
Recreational substance use and aneurysmal subarachnoid hemorrhage: differential effects of alcohol and THC
Abstract
Supplementary Information:
The online version contains supplementary material available at 10.1007/s10143-026-04295-w.
Article type: Research Article
Keywords: Intracranial aneurysm, Aneurysmal subarachnoid hemorrhage, Alcohol, THC, Recreational drugs
Affiliations: https://ror.org/04mz5ra38grid.5718.b0000 0001 2187 5445Department of Neurosurgery and Spine Surgery, University Hospital Essen, University of Duisburg-Essen, Essen, Germany; https://ror.org/04mz5ra38grid.5718.b0000 0001 2187 5445Center for Translational Neuro- & Behavioral Sciences (C-TNBS), University of Duisburg, Essen, Germany; https://ror.org/04mz5ra38grid.5718.b0000 0001 2187 5445Department of Diagnostic and Interventional Radiology and Neuroradiology, University Hospital Essen, University of Duisburg-Essen, Essen, Germany
License: © The Author(s) 2026 CC BY 4.0 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Article links: DOI: 10.1007/s10143-026-04295-w | PubMed: 42020885 | PMC: PMC13102730
Relevance: Core topic: mentioned in title and keywords
Full text: PDF (929 KB)
Introduction
The use of recreational drugs is widespread, with alcohol and tobacco being legal in most countries [ref. 1, ref. 2]. In recent years, tetrahydrocannabinol (THC) has also been legalized in several nations [ref. 3]. It is widely known that the use of these substances can have harmful effects on general health. Regarding aneurysmal subarachnoid hemorrhage (aSAH), tobacco use has been established as one of the most significant risk factors for both the formation and rupture of intracranial aneurysms (IA) [ref. 4–ref. 6]. Additionally, the consumption of certain illicit drugs, such as cocaine and amphetamines, has been strongly linked to an increased risk of occurrence, rupture, and severity of rupture in IA [ref. 7–ref. 9].
Despite the wealth of research on tobacco and illicit drugs, the impact of alcohol on intracranial aneurysms remains underexplored. Recent studies investigating the relationship between alcohol consumption and the risk of rupture or severity of aSAH are limited. Previous studies oppose relevant deficits in qualities as reported in meta-analysis [ref. 10, ref. 11]. However, an excessive alcohol consumption has been identified as a key risk factor [ref. 10, ref. 12]. Meanwhile, the effect of THC use on these outcomes is even less understood [ref. 9, ref. 13–ref. 16], as there is a notable lack of relevant studies in this area.
Given the growing prevalence of recreational THC use and the potential for alcohol to influence vascular health, there is a pressing need for further research. Understanding the role of alcohol and THC in the context of IA rupture could have significant implications for public health and clinical practice. This study aims to address this gap in knowledge by investigating the effects of alcohol and THC use on the risk and severity of IA rupture in cases of aSAH.
Methods
All patients aged 18 years or older who were treated for an IA (ruptured or unruptured) between July 2016 and October 2023 at a single tertiary hospital in Germany were eligible for this study. The study received approval from the Institutional Review Board (Ethik-Kommission, Medizinische Fakultät der Universität Duisburg-Essen; Approval No. 15-6331-BO) and was registered with the German Clinical Trials Register (DRKS; ID DRKS00008749; Registration date: 06/09/2015). Patients were prospectively included in this study. After obtaining written consent from the patient or their next of kin, all clinical and radiographic data assessed during each visit were stored in the institutional ARCTICA (Assessment of Risk Clusters in Treatment of Individuals with Cerebral Aneurysms) database. Additional clinical information was collected via a paper-based interview with the patient or their next of kin at first presentation. Furthermore, a telephone-based interview was conducted at the 6-month follow-up to fill in any missing information and reconfirm the initial documentation. All patients and relatives were informed about the confidentiality of the obtained information.
Patients presenting with clinical signs of aSAH underwent cranial computed tomography (CT) to confirm aneurysm rupture. Patients suspected for aSAH with a normal CT scan received a lumbar puncture to rule out or confirm aSAH. The clinical status of aSAH patients was assessed using the World Federation of Neurosurgical Societies (WFNS) scale [ref. 17]. WFNS grades 4 and 5 were classified as poor-grade aSAH. The radiographic severity was assessed using the modified Fisher (mFisher) scale [ref. 18]. mFisher grades 3 and 4 were defined as radiographic severe aSAH.
All patients underwent additional digital subtraction angiography (DSA) to confirm the presence of the IAs. In cases with signs of herniation requiring immediate surgical treatment upon admission, CT angiography (CTA) was performed as stand alone. IA size and morphology were determined using DSA, or CTA when DSA was not available. IAs with multiple lobes or daughter aneurysms were classified as irregular. The location of the IA was further stratified into anterior and posterior circulation. Patients with more than one IA were classified as multiple IA (MIA) bearers.
Information on alcohol use, premorbid conditions, drug use, and positive family history of IA was collected during the interview. A positive family history was defined as at least one first-degree relative with an IA. Premorbid conditions including hypertension were assed as part of the structured interview, documented diagnosis from primary care physicans and regular medication intake before first presentation. use was categorized into THC use and polytoxicomania to identify patients with heavy use of illicit drugs. Polytoxicomania was defined as the use of two or more recreational drugs other than alcohol. Alcohol use was further stratified at a consumption of over 20 g per day in male and over 10 g per day in female patients, classified as risky alcohol use. We used the mean consumption over the last 12 month.
Statistical analysis was performed using SPSS Version 25 for Windows. Univariate analysis was conducted to assess correlations between different alcohol and drug use and the radiographic characteristics of the IA, as well as the presence of ruptured IA in the whole IA cohort and clinical severity of aSAH among cases with ruptured IA. Dichotomous variables were evaluated using Chi-square tests or Fisher’s exact test for sample sizes less than five. The significance level was set at p < 0.05. Finally, a multivariate analysis was performed for significant correlations identified in the univariate analysis to assess the independent association of recreational drugs with the occurrence and clinical severity of aSAH. Adjustments were made for the common risk factors age, smoking, IA sac size, sex, arterial hypertension, and family history of IA. Missing data for covariants in the multivariant analyses were replaced using multiple implications.
Chat GPT 5 (Open AI, 2025) was used solely for help with text style/grammar corrections and figure design. The scientific content, statistical data analysis, and interpretation of the results were entirely performed and verified by the authors without the use.
Results
The final cohort consisted of 954 patients with IA. Eight patients were excluded due to missing data on alcohol or drug consumption. The majority of patients were female (674; 70.6%). Over two-thirds of the cohort (641; 67.2%) reported consuming alcohol to some extent, while 4.6% (44 patients) reported risky levels of alcohol consumption. THC use was reported by 51 patients (5.3%), and polytoxicomania was documented in 31 patients (3.2%). A total of 394 patients (41.3%) presented with a ruptured IA. A comprehensive list of baseline characteristics is provided in Supplemental Table 1.
Sex and age differences in substance use in the whole IA cohort
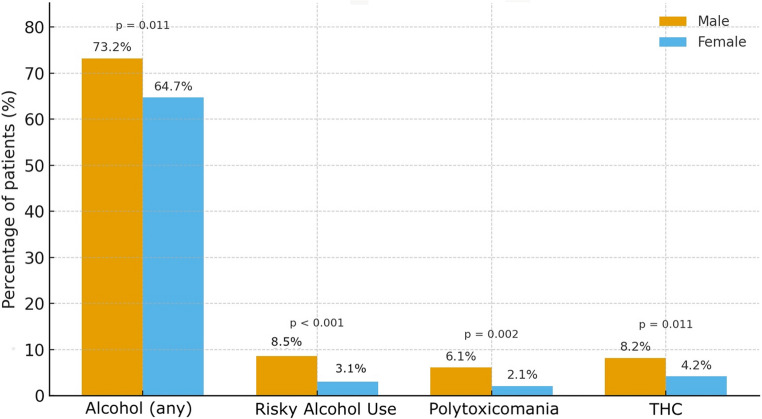
For all categories of recreational drug use, consumption rates were significantly lower among female patients. Specifically, women were significantly less likely to consume any alcohol (p = 0.011; odds ratio [OR] 0.67; 95% confidence interval [CI] 0.49–0.91), engage in risky alcohol consumption (p < 0.001; OR 0.33; 95% CI 0.18–0.60), use THC (p = 0.011; OR 0.27; 95% CI not specified), or report polytoxicomania (p = 0.002; OR 0.33; 95% CI 0.16–0.68) compared to their male counterparts (Fig. 1).
Additionally, patients who used THC, consumed any alcohol or reported polytoxicomania use were significantly younger than those who did not. This age difference was not observed for risky alcohol consumption (Table 1).
Table 1: Mean age distribution between drug users and alcohol consumers
| Parameter | Yes | No | p | ||
|---|---|---|---|---|---|
| Mean age (years) | ±SD (years) | Mean age (years) | ±SD (years) | ||
| Alcohol any | 56 | 12 | 58 | 14 | 0.029 |
| Risky Alcohol Use | 54 | 11 | 57 | 13 | 0.256 |
| THC | 43 | 10 | 57 | 12 | < 0.001 |
| Polytoxicomania | 42 | 10 | 57 | 13 | < 0.001 |
Impact of alcohol, THC, and polytoxicomania on IA rupture
Patients who reported risky alcohol consumption had a significantly increased risk of presenting with a ruptured IA in univariate analysis (p = 0.014; OR 2.13; 95% CI 1.15–3.94). This association remained significant after adjusting for common risk factors in multivariate analysis (p = 0.031; adjusted OR [aOR] 2.00; 95% CI 1.07–3.75; Table 2).
Table 2: Multivariant analysis of risk of IA rupture, significant parameters are marked bold
| Parameter | p | aOR | 95%CI |
|---|---|---|---|
| Sex female | 0.047 | 1.34 | 1.01–1.80 |
| Age > 70 years | 0.031 | 1.55 | 1.04–2.32 |
| Smoking | 0.613 | 0.92 | 0.66–1.28 |
| Art.hypertension | 0.053 | 0.76 | 0.58–1.01 |
| Familial IA | 0.951 | 1.01 | 0.69–1.50 |
| IA sack>7 mm | < 0.001 | 1.68 | 1.28–2.21 |
| Risky Alcohol Use | 0.031 | 2.00 | 1.07–3.75 |
No significant association with IA rupture was observed for general alcohol consumption (p = 0.751), THC use (p = 0.756), or polytoxicomania (p = 0.236) in univariate analysis.
Impact of substance use on severity of aSAH
Risky alcohol consumption was associated with a significantly increased risk of presenting with clinically severe aSAH (p = 0.011; OR 2.95; 95% CI 1.24–6.90), but not with radiographically severe aSAH (p = 0.856; OR 0.93; 95% CI 0.40–2.14). In multivariate analysis, risky alcohol consumption remained an independently associated with clinically severe aSAH (p = 0.009; aOR 3.26; 95% CI 1.34–7.95; Table 3).
Table 3: Multivariant analysis of risk of presentation with a clinical severe aSAH (WFNS 4/5) in case of IA rupture, significant parameters are marked bold
| Parameter | p | aOR | 95%CI |
|---|---|---|---|
| Sex female | 0.534 | 0.87 | 0.55–1.37 |
| Age > 70 years | 0.079 | 1.71 | 0.94–3.12 |
| Smoking | 0.437 | 0.81 | 0.48–1.38 |
| Art.hypertension | 0.012 | 1.73 | 1.13–2.67 |
| Familial IA | 0.119 | 0.59 | 0.31–1.15 |
| IA sack>7 mm | 0.028 | 1.60 | 1.05–2.45 |
| Risky Alcohol Use | 0.009 | 3.26 | 1.34–7.95 |
There was no significant association between any alcohol consumption, THC use, or polytoxicomania and either clinical or radiographic severity of aSAH (Table 4).
Table 4: Univariate analysis of risk of presentation with a clinical severe (WFNS 4/5) or radiographic severe (mFisher 3/4) aSAH in case of IA rupture
| Parameter | WFNS 4/5 | ||||
|---|---|---|---|---|---|
| yes | no | p | OR | 95%CI | |
| Alcohol any | 44.6% | 46.5% | 0.725 | 0.93 | 0.61–1.42 |
| Polytoxicomania | 50.0% | 45.0% | 0.692 | 1.22 | 0.45–3.33 |
| THC | 40.0% | 45.5% | 0.633 | 0.80 | 0.32-2.00 |
| mFisher 3/4 | |||||
| yes | no | p | OR | 95%CI | |
| Alcohol any | 67.4% | 71.7% | 0.396 | 0.82 | 0.52–1.30 |
| Polytoxicomania | 68.8% | 68.8% | > 0.99 | 0.99 | 0.34–2.93 |
| THC | 60.0% | 69.3% | 0.384 | 0.67 | 0.27–1.67 |
Impact of substance use on aneurysm characteristics
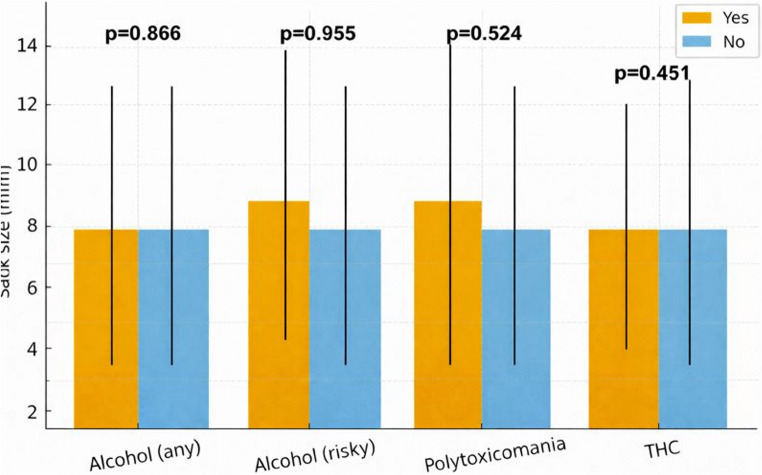
No significant differences could be shown regarding the size of the IA and the different drug uses (Fig. 2). Regarding the MIA patients with polytoxicomania showed the highest in group incidence with 48.4% and lowest rate of posterior circulation IA (6.5%). However, this difference showed no significant difference (p = 0.131 and p = 0.118, respectively). Furthermore, no subgroup showed a significant increased rate of irregular IA (Supplemental Table 2).
Discussion
The aim of this study was to elucidate the influence of recreational drug use on the occurrence and severity of aSAH. We utilized our prospective IA database and included 954 patients over a six-year span. Alcohol consumption to any extent was relatively common, affecting about two thirds of the cohort. Risky alcohol consumption and THC use affected only a much smaller group of patients. Our data show a connection between risky alcohol consumption and IA rupture, as well as the clinical severity of aSAH. There were no corresponding results for patients consuming THC.
Alcohol is known as a substance with a multitude of harmful effects and is the origin of a relevant social burden. In addition to vascular diseases, it plays a role in multiple other chronic and malignant diseases [ref. 19, ref. 20]. Previous studies have shown that current alcohol consumption and the amount of alcohol consumed increase the risk of aSAH, which is in line with our own results [ref. 10–ref. 12, ref. 21–ref. 23]. Furthermore, three meta-analyses, mainly based on smaller and earlier studies with certain methodological limitations, drew a similar conclusion: they connected excessive alcohol consumption with IA rupture [ref. 10–ref. 12]. Other authors linked alcohol consumption to rupture and outcome, but only as part of a panel of factors contributing to an unhealthy lifestyle [ref. 24]. Additionally, genetically determined alcohol consumption has so far failed to predict IA rupture [ref. 23]. Our analysis also showed that risky alcohol consumption leads to clinically but not radiographic more severe aSAH. One possible explanation is that the systemic effects of alcohol—such as transient or chronic hypertension, impaired platelet function, and alcohol-related coagulopathy—may worsen early neurological status at presentation without necessarily increasing the initial hemorrhage volume. These mechanisms could contribute to a more severe clinical presentation independent of radiographic bleeding extent. Finally, patients with high levels of alcohol consumption often exhibit increased overall frailty and a poorer general health status. exact effect of alcohol on the risk of IA rupture is not fully understood. One possible mechanism may be that regular alcohol consumption increases the risk of hypertension [ref. 25]. However, in our study the negative effect of alcohol persisted even after adjusting for hypertension. Alcohol has been shown to cause oxidative stress [ref. 26] and leads to mitochondrial damage [ref. 27]. In turn, oxidative stress has been linked to IA formation and rupture [ref. 28]. Notably, it has been shown that in case of cessation of alcohol consumption the likelihood of IA rupture no longer increased, emphasizing the potential positive effects of alcohol cessation [ref. 21]. Acknowledging that alcohol consumption seems to play a crucial role only above certain levels, as demonstrated in our and other studies [ref. 10, ref. 11, ref. 21], it can be hypothesized that reducing consumption below a specific threshold might also have beneficial effects.
Results on the influence of THC on IA and aSAH are contradictory so far. There are three analyses of national cohort patient data regarding the use of THC in connection with IA. One reported no effect on outcome after aSAH but cited possible underreporting of usage [ref. 29]. Others reported a higher rate of perioperative complications in THC users with aSAH and a higher likelihood of aSAH occurrence [ref. 30], [ref. 14]. On the other hand, a retrospective single-institution analysis from 2022 found no association between THC consumption and aSAH occurrence [ref. 31]. Finally, a smaller study from 2006 found evidence of a negative effect of THC consumption on outcome after aSAH but failed to prove an independent association [ref. 13]. THC use has been associated with oxidative stress as well as with ischemic stroke in young adults. Both of these facts suggest possible negative effects on patients with IA [ref. 32, ref. 33]. Our study failed to support these suggestions. One possible reason may be that the group of drug users in our cohort was relatively small and the heterogeneity regarding the amount and mode of consumption inside these groups was higher among THC users and patients with polytoxicomania than in the alcohol subgroup. Like in previous studies, we did not specify the method of THC consumption. As there are many different ways to consume THC, a possible effect of the route of administration remains unclear.
While multiple studies have connected the use of illicit drugs with the risk of aSAH [ref. 8, ref. 9, ref. 34–ref. 37], our study failed to draw a similar conclusion for patients consuming a mixture of such substances. The reasons for this appear to be multifactorial: one is the small sample size in our cohort, most likely due to underreporting and the fact that individuals with drug addiction tend not to undergo regular medical check-ups. Another theoretical explanation could be that patients with severe drug addiction may die from aSAH before reaching the hospital, which would also contribute to underreporting of such cases. We additionally failed, also most likely due to the small sample size, to connect drug use with different aneurysm characteristics.
Limitations
This study faces several limitations. First, the study is single-center and not population-based. The number of THC users in this cohort is relatively small which limits the statistical power. One factor may be that the data were collected before THC use was legalized for recreational purposes in Germany (April 2024). Furthermore, it relies on self- or relative-reported drug and alcohol consumption which might be an additional reason for underreporting. Nevertheless, the relatively large sample size and the prospective data collection contribute to the robustness of this study.
Conclusion
This prospective single-center study adds evidence to the growing body of literature supporting the negative effect of alcohol consumption on the risk of IA rupture, while also independently linking it to more severe clinical presentation in cases of aSAH. However, given the observational design, causality cannot be established. While no negative effect of THC use could be demonstrated in this study, this may be due to underreporting of polysubstance use. Alcohol consumption in patients with IA should be carefully evaluated and addressed in patient counseling regarding lifestyle modification after diagnosis. As an increasing number of countries move toward legalization of THC, further large-scale, multicenter studies with more detailed substance-use assessment will be necessary to better clarify the potential impact of THC and other psychoactive substances on IA progression and aSAH outcomes.
Supplementary Materials
References
- T Sun, A Anandan, CCW Lim, K East, SS Xu, ACK Quah, BN Rutherford, B Johnson, Y Qi, D Stjepanovic, J Leung, JP Connor, C Gartner, WD Hall, G Vu, GCK Chan. Global prevalence of heated tobacco product use, 2015-22: A systematic review and meta-analysis. Addiction, 2023. [DOI | PubMed]
- 2.World Health Organization (2024) Global status report on alcohol and health and treatment of substance use disorders
- M Isorna, F Pascual, E Aso, F Arias. Impact of the legalisation of recreational cannabis use. Adicciones, 2023. [DOI | PubMed]
- RM Starke, JW Thompson, MS Ali, CL Pascale, A Martinez Lege, D Ding, N Chalouhi, DM Hasan, P Jabbour, GK Owens, M Toborek, JM Hare, AS Dumont. Cigarette smoke initiates oxidative stress-induced cellular phenotypic modulation leading to cerebral aneurysm pathogenesis. Arterioscler Thromb Vasc Biol, 2018. [DOI | PubMed]
- H Wang, L Wang, J Wang, L Zhang, C Li. The Biological Effects of Smoking on the Formation and Rupture of Intracranial Aneurysms: A Systematic Review and Meta-Analysis. Front Neurol, 2022. [DOI | PubMed]
- MJ Pachón-Londoño, MT Ghoche, BA Nguyen, SF Maroufi, V Olson, DP Patra, EL Turcotte, Z Wang, BS Halpin, C Krishna, A Turkmani, FB Meyer, BR Bendok. Cigarette Smoking and Observed Growth of Unruptured Intracranial Aneurysms: A Systematic Literature Review and Meta-Analysis. Stroke, 2024. [DOI | PubMed]
- AW McEvoy, ND Kitchen, DG Thomas. Intracerebral haemorrhage and drug abuse in young adults. Br J Neurosurg, 2000. [DOI | PubMed]
- 8.Pozzi M, Roccatagliata D, Sterzi R (2008) Drug abuse and intracranial hemorrhage. neurological sciences: official journal of the Italian neurological society and of the Italian society of clinical neurophysiology 29 Suppl. 2S269–270. 10.1007/s10072-008-0960-z
- WA Florez-Perdomo, JS Reyes Bello, E García-Ballestas, LR Moscote-Salazar, EJ Barthélemy, T Janjua, VP Maurya, A Agrawal. Aneurysmal Subarachnoid Hemorrhage and Cocaine Consumption: A Systematic Review and Metanalysis. World Neurosurg, 2024. [DOI | PubMed]
- VL Feigin, GJ Rinkel, CM Lawes, A Algra, DA Bennett, J van Gijn, CS Anderson. Risk factors for subarachnoid hemorrhage: an updated systematic review of epidemiological studies. Stroke, 2005. [DOI | PubMed]
- X Yao, K Zhang, J Bian, G Chen. Alcohol consumption and risk of subarachnoid hemorrhage: A meta-analysis of 14 observational studies. Biomed Rep, 2016. [DOI | PubMed]
- M Ali, MJA van Eldik, S Rietkerken, JW Schoones, ND Kruyt, GJE Rinkel, MJH Wermer, S Peters, YM Ruigrok. Risk Factors of Aneurysmal Subarachnoid Hemorrhage Including Analysis by Sex: A Systematic Review and Meta-Analysis. Neurology, 2025. [DOI | PubMed]
- R Behrouz, L Birnbaum, R Grandhi, J Johnson, V Misra, S Palacio, A Seifi, C Topel, R Garvin, JL Caron. Cannabis Use and Outcomes in Patients With Aneurysmal Subarachnoid Hemorrhage. Stroke, 2016. [DOI | PubMed]
- K Rumalla, AY Reddy, MK Mittal. Association of Recreational Marijuana Use with Aneurysmal Subarachnoid Hemorrhage. J stroke Cerebrovasc diseases: official J Natl Stroke Association, 2016. [DOI]
- E Bouquet, S Pain, C Eiden, E Jouanjus, N Richard, B Fauconneau, MC Pérault-Pochat. Adverse events of recreational cannabis use reported to the French addictovigilance network (2012–2017). Br J Clin Pharmacol, 2021. [DOI | PubMed]
- PMR Lai, I Ng, WB Gormley, N Patel, KU Frerichs, MA Aziz-Sultan, R Du. Cannabis Use and Increased Nonaneurysmal Subarachnoid Hemorrhage in the Past Decade. World Neurosurg, 2021. [DOI | PubMed]
- GM Teasdale, CG Drake, W Hunt, N Kassell, K Sano, B Pertuiset, JC De Villiers. A universal subarachnoid hemorrhage scale: report of a committee of the World Federation of Neurosurgical Societies. J Neurol Neurosurg Psychiatry, 1988. [DOI | PubMed]
- JA Frontera, J Claassen, JM Schmidt, KE Wartenberg, R Temes, ES Connolly, RL MacDonald, SA Mayer. Prediction of symptomatic vasospasm after subarachnoid hemorrhage: the modified fisher scale. Neurosurgery, 2006. [DOI | PubMed]
- PF Bau, CH Bau, GA Rosito, WC Manfroi, FD Fuchs. Alcohol consumption, cardiovascular health, and endothelial function markers. Alcohol, 2007. [DOI | PubMed]
- N Bouajila, C Domenighetti, HJ Aubin, M Naassila. Alcohol consumption and its association with cancer, cardiovascular, liver and brain diseases: a systematic review of Mendelian randomization studies. Front Epidemiol, 2024. [DOI | PubMed]
- A Can, VM Castro, YH Ozdemir, S Dagen, D Dligach, S Finan, S Yu, V Gainer, NA Shadick, G Savova, S Murphy, T Cai, ST Weiss, R Du. Alcohol Consumption and Aneurysmal Subarachnoid Hemorrhage. Translational stroke Res, 2018. [DOI]
- T Sankai, H Iso, T Shimamoto, A Kitamura, Y Naito, S Sato, T Okamura, H Imano, M Iida, Y Komachi. Prospective study on alcohol intake and risk of subarachnoid hemorrhage among Japanese men and women. Alcohol Clin Exp Res, 2000. [DOI | PubMed]
- H Lin, Y Yin, J Li, S Liu, X Long, Z Liao. Exploring the causal links between cigarette smoking, alcohol consumption, and aneurysmal subarachnoid hemorrhage: a two-sample Mendelian randomization analysis. Front Nutr, 2024. [DOI | PubMed]
- 24.Swiatek VM, Fischer I, Khajuria R, Amini A, Steinkusch H, Rashidi A, Stein KP, Dumitru CA, Sandalcioglu IE, Neyazi B (2024) The MARVIN hypothesis: Linking unhealthy lifestyles to intracranial aneurysm rupture risk and clinical prognosis. Med (Kaunas) 60(11). 10.3390/medicina60111813
- GS Stokes. Hypertension and alcohol: is ther a link?. J Chronic Dis, 1982. [DOI | PubMed]
- J Haorah, SH Ramirez, N Floreani, S Gorantla, B Morsey, Y Persidsky. Mechanism of alcohol-induced oxidative stress and neuronal injury. Free Radic Biol Med, 2008. [DOI | PubMed]
- VD Reddy, P Padmavathi, G Kavitha, B Saradamma, N Varadacharyulu. Alcohol-induced oxidative/nitrosative stress alters brain mitochondrial membrane properties. Mol Cell Biochem, 2013. [DOI | PubMed]
- RM Starke, N Chalouhi, MS Ali, PM Jabbour, SI Tjoumakaris, LF Gonzalez, RH Rosenwasser, WJ Koch, AS Dumont. The role of oxidative stress in cerebral aneurysm formation and rupture. Curr Neurovasc Res, 2013. [DOI | PubMed]
- C Dandurand, JXC Ke, RA Mekary, S Prakash, G Redekop, P Gooderham, CS Haw. Cannabis use and outcomes after aneurysmal subarachnoid hemorrhage: A nationwide retrospective cohort study. J Clin neuroscience: official J Neurosurgical Soc Australasia, 2020. [DOI]
- RG Chiu, AM Fuentes, SN Patil, R Chiu, LS McGuire, AI Mehta. Cannabis Abuse and Perioperative Complications After Treatment of Intracranial Aneurysms: A Nationwide Analysis. World Neurosurg, 2022. [DOI | PubMed]
- F Akbik, HD Konan, KP Williams, LM Ermias, Y Shi, O Takieddin, JA Grossberg, BM Howard, F Tong, CM Cawley, Y Mei, OB Samuels, O Sadan. Cannabis Use Is Not Associated With Aneurysmal Subarachnoid Hemorrhage Complications or Outcomes. Stroke, 2022. [DOI | PubMed]
- V Wolff, AI Schlagowski, O Rouyer, AL Charles, F Singh, C Auger, V Schini-Kerth, C Marescaux, JS Raul, J Zoll, B Geny. Tetrahydrocannabinol induces brain mitochondrial respiratory chain dysfunction and increases oxidative stress: a potential mechanism involved in cannabis-related stroke. Biomed Res Int, 2015. [DOI | PubMed]
- V Wolff, V Lauer, O Rouyer, F Sellal, N Meyer, JS Raul, C Sabourdy, F Boujan, C Jahn, R Beaujeux, C Marescaux. Cannabis use, ischemic stroke, and multifocal intracranial vasoconstriction: a prospective study in 48 consecutive young patients. Stroke, 2011. [DOI | PubMed]
- JA Gledhill, DF Moore, D Bell, JA Henry. Subarachnoid haemorrhage associated with MDMA abuse. J Neurol Neurosurg Psychiatry, 1993. [DOI | PubMed]
- JE Conway, RJ Tamargo. Cocaine use is an independent risk factor for cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Stroke, 2001. [DOI | PubMed]
- K Moon, FC Albuquerque, M Mitkov, AF Ducruet, DA Wilson, RW Crowley, P Nakaji, CG McDougall. Methamphetamine use is an independent predictor of poor outcome after aneurysmal subarachnoid hemorrhage. J neurointerventional Surg, 2015. [DOI]
- A Can, VM Castro, YH Ozdemir, S Dagen, D Dligach, S Finan, S Yu, V Gainer, NA Shadick, G Savova, S Murphy, T Cai, ST Weiss, R Du. Heroin Use Is Associated with Ruptured Saccular Aneurysms. Translational stroke Res, 2018. [DOI]