
Obstructive Sleep Apneas and Cardiovascular Diseases
Abstract
Obstructive sleep apnea (OSA) is a sleep-disordered breathing condition characterized by recurrent upper-airway obstruction, leading to intermittent hypoxemia, sleep fragmentation, and sympathetic activation. OSA is highly prevalent in patients with cardiovascular diseases and is strongly associated with hypertension, atrial fibrillation, coronary artery disease, heart failure, and adverse prognosis. This review summarizes current evidence on the pathophysiology of OSA, its cardiovascular consequences, and available diagnostic and therapeutic strategies, with particular attention to clinical implications in cardiology practice. We discuss established treatments such as lifestyle interventions, continuous positive airway pressure, mandibular advancement devices, and selected surgical options, as well as emerging therapies, including pharmacological approaches targeting weight loss and ventilatory control. While OSA treatment improves symptoms and quality of life, evidence for cardiovascular event reduction remains heterogeneous and appears strongly influenced by patient selection and treatment adherence. Identifying patients most likely to benefit from targeted OSA management remains a key challenge.
Article type: Review Article
Keywords: obstructive sleep apnea, obesity, heart failure, continuous positive airway pressure
Affiliations: Health Science Interdisciplinary Research Center, Scuola Superiore Sant’Anna, 56127 Pisa, Italy; Cardiology and Cardiovascular Medicine Division, Fondazione Monasterio, 56124 Pisa, Italy; Cardioncology Unit, European Institute of Oncology, IRCCS, 20141 Milan, Italy
License: © 2026 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Article links: DOI: 10.3390/clockssleep8020028 | PubMed: 42200975 | PMC: PMC13214718
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (4.7 MB)
1. Introduction
Obstructive sleep apnea (OSA) is a form of sleep-disordered breathing (SDB) caused by partial or complete upper-airway obstruction during sleep, leading to repeated episodes of reduced (hypopnea) or absent (apnea) inspiratory flow despite persistent respiratory effort [ref. 1].
SDB includes respiratory events such as apneas and hypopneas, typically associated with desaturation and/or arousals during sleep. An apnea is defined as a ≥90% reduction in airflow for ≥10 s [ref. 2]. Hypopnea is variably defined as a ≥30% airflow reduction for ≥10 s, associated with either a ≥3% desaturation or arousal, or a ≥4% desaturation alone [ref. 2]. Both definitions are used in clinical studies, and their relative diagnostic impact remains under investigation [ref. 2].
OSA must be distinguished from central apneas (CAs), which result from impaired respiratory drive rather than upper-airway obstruction. CAs are linked to altered chemoreflex control, circulatory delay, and increased “plant gain”, i.e., ventilatory oversensitivity to CO2 changes [ref. 1,ref. 3,ref. 4]. A typical manifestation is Cheyne–Stokes breathing, with alternating CA and hyperventilation phases [ref. 3]. If these oscillations do not meet CA criteria, the pattern is termed periodic breathing, which can also be detected during exercise testing [ref. 5].
In OSA, airflow cessation occurs despite continued thoracoabdominal effort, whereas in CA both airflow and respiratory effort are absent due to a lack of central respiratory drive [ref. 1]. Both conditions may coexist in the same patient, and mixed apneas typically begin as central events and end with obstructive features [ref. 2].
OSA has major effects on quality of life and on multiple organs, particularly the cardiovascular system [ref. 6]. Typical symptoms include asthenia and excessive daytime sleepiness, leading to reduced attention, cognitive impairment, decreased productivity, and increased risk of work and road accidents [ref. 7]. OSA is associated with a higher incidence of type 2 diabetes, systemic and pulmonary hypertension (PH), coronary artery disease (CAD), atrial fibrillation (AF), stroke, heart failure (HF), and increased mortality [ref. 8].
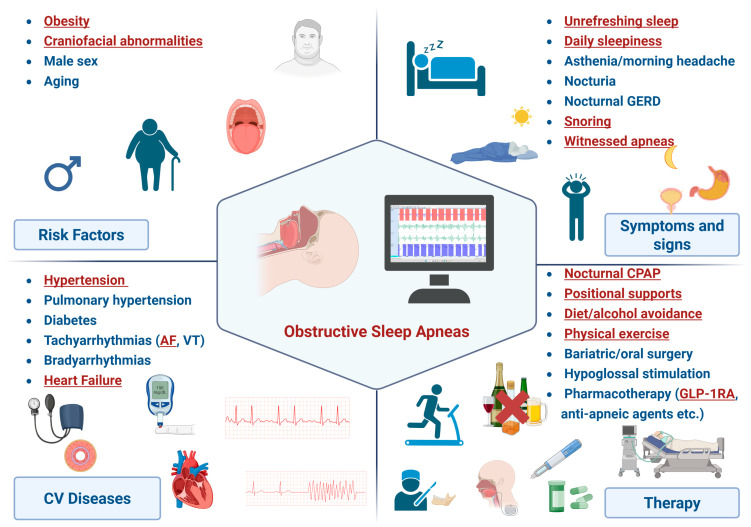
Despite its high prevalence in cardiovascular patients and clear prognostic impact, OSA remains underdiagnosed and undertreated in cardiology. This narrative review summarizes current evidence on OSA, with emphasis on its interaction with cardiovascular disease and therapeutic implications (Figure 1).
2. Staging
OSA severity is primarily assessed through the apnea–hypopnea index (AHI), defined as the number of apneas and hypopneas per hour of sleep [ref. 1]. Home monitoring devices lack electroencephalographic monitoring (EEG) and therefore estimate sleep time; in this setting, AHI is reported as the respiratory event index (REI) [ref. 1,ref. 9]. OSA severity is graded as follows: AHI/REI < 5 (normal), 5–15 (mild), 15–30 (moderate), >30 (severe) [ref. 2]. When polysomnography is available, some centres report the respiratory disturbance index (RDI), which also includes respiratory-effort-related arousals (RERAs), defined as sleep interruptions that do not formally meet the criteria for apnea or hypopnea, but still disturb breathing during sleep and may trigger arousal [ref. 10]. Desaturation-based metrics are also used in addition to event-based indices. The oxygen desaturation index (ODI) counts ≥3% desaturation events per sleep hour [ref. 2], but T < 90% (time spent with SaO2 < 90%) is often more informative [ref. 2,ref. 11].
3. Epidemiology
OSA is the most common sleep-related respiratory disorder, with comparable prevalence across industrialized countries [ref. 8]. In the Wisconsin Sleep Cohort, mild OSA (AHI 5–15) affected 34% of men and 17% of women aged 30–70, while moderate–severe OSA (AHI > 15) occurred in 13% of men and 6% of women [ref. 12]. However, OSA remains largely underdiagnosed, with an estimated 24 million undetected cases in the United States alone [ref. 13]. Between 1990 and 2010, OSA prevalence increased by ~30%, rising by 4% in women and 8% in men [ref. 12]. Prevalence rises with age and is roughly twice as high in men as in women, although it increases in women after menopause [ref. 12]. OSA is strongly correlated with overweight and obesity, with prevalence increasing proportionally to body mass index (BMI) [ref. 12]. Among patients with cardiovascular disease, OSA prevalence reaches ~40%, markedly higher than in the general population [ref. 14].
Cardiovascular Patients at High Risk for OSA
Certain patient subgroups carry a particularly high probability of clinically significant disease and should therefore be prioritized for targeted screening.
Patients with resistant hypertension represent one of the highest-risk groups, as OSA frequently contributes to poor blood pressure control through sympathetic activation and nocturnal fluid redistribution [ref. 15]. Similarly, OSA is highly prevalent in patients with atrial fibrillation, particularly in those with recurrent arrhythmia after cardioversion or catheter ablation [ref. 16]. Patients with heart failure also warrant focused attention, especially those with preserved ejection fraction, obesity-related phenotypes, or persistent congestion, in whom SDB is common and often underrecognized [ref. 17].
Additional high-risk categories include patients with pulmonary hypertension, coronary artery disease with recurrent ischemic events, and prior stroke or transient ischemic attack [ref. 18].
4. Pathophysiology
4.1. Anatomical Mechanisms
Airway patency during sleep depends on the activity of upper-airway dilator muscles (e.g., the genioglossus and soft-palate elevator muscles), which prevent tongue collapse and pharyngeal narrowing [ref. 19]. Patients with OSA often have structurally narrow upper airways due to parapharyngeal fat deposition, fatty infiltration of the pharyngeal muscles, or craniofacial abnormalities. The severity of OSA may vary across individuals and populations because of differences in the prevalence of soft-tissue abnormalities (more common in Western countries) and craniofacial skeletal abnormalities (more common in Eastern countries). The normal reduction in dilator muscle tone during sleep promotes airway collapse in anatomically predisposed individuals [ref. 19].
4.2. Functional Mechanisms
Beyond structural collapse, OSA is influenced by a low arousal threshold, reduced compensatory activation of upper-airway muscles, and unstable ventilatory control (“high loop gain,” i.e., an exaggerated chemoreflex response to changes in blood gases) [ref. 20,ref. 21]. The balance among these traits contributes to distinct OSA phenotypes. High loop gain also contributes to CA, explaining the frequent coexistence of OSA and CA or mixed apneas [ref. 22]. In rare cases, pharyngeal neuropathy or denervation may impair reflex activation of upper-airway dilator muscles [ref. 23]. Hormonal factors such as leptin may modulate dilator muscle tone, possibly explaining why equally obese individuals exhibit different susceptibility to OSA [ref. 24].
4.3. Impact of OSA on Cardiovascular Pathophysiology and Metabolism
Intermittent hypoxia, hypercapnia, and intrathoracic pressure swings during OSA trigger repeated arousals and sleep fragmentation, which are major contributors to daytime sleepiness [ref. 19]. Hypoxia and hypercapnia stimulate peripheral chemoreceptors, while recurrent arousals enhance central sympathetic outflow, resulting in persistent activation of the sympathetic nervous system. This neurohumoral response increases heart rate, peripheral vasoconstriction, and blood pressure (BP), with effects that may extend into wakefulness [ref. 25]. OSA therefore causes nocturnal BP surges and a non-dipping or reverse-dipping profile, which may persist during the daytime because of sustained sympathetic activation [ref. 26]. Indeed, OSA represents one of the main causes of nocturnal and resistant hypertension [ref. 27].
Sympathetic overactivity, together with intermittent hypoxia and reduced intrathoracic pressure, may also activate the renin–angiotensin–aldosterone system (RAAS) through renal vasoconstriction, reduced renal perfusion, and enhanced renin release. Increased angiotensin II and aldosterone levels promote sodium retention, nocturnal rostral fluid shift, vasoconstriction, oxidative stress, and vascular remodelling [ref. 28]. Fluid accumulation within peripharyngeal tissues may narrow the upper-airway lumen and increase tissue pressure, thereby further amplifying upper-airway collapsibility [ref. 29].
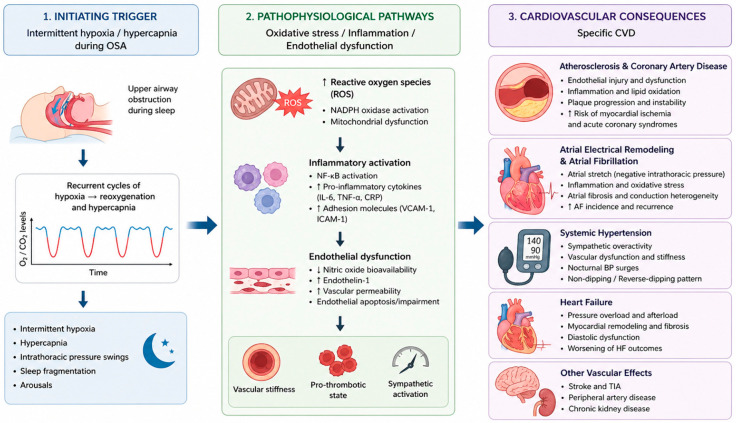
Beyond their hemodynamic effects, recurrent cycles of intermittent hypoxia followed by reoxygenation promote oxidative stress, systemic inflammation, and endothelial dysfunction, thereby accelerating vascular injury. These processes are mediated in part by the generation of reactive oxygen species and upregulation of pro-inflammatory pathways involving hypoxia-inducible factor-1, nuclear factor κB, endothelin-1, interleukins, tumour necrosis factor-α, and interferon-γ. The resulting reduction in nitric oxide bioavailability, increased arterial stiffness, platelet activation, and impaired endothelial repair contribute to the development and progression of hypertension and atherosclerosis [ref. 30] (Figure 2).
These mechanisms are also relevant to coronary artery disease. Chronic inflammation, oxidative stress, platelet activation, and surges in sympathetic tone may promote plaque progression and instability, increasing the risk of myocardial ischemia and acute coronary syndromes. In parallel, repetitive negative intrathoracic pressure swings increase myocardial wall stress and oxygen demand, further exacerbating ischemic burden in susceptible individuals [ref. 31]. OSA also contributes to cardiac electrical and structural remodelling. Sympathetic activation, atrial stretch related to negative intrathoracic pressure, and inflammation may favour atrial fibrosis and conduction heterogeneity, thereby increasing susceptibility to atrial fibrillation and arrhythmia recurrence after rhythm-control strategies [ref. 32]. In addition, sympathetic overactivation and catecholamine excess reduce insulin sensitivity and may induce β-cell apoptosis, thereby linking OSA to diabetes mellitus [ref. 33,ref. 34].
5. Clinical Presentation and Diagnosis
Despite being common, OSA is rarely reported spontaneously, so screening relies on recognizing suggestive symptoms and signs. Restless, non-restorative sleep and excessive daytime sleepiness are the most frequent symptoms, often accompanied by fatigue, morning headache, nocturia, and nocturnal reflux [ref. 35,ref. 36]. Less commonly, during a nocturnal awakening, patients may complain of a sensation of choking, suffocation, or palpitations [ref. 8]. Snoring is common (50–60% of cases) but nonspecific, while witnessed apneas are more specific though less frequently reported (10–15%) [ref. 37,ref. 38,ref. 39].
The Epworth sleepiness scale (ESS) is widely used to quantify sleepiness, although it is not specific to OSA [ref. 40]. Screening tools such as the Berlin and STOP-Bang questionnaires help estimate OSA risk in primary care and hospital settings (Table 1) [ref. 41,ref. 42]. Physical findings suggestive of OSA include obesity, large neck circumference, or upper-airway anatomical narrowing. Polysomnography remains the diagnostic gold standard, providing full sleep staging and respiratory monitoring (airflow, thoracoabdominal movements, oximetry, electrocardiography, EEG). Limitations include cost, limited availability, and possible “first-night effect” [ref. 43]. Home cardiorespiratory monitoring offers a more accessible alternative but lacks EEG and has slightly lower diagnostic accuracy (sensitivity: 79%, 95% confidence interval [CI]: 71–86%; specificity: 79%, 95% CI: 63–89%) [ref. 44,ref. 45]. Oximetry-only devices or implantable device sensors may assist in screening but still require confirmatory testing [ref. 46]. There is growing interest in the potential role of wearable devices (bracelets, chest bands, adhesive patches, headsets, and rings) for both the diagnosis and monitoring of OSA [ref. 47].
Table 1: Diagnostic tools for screening and diagnosis of obstructive sleep apneas.
| Tool | Description | Advantages | Disadvantages |
|---|---|---|---|
| Questionnaire | |||
| Epworth Scale | Assessment and staging of daytime sleepiness indifferent situations | Useful screening toolAccurate estimation of sleepinessEffective evaluation of therapeutic response | Nonspecific for OSA |
| BerlinQuestionnaire | Assessment of the likelihood of OSA based onsnoring, apneas, asthenia, sleepiness, obesity, hypertension | Useful screening toolLow score is associated with a low OSA risk | Low specificity instratifying OSA severity |
| STOP-BangQuestionnaire | Assessment of the likelihood of OSA based on snoring, sleepiness, apneas, hypertension, obesity, neck width, age, sex | Useful screening toolLow score is associated with a low OSA risk | Low specificity instratifying OSA severity |
| Monitoring Systems | |||
| TraditionalPolysomnography | Multi-channel recording (EEG, EOG, EMG, ECG, SaO2, thoracoabdominal movements, airflow) | Diagnostic accuracyPhases of sleep and arousalsCurrent gold standard | High costLow availability“First-night” effectOnly at night |
| AmbulatoryPolysomnography | Multi-channel recording (EEG, EOG, EMG, ECG, SaO2, thoracoabdominal movements, airflow) | Phases of sleep and arousalsAmbulatoryReduced “first night” effect | High costReduced accuracy andvalidationOnly at night |
| Cardiorespiratory Monitoring | Multi-channel recording (ECG, SaO2, thoracoabdominal movements, airflow) | AmbulatoryReduced discomfortDuration up to 24 hLow costHigh availability | Absence of EEGPossibleunderestimationReduced accuracy and validation |
| Oximetry/airflow | Mono-channel recording (SaO2 or airflow) | AmbulatoryReduced discomfortLow costHigh availability | Absence of EEGPossibleunderestimationNot discriminating OSA and CA |
| ImplantableDevices | Assessment of transthoracic impedance by sensors included in PM/ICD | AmbulatoryContinuous recordingIntegration with different data(arrhythmias, congestion estimation, …) | Limited to PM/ICD carriersIntervendor variabilityLimited discrimination of OSA and CAAbsence of EEG and SaO2 |
CA, central apneas; EEG, electroencephalogram; EMG, electromyogram; EOG, electrooculogram; ICD, implantable cardioverter–defibrillator; OSA, obstructive sleep apnea; PM, pacemaker; SaO2, oxygen saturation.
6. Obstructive Sleep Apneas and Cardiovascular Disease
6.1. Systemic Hypertension
Intermittent hypoxia in OSA activates the sympathetic system, increasing arterial tone and BP. OSA is found in 30–50% of hypertensive patients, and ~50% of individuals with OSA develop hypertension [ref. 48]. OSA represents the leading cause of resistant hypertension, accounting for up to 80% of cases [ref. 1,ref. 49]. Patients with untreated OSA have a 2–3-fold higher risk of developing hypertension compared with those receiving treatment [ref. 50,ref. 51,ref. 52]. A meta-analysis of 26 studies showed a dose–response relationship: mild, moderate, and severe OSA increased hypertension risk by 18%, 32%, and 56% respectively [ref. 52]. The association is stronger in Caucasian patients and in men compared with women [ref. 52,ref. 53]. Notably, greater night-to-night variability in AHI independently predicts uncontrolled hypertension, increasing risk by ~50–70% regardless of OSA severity [ref. 54]. OSA is highly prevalent in non-dipper (71%) and reverse-dipper (74%) BP profiles and increases the risk of non-dipping by ~47% [ref. 26,ref. 55,ref. 56]. Similarly, patients with non-dipping or reverse-dipping patterns show a 2.7-fold or 3.5 fold higher risk of developing OSA than those with normal dipping [ref. 56].
Beyond overall AHI, the distribution of respiratory events across sleep stages may also influence cardiovascular risk. In particular, REM (rapid eye movement)-predominant OSA has gained attention because obstructive events during REM sleep are often longer, associated with deeper oxygen desaturation, and occur during a phase characterized by greater autonomic instability and sympathetic activation. These mechanisms may translate into a stronger hypertensive burden than events occurring predominantly during non-REM sleep. Observational data suggest that an elevated REM-AHI is associated with both prevalent and incident hypertension, even in some patients with low overall AHI [ref. 57]. Therefore, REM-specific respiratory burden may provide additional prognostic information beyond conventional AHI and could help identify patients who remain clinically relevant despite apparently mild disease. However, diagnostic criteria remain heterogeneous, prevalence varies according to the definition used, and evidence regarding long-term cardiovascular prognosis and optimal treatment is still limited. Similarly, whether REM-predominant OSA requires specific therapeutic strategies beyond standard OSA management remains uncertain [ref. 58].
Despite a clear mechanistic link between OSA and hypertension, randomized trials in asymptomatic (i.e., without daytime sleepiness) patients have not shown a preventive effect of continuous positive airway pressure (CPAP) on incident hypertension or cardiovascular events over long-term follow-up [ref. 59]. Conversely, observational data indicate that CPAP may lower the risk of developing hypertension in previously normotensive patients with OSA [ref. 60,ref. 61,ref. 62]. Two meta-analyses conducted on patients with resistant hypertension highlighted the modest action of CPAP in reducing 24 h ambulatory levels of systolic (SBP, −5 mmHg) and diastolic (DBP, −3 mmHg) blood pressure, although with high interindividual variability [ref. 63,ref. 64]. Other systematic reviews further confirmed that CPAP use reduces 24 h BP (mean difference for SBP: 4.7–7.2 mmHg, DBP: 2.9–4.9 mmHg) and resting heart rate, especially among patients with severe OSA, high cardiovascular risk or resistant hypertension and high adherence to CPAP [ref. 64,ref. 65,ref. 66,ref. 67]. Of note, the impact of CPAP on BP is characterized by high interpatient variability. Therefore, CPAP lowers BP in resistant hypertension, but its role in primary prevention among asymptomatic OSA remains unproven.
6.2. Pulmonary Hypertension
PH is detected in 70–80% of OSA patients evaluated by right heart catheterization [ref. 68], and ~20% of all patients with OSA develop PH, which is associated with worse outcomes [ref. 69]. Intermittent hypoxia promotes pulmonary vasoconstriction, inflammation, and vascular remodelling, increasing pulmonary vascular resistance [ref. 70]. T < 90% was significantly associated with right ventricular systolic pressure, ejection fraction, hypertrophy and mean pulmonary artery pressure [ref. 71]. Patients with OSA and PH have higher mortality than those without PH [ref. 72]. CPAP therapy has been demonstrated to reduce mean pulmonary artery pressure by 5 mmHg after 12 weeks [ref. 73].
6.3. Coronary Artery Disease
OSA is an independent risk factor for CAD. Intermittent hypoxia–reoxygenation increases oxidative stress, inflammation, and endothelial dysfunction, promoting atherosclerosis and acute coronary events. Indeed, OSA is associated with increased arterial stiffness and early atherosclerosis [ref. 1,ref. 74]. Sympathetic activation in OSA increases endothelial adhesion molecules and leukocyte recruitment, contributing to plaque progression and instability [ref. 75,ref. 76]. An observational cohort showed a 2.5-fold higher risk of myocardial infarction (MI), coronary revascularization, or CV death in patients with OSA compared with controls [ref. 77]. Severe OSA is present in ~40% of patients presenting with ST-elevation MI [ref. 78]. Notably, patients with OSA have a higher incidence of nocturnal MI, likely driven by hypoxic and hemodynamic stress [ref. 79,ref. 80]. The impact of CPAP on prognosis, cardiovascular events, and revascularization procedures remains under debate.
6.4. Atrial Fibrillation
OSA is a major risk factor for AF, with SDB detected in up to ~70% of AF patients [ref. 81,ref. 82]. Nocturnal AF is more frequent in patients with OSA than in the general population (3–5% vs. 0.4–1%) [ref. 83,ref. 84]. Autonomic imbalance, atrial remodelling, and conduction abnormalities contribute to AF development in OSA [ref. 18,ref. 85]. Additionally, sympathetic surges and intrathoracic pressure swings promote atrial stretch and electrical instability [ref. 81]. The VARIOSA-AF study showed a night-to-night association between OSA severity and AF episodes [ref. 86]. In addition, severe OSA is linked to higher stroke risk and reduced efficacy of antiarrhythmic drugs and AF ablation [ref. 81,ref. 87,ref. 88]. Indeed, observational studies suggest that patients with OSA have a ~30% higher risk of post-ablation AF [ref. 89]. In addition, patients with high-frequency AF (defined as persistent or paroxysmal with >6 symptomatic episodes of AF in the previous year) have an enhanced prevalence of SDB than those with low-frequency AF (paroxysmal with <6 symptomatic episodes in the previous year) [ref. 90]. Observational studies and recent meta-analyses have shown that CPAP reduces AF recurrence after cardioversion or ablation [ref. 91,ref. 92,ref. 93,ref. 94], whereas non-administration of CPAP increases recurrence risk by 57% [ref. 89]. Lifestyle interventions (weight loss, alcohol restriction) also reduce AF relapse [ref. 95,ref. 96]. However, the SAVE trial did not show AF prevention with CPAP in patients with moderate or severe OSA with a history of ischemic heart disease or cerebrovascular disease, likely due to poor adherence (3.3 h per night), and the possible inclusion of patients with CA as the prevailing phenotype [ref. 97].
6.5. Other Arrhythmias
Patients with OSA show a higher prevalence of bradyarrhythmias [ref. 98,ref. 99], and in one polysomnography study, 58% of patients with pacemakers for sick sinus syndrome had previously unrecognized sleep apneas [ref. 100]. CPAP therapy is associated with a 72–89% reduction in bradyarrhythmia episodes, especially for nocturnal episodes, thus potentially reducing the need for cardiac implantable devices [ref. 99,ref. 101]. Severe OSA is linked to an increased risk of sudden cardiac death (SCD) [ref. 102], likely due to intrathoracic pressure swings and autonomic imbalance, which promote ventricular repolarization instability [ref. 103]. Ventricular tachycardia is more frequent in OSA than in non-OSA patients (2.24% vs. 1.16%) [ref. 104], and SCD occurs more often during the night in OSA (46% vs. 21%), with higher AHI predicting SCD between midnight and 6 a.m. [ref. 105]. The risk of non-sustained ventricular tachycardia is 3-fold higher in severe OSA compared to subjects without SDB, with a dose–response relationship between AHI and ventricular arrhythmia burden [ref. 106].
6.6. Heart Failure
OSA-related pathophysiological alterations worsen HF through neurohormonal activation, oxidative and inflammatory stress, BP surges, arrhythmias, and acute preload/afterload changes induced by intrathoracic pressure swings [ref. 18]. In HF, venous congestion and fluid retention promote an upper-body fluid shift in the supine position, increasing neck and lung pressure and favouring upper-airway collapse and OSA development [ref. 107]. SDB is highly prevalent in HF, affecting 50–75% of patients [ref. 108,ref. 109]. OSA and CA frequently coexist, although one phenotype is usually predominant [ref. 108]. In HF with reduced ejection fraction (HFrEF), patients with an OSA-predominant pattern show better biventricular function, exercise tolerance, and survival than those with CA-predominant breathing [ref. 3,ref. 110,ref. 111]. Apnea prevalence varies by HF phenotype: CA is more frequent in HFrEF than in HF with mildly reduced (HFmrEF) and preserved EF (HFpEF) (66% vs. 48% vs. 34%), whereas OSA is more prevalent in HFpEF than in HFmrEF and HFrEF (53% vs. 29% vs. 20%). Moderate-to-severe OSA is also more frequent in HFpEF (30% vs. 11% vs. 10%) [ref. 112,ref. 113]. SDB is an independent predictor of mortality, hospitalization, and cardiovascular events in HF [ref. 109]. In fact, severe OSA increases the risk of hospitalization by ~1.5-fold [ref. 114]. Recent studies suggest that CPAP therapy results in improved management of clinical resources (i.e., emergency room access, hospitalization) in patients with HF [ref. 115,ref. 116]. Randomized trials show CPAP reduces neurohormonal activation, arrhythmic burden, and echocardiographic parameters in HFrEF with sleep apnea [ref. 117,ref. 118], but no major trial has yet demonstrated a prognostic benefit on hard outcomes in HF patients with OSA [ref. 71,ref. 119].
Adaptive servo-ventilation (ASV) is an advanced positive airway pressure modality mainly used for CA and Cheyne–Stokes respiration, as it dynamically adjusts ventilatory support and can also treat coexisting obstructive events. The ADVENT-HF trial evaluated the effect of ASV in patients with HFrEF and SDB (OSA: 73%); ASV did not impact the composite endpoint of mortality, cardiovascular hospitalization, new-onset AF or flutter, and appropriate cardioverter–defibrillator shock. However, a positive difference was reported for quality of sleep and quality of life in the intervention group [ref. 120]. Although ASV may improve symptoms, the SERVE-HF trial showed increased cardiovascular and all-cause mortality in patients with symptomatic HFrEF and predominant CA who were treated with ASV [ref. 121]. Therefore, ASV is generally contraindicated in this specific setting. The apparently divergent findings of SERVE-HF and ADVENT-HF may reflect differences in patient selection, SDB phenotype, device algorithms, and treatment adherence, underscoring the need for careful phenotyping before considering ASV in HF. Further studies are needed to better define whether selected HF phenotypes may benefit from individualized use of ventilatory support [ref. 122].
7. Prognosis
Several studies confirm the negative prognostic impact of OSA on cardiovascular outcomes. In the MESA (Multi-Ethnic Study of Atherosclerosis) study, which involved 5338 patients without prior cardiovascular disease with a mean follow-up of 7.5 years, OSA predicted all-cause mortality (hazard ratio [HR]: 2.44, 95% CI: 1.36–4.37) and cardiovascular events, including MI, stroke, angina, resuscitated arrest, and cardiovascular death (HR: 2.16, 95% CI: 1.30–3.58) [ref. 123]. Other studies have shown that untreated severe OSA is associated with a ~3-fold increase in all-cause mortality compared with controls [ref. 61,ref. 124,ref. 125]. A meta-analysis of 16 studies (24,308 patients) confirmed higher overall and cardiovascular mortality in severe OSA compared with milder disease [ref. 126].
Sex-specific prognostic differences have also been observed. In a pooled analysis from ARIC (Atherosclerosis Risk in Communities) and SHHS (Sleep Heart Health Study) studies, women with severe OSA had more comorbidities and a higher risk of incident HF, CAD, left ventricular hypertrophy, or death than men [ref. 127].
8. Treatment
The management of OSA currently focuses on modifiable risk factors and the use of CPAP. Emerging pharmacological therapies may complement this framework rather than replace established treatments [ref. 17]. In particular, anti-obesity agents such as GLP-1 receptor agonists may be especially valuable in overweight or obese patients with OSA, whereas novel anti-apneic compounds may represent alternatives or adjuncts in selected patients intolerant to CPAP or with specific pathophysiological phenotypes. However, their role within clinical practice is still evolving, and further evidence is needed to define their long-term efficacy, safety, and optimal integration into treatment algorithms. Table 2 provides an overview of the currently available therapeutic options for obstructive sleep apnea.
Table 2: Therapeutic options for obstructive sleep apnea.
| Therapy(Drug/Device) | Mechanism ofAction | Clinical Study | Clinical Outcomes | ClinicalIndication |
|---|---|---|---|---|
| Non-Pharmacological Therapy | ||||
| CPAP | Provides continuous positive airway pressure preventing upper-airway collapse | MA: Benjafield et al., 2025 [ref. 66]MA: Feltner et al., 2022 [ref. 195]MA: Soltaninejad et al., 2025 [ref. 196]MA: Tregear et al., 2010 [ref. 197]MA [ref. 63,ref. 64,ref. 65,ref. 66,ref. 67]OS: Montesi et al., 2012 [ref. 73]OS [ref. 92,ref. 93,ref. 94]OS: Simantirakis et al., 2004 [ref. 98]RCTs [ref. 117,ref. 118,ref. 182]RCT: Barbe et al. [ref. 59] | ↓Mortality and CV-Mortality↑Sleep-QoL and overall QoL↑Working memory and emotional scales↓Road accidents↓BP in resistant HTA↓BP in PH↓AF recurrence after DCCV/CA↓Bradyarrhythmias↓Neuro-hormonal activation, arrhythmias, ↑echo parameters in HFrEFNo ↓of incident HTA | First-line therapy for symptomatic OSA |
| LifestyleIntervention for Weight Loss and Exercise | Reducesperipharyngeal fat, fluid shift, and ventilatory load | MA [ref. 133,ref. 134,ref. 135,ref. 136,ref. 137,ref. 138,ref. 139,ref. 154,ref. 155,ref. 157]RCT: Chirinos et al., 2014 [ref. 142]RCT: Abed et al., 2016 [ref. 95] | ↓AHI, ODI, ESS↓BP↓AF recurrence | Recommended in all overweight and obese patients |
| Bariatric Surgery | Marked weight loss and airway fat reduction | MA [ref. 148,ref. 149] | ↓BMI, AHI, RDI, ESS,↑Sleep-parameters | Recommended in selected obese patients |
| MAD | Mandibular protrusion enlarges upper-airway lumen | MA: Ramar et al., 2015 [ref. 200]MA: Bratton et al., 2015 [ref. 201] | ↓AHI↓BP similar to CPAP | Alternative to CPAP in mild–moderate OSA or CPAP intolerance |
| Hypoglossal Nerve Stimulation | Stimulates upper-airway dilator muscles | STAR trial [ref. 209]OS: Heiser et al., 2022 [ref. 214] | ↓AHI, ODI, T < 90%, ESS, FOSQ scale↑Effect size vs. CPAP | Approved for selected moderate–severe OSA unfit for CPAP |
| SupplementalOxygen | Reduces hypoxemia and chemoreflex drive | MA [ref. 240,ref. 241] | Modest ↓AHI (inferior to CPAP)No effect on BP or sleepiness | Not recommended as monotherapy |
| Pharmacological Therapy | ||||
| GLP-1RA | Weight loss, reduced hypoxic burden and upper-airway fat through appetite suppression and metabolic regulation | SCALE Sleep Apnea trial [ref. 168]SURMOUNT-OSA trial [ref. 170]MA [ref. 175,ref. 176] | Liraglutide: ↓AHI, HbA1c, SBPTirzepatide: ↓weight, AHI, hypoxic burden, SBP, hs-CRP, PROMIS-SRI, and PROMIS-SD scales↓AHI | Approved for obesity. It represents an emerging option for OSA. |
| Acetazolamide | Carbonic anhydrase inhibition lowers loop gain | MA [ref. 237]RCT: Eskandari et al., 2018 [ref. 239] | Controversial results about AHI reductionSynergic effect with CPAP on BP and AHI | Although effective in CSA, experimental/selective role in OSA |
| Sulthiame | RCT: Hedner et al., 2022 [ref. 238] | ↓AHI, high rate of AEs | Experimental, not guideline-recommended | |
| Zonisamide | RCT: Eskandari et al., 2014 [ref. 239] | ↓AHIHigh rate of AE | ||
| AD109(aroxybutynin +atomoxetine) | Noradrenergic and antimuscarinic actionincreases tone of airway dilators | RCTs: LunAIRo and SynAIRgy trials [ref. 225,ref. 226] | ↓AHI, ODI, PROMIS-Fatigue and Sleep Impairment T-scores | Experimental, not guideline-recommended |
| TCA (protriptyline, desipramine) | Noradrenergic action increases tone of airway dilators | RCTs [ref. 227,ref. 229]MA: AbdelFattah et al., 2020 [ref. 230] | Modest ↓AHI | Not recommended due to poor tolerability |
| SSRIs (mirtazapine, paroxetine,fluoxetine) | Serotonergic modulation of airway motor neurons | MA: AbdelFattah et al., 2020 [ref. 230] | Modest ↓AHI,No effects on sleepiness | Not recommended |
| Z-drugs (eszoplicone, zolpidem), sedatives (trazodone, sodium oxybate), andpimavanserin | Increases arousal threshold | RCTs: [ref. 244,ref. 245] | Controversial results about AHI reduction and sleepiness | Experimental; not guideline-recommended; safety concerns |
| Dronabinol | Cannabinoid receptor agonist modulating ventilatory control and arousal threshold | PACE trialMA [ref. 247] | ↓AHIHigh rate of AE (70–80%)Effective but unsafe in combination therapy (acetazolamide, atomoxetine) | Notrecommended by AASM [ref. 249] |
| Modafinil/Armodafinil/Solriamfetol | Dopamine–norepinephrine reuptake inhibition promoting wakefulness | MA [ref. 249,ref. 254,ref. 255,ref. 256]RCT [ref. 253] | ↓Sleepiness, attention, and vigilanceCV-AEs | Approved for residual sleepiness in treated OSA without CV contraindications |
| Pitolisant | Histamine H3 inverse agonist promoting wakefulness | MA [ref. 249,ref. 254,ref. 255,ref. 256]RCT [ref. 252] | ↓SleepinessAE: headache and insomnia | Approved for residualsleepiness in OSA |
AE, adverse event; AF, atrial fibrillation; AHI, apnea–hypopnea index; BMI, body mass index; BP, blood pressure; CA, catheter ablation; CSA, central sleep apnea; CPAP, continuous positive airway pressure; DBP, diastolic blood pressure; DCCV, direct-current cardioversion; ESS, Epworth sleepiness scale; FOSQ, functional outcomes of sleep questionnaire; GLP-1RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycated hemoglobin; HFrEF, heart failure with reduced ejection fraction; hs-CRP, high-sensitivity C-reactive protein; HTA, hypertension; IS, interventional study; MA, meta-analysis; ODI, oxygen desaturation index; OS, observational study; OSA, obstructive sleep apnea; PH, pulmonary hypertension; PROMIS, patient-reported outcomes measurement information system; PROMIS-SRI/PROMIS-SD, sleep-related impairment/sleep disturbance; QoL, quality of life; RCT, randomized controlled trial; RDI, respiratory disturbance index; SBP, systolic blood pressure; ↑, increased; ↓, decreased.
8.1. Lifestyle Changes
Lifestyle change is the cornerstone of OSA treatment and includes abstinence from alcohol, adoption of an appropriate sleeping position, exercise, and weight loss through a hypocaloric diet. In patients with predominantly positional OSA, namely those with an AHI that decreases by ≥50% in the non-supine position, avoiding the supine position during sleep is recommended [ref. 128]. Several devices (e.g., structured pillows, positional supports, vibratory feedback systems) can promote lateral sleep [ref. 129]. A systematic review showed that positional therapy is superior to no intervention but less effective than CPAP [ref. 129].
8.2. Weight Loss: Lifestyle Interventions and Bariatric Surgery
Obesity is the main risk factor for the development of OSA and accounts for at least 40% of cases. It is therefore a crucial goal in the management of OSA [ref. 130]. Weight loss is always recommended for overweight or obese patients with OSA, even if asymptomatic or with mild symptoms [ref. 8,ref. 131,ref. 132]. Previous meta-analyses have demonstrated the beneficial impact of lifestyle interventions in this population in terms of reduction in AHI, ODI, ESS, and sleep-related parameters (i.e., arousal index and sleep efficiency), regardless of intervention duration or CPAP use [ref. 133,ref. 134,ref. 135,ref. 136,ref. 137,ref. 138,ref. 139]. Interestingly, lifestyle interventions displayed reduced effects in women compared with men, thus suggesting that OSA may present with a different phenotype in females [ref. 139]. The role of psychological or coaching support for weight loss still needs to be elucidated [ref. 140].
In the largest study evaluating lifestyle intervention in obese patients with OSA and diabetes (i.e., the AHEAD Study), diet and exercise resulted in a mean weight loss >10 kg and a reduction in AHI of 9.7 events/h after one year of follow-up, compared with education in diabetes management alone [ref. 141]. In addition, patients with moderate-to-severe OSA undergoing combined therapy with CPAP plus weight loss (defined as dietary intervention and exercise sessions) showed a greater reduction in systolic and mean BP values, compared to subjects receiving CPAP alone or weight loss alone [ref. 142]. Few studies have evaluated the long-term effects of lifestyle intervention. Beneficial effects may persist after 4 years despite a significant weight regain [ref. 143]. Benefits of lifestyle intervention were significant across OSA stages, but a stronger effect was reported in severe OSA [ref. 144,ref. 145].
In cohorts of patients eligible for bariatric surgery, the prevalence of OSA was estimated to be approximately 75%, with most of them being severe [ref. 8,ref. 146,ref. 147]. Meta-analyses demonstrated that weight loss induced by bariatric surgery led to a significant reduction in BMI and AHI, but also to an improvement in pulmonary or sleeping functional parameters (forced vital capacity, mean SaO2, nadir SaO2, sleep efficiency, N3-REM%) and patient-reported measures of sleep quality (i.e., ESS) [ref. 148,ref. 149]. Pooled data displayed a mean reduction in AHI of 19 events/h, a mean BMI reduction of 12 kg/m2 after surgery, and a mean RDI reduction of 34 events/h, with OSA remission rates around 65% at 1 year [ref. 150]. Although bariatric surgery is highly associated with improvement in respiratory and sleep parameters (~68%), the incidence of OSA regression is considered relatively low (~16%) [ref. 147,ref. 151].
An inverse dose-dependent association between physical activity and prevalence of OSA exists [ref. 152]. In randomized clinical trials including patients with moderate or severe OSA, exercise resulted in a reduction of 24–34% in the severity of OSA, even in the absence of significant changes in body weight [ref. 135]. The mechanisms of this weight-independent benefit are still unclear but may be related to the redistribution of body fat, reduced nocturnal rostral fluid shift from the legs, increased tone of the pharyngeal muscles, and improved quality of sleep [ref. 8,ref. 135,ref. 153]. Pooled data reported a mean reduction in AHI of 6–7 events/h, improved ESS score and peakVO2, despite poor changes in BMI [ref. 154,ref. 155,ref. 156,ref. 157]. Although CPAP was superior in determining AHI reduction compared to exercise alone in patients with HF and OSA, exercise was superior to CPAP in improving daytime sleepiness and quality of life, but the two interventions had a synergistic effect when combined [ref. 158]. Moreover, the combination of resistance training and aerobic exercise is more effective compared with aerobic training alone [ref. 155,ref. 159]. In addition to systemic exercise, one meta-analysis demonstrated that oropharyngeal or respiratory exercise (e.g., lip or breathing exercise) led to a reduction in snoring and a 50% decrease in AHI [ref. 160]. Although difficult to compare because of the heterogeneity in effect size and intervention procedures, aerobic exercise, combined exercise, and oropharyngeal exercise showed similar effects in patients with OSA [ref. 161].
8.3. Weight Loss: Pharmacological Therapy
Pharmacological therapy has gained an important role in achieving significant and sustained weight loss. In particular, the glucagon-like peptide-1 receptor agonists (GLP-1RAs), which were originally studied in the context of type 2 diabetes, have emerged as a novel class of pharmacological agents capable of pleiotropic effects by regulating glucose and lipid metabolism [ref. 162]. GLP-1RAs promote insulin secretion, inhibit glucagon release, delay gastric emptying, reduce central appetite drive, and exert systemic anti-inflammatory effects [ref. 163,ref. 164]. Clinical trials investigating GLP-1RA beyond diabetes have reported beneficial effects on weight loss, mortality, cardiovascular events, renal protection, and neurodegenerative outcomes across various populations, thus expanding the potential applications of these drugs [ref. 165,ref. 166,ref. 167].
The SCALE Sleep Apnea trial included obese patients with moderate-to-severe OSA who were unwilling or unable to use CPAP and were randomized to liraglutide or placebo as an adjunct to diet and exercise. Liraglutide, administered at a dose of 3.0 mg, led to a modest reduction in AHI (mean difference: 6.1 events/h), body weight (mean difference: 4.2%), glycated hemoglobin, and SBP after 32 weeks of treatment compared with placebo [ref. 168].
The effect of tirzepatide, a dual agonist targeting both GLP-1receptor and the glucose-dependent insulinotropic polypeptide receptor (GIP-R), has recently been investigated in the SURMOUNT-OSA trial [ref. 169,ref. 170]. The study included patients with OSA with or without concomitant CPAP therapy, randomized to tirzepatide or placebo. After 52 weeks of treatment with tirzepatide at a dose of 10–15 mg, patients achieved a weight reduction of 16% and 17% in the CPAP and non-CPAP groups, respectively. Compared with placebo, tirzepatide was associated with an additional AHI reduction of 20 and 24 events/h in patients with and without CPAP, respectively. In addition, tirzepatide reduced sleep apnea-specific hypoxic burden, calculated according to the frequency, duration, and depth of oxygen desaturation during polysomnography, compared with controls (mean difference: −70% min/h, and −61% min/h). Treatment with tirzepatide also reduced SBP, particularly among patients not receiving CPAP (mean difference: −7.6 mmHg, and −3.7 mmHg), as well as hs-CRP (mean difference: −0.7 mg/L, and −1.0 mg/L). Patient-reported sleep disturbance assessed using PROMIS-SRI and PROMIS-SD also improved with tirzepatide [ref. 170].
A recent meta-analysis of six studies, including patients with OSA (n = 1032) receiving GLP-1RAs, including tirzepatide or liraglutide, reported an estimated AHI reduction of 9.5 events/h compared with controls not receiving therapy [ref. 168,ref. 170,ref. 171,ref. 172,ref. 173,ref. 174,ref. 175,ref. 176]. Concomitant CPAP use did not appear to modify pharmacological effects [ref. 175].
Beyond weight loss, GLP-1RAs may also favourably affect OSA through remodelling of upper-airway fat deposition [ref. 165] and stabilization of respiratory drive and breathing rhythm [ref. 177].
8.4. Continuous Positive Airway Pressure
CPAP remains the first-line treatment for symptomatic OSA of any severity. By delivering continuous positive pressure through a nasal or oronasal mask, it prevents upper-airway collapse during sleep and normalizes AHI in most patients (>90%) [ref. 178,ref. 179,ref. 180]. Its effectiveness, however, is strongly dependent on adherence, with greater clinical benefit observed with longer nightly use. Although a minimum use of 4 h/night is often considered acceptable, higher adherence is consistently associated with better outcomes, and improved mask interfaces, behavioural support, and remote monitoring may enhance long-term use [ref. 8,ref. 178,ref. 179].
Beyond symptom control, the cardiovascular effects of CPAP have generated heterogeneous results. Overall, CPAP consistently lowers sympathetic activation and modestly reduces blood pressure, particularly in patients with resistant hypertension, severe OSA, or high cardiovascular risk. In selected cohorts, reductions in ambulatory BP of approximately 3–8 mmHg have been reported [ref. 63,ref. 64,ref. 65,ref. 66,ref. 67,ref. 181]. In patients with HFrEF and OSA, CPAP has also been associated with improvements in left ventricular ejection fraction, cardiac remodelling, pulmonary pressures, and right ventricular function [ref. 182,ref. 183], while observational studies suggest fewer hospitalizations and lower mortality [ref. 184,ref. 185,ref. 186].
In contrast, several large randomized trials evaluating CPAP for hard cardiovascular outcomes have been neutral. In the CERCAS trial, CPAP did not reduce incident hypertension or cardiovascular events in patients without prior cardiovascular disease, although post hoc analyses suggested benefit in adherent users (>4 h/night) [ref. 1,ref. 59]. Similarly, the SAVE trial, which enrolled patients with established cardio- or cerebrovascular disease, found no reduction in major cardiovascular events after 43 months despite improved sleepiness; however, patients with better adherence showed lower rates of stroke and cerebrovascular events [ref. 97]. Comparable findings emerged from the RICCADSA and ISAACC trials, in which overall event reduction was not demonstrated, whereas signals of benefit were more evident among patients with higher CPAP use or selected clinical profiles [ref. 187,ref. 188].
These apparently contradictory findings may be explained by several factors. First, many randomized trials excluded or underrepresented highly symptomatic patients, who may derive greater benefit from treatment. Second, average adherence in pragmatic trials was often modest and may have been insufficient to influence long-term cardiovascular risk. Third, cardiovascular benefit may require prolonged exposure and longer follow-up than that achieved in some studies. Finally, OSA is a heterogeneous disorder: patients with severe nocturnal hypoxemia, resistant hypertension, marked sleepiness, high hypoxic burden, or specific cardiometabolic phenotypes may respond differently than minimally symptomatic patients with milder disease.
This interpretation is supported by pooled analyses. Some meta-analyses focused on randomized trials reported no clear survival benefit [ref. 189], whereas larger analyses including observational cohorts have shown lower all-cause and cardiovascular mortality, particularly among adherent patients and those with moderate-to-severe OSA or concomitant CAD [ref. 66,ref. 190,ref. 191]. A dose–response relationship has also been suggested, with the greatest benefit in patients using CPAP for ≥6 h/night [ref. 66].
A particularly relevant unresolved issue concerns patients with asymptomatic or minimally symptomatic OSA. Current evidence does not support routine CPAP prescription solely for cardiovascular prevention in all such individuals, as major randomized trials largely failed to demonstrate a clear reduction in hard outcomes in these populations [ref. 97]. Nevertheless, selected asymptomatic patients with severe OSA, marked nocturnal hypoxemia, resistant hypertension, AF, or established cardiovascular disease may still derive benefit, particularly when adherence is high [ref. 187]. Therefore, treatment decisions in asymptomatic OSA should be individualized according to global cardiovascular risk, OSA phenotype, and patient preference.
Taken together, current evidence suggests that CPAP should not be viewed as a universal cardioprotective therapy for all patients with OSA. Rather, its prognostic benefit is likely concentrated in selected subgroups characterized by symptomatic disease, greater OSA burden, higher cardiovascular risk, and good treatment adherence. Future studies should focus on phenotype-guided patient selection and strategies to improve long-term adherence.
In addition to potential prognostic effects, CPAP consistently improves quality of life, daytime sleepiness, and functional status [ref. 180]. Benefits are greatest in patients with excessive daytime sleepiness or moderate-to-severe OSA, but can also be observed in selected patients with mild disease [ref. 192,ref. 193]. Meta-analyses further suggest modest improvements in general and sleep-related quality of life, cognition in older adults, and a marked reduction in road traffic accident risk [ref. 194,ref. 195,ref. 196,ref. 197].
Bilevel positive airway pressure (BiPAP), which provides inspiratory pressure support above expiratory positive airway pressure, may improve tolerance in patients intolerant to CPAP and is particularly useful in conditions associated with hypoventilation or hypercapnia (e.g., neuromuscular disease, chronic hypoventilation syndromes) [ref. 198,ref. 199].
8.5. Mandibular Advancement Devices and Surgical Procedures
Mandibular advancement devices (MADs) represent a non-invasive option for patients with mild–moderate OSA or for those intolerant to CPAP [ref. 8]. Patients with anatomical narrowing of the upper airways are likely to benefit most from MAD therapy. These devices consist of intraoral plates that advance the mandible, increasing upper-airway calibre. A meta-analysis of 34 studies showed a mean AHI reduction of 13.6 events/h (95% CI: 12.0–15.3) with MAD therapy [ref. 200]. Another meta-analysis of 51 studies reported comparable BP reductions with MAD and CPAP [ref. 201].
Surgery aims to enlarge or stabilize the upper airway but is supported by limited evidence, short follow-up, and scarce data on cardiovascular outcomes [ref. 202]. Uvulopalatopharyngoplasty reduces AHI but has largely been replaced by safer soft-tissue techniques (e.g., barbed and expansion pharyngoplasty) [ref. 203,ref. 204,ref. 205]. Maxillomandibular advancement is the most effective surgical option, reducing AHI by ~80% and improving ESS score (from 13.5 to 3.2) in selected patients intolerant to CPAP [ref. 206]. However, surgical morbidity (pain, malocclusion, aesthetic and sensory complications) limits its use, and long-term cost–benefit data remain insufficient [ref. 206,ref. 207].
8.6. Nerve Stimulation
Stimulation of upper-airway dilator muscles represents a novel therapeutic option for OSA. The only FDA-approved device delivers timed stimulation to the medial branch of the hypoglossal nerve via an implanted electrode, coupled with a thoracic sensor that detects respiratory effort and a subcutaneous pulse generator placed in the chest. This treatment was approved for patients unfit for CPAP with at least moderate OSA [ref. 208]. In the STAR trial, hypoglossal nerve stimulation reduced AHI from 29.3 to 9.0 events/h at one year, with sustained benefit at 5 years of follow-up [ref. 209,ref. 210]. Bilateral stimulation systems and non-invasive transcutaneous approaches are currently under evaluation, with preliminary results showing a good safety and efficacy profile [ref. 211,ref. 212,ref. 213]. A comparative study showed that hypoglossal stimulation improves daytime sleepiness to a greater extent than CPAP, while achieving a similar reduction in AHI [ref. 214].
8.7. Pharmacological Therapy
8.7.1. Pharmacotherapy Targeting Pharyngeal Muscle Tone
Experimental pharmacological therapies for OSA primarily aim to enhance the tone of the upper-airway dilator muscles and improve central ventilatory control [ref. 215]. One approach involves modulating central respiratory control through drugs affecting noradrenergic and serotoninergic neurotransmission, referred to as “anti-apneic neuromuscular modulators.”
Among these, the combination of selective norepinephrine reuptake inhibitors (e.g., atomoxetine, reboxetine) and antimuscarinic agents (e.g., oxybutynin, hyoscine butylbromide) has shown reductions in AHI (35–62%) but failed to improve sleepiness [ref. 216,ref. 217,ref. 218,ref. 219,ref. 220]. Atomoxetine monotherapy has demonstrated inconsistent results regarding AHI and daytime sleepiness [ref. 220,ref. 221]. AD109, a combination of atomoxetine (75 mg) and oxybutynin (2.5 mg), has been tested in two Phase 3 trials [ref. 222,ref. 223]. In the SynAIRgy study (n = 639), AD109 significantly reduced AHI (6.1 vs. 0.4 events/h, p < 0.0001) and improved secondary endpoints like ODI and hypoxic burden. In the LunAIRo trial (n = 660), AD109 demonstrated a 46.8% reduction in AHI compared to 6.8% in the placebo group after 26 weeks, with improvements in hypoxic burden and ODI [ref. 224,ref. 225]. Although AD109 showed mild adverse effects, it demonstrated promising reductions in OSA severity, with 39.6% of participants experiencing a ≥50% AHI reduction [ref. 226].
On the other hand, the use of tricyclic antidepressants, such as protriptyline and desipramine, resulted in only modest reductions in AHI, with poor tolerability due to anticholinergic and cardiovascular side effects, making their routine use in OSA management questionable [ref. 227,ref. 228,ref. 229,ref. 230,ref. 231]. Similarly, selective serotonin reuptake inhibitors (SSRIs) like mirtazapine, paroxetine, and fluoxetine have shown inconsistent results in reducing AHI and are no longer considered viable options for OSA treatment due to limited clinical benefit and adverse effects [ref. 230,ref. 232]. The failure of SSRIs in OSA treatment may be linked to increased cholinergic inhibition of hypoglossal motor neurons during REM sleep, reducing their response to excitatory neurotransmitters [ref. 233]. Notably, mirtazapine was also associated with weight gain in one study [ref. 234].
8.7.2. Pharmacotherapy Targeting Loop Gain
Certain forms of OSA are linked to altered acid–base balance due to increased chemoreceptor sensitivity, a condition known as “high loop gain” OSA [ref. 232,ref. 235]. High loop gain describes an unstable ventilatory control system, where small fluctuations in arterial CO2 or O2 levels trigger exaggerated ventilatory responses, leading to unstable breathing and promoting both OSA and CA [ref. 236]. Targeting the downregulation of high loop gain offers a potential pharmacological approach to OSA management.
Carbonic anhydrase inhibitors, such as acetazolamide, have been investigated as a potential treatment by reducing AHI through modulation of acid–base balance. However, clinical studies have shown mixed results. While acetazolamide has demonstrated effectiveness in CA, its impact on OSA has been less consistent, with meta-analyses reporting no significant reduction in AHI across studies [ref. 236,ref. 237]. The effects of acetazolamide in reducing AHI were modest, and further studies are required to better understand its role in OSA treatment.
A recent clinical study evaluated treatment for 4 weeks with the carbonic anhydrase inhibitor sulthiame (200 mg and 400 mg) in patients with moderate-to-severe OSA, reporting a reduction in AHI of 41% [ref. 238]. However, high dose sulthiame resulted in common paresthesias and headaches.
Other drugs, such as zonisamide and topiramate, have also been studied for their potential impact on OSA, but evidence of their effectiveness remains inconclusive. Zonisamide showed some benefit in reducing AHI and oxygen desaturation index (ODI), although adverse effects like dysphoria were noted in a proportion of patients [ref. 239].
Supplemental oxygen, another strategy aimed at modulating loop gain, has shown limited benefit compared to CPAP in reducing AHI and has not demonstrated improvements in blood pressure or sleepiness [ref. 240,ref. 241].
8.7.3. Pharmacotherapy Targeting Arousal Threshold
Sedative and myorelaxant drugs, such as benzodiazepines and Z-drugs (zolpidem, zopiclone, eszopiclone), have traditionally been contraindicated in OSA due to concerns about worsening upper-airway collapse. However, recent studies suggest that these medications may have a beneficial effect in certain OSA patients, especially those with a low arousal threshold [ref. 232,ref. 242]. In these individuals, the intense ventilatory stimulus following an obstructive event may lead to early arousal, which disrupts breath and sleep stabilization. Sedatives could mitigate this issue by attenuating the arousal response, as suggested by studies in patients with moderate OSA [ref. 232,ref. 243].
The effectiveness of eszopiclone in reducing AHI remains controversial, likely due to study heterogeneity [ref. 244,ref. 245]. Additionally, the use of sedatives like temazepam has been associated with respiratory depression in OSA patients with high central chemosensitivity [ref. 243]. Other sedatives, such as trazodone and sodium oxybate, have shown mixed results in terms of AHI reduction, with limited evidence supporting their use for OSA treatment [ref. 232].
Dronabinol, a cannabinoid receptor agonist, has demonstrated some efficacy in reducing AHI and improving sleepiness in a small trial (PACE study), although its safety profile raises significant concerns, with neuropsychiatric and gastrointestinal side effects reported in 70–80% of participants [ref. 246,ref. 247]. Furthermore, the American Academy of Sleep Medicine does not recommend cannabinoids for routine OSA treatment due to insufficient long-term safety data [ref. 248]. While some trials suggest potential benefits of dronabinol in combination with other treatments like atomoxetine or acetazolamide, the overall evidence remains limited, and these therapies are not currently considered standard care for OSA.
8.7.4. Wakefulness-Promoting Agents
An important consequence of OSA is excessive daytime sleepiness, which has a substantial impact on patients’ quality of life. A meta-analysis of eight studies demonstrated the efficacy of modafinil and armodafinil, dual dopamine-norepinephrine reuptake inhibitors, in improving sleepiness, attention and vigilance in patients with OSA, despite their lack of efficacy in improving quality of life and cognitive function [ref. 249]. However, these drugs may present contraindications due to their hypertensive and arrhythmogenic effects mediated by adrenergic activation [ref. 250]. Moreover, armodafinil led to weight loss because of its ability to suppress appetite when combined with lifestyle interventions over 6 months, although it did not improve OSA severity or sleepiness [ref. 251]. Modafinil and armodafinil have received FDA approval for patients with OSA and residual sleepiness.
A multicenter study including 244 patients with persistent OSA despite treatment with CPAP evaluated the effect of pitolisant, a histaminergic antagonist that promotes arousal in patients with OSA. The drug significantly reduced daytime sleepiness in treated patients compared with controls, despite being associated with more frequent adverse effects (mainly headache and insomnia) than placebo [ref. 252]. Finally, solriamfetol, a dopamine-norepinephrine reuptake inhibitor, has proven effective in improving sleepiness and quality of life in patients with OSA, despite a higher percentage of mild-to-moderate adverse effects (headache, nausea, loss of appetite, anxiety, nasopharyngitis) compared to placebo [ref. 253]. Systematic reviews confirmed the efficacy of wakefulness-promoting agents in improving self-reported sleepiness in patients with OSA, with solriamfetol being the most effective and pitolisant being the safest in patients with cardiovascular disease [ref. 254,ref. 255,ref. 256].
9. Who Should Be Screened and Treated for OSA?
There is no universal consensus on systematic screening strategies for OSA [ref. 43,ref. 131]. A practical approach to screening and management of patients at risk for OSA is summarized in Figure 3.
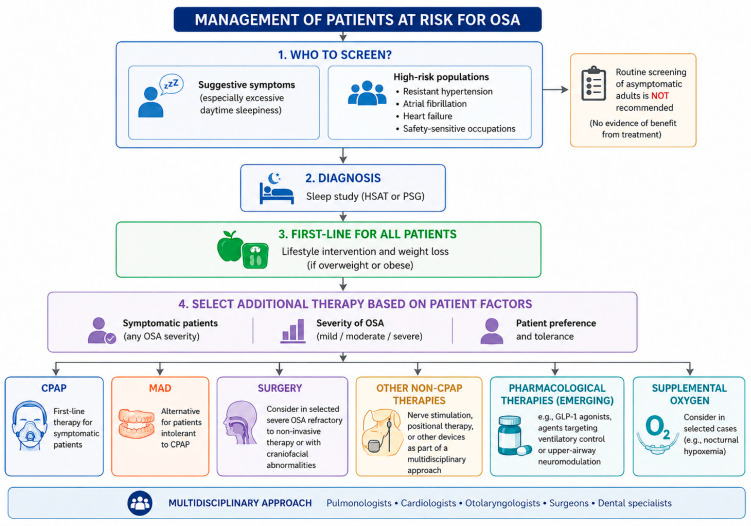
Routine screening of asymptomatic adults is not recommended by the U.S. Preventive Services Task Force or the American College of Physicians, given the lack of evidence that early detection and treatment in asymptomatic individuals improves clinical outcomes. Current recommendations support targeted screening in patients with suggestive symptoms, particularly excessive daytime sleepiness [ref. 257], and in selected high-risk populations, such as patients with resistant hypertension, AF, HF, or those working in safety-sensitive occupations [ref. 8,ref. 258]. However, the impact of screening for OSA on clinical outcomes is unclear, and no evidence currently supports treatment of asymptomatic patients with OSA for prognostic benefit [ref. 195].
Lifestyle intervention, especially weight loss in overweight or obese patients, is universally recommended across guidelines and should be considered first-line therapy irrespective of symptom burden. Beyond lifestyle measures, treatment selection is primarily guided by symptom severity, OSA burden, and patient preference [ref. 131,ref. 259,ref. 260]. In symptomatic patients, the American Heart Association and the American College of Cardiology recommend CPAP as first-line therapy, with MAD as an alternative for patients who are intolerant of CPAP [ref. 18,ref. 131]. Surgical options may be considered in selected cases of severe OSA refractory to non-invasive treatments or in patients with specific craniofacial abnormalities, although long-term cardiovascular outcome data remain limited, as highlighted by the American Academy of Sleep Medicine and the American Academy of Family Physicians [ref. 131,ref. 261]. Non-CPAP therapies are increasingly recognized as part of a multidisciplinary approach to OSA management. In this context, the European Respiratory Society emphasizes individualized treatment strategies involving pulmonologists, cardiologists, otolaryngologists, surgeons, and dental specialists [ref. 262]. Emerging therapeutic options, including pharmacological agents targeting obesity or ventilatory control and upper-airway neuromodulation techniques, offer promising alternatives but require further validation.
10. Conclusions
OSA is a common and often underdiagnosed condition with major cardiovascular implications. While treatment consistently improves symptoms and quality of life, evidence for cardiovascular event reduction remains heterogeneous and appears strongly influenced by patient selection and treatment adherence. Future research should focus on refining screening strategies, improving long-term adherence to therapy, and identifying subgroups of cardiovascular patients most likely to derive prognostic benefit from targeted OSA treatment.
References
- M.R. Cowie, D. Linz, S. Redline, V.K. Somers, A.K. Simonds. Sleep Disordered Breathing and Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol., 2021. [DOI | PubMed]
- R.B. Berry, R. Budhiraja, D.J. Gottlieb, D. Gozal, C. Iber, V.K. Kapur, C.L. Marcus, R. Mehra, S. Parthasarathy, S.F. Quan. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med., 2012. [DOI | PubMed]
- M. Emdin, G. Mirizzi, A. Giannoni, R. Poletti, G. Iudice, F. Bramanti, C. Passino. Prognostic Significance of Central Apneas Throughout a 24-Hour Period in Patients with Heart Failure. J. Am. Coll. Cardiol., 2017. [DOI | PubMed]
- A. Giannoni, C. Borrelli, F. Gentile, P. Sciarrone, J. Spießhöfer, M. Piepoli, G.B. Richerson, J.S. Floras, A.J. Coats, S. Javaheri. Autonomic and respiratory consequences of altered chemoreflex function: Clinical and therapeutic implications in cardiovascular diseases. Eur. J. Heart Fail., 2023. [DOI | PubMed]
- U. Corrà, A. Giordano, E. Bosimini, A. Mezzani, M. Piepoli, A.J. Coats, P. Giannuzzi. Oscillatory ventilation during exercise in patients with chronic heart failure: Clinical correlates and prognostic implications. Chest, 2002. [DOI | PubMed]
- P. Lévy, M. Kohler, W.T. McNicholas, F. Barbé, R.D. McEvoy, V.K. Somers, L. Lavie, J.L. Pépin. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Primers, 2015. [DOI | PubMed]
- R.S. Bucks, M. Olaithe, I. Rosenzweig, M.J. Morrell. Reviewing the relationship between OSA and cognition: Where do we go from here?. Respirology, 2017. [DOI | PubMed]
- D.J. Gottlieb, N.M. Punjabi. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA, 2020. [DOI | PubMed]
- M. Goyal, J. Johnson. Obstructive Sleep Apnea Diagnosis and Management. Mo. Med., 2017. [PubMed]
- A. Ogna, N. Tobback, D. Andries, M. Preisig, P. Vollenweider, G. Waeber, P. Marques-Vidal, J. Haba-Rubio, R. Heinzer. Prevalence and Clinical Significance of Respiratory Effort-Related Arousals in the General Population. J. Clin. Sleep Med., 2018. [DOI | PubMed]
- O. Oldenburg, B. Wellmann, A. Buchholz, T. Bitter, H. Fox, U. Thiem, D. Horstkotte, K. Wegscheider. Nocturnal hypoxaemia is associated with increased mortality in stable heart failure patients. Eur. Hear. J., 2015. [DOI | PubMed]
- P.E. Peppard, T. Young, J.H. Barnet, M. Palta, E.W. Hagen, K.M. Hla. Increased Prevalence of Sleep-Disordered Breathing in Adults. Am. J. Epidemiol., 2013. [DOI | PubMed]
- T. Young, M. Palta, J. Dempsey, P.E. Peppard, F.J. Nieto, K.M. Hla. Burden of sleep apnea: Rationale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ, 2009. [PubMed]
- S. Javaheri, F. Barbe, F. Campos-Rodriguez, J.A. Dempsey, R. Khayat, S. Javaheri, A. Malhotra, M.A. Martinez-Garcia, R. Mehra, A.I. Pack. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequences. J. Am. Coll. Cardiol., 2017. [DOI | PubMed]
- J. Brown, F. Yazdi, M. Jodari-Karimi, J.G. Owen, E. Reisin. Obstructive Sleep Apnea and Hypertension: Updates to a Critical Relationship. Curr. Hypertens. Rep., 2022. [DOI | PubMed]
- E.L. O’KEefe, J.E. Sturgess, J.H. O’KEefe, S. Gupta, C.J. Lavie. Prevention and Treatment of Atrial Fibrillation via Risk Factor Modification. Am. J. Cardiol., 2021. [DOI | PubMed]
- S. Javaheri, S. Javaheri, D. Gozal, F. Campos-Rodriguez, M.A. Martinez-Garcia, B. Mokhlesi, R. Mehra, W.T. McNicholas, V.K. Somers, P.C. Zee. Treatment of OSA and its Impact on Cardiovascular Disease, Part 2: JACC State-of-the-Art Review. J. Am. Coll. Cardiol., 2024. [DOI | PubMed]
- Y. Yeghiazarians, H. Jneid, J.R. Tietjens, S. Redline, D.L. Brown, N. El-Sherif, R. Mehra, B. Bozkurt, C.E. Ndumele, V.K. Somers. Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation, 2021. [DOI | PubMed]
- J.A. Dempsey, S.C. Veasey, B.J. Morgan, C.P. O’Donnell. Pathophysiology of Sleep Apnea. Physiol. Rev., 2010. [DOI | PubMed]
- N.L. Deacon, P.G. Catcheside. The role of high loop gain induced by intermittent hypoxia in the pathophysiology of obstructive sleep apnoea. Sleep Med. Rev., 2015. [DOI | PubMed]
- K.R. Burgess. New insights from the measurement of loop gain in obstructive sleep apnoea. J. Physiol., 2012. [DOI | PubMed]
- J.E. Orr, A. Malhotra, S.A. Sands. Pathogenesis of central and complex sleep apnoea. Respirology, 2017. [DOI | PubMed]
- P. Lévy, J.-L. Pépin, M. Dematteis. Pharyngeal neuropathy in obstructive sleep apnea: Where are we going?. Am. J. Respir. Crit. Care Med., 2012. [DOI | PubMed]
- S.D. Shapiro, C.-H. Chin, J.P. Kirkness, B.M. McGinley, S.P. Patil, V.Y. Polotsky, P.J.C. Biselli, P.L. Smith, H. Schneider, A.R. Schwartz. Leptin and the control of pharyngeal patency during sleep in severe obesity. J. Appl. Physiol., 2014. [DOI | PubMed]
- V.K. Somers, D.P. White, R. Amin, W.T. Abraham, F. Costa, A. Culebras, S. Daniels, J.S. Floras, C.E. Hunt, L.J. Olson. Sleep apnea and cardiovascular disease: An American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. J. Am. Coll. Cardiol., 2008. [PubMed]
- C. Cuspidi, M. Tadic, C. Sala, E. Gherbesi, G. Grassi, G. Mancia. Blood Pressure Non-Dipping and Obstructive Sleep Apnea Syndrome: A Meta-Analysis. J. Clin. Med., 2019. [DOI | PubMed]
- S. Jehan, F. Zizi, S.R. Pandi-Perumal, S.I. McFarlane, G. Jean-Louis, A.K. Myers. Obstructive sleep apnea, hypertension, resistant hypertension and cardiovascular disease. Sleep Med. Disord., 2020. [PubMed]
- H.H. Loh, Q.H. Lim, C.S. Chai, S.L. Goh, L.L. Lim, A. Yee, N. Sukor. Influence and implications of the renin–angiotensin–aldosterone system in obstructive sleep apnea: An updated systematic review and meta-analysis. J. Sleep Res., 2023. [DOI | PubMed]
- D. Yumino, S. Redolfi, P. Ruttanaumpawan, M.C. Su, S. Smith, G.E. Newton, S. Mak, T.D. Bradley. Nocturnal rostral fluid shift: A unifying concept for the pathogenesis of obstructive and central sleep apnea in men with heart failure. Circulation, 2010. [DOI | PubMed]
- L. Lavie. Oxidative stress in obstructive sleep apnea and intermittent hypoxia—Revisited—The bad ugly and good: Implications to the heart and brain. Sleep Med. Rev., 2015. [DOI | PubMed]
- A. Bikov, M. Kolossváry, A.L. Jermendy, Z.D. Drobni, A.D. Tarnoki, D.L. Tarnoki, B. Forgó, D.T. Kovacs, G. Losonczy, L. Kunos. Comprehensive coronary plaque assessment in patients with obstructive sleep apnea. J. Sleep Res., 2019. [DOI | PubMed]
- A.M. May, D.R. Van Wagoner, R. Mehra. OSA and Cardiac Arrhythmogenesis: Mechanistic Insights. Chest, 2017. [DOI | PubMed]
- A. Briançon-Marjollet, M. Weiszenstein, M. Henri, A. Thomas, D. Godin-Ribuot, J. Polak. The impact of sleep disorders on glucose metabolism: Endocrine and molecular mechanisms. Diabetol. Metab. Syndr., 2015. [DOI | PubMed]
- S. Reutrakul, B. Mokhlesi. Obstructive Sleep Apnea and Diabetes: A State of the Art Review. Chest, 2017. [DOI | PubMed]
- R.J. Davies, N.J. Ali, J.R. Stradling. Neck circumference and other clinical features in the diagnosis of the obstructive sleep apnoea syndrome. Thorax, 1992. [DOI | PubMed]
- C. Guilleminault, J.E. Black, L. Palombini, M. Ohayon. A clinical investigation of obstructive sleep apnea syndrome (OSAS) and upper airway resistance syndrome (UARS) patients. Sleep Med., 2000. [DOI | PubMed]
- E.S. Arnardottir, E. Bjornsdottir, K.A. Olafsdottir, B. Benediktsdottir, T. Gislason. Obstructive sleep apnoea in the general population: Highly prevalent but minimal symptoms. Eur. Respir. J., 2016. [DOI | PubMed]
- T. Young, E. Shahar, F.J. Nieto, S. Redline, A.B. Newman, D.J. Gottlieb, J.A. Walsleben, L. Finn, P. Enright, J.M. Samet. Predictors of sleep-disordered breathing in community-dwelling adults: The Sleep Heart Health Study. Arch. Intern. Med., 2002. [DOI | PubMed]
- T. Young, M. Palta, J. Dempsey, J. Skatrud, S. Weber, S. Badr. The Occurrence of Sleep-Disordered Breathing among Middle-Aged Adults. N. Engl. J. Med., 1993. [DOI | PubMed]
- M.W. Johns. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep, 1991. [DOI | PubMed]
- N.C. Netzer, R.A. Stoohs, C.M. Netzer, K. Clark, K.P. Strohl. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann. Intern. Med., 1999. [DOI | PubMed]
- F. Chung, B. Yegneswaran, P. Liao, S.A. Chung, S. Vairavanathan, S. Islam, A. Khajehdehi, C.M. Shapiro. STOP questionnaire: A tool to screen patients for obstructive sleep apnea. Anesthesiology, 2008. [DOI | PubMed]
- V.K. Kapur, D.H. Auckley, S. Chowdhuri, D.C. Kuhlmann, R. Mehra, K. Ramar, C.G. Harrod. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med., 2017. [DOI | PubMed]
- M. El Shayeb, L.-A. Topfer, T. Stafinski, L. Pawluk, D. Menon. Diagnostic accuracy of level 3 portable sleep tests versus level 1 polysomnography for sleep-disordered breathing: A systematic review and meta-analysis. Can. Med. Assoc. J., 2013. [DOI | PubMed]
- R.L. Riha, M. Celmina, B. Cooper, R. Hamutcu-Ersu, A. Kaditis, A. Morley, A. Pataka, T. Penzel, L. Roberti, W. Ruehland. ERS technical standards for using type III devices (limited channel studies) in the diagnosis of sleep disordered breathing in adults and children. Eur. Respir. J., 2022. [DOI]
- R. Poletti, A. Aimo, V. Castiglione, A. Di Gangi, G. Iudice, M. Micalizzi, C. Passino, M. Emdin. Diagnostic Tools: The Easier, the Better. The Breathless Heart: Apneas in Heart Failure, 2017
- A. Osa-Sanchez, J. Ramos-Martinez-De-Soria, A. Mendez-Zorrilla, I.O. Ruiz, B. Garcia-Zapirain. Wearable Sensors and Artificial Intelligence for Sleep Apnea Detection: A Systematic Review. J. Med. Syst., 2025. [DOI | PubMed]
- R. Shirahama, T. Tanigawa, Y. Ida, K. Fukuhisa, R. Tanaka, K. Tomooka, F.-Y. Lan, A. Ikeda, H. Wada, S.N. Kales. Long-term effect of continuous positive airway pressure therapy on blood pressure in patients with obstructive sleep apnea. Sci. Rep., 2021. [DOI | PubMed]
- D.S. Silverberg, A. Oksenberg, A. Iaina. Sleep-related breathing disorders as a major cause of essential hypertension: Fact or fiction?. Curr. Opin. Nephrol. Hypertens., 1998. [DOI | PubMed]
- P.E. Peppard, T. Young, M. Palta, J. Skatrud. Prospective study of the association between sleep-disordered breathing and hypertension. N. Engl. J. Med., 2000. [DOI | PubMed]
- R. Tamisier, J. Pépin, J. Rémy, J. Baguet, J. Taylor, J. Weiss, P. Lévy. 14 nights of intermittent hypoxia elevate daytime blood pressure and sympathetic activity in healthy humans. Eur. Respir. J., 2011. [DOI | PubMed]
- H. Hou, Y. Zhao, W. Yu, H. Dong, X. Xue, J. Ding, W. Xing, W. Wang. Association of obstructive sleep apnea with hypertension: A systematic review and meta-analysis. J. Glob. Health, 2018. [DOI | PubMed]
- D.A. Johnson, S.J. Thomas, M. Abdalla, N. Guo, Y. Yano, M. Rueschman, R.M. Tanner, M.A. Mittleman, D.A. Calhoun, J.G. Wilson. Association Between Sleep Apnea and Blood Pressure Control Among Blacks. Circulation, 2019. [DOI | PubMed]
- B. Lechat, K.A. Loffler, A.C. Reynolds, G. Naik, A. Vakulin, G. Jennings, P. Escourrou, R.D. McEvoy, R.J. Adams, P.G. Catcheside. High night-to-night variability in sleep apnea severity is associated with uncontrolled hypertension. npj Digit. Med., 2023. [DOI | PubMed]
- S.J. Crinion, S. Ryan, J. Kleinerova, B.D. Kent, J. Gallagher, M. Ledwidge, K. McDonald, W.T. McNicholas. Nondipping Nocturnal Blood Pressure Predicts Sleep Apnea in Patients with Hypertension. J. Clin. Sleep Med., 2019. [DOI | PubMed]
- D.C. Genta-Pereira, S.F. Furlan, D.Q. Omote, D.M. Giorgi, L.A. Bortolotto, G. Lorenzi-Filho, L.F. Drager. Nondipping Blood Pressure Patterns Predict Obstructive Sleep Apnea in Patients Undergoing Ambulatory Blood Pressure Monitoring. Hypertension, 2018. [DOI | PubMed]
- B. Mokhlesi, E.W. Hagen, L.A. Finn, K.M. Hla, J.R. Carter, P.E. Peppard. Obstructive sleep apnoea during REM sleep and incident non-dipping of nocturnal blood pressure: A longitudinal analysis of the Wisconsin Sleep Cohort. Thorax, 2015. [DOI | PubMed]
- A.R. Rishi, M.A. Rishi. Rapid eye movement related obstructive sleep apnea: Where do we stand?. Respir. Investig., 2021. [DOI | PubMed]
- F. Barbé, J. Durán-Cantolla, M. Sánchez-de-la-Torre, M. Martínez-Alonso, C. Carmona, A. Barceló, E. Chiner, J.F. Masa, M. Gonzalez, J.M. Marín. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: A randomized controlled trial. JAMA, 2012. [DOI | PubMed]
- J.M. Marin, A. Agusti, I. Villar, M. Forner, D. Nieto, S.J. Carrizo, F. Barbé, E. Vicente, Y. Wei, F.J. Nieto. Association between treated and untreated obstructive sleep apnea and risk of hypertension. JAMA, 2012. [DOI | PubMed]
- J.M. Marin, S.J. Carrizo, E. Vicente, A.G. Agusti. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet, 2005. [DOI | PubMed]
- Y.-C. Lin, C.-T. Chen, P.-Z. Chao, P.-Y. Chen, W.-T. Liu, S.-T. Tsao, S.-F. Lin, C.-H. Bai. Prevention of Incident Hypertension in Patients with Obstructive Sleep Apnea Treated with Uvulopalatopharyngoplasty or Continuous Positive Airway Pressure: A Cohort Study. Front. Surg., 2022. [DOI | PubMed]
- L. Liu, Q. Cao, Z. Guo, Q. Dai. Continuous Positive Airway Pressure in Patients with Obstructive Sleep Apnea and Resistant Hypertension: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Hypertens., 2016. [DOI]
- I.H. Iftikhar, C.W. Valentine, L.R. Bittencourt, D.L. Cohen, A.C. Fedson, T. Gíslason, T. Penzel, C.L. Phillips, L. Yu-Sheng, A.I. Pack. Effects of continuous positive airway pressure on blood pressure in patients with resistant hypertension and obstructive sleep apnea: A meta-analysis. J. Hypertens., 2014. [DOI | PubMed]
- W. Shang, Y. Zhang, L. Liu, F. Chen, G. Wang, D. Han. Benefits of continuous positive airway pressure on blood pressure in patients with hypertension and obstructive sleep apnea: A meta-analysis. Hypertens. Res., 2022. [DOI | PubMed]
- A.V. Benjafield, J.-L. Pepin, P.A. Cistulli, A. Wimms, F. Lavergne, F.H.S. Kuniyoshi, S.H. Munson, B. Schuler, S.R. Badikol, K.C. Wolfe. Positive airway pressure therapy and all-cause and cardiovascular mortality in people with obstructive sleep apnoea: A systematic review and meta-analysis of randomised controlled trials and confounder-adjusted, non-randomised controlled studies. Lancet Respir. Med., 2025. [DOI | PubMed]
- M.F. Pengo, E.I. Schwarz, F. Barbé, P.A. Cistulli, L.F. Drager, C. Fava, F.D. Fuchs, M.S. Ip, K.A. Loffler, M.M. Lui. Effect of CPAP therapy on blood pressure in patients with obstructive sleep apnoea: A worldwide individual patient data meta-analysis. Eur. Respir. J., 2024. [DOI]
- F.N. Jilwan, P. Escourrou, G. Garcia, X. Jaïs, M. Humbert, G. Roisman. High occurrence of hypoxemic sleep respiratory disorders in precapillary pulmonary hypertension and mechanisms. Chest, 2013. [DOI | PubMed]
- A. Chaouat, E. Weitzenblum, J. Krieger, M. Oswald, R. Kessler. Pulmonary hemodynamics in the obstructive sleep apnea syndrome. Results in 220 consecutive patients. Chest, 1996. [DOI | PubMed]
- C. Kholdani, W.H. Fares, V. Mohsenin. Pulmonary hypertension in obstructive sleep apnea: Is it clinically significant? A critical analysis of the association and pathophysiology. Pulm. Circ., 2015. [DOI | PubMed]
- M.M. Lowery, N.S. Hill, L. Wang, E.B. Rosenzweig, A. Bhat, S. Erzurum, J.E. Finet, C.L. Jellis, S. Kaur, D.H. Kwon. Sleep-Related Hypoxia, Right Ventricular Dysfunction, and Survival in Patients with Group 1 Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol., 2023. [DOI | PubMed]
- O.A. Minai, B. Ricaurte, R. Kaw, J. Hammel, M. Mansour, K. McCarthy, J.A. Golish, J.K. Stoller. Frequency and impact of pulmonary hypertension in patients with obstructive sleep apnea syndrome. Am. J. Cardiol., 2009. [DOI | PubMed]
- S.B. Montesi, B.A. Edwards, A. Malhotra, J.P. Bakker. The effect of continuous positive airway pressure treatment on blood pressure: A systematic review and meta-analysis of randomized controlled trials. J. Clin. Sleep Med., 2012. [DOI | PubMed]
- D. Sorajja, A.S. Gami, V.K. Somers, T.R. Behrenbeck, A. Garcia-Touchard, F. Lopez-Jimenez. Independent association between obstructive sleep apnea and subclinical coronary artery disease. Chest, 2008. [DOI | PubMed]
- B.U. Peres, A.J.H. Allen, P. Daniele, K.H. Humphries, C. Taylor, I. Laher, F. Almeida, R. Jen, A.J. Sandford, S.F. van Eeden. Circulating levels of cell adhesion molecules and risk of cardiovascular events in obstructive sleep apnea. PLoS ONE, 2021. [DOI | PubMed]
- T. Konishi, Y. Kashiwagi, N. Funayama, T. Yamamoto, H. Murakami, D. Hotta, S. Tanaka. Obstructive sleep apnea is associated with increased coronary plaque instability: An optical frequency domain imaging study. Heart Vessel., 2019. [DOI | PubMed]
- N.A. Shah, H.K. Yaggi, J. Concato, V. Mohsenin. Obstructive sleep apnea as a risk factor for coronary events or cardiovascular death. Sleep Breath., 2010. [DOI | PubMed]
- C.-H. Lee, S.-M. Khoo, M.Y. Chan, H.-B. Wong, A.F. Low, Q.-H. Phua, A.M. Richards, H.-C. Tan, T.-C. Yeo. Severe obstructive sleep apnea and outcomes following myocardial infarction. J. Clin. Sleep Med., 2011. [DOI | PubMed]
- F. Sadabadi, S. Darroudi, H. Esmaily, Z. Asadi, G.A. Ferns, A.H. Mohammadpour, A.H. Nooriyan, M. Ghayour-Mobarhan, M. Moohebati. The importance of sleep patterns in the incidence of coronary heart disease: A 6-year prospective study in Mashhad, Iran. Sci. Rep., 2023. [DOI | PubMed]
- F.H.S. Kuniyoshi, A. Garcia-Touchard, A.S. Gami, A. Romero-Corral, C. van der Walt, S. Pusalavidyasagar, T. Kara, S.M. Caples, G.S. Pressman, E.C. Vasquez. Day-night variation of acute myocardial infarction in obstructive sleep apnea. J. Am. Coll. Cardiol., 2008. [DOI | PubMed]
- D. Linz, R.D. McEvoy, M.R. Cowie, V.K. Somers, S. Nattel, P. Lévy, J.M. Kalman, P. Sanders. Associations of Obstructive Sleep Apnea with Atrial Fibrillation and Continuous Positive Airway Pressure Treatment: A Review. JAMA Cardiol., 2018. [DOI | PubMed]
- A. Deshmukh, N. Covassin, Y. Dauvilliers, V.K. Somers. Sleep Disruption and Atrial Fibrillation: Evidence, Mechanisms and Clinical Implications. Circ. Res., 2025. [DOI | PubMed]
- K. Monahan, A. Storfer-Isser, R. Mehra, E. Shahar, M. Mittleman, J. Rottman, N. Punjabi, M. Sanders, S.F. Quan, H. Resnick. Triggering of nocturnal arrhythmias by sleep-disordered breathing events. J. Am. Coll. Cardiol., 2009. [DOI | PubMed]
- R. Mehra, E.J. Benjamin, E. Shahar, D.J. Gottlieb, R. Nawabit, H.L. Kirchner, J. Sahadevan, S. Redline. Association of nocturnal arrhythmias with sleep-disordered breathing: The Sleep Heart Health Study. Am. J. Respir. Crit. Care Med., 2006. [DOI | PubMed]
- N. Patel, C. Donahue, A. Shenoy, A. Patel, N. El-Sherif. Obstructive sleep apnea and arrhythmia: A systemic review. Int. J. Cardiol., 2017. [DOI | PubMed]
- D. Linz, A.G. Brooks, A.D. Elliott, J.M. Kalman, R.D. McEvoy, D.H. Lau, P. Sanders. Nightly Variation in Sleep Apnea Severity as Atrial Fibrillation Risk. J. Am. Coll. Cardiol., 2018. [DOI | PubMed]
- K. Monahan, J. Brewster, L. Wang, B. Parvez, S. Goyal, D.M. Roden, D. Darbar. Relation of the severity of obstructive sleep apnea in response to anti-arrhythmic drugs in patients with atrial fibrillation or atrial flutter. Am. J. Cardiol., 2012. [DOI | PubMed]
- D.M. Yaranov, A. Smyrlis, N. Usatii, A. Butler, J.R. Petrini, J. Mendez, M.K. Warshofsky. Effect of obstructive sleep apnea on frequency of stroke in patients with atrial fibrillation. Am. J. Cardiol., 2015. [DOI | PubMed]
- L. Li, Z.-W. Wang, J. Li, X. Ge, L.-Z. Guo, Y. Wang, W.-H. Guo, C.-X. Jiang, C.-S. Ma. Efficacy of catheter ablation of atrial fibrillation in patients with obstructive sleep apnoea with and without continuous positive airway pressure treatment: A meta-analysis of observational studies. Europace, 2014. [DOI | PubMed]
- I.H. Stevenson, H. Teichtahl, D. Cunnington, S. Ciavarella, I. Gordon, J.M. Kalman. Prevalence of sleep disordered breathing in paroxysmal and persistent atrial fibrillation patients with normal left ventricular function. Eur. Heart J., 2008. [DOI | PubMed]
- R. Kanagala, N.S. Murali, P.A. Friedman, N.M. Ammash, B.J. Gersh, K.V. Ballman, A.S. Shamsuzzaman, V.K. Somers. Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation, 2003. [DOI | PubMed]
- A.S. Fein, A. Shvilkin, D. Shah, C.I. Haffajee, S. Das, K. Kumar, D.B. Kramer, P.J. Zimetbaum, A.E. Buxton, M.E. Josephson. Treatment of obstructive sleep apnea reduces the risk of atrial fibrillation recurrence after catheter ablation. J. Am. Coll. Cardiol., 2013. [DOI | PubMed]
- Y. Naruse, H. Tada, M. Satoh, M. Yanagihara, H. Tsuneoka, Y. Hirata, Y. Ito, K. Kuroki, T. Machino, H. Yamasaki. Concomitant obstructive sleep apnea increases the recurrence of atrial fibrillation following radiofrequency catheter ablation of atrial fibrillation: Clinical impact of continuous positive airway pressure therapy. Heart Rhythm, 2013. [DOI | PubMed]
- V. Condoleo, G. Severini, G. Armentaro, M. Francica, G. Crudo, M. De Marco, F. Maruca, G. Ciaccio, C. Fuoco, C.A. Pastura. Effect of continuous positive airway pressure on non-fatal stroke and paroxysmal atrial fibrillation recurrence in obstructive sleep apnoea elderly patients. Eur. J. Intern. Med., 2024. [DOI | PubMed]
- H.S. Abed, G.A. Wittert, D.P. Leong, M.G. Shirazi, B. Bahrami, M.E. Middeldorp, M.F. Lorimer, D.H. Lau, N.A. Antic, A.G. Brooks. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: A randomized clinical trial. JAMA, 2013. [DOI | PubMed]
- S. Jamaly, L. Carlsson, M. Peltonen, P. Jacobson, L. Sjöström, K. Karason. Bariatric Surgery and the Risk of New-Onset Atrial Fibrillation in Swedish Obese Subjects. J. Am. Coll. Cardiol., 2016. [DOI | PubMed]
- R.D. McEvoy, N.A. Antic, E. Heeley, Y. Luo, Q. Ou, X. Zhang, O. Mediano, R. Chen, L.F. Drager, Z. Liu. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N. Engl. J. Med., 2016. [DOI | PubMed]
- E.N. Simantirakis, S.I. Schiza, M.E. Marketou, S.I. Chrysostomakis, G.I. Chlouverakis, N.C. Klapsinos, N.S. Siafakas, P.E. Vardas. Severe bradyarrhythmias in patients with sleep apnoea: The effect of continuous positive airway pressure treatment: A long-term evaluation using an insertable loop recorder. Eur. Heart J., 2004. [DOI | PubMed]
- R. Mehra, M.K. Chung, B. Olshansky, D. Dobrev, C.L. Jackson, V. Kundel, D. Linz, N.S. Redeker, S. Redline, P. Sanders. Sleep-Disordered Breathing and Cardiac Arrhythmias in Adults: Mechanistic Insights and Clinical Implications: A Scientific Statement From the American Heart Association. Circulation, 2022. [DOI | PubMed]
- S. Garrigue, J.L. Pépin, P. Defaye, F. Murgatroyd, Y. Poezevara, J. Clémenty, P. Lévy. High prevalence of sleep apnea syndrome in patients with long-term pacing: The European Multicenter Polysomnographic Study. Circulation, 2007. [DOI | PubMed]
- F.M. Kusumoto, M.H. Schoenfeld, C. Barrett, J.R. Edgerton, K.A. Ellenbogen, M.R. Gold, N.F. Goldschlager, R.M. Hamilton, J.A. Joglar, R.J. Kim. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation, 2019. [DOI | PubMed]
- A.S. Gami, E.J. Olson, W.K. Shen, R.S. Wright, K.V. Ballman, D.O. Hodge, R.M. Herges, D.E. Howard, V.K. Somers. Obstructive sleep apnea and the risk of sudden cardiac death: A longitudinal study of 10,701 adults. J. Am. Coll. Cardiol., 2013. [DOI | PubMed]
- D. Linz, A. Denner, S. Illing, M. Hohl, C. Ukena, F. Mahfoud, S. Ewen, J.C. Reil, K. Wirth, M. Böhm. Impact of obstructive and central apneas on ventricular repolarisation: Lessons learned from studies in man and pigs. Clin. Res. Cardiol., 2016. [DOI | PubMed]
- A. Salama, A. Abdullah, A. Wahab, G. Eigbire, R. Hoefen, R. Kouides, N. Ritter, H. Mieszczanska, R. Alweis. Is obstructive sleep apnea associated with ventricular tachycardia? A retrospective study from the National Inpatient Sample and a literature review on the pathogenesis of Obstructive Sleep Apnea. Clin. Cardiol., 2018. [DOI | PubMed]
- A. Gami, D. Howard, E. Olson, V. Somers. Day-night pattern of sudden death in obstructive sleep apnea. ACC Curr. J. Rev., 2005. [DOI]
- T. Menon, I. Ogbu, D.K. Kalra. Sleep-Disordered Breathing and Cardiac Arrhythmias. J. Clin. Med., 2024. [DOI | PubMed]
- L.H. White, T.D. Bradley. Role of nocturnal rostral fluid shift in the pathogenesis of obstructive and central sleep apnoea. J. Physiol., 2013. [DOI | PubMed]
- O. Oldenburg, B. Lamp, L. Faber, H. Teschler, D. Horstkotte, V. Töpfer. Sleep-disordered breathing in patients with symptomatic heart failure: A contemporary study of prevalence in and characteristics of 700 patients. Eur. J. Hear. Fail., 2007. [DOI]
- J.R. Tietjens, D. Claman, E.J. Kezirian, T. De Marco, A. Mirzayan, B. Sadroonri, A.N. Goldberg, C. Long, E.P. Gerstenfeld, Y. Yeghiazarians. Obstructive Sleep Apnea in Cardiovascular Disease: A Review of the Literature and Proposed Multidisciplinary Clinical Management Strategy. J. Am. Heart Assoc., 2019. [DOI | PubMed]
- M. Hunasikatti. Predictors of Obstructive Sleep Apnea on Home Sleep Apnea Test After a Negative Attended Polysomnography: Not So Fast. J. Clin. Sleep Med., 2019. [DOI | PubMed]
- T. Bitter, N. Westerheide, C. Prinz, M.S. Hossain, J. Vogt, C. Langer, D. Horstkotte, O. Oldenburg. Cheyne-Stokes respiration and obstructive sleep apnoea are independent risk factors for malignant ventricular arrhythmias requiring appropriate cardioverter-defibrillator therapies in patients with congestive heart failure. Eur. Heart J., 2010. [DOI | PubMed]
- C. Borrelli, F. Gentile, P. Sciarrone, G. Mirizzi, G. Vergaro, N. Ghionzoli, F. Bramanti, G. Iudice, C. Passino, M. Emdin. Central and Obstructive Apneas in Heart Failure with Reduced, Mid-Range and Preserved Ejection Fraction. Front. Cardiovasc. Med., 2019. [DOI | PubMed]
- F. Gentile, N. Ghionzoli, C. Borrelli, G. Vergaro, M.C. Pastore, M. Cameli, M. Emdin, C. Passino, A. Giannoni. Epidemiological and clinical boundaries of heart failure with preserved ejection fraction. Eur. J. Prev. Cardiol., 2021. [DOI]
- R. Khayat, D. Jarjoura, K. Porter, A. Sow, J. Wannemacher, R. Dohar, A. Pleister, W.T. Abraham. Sleep disordered breathing and post-discharge mortality in patients with acute heart failure. Eur. Heart J., 2015. [DOI | PubMed]
- P.A. Cistulli, A. Malhotra, K.V. Cole, A.S. Malik, J. Pépin, F.H.S. Kuniyoshi, A.V. Benjafield, V.K. Somers, K.L. Sterling, C.M. Nunez. Positive Airway Pressure Therapy Adherence and Health Care Resource Use in Patients with Obstructive Sleep Apnea and Heart Failure with Preserved Ejection Fraction. J. Am. Heart Assoc., 2023. [DOI | PubMed]
- A. Malhotra, K.V. Cole, A.S. Malik, J.L. Pépin, F.H. Sert Kuniyoshi, P.A. Cistulli, A.V. Benjafield, V.K. Somers. Positive Airway Pressure Adherence and Health Care Resource Utilization in Patients with Obstructive Sleep Apnea and Heart Failure with Reduced Ejection Fraction. J. Am. Heart Assoc., 2023. [DOI | PubMed]
- C.M. Ryan, K. Usui, J.S. Floras, T.D. Bradley. Effect of continuous positive airway pressure on ventricular ectopy in heart failure patients with obstructive sleep apnoea. Thorax, 2005. [DOI | PubMed]
- M.A. Arias, F. García-Río, A. Alonso-Fernández, O. Mediano, I. Martínez, J. Villamor. Obstructive sleep apnea syndrome affects left ventricular diastolic function: Effects of nasal continuous positive airway pressure in men. Circulation, 2005. [DOI | PubMed]
- F. Piccirillo, S.P. Crispino, L. Buzzelli, A. Segreti, R.A. Incalzi, F. Grigioni. A State-of-the-Art Review on Sleep Apnea Syndrome and Heart Failure. Am. J. Cardiol., 2023. [DOI | PubMed]
- T.D. Bradley, A.G. Logan, G.L. Filho, R.J. Kimoff, J.D. Cantolla, M. Arzt, S. Redolfi, G. Parati, T. Kasai, M.E. Dunlap. Adaptive servo-ventilation for sleep-disordered breathing in patients with heart failure with reduced ejection fraction (ADVENT-HF): A multicentre, multinational, parallel-group, open-label, phase 3 randomised controlled trial. Lancet Respir. Med., 2024. [DOI | PubMed]
- M.R. Cowie, H. Woehrle, K. Wegscheider, C. Angermann, M.-P. D’ortho, E. Erdmann, P. Levy, A.K. Simonds, V.K. Somers, F. Zannad. Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure. N. Engl. J. Med., 2015. [DOI | PubMed]
- C.M. O’cOnnor, D.J. Whellan, M. Fiuzat, N.M. Punjabi, G. Tasissa, K.J. Anstrom, A.V. Benjafield, H. Woehrle, A.B. Blase, J. Lindenfeld. Cardiovascular Outcomes with Minute Ventilation-Targeted Adaptive Servo-Ventilation Therapy in Heart Failure: The CAT-HF Trial. J. Am. Coll. Cardiol., 2017. [DOI | PubMed]
- J. Yeboah, S. Redline, C. Johnson, R. Tracy, P. Ouyang, R.S. Blumenthal, G.L. Burke, D.M. Herrington. Association between sleep apnea, snoring, incident cardiovascular events and all-cause mortality in an adult population: MESA. Atherosclerosis, 2011. [DOI | PubMed]
- T. Young, L. Finn, P.E. Peppard, M. Szklo-Coxe, D. Austin, F.J. Nieto, R. Stubbs, K.M. Hla. Sleep disordered breathing and mortality: Eighteen-year follow-up of the Wisconsin sleep cohort. Sleep, 2008. [DOI | PubMed]
- F. Campos-Rodriguez, M.A. Martinez-Garcia, N. Reyes-Nuñez, I. Caballero-Martinez, P. Catalan-Serra, C.V. Almeida-Gonzalez. Role of sleep apnea and continuous positive airway pressure therapy in the incidence of stroke or coronary heart disease in women. Am. J. Respir. Crit. Care Med., 2014. [DOI | PubMed]
- C. Xie, R. Zhu, Y. Tian, K. Wang. Association of obstructive sleep apnoea with the risk of vascular outcomes and all-cause mortality: A meta-analysis. BMJ Open, 2017. [DOI]
- G.Q. Roca, S. Redline, B. Claggett, N. Bello, C.M. Ballantyne, S.D. Solomon, A.M. Shah. Sex-Specific Association of Sleep Apnea Severity with Subclinical Myocardial Injury, Ventricular Hypertrophy, and Heart Failure Risk in a Community-Dwelling Cohort: The Atherosclerosis Risk in Communities-Sleep Heart Health Study. Circulation, 2015. [DOI | PubMed]
- G. Iannella, G. Magliulo, C.A.M.L. Iacono, G. Bianchi, A. Polimeni, A. Greco, A. De Vito, G. Meccariello, G. Cammaroto, R. Gobbi. Positional Obstructive Sleep Apnea Syndrome in Elderly Patients. Int. J. Environ. Res. Public Health, 2020. [DOI | PubMed]
- P.R. Srijithesh, R. Aghoram, A. Goel, J. Dhanya. Positional therapy for obstructive sleep apnoea. Cochrane Database Syst. Rev., 2019. [DOI | PubMed]
- T. Young, P.E. Peppard, S. Taheri. Excess weight and sleep-disordered breathing. J. Appl. Physiol., 1985. [DOI | PubMed]
- A. Qaseem, J.E. Holty, D.K. Owens, P. Dallas, M. Starkey, P. Shekelle. Clinical Guidelines Committee of the American College of Physicians. Management of obstructive sleep apnea in adults: A clinical practice guideline from the American College of Physicians. Ann. Intern. Med., 2013. [DOI | PubMed]
- A. Sharafkhaneh, A. Thomas, C. Ulmer, C. Fung, J.L. Martin, M. Colandrea, M.A. Fuller, T. Thomas, M. Brock, V. Capaldi. VA/DoD Clinical Practice Guideline for the Management of Chronic Insomnia Disorder and Obstructive Sleep Apnea, 2025
- K.D. Aiello, W.G. Caughey, B. Nelluri, A. Sharma, F. Mookadam, M. Mookadam. Effect of exercise training on sleep apnea: A systematic review and meta-analysis. Respir. Med., 2016. [DOI | PubMed]
- M.H. Araghi, Y.-F. Chen, A. Jagielski, S. Choudhury, D. Banerjee, S. Hussain, G.N. Thomas, S. Taheri. Effectiveness of lifestyle interventions on obstructive sleep apnea (OSA): Systematic review and meta-analysis. Sleep, 2013. [DOI | PubMed]
- I.H. Iftikhar, L. Bittencourt, S.D. Youngstedt, N. Ayas, P. Cistulli, R. Schwab, M.W. Durkin, U.J. Magalang. Comparative efficacy of CPAP, MADs, exercise-training, and dietary weight loss for sleep apnea: A network meta-analysis. Sleep Med., 2017. [DOI | PubMed]
- L.J. Mitchell, Z.E. Davidson, M. Bonham, D.M. O’Driscoll, G.S. Hamilton, H. Truby. Weight loss from lifestyle interventions and severity of sleep apnoea: A systematic review and meta-analysis. Sleep Med., 2014. [DOI | PubMed]
- W.L. Ng, C.E. Stevenson, E. Wong, S. Tanamas, T. Boelsen-Robinson, J.E. Shaw, M.T. Naughton, J. Dixon, A. Peeters. Does intentional weight loss improve daytime sleepiness? A systematic review and meta-analysis. Obes. Rev., 2017. [DOI | PubMed]
- M.-A. Thomasouli, E.M. Brady, M.J. Davies, A.P. Hall, K. Khunti, D.H. Morris, L.J. Gray. The impact of diet and lifestyle management strategies for obstructive sleep apnoea in adults: A systematic review and meta-analysis of randomised controlled trials. Sleep Breath., 2013. [DOI | PubMed]
- A. Carneiro-Barrera, A. Díaz-Román, A. Guillén-Riquelme, G. Buela-Casal. Weight loss and lifestyle interventions for obstructive sleep apnoea in adults: Systematic review and meta-analysis. Obes. Rev., 2019. [DOI | PubMed]
- E. Burgess, P. Hassmén, M. Welvaert, K. Pumpa. Behavioural treatment strategies improve adherence to lifestyle intervention programmes in adults with obesity: A systematic review and meta-analysis. Clin. Obes., 2017. [DOI | PubMed]
- G.D. Foster, K.E. Borradaile, M.H. Sanders, R. Millman, G. Zammit, A.B. Newman, T.A. Wadden, D. Kelley, R.R. Wing, F.X. Pi-Sunyer. Sleep AHEAD Research Group of Look AHEAD Research Group. A randomized study on the effect of weight loss on obstructive sleep apnea among obese patients with type 2 diabetes: The Sleep AHEAD study. Arch. Intern. Med., 2009. [DOI | PubMed]
- J.A. Chirinos, I. Gurubhagavatula, K. Teff, D.J. Rader, T.A. Wadden, R. Townsend, G.D. Foster, G. Maislin, H. Saif, P. Broderick. CPAP, Weight Loss, or Both for Obstructive Sleep Apnea. N. Engl. J. Med., 2014. [DOI | PubMed]
- S.T. Kuna, D.M. Reboussin, K.E. Borradaile, M.H. Sanders, R.P. Millman, G. Zammit, A.B. Newman, T.A. Wadden, J.M. Jakicic, R.R. Wing. Long-term effect of weight loss on obstructive sleep apnea severity in obese patients with type 2 diabetes. Sleep, 2013. [DOI | PubMed]
- H. Tuomilehto, H. Gylling, M. Peltonen, T. Martikainen, J. Sahlman, J. Kokkarinen, J. Randell, H. Tukiainen, E. Vanninen, M. Partinen. Sustained improvement in mild obstructive sleep apnea after a diet- and physical activity-based lifestyle intervention: Postinterventional follow-up. Am. J. Clin. Nutr., 2010. [DOI | PubMed]
- K. Johansson, E. Hemmingsson, R. Harlid, Y.T. Lagerros, F. Granath, S. Rössner, M. Neovius. Longer term effects of very low energy diet on obstructive sleep apnoea in cohort derived from randomised controlled trial: Prospective observational follow-up study. BMJ, 2011. [DOI | PubMed]
- S. Aggarwal, P. Priyadarshini, V.P. Singh, H. Garg, S. Sinha, R. Guleria. Impact of bariatric surgery on obstructive sleep apnoea-hypopnea syndrome in morbidly obese patients. J. Minimal Access Surg., 2017. [DOI]
- P. Nastałek, K. Polok, N. Celejewska-Wójcik, A. Kania, K. Sładek, P. Małczak, P. Major. Impact of bariatric surgery on obstructive sleep apnea severity and continuous positive airway pressure therapy compliance-prospective observational study. Sci. Rep., 2021. [DOI | PubMed]
- H. Qin, Y. Wang, X. Chen, N. Steenbergen, T. Penzel, X. Zhang, R. Li. The efficacy of bariatric surgery on pulmonary function and sleep architecture of patients with obstructive sleep apnea and co-morbid obesity: A systematic review and meta-analysis. Surg. Obes. Relat. Dis., 2023. [DOI | PubMed]
- Y. Zhang, W. Wang, C. Yang, J. Shen, M. Shi, B. Wang. Improvement in Nocturnal Hypoxemia in Obese Patients with Obstructive Sleep Apnea after Bariatric Surgery: A Meta-Analysis. Obes. Surg., 2019. [DOI | PubMed]
- K. Al Oweidat, A.A. Toubasi, R.B. Abu Tawileh, H.B. Abu Tawileh, M.M. Hasuneh. Bariatric surgery and obstructive sleep apnea: A systematic review and meta-analysis. Sleep Breath., 2023. [DOI | PubMed]
- C. Puech, J. Thereaux, F. Couturaud, C. Leroyer, C. Tromeur, C. Gut-Gobert, C. Orione, R. Le Mao, C. L’hÉvéder. Evolution of treated obstructive sleep apneas syndrome after bariatric surgery: An observational retrospective study. Surg. Obes. Relat. Dis., 2025. [DOI | PubMed]
- Y. Liu, L. Yang, M.J. Stampfer, S. Redline, S.S. Tworoger, T. Huang. Physical activity, sedentary behaviour and incidence of obstructive sleep apnoea in three prospective US cohorts. Eur. Respir. J., 2022. [DOI | PubMed]
- O. Lins-Filho, J.L.P. Aguiar, J.R.V. de Almeida, A.H. Soares, R. Ritti-Dias, M.J. da Silva, R.P. Pedrosa. Effect of exercise training on body composition in patients with obstructive sleep apnea: A systematic review and meta-analysis. Sleep Med., 2021. [DOI | PubMed]
- I.H. Iftikhar, C.E. Kline, S.D. Youngstedt. Effects of Exercise Training on Sleep Apnea: A Meta-analysis. Lung, 2014. [DOI | PubMed]
- J. Peng, Y. Yuan, Y. Zhao, H. Ren. Effects of Exercise on Patients with Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health, 2022. [DOI | PubMed]
- C.-F. Lin, N.-H. Ho, W.-L. Hsu, C.-H. Lin, Y.-H. Wang, Y.-P. Wang. Effects of aerobic exercise and resistance training on obstructive sleep apnea: A systematic review and meta-analysis. J. Clin. Sleep Med., 2024. [DOI | PubMed]
- C. Justribó-Manion, E.A. Sánchez-Romero, J.-N. Cuenca-Zaldivar, A. Cerdà-Ribó, N. Felipe-Spada, J. Tomàs-Aliberas, J. Padrós-Augé. Active conservative interventions for obstructive sleep apnea: An umbrella review and meta-meta-analysis of systematic reviews. Sleep Med., 2025. [DOI | PubMed]
- D.M. Servantes, S. Javaheri, A.C.P. Kravchychyn, L.J. Storti, D.R. Almeida, M.T. de Mello, F.D. Cintra, S. Tufik, L. Bittencourt. Effects of Exercise Training and CPAP in Patients with Heart Failure and OSA: A Preliminary Study. Chest, 2018. [DOI | PubMed]
- L.M. Revuelta, J. Flores-Fraile, Á. Zubizarreta-Macho, J.M. Montiel-Company, A.B. Lobo-Galindo, P.A. Blanco. Relationship Between Obstructive Sleep Apnea and Sports-Systematic Review and Meta-Analysis. J. Clin. Med., 2024. [DOI | PubMed]
- M. Camacho, V. Certal, J. Abdullatif, S. Zaghi, C.M. Ruoff, R. Capasso, C.A. Kushida. Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep, 2015. [DOI | PubMed]
- R. Tang, J. Pan, Y. Huang, X. Ren. Efficacy comparison of aerobic exercise, combined exercise, oropharyngeal exercise and respiratory muscle training for obstructive sleep apnea: A systematic review and network meta-analysis. Sleep Med., 2024. [DOI | PubMed]
- Z. Zheng, Y. Zong, Y. Ma, Y. Tian, Y. Pang, C. Zhang, J. Gao. Glucagon-like peptide-1 receptor: Mechanisms and advances in therapy. Signal Transduct. Target. Ther., 2024. [DOI | PubMed]
- K. Heinla, E. Vasar, I. Reppo, T. Sedman, V. Volke. GLP-1 Receptor Agonists Induce Growth Hormone Secretion in Healthy Volunteers. Diabetes Ther., 2023. [DOI | PubMed]
- C.R. Andreasen, A. Andersen, F.K. Knop, T. Vilsbøll. How glucagon-like peptide 1 receptor agonists work. Endocr. Connect., 2021. [DOI | PubMed]
- J.P.H. Wilding, R.L. Batterham, S. Calanna, M. Davies, L.F. Van Gaal, I. Lingvay, B.M. McGowan, J. Rosenstock, M.T. Tran, T.A. Wadden. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med., 2021. [DOI | PubMed]
- J.P. Frías, M.J. Davies, J. Rosenstock, F.C. Pérez Manghi, L. Fernández Landó, B.K. Bergman, B. Liu, X. Cui, K. Brown. SURPASS-2 Investigators. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N. Engl. J. Med., 2021. [DOI | PubMed]
- A.M. Jastreboff, L.J. Aronne, A. Stefanski. Tirzepatide Once Weekly for the Treatment of Obesity. Reply. N. Engl. J. Med., 2022. [DOI | PubMed]
- A. Blackman, G.D. Foster, G. Zammit, R. Rosenberg, L. Aronne, T. Wadden, B. Claudius, C.B. Jensen, E. Mignot. Effect of liraglutide 3.0 mg in individuals with obesity and moderate or severe obstructive sleep apnea: The SCALE Sleep Apnea randomized clinical trial. Int. J. Obes., 2016. [DOI | PubMed]
- S.R. Patel. Entering a New Era in Sleep-Apnea Treatment. N. Engl. J. Med., 2024. [DOI | PubMed]
- A. Malhotra, R.R. Grunstein, I. Fietze, T.E. Weaver, S. Redline, A. Azarbarzin, S.A. Sands, R.J. Schwab, J.P. Dunn, S. Chakladar. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity. N. Engl. J. Med., 2024. [DOI | PubMed]
- C. O’dOnnell, S. Crilly, A. O’mAhony, B. O’rIordan, M. Traynor, R. Gitau, K. McDonald, M. Ledwidge, D. O’sHea, D.J. Murphy. Continuous Positive Airway Pressure but Not GLP1-mediated Weight Loss Improves Early Cardiovascular Disease in Obstructive Sleep Apnea: A Randomized Proof-of-Concept Study. Ann. Am. Thorac. Soc., 2024. [DOI | PubMed]
- W. Jiang, W. Li, J. Cheng, W. Li, F. Cheng. Efficacy and safety of liraglutide in patients with type 2 diabetes mellitus and severe obstructive sleep apnea. Sleep Breath., 2023. [DOI | PubMed]
- K.M. Liu, H. Yuan, D. Wang, Q. Yuan, X. Shi. Effects of liraglutide on sleep-disordered breathing and diabetic microangiopathy in patients with type 2 diabetes mellitus and obstructive sleep apnea-hypopnea syndrome. Chin. J. Diabetes Mellit., 2020
- R.S. Amin, N. Simakajornboon, R.V. Szczesniak. Treatment of obstructive sleep apnea with glucagon like peptide-1 receptor agonist. Am. J. Respir. Crit. Care Med., 2015
- M. Li, H. Lin, Q. Yang, X. Zhang, Q. Zhou, J. Shi, F. Ge. Glucagon-like peptide-1 receptor agonists for the treatment of obstructive sleep apnea: A meta-analysis. Sleep, 2024. [DOI]
- C.S. Kow, D.S. Ramachandram, S.S. Hasan, K. Thiruchelvam. Efficacy and safety of GLP-1 receptor agonists in the management of obstructive sleep apnea in individuals without diabetes: A systematic review and meta-analysis of randomized, placebo-controlled trials. Sleep Med., 2025. [DOI | PubMed]
- D.J. Drucker. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab., 2018. [DOI | PubMed]
- B. Mokhlesi, L.A. Finn, E.W. Hagen, T. Young, K.M. Hla, E. Van Cauter, P.E. Peppard. Obstructive sleep apnea during REM sleep and hypertension. results of the Wisconsin Sleep Cohort. Am. J. Respir. Crit. Care Med., 2014. [DOI | PubMed]
- J.P. Bakker, R. Wang, J. Weng, M.S. Aloia, C. Toth, M.G. Morrical, K.J. Gleason, M. Rueschman, C. Dorsey, S.R. Patel. Motivational Enhancement for Increasing Adherence to CPAP: A Randomized Controlled Trial. Chest, 2016. [DOI | PubMed]
- S.P. Patil, I.A. Ayappa, S.M. Caples, R.J. Kimoff, S.R. Patel, C.G. Harrod. Treatment of Adult Obstructive Sleep Apnea with Positive Airway Pressure: An American Academy of Sleep Medicine Systematic Review, Meta-Analysis, and GRADE Assessment. J. Clin. Sleep Med., 2019. [DOI | PubMed]
- Z. Huang, Z. Liu, Q. Luo, Q. Zhao, Z. Zhao, X. Ma, W. Liu, D. Yang. Long-term effects of continuous positive airway pressure on blood pressure and prognosis in hypertensive patients with coronary heart disease and obstructive sleep apnea: A randomized controlled trial. Am. J. Hypertens., 2015. [DOI | PubMed]
- D.R. Mansfield, N.C. Gollogly, D.M. Kaye, M. Richardson, P. Bergin, M.T. Naughton. Controlled trial of continuous positive airway pressure in obstructive sleep apnea and heart failure. Am. J. Respir. Crit. Care Med., 2004. [DOI | PubMed]
- J. Colish, J.R. Walker, N. Elmayergi, S. Almutairi, F. Alharbi, M. Lytwyn, A. Francis, S. Bohonis, M. Zeglinski, I.D.C. Kirkpatrick. Obstructive sleep apnea: Effects of continuous positive airway pressure on cardiac remodeling as assessed by cardiac biomarkers, echocardiography, and cardiac MRI. Chest, 2012. [DOI | PubMed]
- T. Damy, L. Margarit, A. Noroc, D. Bodez, S. Guendouz, L. Boyer, X. Drouot, A. Lamine, A. Paulino, S. Rappeneau. Prognostic impact of sleep-disordered breathing and its treatment with nocturnal ventilation for chronic heart failure. Eur. J. Heart Fail., 2012. [DOI | PubMed]
- S. Javaheri, E. Ben Caref, E. Chen, K.B. Tong, W.T. Abraham. Sleep apnea testing and outcomes in a large cohort of Medicare beneficiaries with newly diagnosed heart failure. Am. J. Respir. Crit. Care Med., 2011. [DOI | PubMed]
- T. Kasai, K. Narui, T. Dohi, N. Yanagisawa, S. Ishiwata, M. Ohno, T. Yamaguchi, S.-I. Momomura. Prognosis of patients with heart failure and obstructive sleep apnea treated with continuous positive airway pressure. Chest, 2008. [DOI | PubMed]
- Y. Peker, H. Glantz, C. Eulenburg, K. Wegscheider, J. Herlitz, E. Thunström. Effect of Positive Airway Pressure on Cardiovascular Outcomes in Coronary Artery Disease Patients with Nonsleepy Obstructive Sleep Apnea. The RICCADSA Randomized Controlled Trial. Am. J. Respir. Crit. Care Med., 2016. [DOI | PubMed]
- M. Sánchez-De-La-Torre, A. Sánchez-De-La-Torre, S. Bertran, J. Abad, J. Duran-Cantolla, V. Cabriada, O. Mediano, M.J. Masdeu, M.L. Alonso, J.F. Masa. Effect of obstructive sleep apnoea and its treatment with continuous positive airway pressure on the prevalence of cardiovascular events in patients with acute coronary syndrome (ISAACC study): A randomised controlled trial. Lancet Respir. Med., 2020. [DOI | PubMed]
- F.d.S. Paulitsch, L. Zhang. Continuous positive airway pressure for adults with obstructive sleep apnea and cardiovascular disease: A meta-analysis of randomized trials. Sleep Med., 2019. [DOI | PubMed]
- D. Yang, L. Li, J. Dong, W. Yang, Z. Liu. Effects of continuous positive airway pressure on cardiac events and metabolic components in patients with moderate to severe obstructive sleep apnea and coronary artery disease: A meta-analysis. J. Clin. Sleep Med., 2023. [DOI | PubMed]
- M. Sánchez-de-la-Torre, E. Gracia-Lavedan, I.D. Benitez, A. Sánchez-de-la-Torre, A. Moncusí-Moix, G. Torres, K. Loffler, R. Woodman, R. Adams, G. Labarca. Adherence to CPAP Treatment and the Risk of Recurrent Cardiovascular Events: A Meta-Analysis. JAMA, 2023. [DOI | PubMed]
- S. Batool-Anwar, J.L. Goodwin, C.A. Kushida, J.A. Walsh, R.D. Simon, D.A. Nichols, S.F. Quan. Impact of continuous positive airway pressure (CPAP) on quality of life in patients with obstructive sleep apnea (OSA). J. Sleep Res., 2016. [DOI | PubMed]
- A.J. Wimms, J.L. Kelly, C.D. Turnbull, A. McMillan, S.E. Craig, J.F. O’Reilly, A.H. Nickol, E.L. Hedley, M.D. Decker, L.A. Willes. Continuous positive airway pressure versus standard care for the treatment of people with mild obstructive sleep apnoea (MERGE): A multicentre, randomised controlled trial. Lancet Respir. Med., 2019. [DOI | PubMed]
- V. Timkova, I. Nagyova, S.A. Reijneveld, R. Tkacova, J.P. van Dijk, U. Bültmann. Quality of life of obstructive sleep apnoea patients receiving continuous positive airway pressure treatment: A systematic review and meta-analysis. Heart Lung, 2020. [DOI | PubMed]
- C. Feltner, I.F. Wallace, S. Aymes, J. Cook Middleton, K.L. Hicks, M. Schwimmer, C. Baker, C.P. Balio, D. Moore, C.E. Voisin. Screening for Obstructive Sleep Apnea in Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA, 2022. [DOI | PubMed]
- F. Soltaninejad, R. Golastaneh, P.I. Ghahfarokhi, M. Salmasi, B. Amra. Continuous positive airway pressure treatment for sleep apnea in elderly patients systematic review and meta-analysis. Sleep Breath., 2025. [DOI | PubMed]
- S. Tregear, J. Reston, K. Schoelles, B. Phillips. Continuous positive airway pressure reduces risk of motor vehicle crash among drivers with obstructive sleep apnea: Systematic review and meta-analysis. Sleep, 2010. [DOI | PubMed]
- A.V. Benjafield, J.L.D. Pépin, K. Valentine, P.A. Cistulli, H. Woehrle, C.M. Nunez, J. Armitstead, A. Malhotra. Compliance after switching from CPAP to bilevel for patients with non-compliant OSA: Big data analysis. BMJ Open Respir. Res., 2019. [DOI]
- C. Guilleminault, P. Philip, A. Robinson. Sleep and neuromuscular disease: Bilevel positive airway pressure by nasal mask as a treatment for sleep disordered breathing in patients with neuromuscular disease. J. Neurol. Neurosurg. Psychiatry, 1998. [DOI | PubMed]
- K. Ramar, L.C. Dort, S.G. Katz, C.J. Lettieri, C.G. Harrod, S.M. Thomas, R.D. Chervin. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J. Dent. Sleep Med., 2015. [DOI]
- D.J. Bratton, T. Gaisl, A.M. Wons, M. Kohler. CPAP vs Mandibular Advancement Devices and Blood Pressure in Patients with Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. JAMA, 2015. [DOI | PubMed]
- M.P. Mansukhani, E.J. Olson, S.M. Caples. Upper Airway Surgery for Obstructive Sleep Apnea. JAMA, 2020. [DOI | PubMed]
- N. Browaldh, P. Nerfeldt, M. Lysdahl, J. Bring, D. Friberg. SKUP3 randomised controlled trial: Polysomnographic results after uvulopalatopharyngoplasty in selected patients with obstructive sleep apnoea. Thorax, 2013. [DOI | PubMed]
- J.U. Sommer, C. Heiser, C. Gahleitner, R.M. Herr, K. Hörmann, J.T. Maurer, B.A. Stuck. Tonsillectomy with Uvulopalatopharyngoplasty in Obstructive Sleep Apnea. Dtsch. Ärzteblatt Int., 2016. [DOI | PubMed]
- A. De Vito, B.T. Woodson, V. Koka, G. Cammaroto, G. Iannella, M. Bosi, S. Pelucchi, G.R. Filograna-Pignatelli, P. El Chater, C. Vicini. OSA Upper Airways Surgery: A Targeted Approach. Medicina, 2021. [DOI | PubMed]
- S. Zaghi, J.E.C. Holty, V. Certal, J. Abdullatif, C. Guilleminault, N.B. Powell, M. Camacho. Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea: A Meta-analysis. JAMA Otolaryngol. Head Neck Surg., 2016. [DOI | PubMed]
- K. Li, J.-E. Holey, C. Guilleminault. Maxillomandibular Advancement for OSA: A 25-year perspective. L’Orthod. Fr., 2022. [DOI]
- M.D. Olson, M.R. Junna. Hypoglossal Nerve Stimulation Therapy for the Treatment of Obstructive Sleep Apnea. Neurotherapeutics, 2021. [DOI | PubMed]
- P.J. Strollo, R.J. Soose, J.T. Maurer, N. de Vries, J. Cornelius, O. Froymovich, R.D. Hanson, T.A. Padhya, D.L. Steward, M.B. Gillespie. Upper-airway stimulation for obstructive sleep apnea. N. Engl. J. Med., 2014. [DOI | PubMed]
- B.T. Woodson, K.P. Strohl, R.J. Soose, M.B. Gillespie, J.T. Maurer, N. de Vries, T.A. Padhya, M.S. Badr, H. Lin, O.M. Vanderveken. Upper Airway Stimulation for Obstructive Sleep Apnea: 5-Year Outcomes. Otolaryngol. Head Neck Surg., 2018. [DOI | PubMed]
- P.R. Eastwood, M. Barnes, S.G. MacKay, J.R. Wheatley, D.R. Hillman, X.-L. Nguyên, R. Lewis, M.C. Campbell, B. Pételle, J.H. Walsh. Bilateral hypoglossal nerve stimulation for treatment of adult obstructive sleep apnoea. Eur. Respir. J., 2019. [DOI]
- B. He, M. Al-Sherif, M. Nido, R. Tas, M. Beach, E.I. Schwarz, M. Cheng, A. Ishak, K. Lee, N. Shah. Domiciliary use of transcutaneous electrical stimulation for patients with obstructive sleep apnoea: A conceptual framework for the TESLA home programme. J. Thorac. Dis., 2019. [DOI | PubMed]
- B.T. Woodson, D.T. Kent, C. Huntley, M.K. Hancock, D.J. Van Daele, M.S. Boon, T.C. Huntley, S. Mickelson, M.B. Gillespie, M.V. Suurna. Bilateral hypoglossal nerve stimulation for obstructive sleep apnea: A nonrandomized clinical trial. J. Clin. Sleep Med., 2025. [DOI | PubMed]
- C. Heiser, A. Steffen, P.J. Strollo, C. Giaie-Miniet, O.M. Vanderveken, B. Hofauer. Hypoglossal nerve stimulation versus positive airway pressure therapy for obstructive sleep apnea. Sleep Breath., 2023. [DOI | PubMed]
- S. Luu, D.E.C.Y. Chan, N.S. Marshall, C.L. Phillips, R.R. Grunstein, B.J. Yee. Pharmacotherapy for obstructive sleep apnea: A critical review of randomized placebo-controlled trials. Sleep Med. Rev., 2025. [DOI | PubMed]
- R. Lim, J.C. Carberry, A. Wellman, R. Grunstein, D.J. Eckert. Reboxetine and hyoscine butylbromide improve upper airway function during nonrapid eye movement and suppress rapid eye movement sleep in healthy individuals. Sleep, 2018. [DOI]
- E. Perger, L. Taranto Montemurro, D. Rosa, S. Vicini, M. Marconi, L. Zanotti, P. Meriggi, A. Azarbarzin, S.A. Sands, A. Wellman. Reboxetine Plus Oxybutynin for OSA Treatment: A 1-Week, Randomized, Placebo-Controlled, Double-Blind Crossover Trial. Chest, 2022. [DOI | PubMed]
- L. Taranto-Montemurro, L. Messineo, S.A. Sands, A. Azarbarzin, M. Marques, B.A. Edwards, D.J. Eckert, D.P. White, A. Wellman. The Combination of Atomoxetine and Oxybutynin Greatly Reduces Obstructive Sleep Apnea Severity. A Randomized, Placebo-controlled, Double-Blind Crossover Trial. Am. J. Respir. Crit. Care Med., 2019. [DOI | PubMed]
- R. Rosenberg, B. Abaluck, S. Thein. Combination of atomoxetine with the novel antimuscarinic aroxybutynin improves mild to moderate OSA. J. Clin. Sleep Med., 2022. [DOI | PubMed]
- P.K. Schweitzer, L. Taranto-Montemurro, J.M. Ojile, S.G. Thein, C.L. Drake, R. Rosenberg, B. Corser, B. Abaluck, R.B. Sangal, J. Maynard. The Combination of Aroxybutynin and Atomoxetine in the Treatment of Obstructive Sleep Apnea (MARIPOSA): A Randomized Controlled Trial. Am. J. Respir. Crit. Care Med., 2023. [DOI | PubMed]
- P.K. Schweitzer, J.P. Maynard, P.E. Wylie, H.A. Emsellem, S.A. Sands. Efficacy of atomoxetine plus oxybutynin in the treatment of obstructive sleep apnea with moderate pharyngeal collapsibility. Sleep Breath., 2023. [DOI | PubMed]
- L. Taranto-Montemurro, S.R. Patel, P.J. Strollo, J. Cronin, J. Yee, H. Pho, A. Werner, R. Farkas. Aroxybutynin and atomoxetine (AD109) for the treatment of obstructive sleep apnea: Rationale, design and baseline characteristics of the phase 3 clinical trials. Contemp. Clin. Trials Commun., 2025. [DOI | PubMed]
- P. Strollo, J. Cronin, H. Pho, L. Taranto-Montemurro, R. Farkas. 0783 Demographic and Baseline Disease Characteristics of SynAIRgy: A Phase 3 Trial of Aroxybutynin and Atomoxetine (AD109) in Obstructive Sleep Apnea. Sleep, 2025. [DOI]
- Apnimed Reports Positive Topline Results from Second Phase 3 Trial of AD109, Reinforcing Potential of First Oral Pill for Obstructive Sleep Apnea
- S. Patel, R. Farkas, L. Taranto, J.W. Cronin, P.J. Strollo. The LUNAIR-O trial: A 51-week phase 3, randomized, double-blind, placebo-controlled study of aroxybutynin and atomoxetine (AD109) in obstructive sleep apnea. Chest, 2025. [DOI]
- P.J. Strollo, R. Farkas, L. Taranto, J.W. Cronin, S. Patel. The SYNAIRGY trial: A 26-week phase 3, randomized, double-blind, placebo-controlled study of aroxybutynin and atomoxetine (AD109) in obstructive sleep apnea. Chest, 2025. [DOI]
- L.G. Brownell, P. West, P. Sweatman, J.C. Acres, M.H. Kryger. Protriptyline in obstructive sleep apnea: A double-blind trial. N. Engl. J. Med., 1982. [DOI | PubMed]
- P.L. Smith, E.F. Haponik, R.P. Allen, E.R. Bleecker. The effects of protriptyline in sleep-disordered breathing. Am. Rev. Respir. Dis., 1983. [DOI | PubMed]
- L. Taranto-Montemurro, S.A. Sands, B.A. Edwards, A. Azarbarzin, M. Marques, C. de Melo, D.J. Eckert, D.P. White, A. Wellman. Desipramine improves upper airway collapsibility and reduces OSA severity in patients with minimal muscle compensation. Eur. Respir. J., 2016. [DOI | PubMed]
- M.R. AbdelFattah, S.W. Jung, M.A. Greenspan, M. Padilla, R. Enciso. Efficacy of Antidepressants in the Treatment of Obstructive Sleep Apnea Compared to Placebo. A Systematic Review with Meta-Analyses. Sleep Breath., 2019. [DOI | PubMed]
- T. Gaisl, S.R. Haile, S. Thiel, M. Osswald, M. Kohler. Efficacy of pharmacotherapy for OSA in adults: A systematic review and network meta-analysis. Sleep Med. Rev., 2019. [DOI | PubMed]
- W. Randerath, J. de Lange, J. Hedner, J.P.T. Ho, M. Marklund, S. Schiza, J. Steier, J. Verbraecken. Current and novel treatment options for obstructive sleep apnoea. ERJ Open Res., 2022. [DOI | PubMed]
- D.P. White. Pharmacologic Approaches to the Treatment of Obstructive Sleep Apnea. Sleep Med. Clin., 2016. [DOI | PubMed]
- N.S. Marshall, B.J. Yee, A.V. Desai, P.R. Buchanan, K.K. Wong, R. Crompton, K.L. Melehan, N. Zack, S.G. Rao, R.M. Gendreau. Two randomized placebo-controlled trials to evaluate the efficacy and tolerability of mirtazapine for the treatment of obstructive sleep apnea. Sleep, 2008. [DOI | PubMed]
- T. Wang, D. Eskandari, D. Zou, L. Grote, J. Hedner. Increased Carbonic Anhydrase Activity is Associated with Sleep Apnea Severity and Related Hypoxemia. Sleep, 2015. [DOI | PubMed]
- M.C.K. Khoo. Using loop gain to assess ventilatory control in obstructive sleep apnea. Am. J. Respir. Crit. Care Med., 2001. [DOI | PubMed]
- Y.-N. Ni, H. Yang, R.J. Thomas. The role of acetazolamide in sleep apnea at sea level: A systematic review and meta-analysis. J. Clin. Sleep Med., 2021. [DOI | PubMed]
- J. Hedner, K. Stenlöf, D. Zou, E. Hoff, C. Hansen, K. Kuhn, P. Lennartz, L. Grote. A Randomized Controlled Clinical Trial Exploring Safety and Tolerability of Sulthiame in Sleep Apnea. Am. J. Respir. Crit. Care Med., 2022. [DOI | PubMed]
- D. Eskandari, D. Zou, M. Karimi, K. Stenlöf, L. Grote, J. Hedner. Zonisamide reduces obstructive sleep apnoea: A randomised placebo-controlled study. Eur. Respir. J., 2014. [DOI | PubMed]
- S.L. Phyu, S. Ercan, E. Harriss, C. Turnbull. Nocturnal oxygen therapy in obstructive sleep apnoea: A systematic review and meta-analysis. Eur. Respir. Rev., 2024. [DOI | PubMed]
- B. Ruan, M. Nagappa, M. Rashid-Kolvear, K. Zhang, R. Waseem, M. Englesakis, F. Chung. The effectiveness of supplemental oxygen and high-flow nasal cannula therapy in patients with obstructive sleep apnea in different clinical settings: A systematic review and meta-analysis. J. Clin. Anesth., 2023. [DOI | PubMed]
- S.G. Carter, M.S. Berger, J.C. Carberry, L.E. Bilston, J.E. Butler, B.K. Tong, R.T. Martins, L.P. Fisher, D.K. McKenzie, R.R. Grunstein. Zopiclone Increases the Arousal Threshold without Impairing Genioglossus Activity in Obstructive Sleep Apnea. Sleep, 2016. [DOI | PubMed]
- D. Wang, N.S. Marshall, J. Duffin, B.J. Yee, K.K. Wong, N. Noori, S.S.W. Ng, R.R. Grunstein. Phenotyping interindividual variability in obstructive sleep apnoea response to temazepam using ventilatory chemoreflexes during wakefulness. J. Sleep Res., 2011. [DOI | PubMed]
- R. Rosenberg, J.M. Roach, M. Scharf, D.A. Amato. A pilot study evaluating acute use of eszopiclone in patients with mild to moderate obstructive sleep apnea syndrome. Sleep Med., 2007. [DOI | PubMed]
- D.J. Eckert, R.L. Owens, G.B. Kehlmann, A. Wellman, S. Rahangdale, S. Yim-Yeh, D.P. White, A. Malhotra. Eszopiclone increases the respiratory arousal threshold and lowers the apnoea/hypopnoea index in obstructive sleep apnoea patients with a low arousal threshold. Clin. Sci., 2011. [DOI]
- D.W. Carley, B. Prasad, K.J. Reid, R. Malkani, H. Attarian, S.M. Abbott, B. Vern, H. Xie, C. Yuan, P.C. Zee. Pharmacotherapy of Apnea by Cannabimimetic Enhancement, the PACE Clinical Trial: Effects of Dronabinol in Obstructive Sleep Apnea. Sleep, 2017. [DOI]
- P.M. Boylan, M. Santibañez, J. Thomas, E. Weeda, Z.R. Noel, J. Caballero. Cannabinoids for obstructive sleep apnea: A systematic review. Pharmacotherapy, 2024. [DOI | PubMed]
- K. Ramar, I.M. Rosen, D.B. Kirsch, R.D. Chervin, K.A. Carden, R.N. Aurora, D.A. Kristo, R.K. Malhotra, J.L. Martin, E.J. Olson. Medical Cannabis and the Treatment of Obstructive Sleep Apnea: An American Academy of Sleep Medicine Position Statement. J. Clin. Sleep Med., 2018. [DOI | PubMed]
- A.B. Avellar, L.B. Carvalho, G.F. Prado, L.B. Prado. Pharmacotherapy for residual excessive sleepiness and cognition in CPAP-treated patients with obstructive sleep apnea syndrome: A systematic review and meta-analysis. Sleep Med. Rev., 2016. [DOI | PubMed]
- S. Kaplan, E.L. Goehring, S. Melamed-Gal, B. Nguyen-Khoa, H. Knebel, J.K. Jones. Modafinil and the risk of cardiovascular events: Findings from three US claims databases. Pharmacoepidemiol. Drug Saf., 2018. [DOI | PubMed]
- J.L. Chapman, E.A. Cayanan, C.M. Hoyos, Y. Serinel, M. Comas, B.J. Yee, K.K.H. Wong, R.R. Grunstein, N.S. Marshall. Does Armodafinil Improve Driving Task Performance and Weight Loss in Sleep Apnea? A Randomized Trial. Am. J. Respir. Crit. Care Med., 2018. [DOI | PubMed]
- J.L. Pépin, O. Georgiev, R. Tiholov, V. Attali, J. Verbraecken, B. Buyse, M. Partinen, I. Fietze, G. Belev, D. Dokic. Pitolisant for Residual Excessive Daytime Sleepiness in OSA Patients Adhering to CPAP: A Randomized Trial. Chest, 2021. [DOI | PubMed]
- P.K. Schweitzer, R. Rosenberg, G.K. Zammit, M. Gotfried, D. Chen, L.P. Carter, H. Wang, Y. Lu, J. Black, A. Malhotra. Solriamfetol for Excessive Sleepiness in Obstructive Sleep Apnea (TONES 3). A Randomized Controlled Trial. Am. J. Respir. Crit. Care Med., 2019. [DOI | PubMed]
- P. Tanayapong, V. Tantrakul, S. Liamsombut, S. Siriyotha, G. McKay, J. Attia, A. Thakkinstian. Comparative Efficacy and Safety of Multiple Wake-Promoting Agents for the Treatment of Residual Sleepiness in Obstructive Sleep Apnea Despite Continuous Positive Airway Pressure: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. CNS Drugs, 2025. [DOI | PubMed]
- T. Pitre, J. Mah, S. Roberts, K. Desai, Y. Gu, C. Ryan, J.W. Busse, D. Zeraatkar. Comparative Efficacy and Safety of Wakefulness-Promoting Agents for Excessive Daytime Sleepiness in Patients with Obstructive Sleep Apnea: A Systematic Review and Network Meta-analysis. Ann. Intern. Med., 2023. [DOI | PubMed]
- J.L. Pépin, P. Lehert, R. Ben Messaoud, M. Joyeux-Faure, C. Caussé, J. Asin, F. Barbé, M.R. Bonsignore, W. Randerath, J. Verbraecken. Comparative efficacy, safety and benefit/risk of alerting agents for excessive daytime sleepiness in patients with obstructive sleep apnoea: A network meta-analysis. eClinicalMedicine, 2024. [DOI | PubMed]
- C.M. Mangione, M.J. Barry, W.K. Nicholson, M. Cabana, D. Chelmow, T. Rucker Coker, K.W. Davidson, E.M. Davis, K.E. Donahue. Screening for Obstructive Sleep Apnea in Adults: US Preventive Services Task Force Recommendation Statement. JAMA, 2022. [PubMed]
- G. Hindricks, T. Potpara, N. Dagres, E. Arbelo, J.J. Bax, C. Blomström-Lundqvist, G. Boriani, M. Castella, G.A. Dan, P.E. Dilaveris. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J., 2021. [PubMed]
- D.W. Jones, K.C. Ferdinand, S.J. Taler, H.M. Johnson, D. Shimbo, M. Abdalla, M.M. Altieri, N. Bansal, N.A. Bello, A.P. Bress. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol., 2025. [PubMed]
- D.W. Hudgel, S.R. Patel, A.M. Ahasic, S.J. Bartlett, D.H. Bessesen, M.A. Coaker, P.M. Fiander, R.R. Grunstein, I. Gurubhagavatula, V.K. Kapur. The Role of Weight Management in the Treatment of Adult Obstructive Sleep Apnea. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med., 2018. [DOI | PubMed]
- J.L. Creamer, S.K. Arora, M.R. Rusting. Surgical Treatments for Obstructive Sleep Apnea: Updated Guidelines From the American Academy of Sleep Medicine. Am. Fam. Physician, 2022. [PubMed]
- W. Randerath, J. Verbraecken, C.A. de Raaff, J. Hedner, S. Herkenrath, W. Hohenhorst, T. Jakob, O. Marrone, M. Marklund, W.T. McNicholas. European Respiratory Society guideline on non-CPAP therapies for obstructive sleep apnoea. Eur. Respir. Rev., 2021. [DOI | PubMed]