Rate and predictors of 30-day readmission for clostridiodes difficile: a United States analysis
Abstract
Background:
Clostridiodes difficile is a leading cause of healthcare-associated diarrhea. In this study, we aimed to identify the rates and predictors for 30-day readmissions of Clostridiodes difficile Enterocolitis (CDE) in the United States.
Methods:
We conducted a retrospective study of the Nationwide Readmissions Database to identify adult hospitalizations with a principal diagnosis of CDE for 2018. Individuals <18 years old and elective hospitalizations were excluded. Primary outcomes included readmission rate and the top ten principal diagnosis on readmission, while the secondary outcomes were inpatient mortality, hospital costs and independent predictors of 30-day all-cause readmissions. Furthermore, we devised a scoring system to estimate the risk of CDE readmissions. Stata® Version 16 was used for statistical analysis and p-values ≤0.05 were statistically significant.
Results:
We identified 94,668 index hospitalizations and 18,296 readmissions at 30-days for CDE in 2018. The 30-day all-cause readmission rate was 25.7%. On readmission, CDE was the most common principal diagnosis (25.7%), followed by unspecified sepsis, and acute renal failure. A female predominance was also noted for index and 30-day readmissions of CDE. Compared to index admissions, we noted higher odds of inpatient mortality [4.4 vs 1.4%, Odds Ratio (OR):3.32, 95% Confidence Interval (CI):2.87–3.84, p < 0.001], longer mean length of stay (LOS) [6.4 vs 5.6 days, Mean Difference (MD):0.9, 95% CI:0.7–1.0, p < 0.001), and higher mean total hospital charge (THC) [$56,015 vs $40,871, MD:15,144, 95% CI:13,260–17,027, p < 0.001] for 30-day readmissions of CDE. Independent predictors for 30-day all-cause readmissions of CDE included discharged against medical advice (AMA) [Adjusd Hazard Ratio (aHR):2.01, 95% CI:1.73–2.53, p < 0.001], diabetes mellitus (DM) [aHR:1.22, 95% CI:1.16–1.29, p < 0.001], and chronic kidney disease (CKD) [aHR:1.29, 95% CI:1.21–1.37, p < 0.001].
Conclusion:
The all-cause 30-day readmission rate and inpatient mortality for CDE was 25.7% and 4.4%, respectively. Discharge AMA, DM and CKD were independent predictors for 30-day all-cause readmissions of CDE.
Article type: Research Article
Keywords: readmission, epidemiology predictors, mortality costs
Affiliations: Department of Internal Medicine, Central Michigan University College of Medicine, Saginaw, MI, USA; Department of Internal Medicine, Samaritan Medical Center, Watertown, NY, USA; Division of Gastroenterology and Hepatology, Department of Internal Medicine, Indiana University School of Medicine, Indianapolis, IN, USA; Department of Nephrology, Guthrie Robert Packer Hospital, Sayre, PA, USA; Department of Medicine and Endocrinology, Our Lady of Lourdes Memorial Hospital, Binghamton, NY, USA; Department of Internal Medicine, John H. Stronger Jr. Hospital of Cook County, Chicago, IL, USA
License: © 2022 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group CC BY 4.0 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article links: DOI: 10.1080/07853890.2021.2023211 | PubMed: 34989297 | PMC: PMC8741240
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (1.5 MB)
Introduction
Clostridiodes difficile is a gram-positive, spore-forming, anaerobic bacillus that can lead to diarrhea and/or enterocolitis of varying severity [ref. 1]. It is closely associated with antibiotic use and has been identified as the leading cause of healthcare-associated diarrhea in the United States (US) with literature reporting a 200% increase in C. difficile related hospitalizations between 2000 and 2009 [ref. 2–4]. Furthermore, studies continue to report rising rates of incidence, severity, and mortality associated with C. difficile [ref. 4]. From a hospitalization perspective, it has been estimated that over 200,000 individuals require hospitalization for C. difficle-associated diarrhea every year accounting for 1% of all US hospitalizations [ref. 5,ref. 6]. Hence, it is well established that CDE places a significant burden on the US healthcare system in terms of costs (over $4 billion at acute care facilities) and resource utilization [ref. 2,ref. 7]. Additionally, CDE is also a major health risk to individual patients, particularly those admitted to the hospital, and may affect the patients’ overall quality of life [ref. 8].
Readmission of CDE have been thoroughly investigated; however, there continue to be significant gaps in current literature. Prior studies have focussed their attention on the characteristics and associations of readmissions, but do not provide additional information on key hospitalization characteristics and predictors of readmissions. Identification of these variables may help reduce readmissions rates, inpatient mortality, and the burden of CDE on the US healthcare system [ref. 5,ref. 9]. Hence, we designed this retrospective study to determine hospitalization characteristics and adverse outcomes of 30-day readmissions of CDE, and compare them to index admissions to identify key differences. Furthermore, we also developed a scoring system to estimate the risk of CDE readmissions.
Materials and methods
Design and data source
We conducted a retrospective study from the Nationwide Readmissions Database (NRD) to identify adult hospitalizations with a principal diagnosis of CDE. The NRD is the largest, publicly available, multi-ethnic, all-payer inpatient healthcare readmission database in the US, drawn from the Agency for Healthcare Research and Quality (AHRQ) Healthcare Cost and Utilization Project (HCUP) State Inpatient Databases (SID). It is an annual file constructed using one calendar year of discharge data. The discharges included in the study were treated at hospitals across the US (excluding rehabilitation or long-term acute care hospitals) and had patient linkage numbers that were verified and used to identify the study population. Discharge weights were calculated using post-stratification for hospital characteristics (census region, urban/rural location, teaching status, bed size, and hospital control) and patient characteristics (sex and five age groups [0, 1–17, 18–44, 45–64, and 65 and older]) [ref. 10]. For the 2018 calendar year, the NRD had discharge data from 28 geographically dispersed states accounting for 59.7% of the total US resident population and 58.7% of all US hospitalizations [ref. 10]. The database is validated by HCUP and designed to support readmission analyses on a national scale as the weighted analysis allows us to obtain 100% of the US hospitalizations within a given year [ref. 10]. In the NRD, up to 40 discharge diagnoses and 25 procedures are collected for each patient using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD10-CM/PCS) for each calendar year. The diagnoses are classified as the principal diagnosis, which is the primary reason for hospitalization, and secondary diagnosis, which includes any other discharge diagnosis.
Study population
The study involved all adult (≥18 years) hospitalizations with a primary diagnosis of CDE using the ICD-10 diagnostic codes (A04.7X). The CDE types in this diagnostic code included patients with recurrent CDE (A04.71) and CDE without mention of recurrence (A04.72). Individuals <18 years of age and elective hospitalizations were excluded. Furthermore, we excluded hospitalizations in December due to the lack of an adjoining 30-day period to assess 30-day readmissions. Using the unique hospitalization identifiers available within the NRD, we identified index hospitalizations, and one subsequent hospitalization within 30 days tagged as readmission for CDE.
Outcome measures
The primary outcomes included the rates of 30-day readmissions and the top ten principal diagnosis on readmission for 30-day readmission of CDE. Moreover, the secondary outcomes were inpatient mortality, mean length of stay (LOS), hospital costs [mean total healthcare cost (THC) and mean cost of hospitalization (COH)], and independent predictors for 30-day all-cause readmissions of CDE. Furthermore, we also developed a readmission risk scoring system based on these independent predictors to estimate the risk of CDE readmissions.
Statistical analysis
The data was analysed using Stata® Version 16 software (StataCorp, Texas, USA). We conducted all the analysis using the weighted samples for national estimates in adjunct with HCUP regulations for using the NRD. Age grouped as 18–39 years represented young adults, 40–64 years represented middle-aged adults, and ≥65 years represented the elderly.
The comorbidity burden was assessed using the Sundararajan’s adaptation of the modified Deyo’s Charlson comorbidity index (CCI) [ref. 11]. The CCI contains a list of comorbidities with an assigned weighted score based on the relative risk of 1-year mortality. Consequently, the sum of the index score is an indicator of disease burden and an excellent estimator of mortality. The modified Deyo’s CCI is classified into four groups with increasing risk for mortality and has been adapted in population-based research [ref. 11]. A score of >3 has about a 25% 10-year mortality, while a score of 2 or 1 has a 10% and 4% 10-year mortality, respectively. This cut-off point was chosen as a means of assessment of the increased risk of mortality [ref. 11,ref. 12].
For the comparative analysis, we used the Pearson’s chi-square test to compare the characteristics between the index hospitalization and readmissions. A univariable logistic regression was employed to compare readmission mortality, and linear regression model was used to compare readmission, LOS, THC, and COH to the index hospitalization. Furthermore, we employed a univariable pre-screening analysis to identify variables associated with readmission and potential predictors of 30-day all-cause readmission. Additionally, we identified mean age, sex, hospital location, hospital teaching status, hospital bed size, mean household income, and the comorbidities for CDE readmissions. Variables with p-value less than 0.2 were included in the final multivariable regression analysis. Subsequently, we performed a multivariable Cox regression analysis to identify independent predictors of readmissions with p-values <0.05 set as the threshold for statistical significance. This model included CDE type (CDE with or without mention of recurrence), sex, discharg against medical advice (AMA), insurance status, hospital teaching status, hospital location, Hypertension, Chronic Obstructive Pulmonary Disease (COPD), Diabetes Mellitus (DM), Chronic Kidney Disease (CKD), Protein-Energy Malnutrition (PEM), and history of neoplasm.
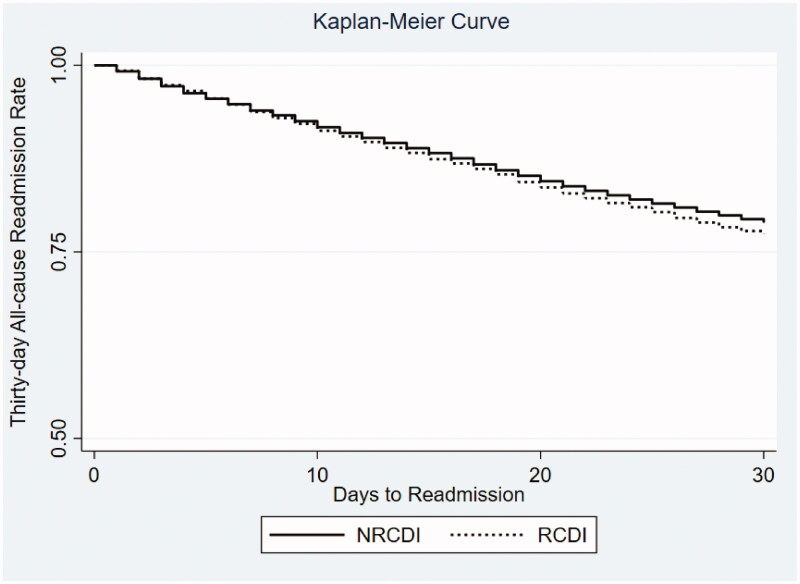
Furthermore, we selected independent predictors which have >10% increased hazard ratio for 30-day readmission to develop a risk scoring system following index CDE hospitalizations. Variables such as DM, COPD, CKD, PEM, and AMA were included. A score of 1 was assigned to these five variables and the incidence rate for readmission for aggregate scores were obtained. Finally, a Kaplan-Meier curve (Figure 1) was generated based on the findings of our study.
Ethical considerations
This was a database study using the NRD. As NRD lacks specific patient identifiers, our study was exempt from Institutional Review Board (IRB) approval as per guidelines put forth by our institutional IRB for analysis of HCUP databases.
Results
Rate and top ten principal diagnosis for 30-Day readmissions of CDE
For 2018, there were 94,668 index hospitalizations and 18,296 readmissions at 30-days for CDE. The 30-day all-cause readmission rate was noted to be 25.7%. On readmission, CDE was identified as the most common principal diagnosis (25.7%), followed by unspecified sepsis (11.1%), acute renal failure (2.9%), urinary tract infections (unspecified site) [1.7%], and dehydration (0.9%) (Tables 1 and 2).
Table 1.: Top principal diagnoses based on International Classification of Diseases (ICD)-10 diagnostic chapters for 30-day readmissions of Clostridiodes difficile Enterocolitis in the United States.
| Principal Readmission Diagnosis Based on ICD-10 Diagnostic Chapters | Proportion (%) |
|---|---|
| Certain Infectious and Parasitic Diseases | 41.7 |
| Diseases of the Digestive System | 14.4 |
| Diseases of the Circulatory system | 11.2 |
| Diseases of the Genitourinary System | 6.5 |
| Endocrine, Nutritional and Metabolic Diseases | 5.7 |
| Diseases of the Respiratory system | 5.6 |
| Neoplasms | 2.1 |
| Mental, Behavioural and Neurodevelopmental Disorders | 2.0 |
| Diseases of the Nervous System | 1.8 |
| Diseases of the Musculoskeletal System and Connective Tissue Diseases | 1.4 |
| Diseases of the Skin and Subcutaneous Tissue | 1.3 |
| Diseases of Blood and Blood-Forming Organs | 1.1 |
ICD: International Classification of Diseases
Table 2.: Top ten principal diagnoses for 30-day readmissions of Clostridiodes difficile Enterocolitis in the United States.
| Principal readmission diagnosis | Proportion (%) |
|---|---|
| Clostridium Difficile Enterocolitis | 25.7 |
| Unspecified Sepsis | 11.1 |
| Acute Renal Failure | 2.9 |
| Hypertensive Heart and Chronic Kidney Disease with Heart Failure | 2.3 |
| Urinary Tract Infection (site not specified) | 1.7 |
| Pneumonia (unspecified organism) | 1.4 |
| Hypertensive Heart Disease with Heart Failure | 1.3 |
| Sepsis secondary to Anaerobes | 1.1 |
| Noninfective Gastroenteritis and Colitis (unspecified) | 1.1 |
| Dehydration | 0.9 |
Comparative analysis of hospitalization characteristics for index admission and 30-Day readmissions of CDE
Compared to index admissions, 30-day readmissions of CDE had a lower proportion of females (61.8 vs. 64.1%, p < 0.001) without a statistically significant difference in mean age. Thirty-day readmissions of CDE had a higher proportion of patients with CCI score ≥3 (50.5 vs. 38.1%, p < 0.001) compared to index admissions. Furthermore, there were a higher portion of patients with comorbidities such as DM, congestive heart failure (CHF), CKD and COPD in the 30-day readmission cohort compared to index admissions.
Comparative analysis of clinical outcomes for index admissions and 30-Day readmissions of CDE
From a mortality perspective, 30-day readmissions of CDE were associated with significantly higher odds of inpatient mortality (4.4 vs 1.4%, OR:3.32, 95% CI:2.87–3.84, p < 0.001) compared to index admissions. Additionally, these readmissions also had longer mean LOS, and higher THC and COH (Table 3).
Table 3.: Comparative analysis of clinical outcomes for index admissions and 30-day readmissions of Clostridiodes difficile enterocolitis in the United States.
| Outcome | Index admission | 30-day readmission | Odds ratio (95% ci) | p-value |
|---|---|---|---|---|
| In-patient Mortality (%) | 1.4 | 4.4 | 3.32 (2.87–3.84) | <.001 |
| Mean Length of Stay (days) | 5.6 | 6.4 | 0.9# (0.7–1.0) | <.001 |
| Mean Total Hospital Charges (USD) | 40,871 | 56,015 | 15,144# (13260–17027) | <.001 |
| Mean Total Hospital Cost (USD) | 10,064 | 13,504 | 3,439# (1486–2101) | <.001 |
#Mean difference, CI: confidence interval.
Predictors for 30-day all-cause readmissions of CDE
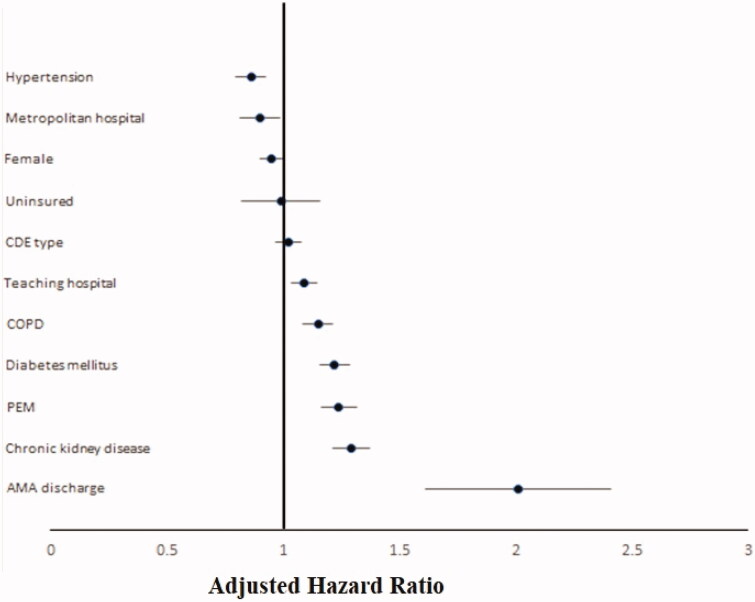
Independent predictors for 30-day all-cause readmissions of CDE included discharge AMA (aHR:2.01, 95% CI:1.73–2.53, p < 0.001), DM (aHR:1.22, 95% CI:1.16–1.29, p < 0.001), and CKD (aHR:1.29, 95% CI:1.21–1.37, p < 0.001) [Table 4 and Figure 2].
Table 4.: Hospitalization characteristics for index admissions and 30-day readmissions of Clostridiodes difficile Enterocolitis in the United States.
| Variable | Index admission (%) | Thirty-day readmission (%) | p-value |
|---|---|---|---|
| Total Number of Hospitalizations | 94,668 | 18,296 | |
| Patient characteristics | |||
| Age (mean years) ± SE | 66.4 ± 0.3 | 66.4 ±.4 | .907 |
| Women (%) | 64.1 | 61.8 | <.001 |
| Charlson Comorbidity Index Score (%) | <.001 | ||
| 0 | 25.3 | 15.6 | |
| 1 | 19.7 | 16.9 | |
| 2 | 16.9 | 17.0 | |
| ≥3 | 38.1 | 50.5 | |
| Insurance Type (%) | <.001 | ||
| Medicare | 69.2 | 71.6 | |
| Medicaid | 10.3 | 11.9 | |
| Private | 18.2 | 14.4 | |
| Uninsured | 2.3 | 2.1 | |
| Median Annual Income in Patient’s Zip Code* (USD) | .114 | ||
| 1–45,999 | 27.6 | 28.7 | |
| 46,000–58,999 | 29.7 | 29.6 | |
| 59,000–78,999 | 25.0 | 24.6 | |
| ≥79,000 | 17.7 | 17.1 | |
| Comorbidities | |||
| Hypertension | 37.5 | 31.6 | <.001 |
| Diabetes Mellitus | 30.0 | 33.3 | <.001 |
| Smoking History | 14.3 | 13.5 | .046 |
| Congestive Heart Failure | 18.1 | 22.7 | <.001 |
| Chronic Kidney Disease | 27.1 | 31.4 | <.001 |
| Obesity | 12.9 | 12.9 | .961 |
| Dyslipidemia | 38.9 | 38.9 | .952 |
| Coronary Artery Disease | 23.7 | 27.5 | <.001 |
| Prior Cerebrovascular Accident | 2.8 | 3.4 | .003 |
| Protein-Energy Malnutrition | 14.8 | 20.0 | <.001 |
| Chronic Obstructive Pulmonary Disease | 17.6 | 21.3 | <.001 |
| History of Neoplasm | 14.4 | 17.7 | <.001 |
| Hospital characteristics | |||
| Hospital Bed Size | <.001 | ||
| Small | 19.3 | 17.7 | |
| Medium | 27.5 | 25.9 | |
| Large | 53.2 | 56.4 | |
| Metropolitan Location | 76.2 | 77.5 | .010 |
| Teaching Status | 65.3 | 68.6 | <.001 |
Kichloo’s score for 30-Day readmission following CDE hospitalization
Five independent predictors of 30-day readmission of CDE, namely DM, COPD, CKD, PEM, and discharge AMA, were used to develop the Kichloo’s scoring system. CDE hospitalizations with a score of 0 had a 17.9% rate of readmission, while hospitalizations with a score of ≥3 had a readmission rate of 36.8% (Table 5). The score was structured into average risk (0), and high risk (≥1) for 30-day readmission.
Table 5.: Risk assessment model for 30-day readmissions of Clostridiodes difficile Enterocolitis in the United States using the Kichloo Scoring System.
| Kichloo Score | Incidence Rate Per Day Per 1,000 Hospitalizations | 30-Day Readmission Incidence Rate (%) | Index Admission (%) | Readmission (%) |
|---|---|---|---|---|
| 0 | 6 | 17.9 | 40.9 | 32.5 |
| 1 | 9 | 25.8 | 33.9 | 37.6 |
| 2 | 11 | 32.4 | 19.9 | 23.5 |
| ≥3 | 13 | 36.8 | 5.3 | 5.4 |
Kichloo Score [readmission risk following Clostridiodes difficile enterocolitis (CDE) hospitalizations]: One point each for Diabtes Mellitus, Chronic Obstructive Pulmonary Disease, Chronic Kidney Disease, Protein Energy Malnutrition, and Discharge Against Medical Advice.
Discussion
Readmission rate and top ten principal diagnosis for 30-Day readmissions of CDE
The 30-day all-cause readmission rate for CDE was noted to be 25.7%. This high readmission rate may be due to the fact that patients with a history of C. difficile infections tend to have a higher degree of relapse and therefore readmission. We also noted that at the time of readmission, CDE was the most common principal diagnosis. This finding aligns with current literature which reports that patients with recurrent C. difficile infections are more likely to be readmitted and have longer lengths of hospitalizations compared to patients without a recurrent CDE infection [ref. 9,ref. 13]. Furthermore, other top common principal diagnosis on readmission included unspecified sepsis, and acute renal failure. The relationship between sepsis and CDE is relatively well studied with literature reporting increased risk of severe sepsis in patients with CDE [ref. 14–16]. Moreover, acute renal failure, which was also noted in our study, may be a consequence of volume depletion secondary to watery diarrhea and may increase the odds of subsequent readmissions [ref. 17].
Hospitalization characteristics of index admissions and 30-Day readmissions of CDE
We noted that 30-day readmissions of CDE had a higher proportion of patients with comorbidities such as DM, CHF, CKD, and COPD compared to the index admissions. The association between several of these comorbidities with CDE has already been established in literature. For example, patients with CDE may have prolonged periods of continued watery diarrhea leading to volume depletion and progression of pre-renal acute kidney injury to acute tubular necrosis and ultimately CKD [ref. 17]. Additionally, these patients with underlying CKD may be at a higher risk of developing acute on chronic kidney failure due to significant dehydration secondary to diarrhea. CDE has also been linked to acute renal failure due to the action of toxin B on the collecting duct leading to increased loss of volume and subsequent death [ref. 18]. Additionally, C. difficile infection has also been linked to the development of immunoglobulin A (IgA) nephropathy in patients with a prior diagnosis of acute and chronic renal failure [ref. 18]. Hence, through multiple mechanisms, CDE may lead to readmission in patients with pre-existing renal disease. Furthermore, per guidelines, for patients with inflammatory bowel disease, renal failure, DM, and haematologic malignancies, who present to the hospital for acute-onset diarrhea, screening studies for C. difficile are recommended as they are prominent risk factor for index or recurrent infection [ref. 19,ref. 20].
Thirty-day readmissions of CDE also had a higher proportion of patients with CCI score ≥3 compared to index admissions reflecting a higher comorbidity burden in these patients. Hence, we advocate for the need of increased surveillance for C. difficile in patients with multiple comorbidities as they may be at higher-than-average risk of acquiring CDE and subsequent readmissions after CDE.
Comparison of clinical outcomes for index admission and 30-Day readmissions, and predictors of 30-day readmissions of CDE
Compared to index admissions, 30-day readmissions of CDE were associated with significantly higher odds of inpatient mortality (Table 3). These readmissions were also associated with increased mean LOS, and higher THC and COH (Table 3). These findings reflected current literature as CDE is associated with increased LOS, THC, and risk of readmissions [ref. 5]. Higher hospital costs and longer length of hospital stay may, in part, be due to the need of subspeciality care and a higher prevalence of comorbidities in these patients which may require an interdisciplinary team and additional resources for management [ref. 21]. Moreover, readmissions within 60 days of an initial C. difficile infection with a secondary diagnosis of recurrent C. difficile has also been shown to have poor clinical outcomes and high healthcare costs, highlighting the healthcare burden that the infection poses [ref. 22].
In this study, independent predictors for 30-day all-cause readmissions of CDE included discharge AMA, DM, PEM, COPD and CKD. In an attempt to identify individuals at the highest risk of readmissions and thereby inpatient mortality, we developed a scoring system (Kichloo’s Score) for CDE readmissions. We used these independent risk factors for our scoring system and one point each was given for DM, COPD, CKD, PEM, and AMA. We then calculated the risk of readmissions for these patients based on the assigned scores. We noted that patients with a score of 0 had a readmission rate of 17.9%, while patients with a score of ≥3 had a readmission rate of 36.8% (Table 5). We believe that this scoring system may help physicians identify and closely monitor individuals with the highest risk of readmission on index admission, thereby reducing the overall readmission rates, healthcare utilization and inpatient mortality.
Strengths and limitations
This study has several strengths and limitations. The study population, which is derived from one of the large, multi-ethnic hospital-based databases in the US, is believed to be a key strength of this study. Though our unique analysis, we examine numerous outcome-oriented facets for index admissions and 30-day readmissions of CDE. However, as with any study, this study is not exempt for limitations. The data available from the NRD is subject to biases associated with retrospective studies such as selection bias (all hospitalized patients) and the innate ability to discern patterns in seemingly random sets of data, as recognition of a pattern prior to analysis [ref. 23]. Hence, our study is meant to be a means to encourage future large, prospective, multicenter studies on the disease entity to further investigate our findings. Additionally, the NRD contains hospitalization data rather than data for individual patients. Thus, patients readmitted numerous times would be included more than once in our dataset. Moreover, the NRD lacks data on the time from hospital discharge after index hospitalization to readmission, severity of the disease, hospital course and the treatment aspects of the disease. Furthermore, like other administrative databases, there may be imitations related to reporting due to a lack of a financial incentive to document data. This limitation has been noted specifically with less costly and non-invasive studies, such as computed tomographic scans, ultrasound, and electrocardiography [ref. 23]. Our study does not investigate diagnostic procedures, and the limitations of the use of administrative databases regarding CDE are not clear; however, it is recognized that not all studies are affected by under-coding to the same degree [ref. 24]. The NRD also uses ICD-10 codes to report hospitalizations and thus may be prone to human coding errors. Finally, our study population had more females compared to males; however, previous retrospective studies have reported an equitable distribution of CDE with gender [ref. 25]. This may be due to an intrinsic limitation of this retrospective database. However, despite these limitations, we believe that the demographics studied, large sample size, and a unique analysis technique adds meaningful data on one of the major healthcare burdens in the US responsible for index admissions, readmissions and hospital acquired infections. Through this study, we aim to encourage further conversation and research on CDE readmissions.
Conclusion
CDE places substantial burden on the US healthcare system in terms of costs and resource utilization. Patients admitted to the hospital for CDE, particularly those with multiple comorbidities, are at a higher risk of significant morbidity and mortality. In this study, we identified 94,668 index admissions and 18,296 readmissions at 30-days for CDE. The 30-day all-cause readmission rate for CDE was 25.7% with CDE being the most common principal diagnosis on readmission. Compared to index admissions, we noted higher odds of inpatient mortality (4.4 vs 1.4%, OR:3.32, 95% CI:2.87–3.84, p < 0.001), longer mean LOS (6.4 vs 5.6 days, MD: 0.9, 95% CI:0.7–1.0, p < 0.001), and higher mean THC ($56,015 vs $40,871, MD:15,144, 95% CI:13,260–17,027, p < 0.001) for 30-day readmissions of CDE. Independent predictors for 30-day all-cause readmissions of CDE included being discharge AMA, DM, and CKD. Additional large, prospective, multi-center studies are needed to further confirm these findings.
Author contributions
Asim Kichloo, Zain El-Amir and Dushyant Singh Dahiya are credited with substantial contribution to the design of the work, acquisition, and interpretation of the data, drafting the manuscript, revision of important intellectual content, final approval of the version published, and agreement of accountability for all aspects of the work. Mohammad Al-Haddad, Jagmeet Singh, Gurdeep Singh and Carlos Corpez are credited with substantial contribution to interpretation of data, literature review of all sections discussed, final approval of the version published, and agreement of accountability for all aspects of the work. Hafeez Shaka is credited with analysis of the data, interpretation of the data, literature review of all sections discussed, final approval of the version published, and agreement of accountability for all aspects of the work.
References
- Risk factors for Clostridium difficile infection in hospitalized patients with community-acquired pneumonia.. J Infect., 2016. [PubMed]
- Antibiotics and hospital-acquired Clostridium difficile infection: update of systematic review and meta-analysis.. J Antimicrob Chemother., 2014. [PubMed]
- Current status of clostridium difficile infection epidemiology.. Arch Clin Infect Dis., 2012
- Clostridioides difficile infection.. Ann Intern Med., 2018. [PubMed]
- Impact of Clostridium difficile-associated diarrhea on acute care length of stay, hospital costs, and readmission: a multicenter retrospective study of inpatients, 2009–2011.. Am J Infect Control., 2015. [PubMed]
- Clostridium difficile infection hospitalizations in the United States: insights from the 2017 national inpatient sample.. Gastroenterology Res., 2021. [PubMed]
- Burden of Clostridium difficile infection in the United States.. N Engl J Med., 2015. [PubMed]
- Increase in clostridium difficile-related mortality rates, United States, 1999–2004.. Emerg Infect Dis., 2007. [PubMed]
- Impact of Clostridium difficile recurrence on hospital readmissions.. Am J Infect Control., 2015. [PubMed]
- 10Overview of the Nationwide Readmissions Database (NRD) Rockville, MD: Healthcare Cost and Utilization Project; 2018. Available from: https://www.hcup-us.ahrq.gov/nrdoverview.jsp.
- Cross-national comparative performance of three versions of the ICD-10 charlson index.. Med Care., 2007. [PubMed]
- 12Cost-to-Charge Ratio Files Rockville, MD: Healthcare Cost and Utilization Project; 2020. Available from: https://www.hcup-us.ahrq.gov/db/ccr/costtocharge.jsp.
- Clinical, epidemiological and microbiological characteristics of relapse and re-infection in Clostridium difficile infection.. Anaerobe., 2017. [PubMed]
- Hospitalization type and subsequent severe sepsis.. Am J Respir Crit Care Med., 2015. [PubMed]
- An unusual presentation of severe sepsis due to Clostridium difficile enteritis.. Cureus., 2019. [PubMed]
- Clostridium difficile enteritis: diffuse small bowel radiological changes in a patient with abdominal sepsis.. BMJ Case Reports., 2018
- Clostridium difficile infection: a review of current and emerging therapies.. Ann Gastroenterol., 2016. [PubMed]
- Clostridium difficile causing acute renal failure: case presentation and review.. World J Gastroenterol., 2005. [PubMed]
- Comorbidities, exposure to medications, and the risk of community-acquired clostridium difficile infection: a systematic review and meta-analysis.. Infect Control Hosp Epidemiol., 2015. [PubMed]
- Diabetes mellitus as a risk factor for recurrence of clostridium difficile infection in the acute care hospital setting.. Am J Infect Control., 2011. [PubMed]
- Economic healthcare costs of Clostridium difficile infection: a systematic review.. J Hosp Infect., 2010. [PubMed]
- Hospital readmission with Clostridium difficile infection as a secondary diagnosis is associated with worsened outcomes and greater revenue loss relative to principal diagnosis: a retrospective cohort study.. Medicine., 2018. [PubMed]
- Publication bias, retrospective bias, and reproducibility of significant results in observational studies.. Anesth Analg., 2012. [PubMed]
- Limitations of administrative databases.. JAMA., 2012. [PubMed]
- Accuracy of ICD-9 coding for Clostridium difficile infections: a retrospective cohort study.. Epidemiol Infect., 2007. [PubMed]