a cross-national examination among college students in seven countries. Addict Behav Rep, 2021. [DOI | PubMed]
- 9.Conner BT, Smith E, DiCecco S, Sturgess K, Karoly HC, Dooley G, Akagi N, Villanueva C, Hennesy M. Pharmacokinetic differences between fast-acting, standard, and placebo cannabis edibles. (under review).
- MA Cyders, AK Littlefield, S Coffey, KA Karyadi. Examination of a short version of the UPPS-P impulsive behavior scale. Addict Behav, 2014. [DOI | PubMed]
- AR Daros, BJ Pereira, D Khan, AC Ruocco, LC Quilty, JD Wardell. Daily associations between cannabis use and alcohol use in young adults: the moderating role of self-report and behavioral measures of impulsivity. Addict Res Theory, 2022. [DOI]
- 12.Dooley G, Godbole S, Wrobel J, Henthorn TK, Brooks-Russell A, Limbacher S, Kosnett M. Comparison of ∆9-Tetrahydrocannabinol in venous and capillary blood following ad libitum cannabis smoking by occasional and daily users (under review).
- AM Fairlie, S Graupensperger, JC Duckworth, ME Patrick, CM Lee. Unplanned versus planned simultaneous alcohol and marijuana use in relation to substance use and consequences: results from a longitudinal daily study. Psychol Addict Behav, 2021. [DOI | PubMed]
- BA Flannery, AJ Roberts, N Cooney, RM Swift, RF Anton, DJ Rohsenow. The role of craving in alcohol use, dependence, and treatment. Alcohol Clin Exp Res, 2001. [DOI | PubMed]
- CB Fleming, JC Duckworth, IC Rhew, DA Abdallah, K Guttmannova, ME Patrick, CM Lee. Young adult simultaneous alcohol and marijuana use: between- and within-person associations with negative alcohol-related consequences, mental health, and general health across two-years. Addict Behav, 2021. [DOI | PubMed]
- PD Gonçalves, NS Levy, LE Segura, E Bruzelius, AE Boustead, DS Hasin, PM Mauro, SS Martins. Cannabis recreational legalization and prevalence of simultaneous cannabis and alcohol use in the United States. J Gen Intern Med, 2023. [DOI | PubMed]
- KL Gratz, L Roemer. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess, 2004. [DOI]
- T Gunawan, JW Luk, ML Schwandt, LE Kwako, T Vinson, Y Horneffer, DT George, GF Koob, VA Ramchandani, N Diazgranados, D Goldman. Factors underlying the neurofunctional domains of the addictions neuroclinical assessment assessed by a standardized neurocognitive battery. Transl Psychiatry, 2024. [DOI | PubMed]
- RL Gunn, ER Aston, J Metrik. Patterns of cannabis and alcohol co-use: substitution versus complementary effects. Alcohol Res Curr Rev, 2022. [DOI]
- -MAM Hamdan, KF Mahmoud, SAN Al, DH Arabiat. Impulsivity and sensation-seeking personality traits as predictors of substance use among university students. J Psychosoc Nurs Ment Health Serv, 2018. [DOI | PubMed]
- N Heather, JS Tebbutt, RP Mattick, R Zamir. Development of a scale for measuring impaired control over alcohol consumption: a preliminary report. J Stud Alcohol, 1993. [DOI | PubMed]
- SJ Heishman, K Arasteh, ML Stitzer. Comparative effects of alcohol and marijuana on mood, memory, and performance. Pharmacol Biochem Behav, 1997. [DOI | PubMed]
- TK Henthorn, GS Wang, G Dooley, A Brooks-Russell, J Wrobel, S Limbacher, M Kosnett. Dose estimation utility in a population pharmacokinetic analysis of inhaled Δ9-tetrahydrocannabinol cannabis market products in occasional and daily users. Ther Drug Monit, 2024. [DOI | PubMed]
- HC Karoly, MA Prince, NN Emery, EE Smith, CJ Piercey, BT Conner. Protocol for a mobile laboratory study of co-administration of cannabis concentrates with a standard alcohol dose in humans. PLoS One, 2022. [DOI | PubMed]
- GF Koob, ND Volkow. Neurocircuitry of addiction.. Neuropsychopharmacology, 2010. [DOI | PubMed]
- LE Kwako, R Momenan, EN Grodin, RZ Litten, GF Koob, D Goldman. Addictions neuroclinical assessment: a reverse translational approach. Neuropharmacology, 2017. [DOI | PubMed]
- LE Kwako, R Momenan, RZ Litten, GF Koob, D Goldman. Addictions neuroclinical assessment: a neuroscience-based framework for addictive disorders. Biol Psychiatry, 2016. [DOI | PubMed]
- A Looby, MA Prince, MC Villarosa-Hurlocker, BT Conner, TS Schepis, AJ Bravo. Young adult use, dual use, and simultaneous use of alcohol and marijuana: an examination of differences across use status on marijuana use context, rates, and consequences. Psychol Addict Behav, 2021. [DOI | PubMed]
- PF Lovibond, SH Lovibond. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther, 1995. [DOI | PubMed]
- HR Lucke, CR Harbke, EW Mathes, JJ Hammersley. Higher emotion dysregulation and coping motives in alcoholand marijuana users. Substance Use & Misuse, 2021. [DOI | PubMed]
- EM Marceau, PJ Kelly, N Solowij. The relationship between executive functions and emotion regulation in females attending therapeutic community treatment for substance use disorder. Drug Alcohol Depend, 2018. [DOI | PubMed]
- R Martin-Willett, T Helmuth, M Abraha, AD Bryan, L Hitchcock, K Lee, LC Bidwell. Validation of a multisubstance online timeline followback assessment. Brain Behav, 2020. [DOI | PubMed]
- KN McCarty, AK Stevens, RL Gunn, B Borsari, J Metrik. Prospective associations between anxiety sensitivity, distress intolerance, depressive symptoms, and indices of alcohol and cannabis use among veterans. J Stud Alcohol Drugs, 2023. [DOI | PubMed]
- 34.Metrik J, Aston ER, Gunn RL, Swift R, MacKillop J, Kahler CW. Acute effects of cannabis on alcohol craving and consumption: a randomized controlled crossover trial. Am J Psychiatry. 2025;0. 10.1176/appi.ajp.20250115. appi.ajp.20250115.
- KR Moskal, JB Teeters, DC McCollum. Examining differences in emotion dysregulation between emerging adult alcohol-only users, abstainers, and simultaneous users. Cannabis, 2023. [DOI | PubMed]
- SJ Nieto, EN Grodin, R Green, LA Ray. Evaluation of the addictions neuroclinical assessment (ANA) framework through deep phenotyping of problem drinkers. Drug Alcohol Depend, 2021. [DOI | PubMed]
- SJ Nieto, EN Grodin, LA Ray. Neural correlates of the addictions neuroclinical assessment (ANA) incentive salience factor among individuals with alcohol use disorder. Behav Brain Res, 2024. [DOI | PubMed]
- 38.NSDUH. 2023 NSDUH Detailed Tables | CBHSQ Data. 2023. https://www.samhsa.gov/data/report/2023-nsduh-detailed-tables
- ME Patrick, DD Kloska, YM Terry-McElrath, CM Lee, PM O’Malley, LD Johnston. Patterns of simultaneous and concurrent alcohol and marijuana use among adolescents. Am J Drug Alcohol Abuse, 2018. [DOI | PubMed]
- JH Patton, MS Stanford, ES Barratt. Factor structure of the barratt impulsiveness scale. J Clin Psychol, 1995. [DOI | PubMed]
- CL Pince, VT Stallsmith, CJ Piercey, K Weldon, J Ruehrmund, G Dooley, LC Bidwell, HC Karoly. Cannabis administration is associated with reduced alcohol consumption: evidence from a novel laboratory co-administration paradigm.. Drug Alcohol Depend, 2025. [DOI | PubMed]
- 42.R Core Team. R: A language and environment for statistical computing [computer software]. R Foundation for Statistical Computing. 2025. https://www.R-project.org/
- MC Rothstein, AL Stamates. Impulsivity facets, social norms, and co-use of alcohol and cannabis. J Drug Issues, 2025. [DOI | PubMed]
- JB Saunders, OG Aasland, TF Babor, JR de la Fuente, M Grant. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption–II. Addiction, 1993. [DOI | PubMed]
- JP Schacht, KE Voronin, PK Randall, RF Anton. Dopaminergic genetic variation influences aripiprazole effects on alcohol self-administration and the neural response to alcohol cues in a randomized trial. Neuropsychopharmacology, 2018. [DOI | PubMed]
- JP Schacht, Y Im, M Hoffman, KE Voronin, SW Book, RF Anton. Effects of pharmacological and genetic regulation of COMT activity in alcohol use disorder: a randomized, placebo-controlled trial of tolcapone. Neuropsychopharmacology, 2022. [DOI | PubMed]
- AW Sokolovsky, RL Gunn, L Micalizzi, HR White, KM Jackson. Alcohol and marijuana co-use: consequences, subjective intoxication, and the operationalization of simultaneous use. Drug Alcohol Depend, 2020. [DOI | PubMed]
- M SPINELLA. Normative data and a short form of the Barratt Impulsiveness Scale. Int J Neurosci, 2007. [DOI | PubMed]
- AL Stamates, AN Linden-Carmichael, SE Miller, SW Feldstein Ewing. Impulsivity typologies and simultaneous alcohol and cannabis use. Exp Clin Psychopharmacol, 2023. [DOI | PubMed]
- ER Stein, VR Votaw, JE Swan, K Witkiewitz. Validity and measurement invariance of the addictions neuroclinical assessment incentive salience domain among treatment-seekers with alcohol use disorder. J Subst Abuse Treat, 2021. [DOI | PubMed]
- J Stellern, KB Xiao, E Grennell, M Sanches, JL Gowin, ME Sloan. Emotion regulation in substance use disorders: a systematic review and meta-analysis. Addiction, 2023. [DOI | PubMed]
- RS Stephens, RA Roffman, L Curtin. Comparison of extended versus brief treatments for marijuana use. J Consult Clin Psychol, 2000. [DOI | PubMed]
- AK Stevens, RL Gunn, HK Boyle, HR White, KM Jackson. Unplanned versus planned simultaneous alcohol and cannabis use in the daily lives of a predominantly white college student sample: what are the motives, contexts, and outcomes?. Psychol Addict Behav, 2022. [DOI | PubMed]
- BL Stevenson, RD Dvorak, MP Kramer, RS Peterson, ME Dunn, AV Leary, D Pinto. Within- and between-person associations from mood to alcohol consequences: the mediating role of enhancement and coping drinking motives. J Abnorm Psychol, 2019. [DOI | PubMed]
- MS Subbaraman, WC Kerr. Simultaneous versus concurrent use of alcohol and cannabis in the National Alcohol Survey. Alcohol Clin Exp Res, 2015. [DOI | PubMed]
- K Thompson, M Holley, C Sturgess, B Leadbeater. Co-use of alcohol and cannabis: longitudinal associations with mental health outcomes in young adulthood. Int J Environ Res Public Health, 2021. [DOI | PubMed]
- RL Tomko, KE Bountress, KM Gray. Personalizing substance use treatment based on pre-treatment impulsivity and sensation seeking: a review. Drug Alcohol Depend, 2016. [DOI | PubMed]
- JS Tucker, R Seelam, HD Green, A Rodriguez, MS Pollard. Alcohol and cannabis co-use in a national sample of U.S. adults ages 30–80. Addict Behav, 2023. [DOI | PubMed]
- JD VanderVeen, MH Plawecki, JB Millward, J Hays, DA Kareken, S O’Connor, MA Cyders. Negative urgency, mood induction, and alcohol seeking behaviors. Drug Alcohol Depend, 2016. [DOI | PubMed]
- JL Vieira, SG Coelho, LA Snaychuk, N Tabri, SJ Dawson, DC Hodgins, MT Keough, NW Shead, HS Kim. Mental health and dispositional predictors of simultaneous versus concurrent cannabis and alcohol use in a Canadian context. Cannabis, 2024. [DOI | PubMed]
- VR Votaw, MR Pearson, E Stein, K Witkiewitz. The addictions neuroclinical assessment negative emotionality domain among treatment-seekers with alcohol use disorder: construct validity and measurement invariance. Alcohol Clin Exp Res, 2020. [DOI | PubMed]
- JT Waddell. Between- and within-group effects of alcohol and cannabis co-use on AUD/CUD in the NSDUH 2002–2019. Drug Alcohol Depend, 2021. [DOI | PubMed]
- JT Waddell. Hierarchical and mediated relations between internalizing symptoms, alcohol and cannabis co-use, and AUD. Addict Res Theory, 2022. [DOI]
- JT Waddell, AJ Blake, L Chassin. Relations between impulsive personality traits, alcohol and cannabis co-use, and negative alcohol consequences: a test of cognitive and behavioral mediators. Drug Alcohol Depend, 2021. [DOI | PubMed]
- JT Waddell, WR Corbin, KJ Grimm, J Metrik, CM Lee, TJ Trull. Within-episode relations among simultaneous alcohol and cannabis use and continued drinking: the role of momentary subjective responses, craving, and drinking context. Alcohol Clin Exp Res, 2024. [DOI]
- JT Waddell, RL Gunn, WR Corbin, B Borsari, J Metrik. Drinking less on cannabis use days: the moderating role of UPPS-P impulsive personality traits. Psychol Addict Behav, 2021. [DOI | PubMed]
- JT Waddell, LK Howe. Relations among adolescent alcohol and cannabis co-use, adolescent impulsive traits, and prospective change in impulsive traits into emerging adulthood. Cannabis, 2023. [PubMed]
- JT Waddell, J Jager, L Chassin. Maturing out of alcohol and cannabis co-use: a test of patterns and personality predictors. Alcohol Clin Exp Res, 2022. [DOI | PubMed]
- JD Wardell, KN Farrelly, A Moore, N Fox, SG Coelho, JA Cunningham, RM O’Connor, CS Hendershot. Internalizing symptoms are indirectly associated with simultaneous alcohol and cannabis use through specific motives for simultaneous use: a longitudinal study of young adults. Alcohol Clin Exp Res, 2025. [DOI]
- SP Whiteside, DR Lynam, JD Miller, SK Reynolds. Validation of the UPPS impulsive behaviour scale: a four-factor model of impulsivity. Eur J Pers, 2005. [DOI]
- CE Wilcox, JM Pommy, B Adinoff. Neural circuitry of impaired emotion regulation in substance use disorders. Am J Psychiatry, 2016. [DOI | PubMed]
- AM Wycoff, TJ Trull. Affective reinforcement of simultaneous versus single use of alcohol and cannabis. Drug Alcohol Depend, 2025. [DOI | PubMed]
- M Zuckerman, DM Kuhlman, J Joireman, P Teta, M Kraft. A comparison of three structural models for personality: the big three, the big five, and the alternative five. J Personal Soc Psychol, 1993. [DOI]