
Exploring the Influence of Recreational Cannabis Legalization on Women’s Perceptions and Experiences with Perinatal Cannabis Use: A Qualitative Meta-synthesis
Abstract
Objective:
We aimed to explore how women living in places with legalized recreational cannabis perceive perinatal cannabis use, and how legalization potentially impacts their experiences.
Methods:
Between September 2024 and December 2025, we searched databases including PubMed, CINAHL, Scopus, PsycINFO, and Web of Science. All research reports were screened and evaluated based on the inclusion and exclusion criteria. Theory-generating qualitative meta-synthesis methodology was used to extract, analyze, and synthesize the findings from included qualitative research reports. Quality appraisal of each study was also conducted.
Results:
Nineteen qualitative research reports were included, and eight themes were identified. Themes included (1) recreational cannabis legalization, (2) clinical policies and practice, (3) stigma and discrimination, (4) access to and desire for information, (5) clinician-patient relationships, (6) most trusted sources: family and friends, (7) perceptions and experiences and (8) self-management.
Conclusion:
This qualitative meta-synthesis highlights the complex interplay of public policy, institutional and community, interpersonal, and intrapersonal factors influencing women’s perceptions of and experiences with perinatal cannabis use, as well as provides valuable insight into the decision-making process. These implications can help inform targeted public health and clinical practice interventions to address the complexities of cannabis use during the perinatal period.
Article type: Review Article
Keywords: Cannabis, Pregnancy, Breastfeeding, Public policy, Qualitative review
Affiliations: https://ror.org/02ymw8z06grid.134936.a0000 0001 2162 3504Sinclair School of Nursing, University of Missouri, Columbia, MO USA
License: © The Author(s) 2026 CC BY 4.0 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Article links: DOI: 10.1007/s10995-026-04228-5 | PubMed: 41741881 | PMC: PMC12999839
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (1.4 MB)
Cannabis Legalization
Nine countries have legalized recreational cannabis use nationwide, while laws in the United States (US) and Australia vary by state or jurisdiction (Venditti, ref. 2024). In the US, 24 states, two territories, and the District of Columbia have legalized recreational cannabis for adult use (DISA Global Solutions, ref. 2025). Cannabis legalization benefits include justice decriminalization, drug product regulation, and taxation, yet the safety and health-related impacts on vulnerable populations are poorly understood. As recreational cannabis legalization expands and patterns of maternal cannabis use are documented globally, it is critical to understand the implications for pregnant and parenting women.
Perinatal Cannabis Use
Perinatal cannabis use is defined as use before, during, or after pregnancy, including during breastfeeding (The American College of Obstetricians and Gynecologists [ACOG], ref. 2017). According to the most recent data on cannabis use during pregnancy by the Substance Abuse and Mental Health Services Administration (ref. 2022), 8% (n = 164,000) of US pregnant women aged 15 to 44 years reported past month cannabis use in 2020. Prior research has shown that the prevalence of cannabis use during pregnancy is highest among Black, low-income, unmarried, and younger women (Ko et al., ref. 2015, ref. 2020). Although relatively weak associations between maternal cannabis use and adverse infant health outcomes have been estimated, in-utero cannabis exposure has been linked to infant low birth weight (LBW), premature delivery, small for gestational age, and longer neonatal intensive care admissions (Lo et al., ref. 2024). Additionally, recent studies demonstrate an increased risk for attention-deficit/hyperactivity disorder (ADHD) and poor brain neurodevelopment (Bassalov et al., ref. 2024; Paul et al., ref. 2021). While cannabis use during breastfeeding is significantly understudied, two studies found exclusively breastfed infants ingest about 2.5% of the maternal tetrahydrocannabinol (THC) dose used, which may be higher with chronic use and increases in potency (Baker et al., ref. 2018; Bertrand et al., ref. 2018).
Cannabis use among women who are considering pregnancy, pregnant, or breastfeeding is discouraged (Office of the Surgeon General, ref. 2019; ACOG, ref. 2017). Despite these recommendations, pregnant and parenting women continue to use cannabis for its perceived symptom management benefits and misconceptions about legality and safety. Studies have shown that cannabis use during pregnancy frequently occurs in the first trimester for self-management of nausea and vomiting, pain, stress, anxiety, and depression (Vanstone et al., ref. 2022). Limited research suggests that cannabis use during pregnancy is associated with several adverse maternal health outcomes including increased risk for gestational hypertension, preeclampsia, weight issues, and placental abruption (Young-Wolff et al., ref. 2024a).
Research Aims
Understanding the multi-level factors that influence women’s use of cannabis during the perinatal period can provide valuable information to improve public health interventions and clinical practices. The question guiding our qualitative meta-synthesis was: What do women living in a place with legalized recreational cannabis think about perinatal cannabis use, and how does legalization impact their experiences with perinatal cannabis use?
Methods
Design
Theory-generating qualitative meta-synthesis (QMS) methods were used to extract, analyze, and synthesize qualitative research findings from peer-reviewed primary and secondary qualitative research reports (Finfgeld-Connett, ref. 2018). The QMS process extends past combining findings from research reports and moves to the development of a theory that is transferable (i.e., generalizable) beyond the original samples. This broadens the applicability of the newly synthesized theory and its capacity to support decision-making and action initiatives (Finfgeld-Connett, ref. 2018). Ethical review board approval was not needed because the data used was already published and deidentified.
Search Strategy
Guided by a health sciences librarian, we searched the literature focusing on childbearing-aged women’s (18 − 44 years) perceptions of and experiences with perinatal cannabis use where cannabis is legal for recreational purposes, including any country, state, and/or jurisdiction. Because recreational cannabis was first legalized in Colorado in 2012, only research reports published in 2012 and after were included. Searches were limited to English and completed between September 2024 through December 2025. Multiple databases were searched, including the Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed, Scopus, PsycINFO, and Web of Science (Table 1). The PRISMA reporting guidelines provided a structured framework for reporting our search processes (Page et al., ref. 2021). Backward and forward searching of included reports were conducted to identify any other relevant reports (Finfgeld-Connett, ref. 2018). Reports focusing on other substances and outside of the perinatal period were excluded. Reports conducted in places with other forms of cannabis legalization such as medicinal, cannabidiol, and decriminalization only were also excluded (Table 2).
Table 1: PubMed search strategy
| Search ID | Search terms | Search options or filters | Results |
|---|---|---|---|
| S10 | (((cannabis OR marijuana OR THC OR Tetrahydrocannabinol) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum OR intrapartum OR peripartum OR postnatal)) AND (perception OR perceptions OR attitude OR attitudes OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group or interview OR interviews) | All Fields | 60 |
| S9 | ((((cannabis OR marijuana OR THC OR Tetrahydrocannabinol) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum OR intrapartum OR peripartum OR postnatal)) AND (legalization OR liberalization OR policy OR policies OR law OR laws)) AND (perception OR perceptions OR attitude OR attitudes OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group OR interview OR interviews)) | All Fields | 20 |
| S8 | ((((cannabis OR marijuana OR THC OR Tetrahydrocannabinol) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum OR intrapartum OR peripartum OR postnatal)) AND (legalization OR liberalization OR policy OR policies OR law OR laws)) AND (perception OR perceptions OR attitude OR attitudes OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group OR interview OR interviews)) | Title/Abstract | 8 |
| S7 | (((cannabis OR marijuana OR THC OR Tetrahydrocannabinol) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum OR intrapartum OR peripartum OR postnatal)) AND (perception OR perceptions OR attitude OR attitudes OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group or interview OR interviews) | Title/Abstract | 20 |
| S6 | (((cannabis OR marijuana OR THC OR Tetrahydrocannabinol) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum OR intrapartum OR peripartum OR postnatal)) AND (perception OR attitude OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group or interview OR interviews) | All Fields | 54 |
| S5 | (((cannabis OR marijuana) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum)) AND (perception OR attitude OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group or interview OR interviews) | All Fields | 53 |
| S4 | (((cannabis OR marijuana) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum)) AND (perception OR attitude OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group or interview OR interviews) | All Fields | 53 |
| S3 | (((cannabis OR marijuana) AND (pregnancy OR perinatal OR prenatal OR antenatal OR postpartum)) AND (perception OR attitude OR knowledge OR belief OR beliefs)) AND (qualitative OR themes OR thematic OR grounded theory OR ethnographic OR ethnonursing OR phenomenological OR focus groups OR focus group or interview OR interviews) | All Fields | 52 |
| S2 | ((((perinatal cannabis use OR prenatal cannabis use OR cannabis use during pregnancy or cannabis use while breastfeeding) AND (women of childbearing age OR women or woman)) AND (knowledge OR attitudes OR beliefs OR experiences OR perceptions)) AND (Interviews OR focus groups or observations)) AND (qualitative) | All Fields | 11 |
| S1 | ((((perinatal cannabis use OR cannabis use during pregnancy OR cannabis use while breastfeeding OR cannabis use before pregnancy) AND (women of childbearing age OR women OR woman)) AND (view* OR experience* OR opinion OR attitude* OR perception* or belief* OR feel* OR know* OR understand*)) AND (interview OR survey OR focus group OR case stud* OR observe*)) AND (qualitative) | All Fields | 11 |
Table 2: Inclusion and exclusion criteria
| Criteria | Include | Exclude | Rationale |
|---|---|---|---|
| Date | 2012 and after | 2011 and before | Recreational cannabis was first legalized in the State of Colorado in 2012. |
| Topic | Research reports related to perinatal cannabis use knowledge, attitudes, beliefs, or experiences | Research reports not related | Focus is on perinatal cannabis use perceptions and experiences. |
| Location | Places where cannabis is legal for recreational adult use | Research reports conducted in places without legal recreational cannabis use. | Focus is on childbearing-aged women living in places recreational cannabis legalization. |
| Age | 18–44 years | Research reports with participants under 18 and over 44 years | Population of interest are adult women of childbearing age. The Centers for Disease Control and Prevention defines the reproductive age for women as 15 to 44 years (Centers for Disease Control and Prevention, ref. 2014). |
| Sex | Women only | Research reports with participants who are not women | Men who have undergone anatomical alterations by surgical intervention may have different pregnancy and birthing perceptions and experiences. |
| Publications | Qualitative research reports; Peer-reviewed publications | Non-qualitative research reports; Grey literature; Non-peer-reviewed publications | Conducting a theory-generating qualitative meta-synthesis of qualitative research reports that have been formally peer-reviewed. |
Search Outcomes
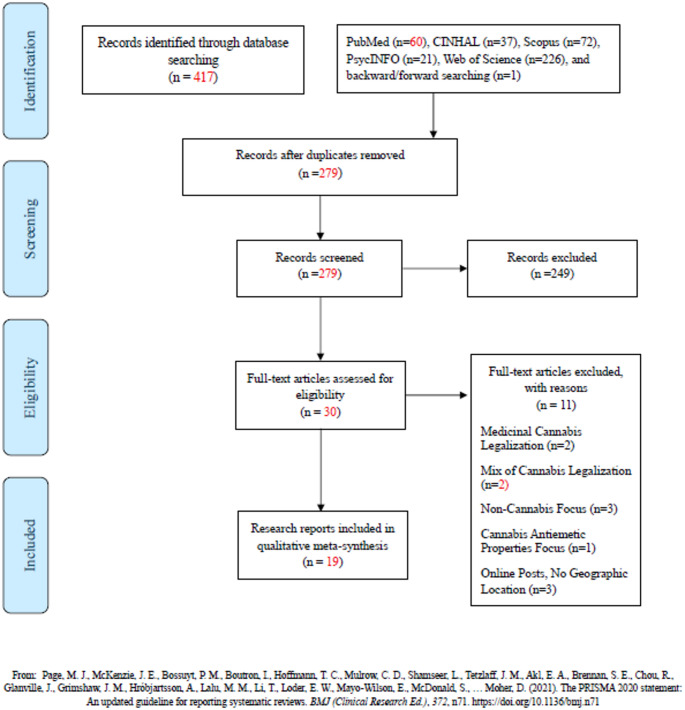
Over 400 published research reports were located (Fig. 1). After removing duplicates, 279 reports were screened for eligibility by reviewing titles and abstracts. Two hundred and forty-nine reports were excluded. Full texts of the remaining 30 reports were retrieved and reviewed. Another 11 reports were excluded because they had a non-cannabis focus (n = 3), focused on the antiemetic properties of cannabis (n = 1), consisted of online posts without geographic information (n = 3), were conducted in US states with only medicinal cannabis legalization (n = 2), or included US states with mixed cannabis legalization statuses (e.g., recreational vs. medicinal) or no form of cannabis legalization at all (n = 2). Nineteen research reports met were included in this QMS. Of the 19 final reports, five were secondary qualitative analyses from the same author group of two primary qualitative research reports also included (Vanstone et al., ref. 2021; Young-Wolff et al., ref. 2022). The rationale for including these reports is that each report addressed a different research question; therefore, there was no expectation that their inclusion would inflate overall findings.
Data Extraction and Analysis
Study characteristics were extracted to familiarize the authors with the study samples and attributes (i.e., purpose, theoretical framework, methods, etc.) (Finfgeld-Connett, ref. 2018). This information was analyzed by summarizing attributes across the reports including article citation, geographic location, study purpose, methods, and sample characteristics (Table 3). We identified the qualitative findings from included research reports, which then served as the raw data analyzed. Raw data included the original authors’ codes, categories, and themes that were primarily found in the results section. Any qualitative findings presented in tables or as direct participant quotes were not considered raw data and were excluded (Finfgeld-Connett, ref. 2018). Extraction of data consisted of copying the full descriptions of the data into a Microsoft Word document and importing those documents into Dedoose qualitative coding software. All extracted data were checked against the research report to prevent transcribing errors and decontextualization of the original qualitative data.
Table 3: CASP: quality appraisal table
| Research reports | Was there a clear statement of the aims of the research? | Is a qualitative methodology appropriate? | Was the research design appropriate to address the aims of the research? | Was the recruitment strategy appropriate to the aims of the research? | Was the data collected, in a way that addressed the research issue? | Has the relationship between researcher and participants been adequately considered? | Have ethical issues been taken into consideration? | Was the data analysis sufficiently rigorous? | Is there a clear statement of findings? | How valuable is the research? |
|---|---|---|---|---|---|---|---|---|---|---|
| Barbosa-Leiker et al. (ref. 2020) | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| English and Greyson (ref. 2022) | Y | Y | NA | Y | Y | Y | Y | Y | Y | Y |
| Foti et al. (ref. 2023) | Y | Y | NA | Y | Y | Y | Y | Y | CT | Y |
| Gould et al. (ref. 2024a, ref. b) | Y | Y | CT | Y | Y | Y | N | Y | Y | Y |
| Gould et al. (ref. 2024a, ref. b) | Y | Y | CT | Y | Y | N | N | Y | Y | Y |
| Greene et al. (ref. 2023) | Y | Y | Y | CT | Y | N | Y | Y | CT | Y |
| Kiel et al. (ref. 2023) | N | Y | NA | Y | Y | N | Y | Y | N | Y |
| Macario and Thomas et al. (ref. 2022) | Y | Y | NA | Y | Y | Y | Y | Y | Y | Y |
| McCoy et al. (ref. 2023) | Y | Y | NA | Y | Y | N | Y | Y | Y | Y |
| Vanstone et al. (ref. 2021) | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Popoola et al. (ref. 2023) | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Taneja et al. (ref. 2023) | Y | Y | NA | Y | Y | Y | Y | Y | CT | Y |
| Woodruff et al. (ref. 2021) | Y | Y | NA | Y | Y | CT | Y | Y | Y | Y |
| Young-Wolff et al. (ref. 2022) | Y | Y | NA | Y | Y | N | Y | Y | Y | Y |
| Young-Wolff et al. (ref. 2024a, ref. b) | Y | Y | NA | Y | Y | Y | Y | Y | Y | Y |
| Mian et al. (ref. 2023) | Y | Y | NA | Y | Y | N | Y | Y | Y | Y |
| Barbosa-Leiker et al. (ref. 2025) | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Denson et al. (ref. 2025) | Y | Y | NA | Y | Y | CT | Y | Y | Y | Y |
| Odgen et al. (ref. 2025) | Y | Y | NA | Y | Y | Y | Y | Y | Y | Y |
Y = ‘Yes’; N = ‘No’; CT = ‘Can’t Tell’; NA = ‘Not Applicable’
Rigor
The purpose of theory-generating QMS research is to develop a new theory without any preexisting assumptions about coding and categorizing structures (Finfgeld-Connett, ref. 2018). The qualitative data extracted from each research report was coded line by line and inductively organized by creating preliminary codes that captured the meaning of the findings. If a single line of data was associated with multiple codes, we examined whether they had captured multiple findings that needed to be separated and analyzed individually. Memoing was used to make sense of concepts and their dynamic relationships within and across research reports, allowing for a robust data analysis process (Finfgeld-Connett, ref. 2018). Reflexivity was also used to ensure that personal biases were not influencing the data analysis process and to evaluate codes and memos to ensure an accurate representation of the data. The trustworthiness and credibility of the resultant theoretical framework were safeguarded through multiple strategies that were used to enhance validity, including unbiased data collection and sampling, memoing, discussions during team meetings, and reflexivity (Finfgeld-Connett, ref. 2018).
Quality Appraisal
The Critical Appraisal Skills Program (CASP) checklist was used to assess the quality of each research report (Table 3). CASP is the most widely used tool for appraising the quality of qualitative research reports and is endorsed by the Cochrane Qualitative and Implementation Methods Group and World Health Organization (Long et al., ref. 2020). This 10-item tool can assess the strengths and limitations of any qualitative research method and is generally believed to be user-friendly for novice researchers.
Results
Attributes of Included Research Reports
All data that was included was collected following recreational cannabis legalization in the respective location. Table 4 presents the attributes of the 19 included research reports, yielding an overall sample of 397 women. Sample sizes from secondary research reports Vanstone et al. (ref. 2021) and Young-Wolff et al. (ref. 2022) were not added to the total count because the samples of their respective primary study were already included. Most of the research reports (n = 15) were conducted in the US and recruited participants from California (n = 8), Washington (n = 3), Colorado (n = 1), Massachusetts (n = 1), Illinois (n = 1), and from a combination of California, Oregon, and Washington (n = 1). The other four research reports were conducted in Canada where recreational cannabis use is legal nationwide. Data collection methods mainly used individual interviews (n = 12) and focus groups (n = 5). One author group used a photovoice workshop (Greene et al., ref. 2023) and another used an online bulletin board in addition to a focus group (Macario & Thomas, ref. 2022). Most research reports described conducting a thematic (n = 11) or content (n = 4) analysis, while the remaining four did not describe data analysis methods.
Table 4: Characteristics of research reports
| First author & year | Geographic location | Study purpose | Methods | Sample characteristics |
|---|---|---|---|---|
| Barbosa-Leiker at al. (ref. 2020) | United States, Washington | To explore pregnant and postpartum women’s perceptions on the benefits and risks of using cannabis perinatally | Interviews, Content Analysis | N = 19 (14 pregnant; 5 postpartum), mostly white between 18 and 29 years, all self-reported cannabis use during pregnancy |
| English and Greyson (ref. 2022) | United States, Massachusetts | To explore how cannabis legalization effects pregnant and breastfeeding women’s perceptions and decision-making about using cannabis perinatally | Semi-structured interviews by phone, Content Analysis | N = 23, 52% 20–29 years, 74% were prior cannabis users and also used during pregnancy and/or breastfeeding |
| Gould et al. (ref. 2024a) | United States, California | To explore pregnant women’s perceptions and patterns of cannabis use, including influences of socio-environmental factors | Semi-structured virtual interviews, Thematic Analysis | N = 19, all over 21 years, self-identified as BIPOC (Black, Indigenous, People of Color), and self-reported cannabis use during pregnancy |
| Gould et al. (ref. 2024b) | United States, California | To explore perceptions about cannabis use during pregnancy among maternal healthcare providers and pregnant cannabis using patients | Semi-structured virtual interviews | N = 7, 57% Hispanic, Mean age = 27 years; Providers: 70% white, 60% 30–59 years |
| Greene et al. (ref. 2023) | Canada | To explore cannabis-using pregnant and breastfeeding women’s experiences with cannabis use stigma and surveillance by health and social care providers | Virtual photovoice workshops, Thematic Analysis | N = 23, 57% Black or Indigenous, all self-reported using cannabis perinatally |
| Kiel et al. (ref. 2023) | United States, Washington | To explore postpartum women’s beliefs, decision-making, and experiences with perinatal cannabis use | Semi-structured interviews | N = 15, 67% white, 73% self-reported continued cannabis use during pregnancy |
| Macario and Thomas (ref. 2022) | United States, Washington | To explore pregnant/breastfeeding and non-pregnant/breastfeeding childbearing aged women’s attitudes and beliefs about perinatal cannabis use | Virtual focus groups and online bulletin board discussions, Thematic Analysis | N = 95 (67 current cannabis users; 28 non-cannabis users), 66% white, Mean age = 32 years |
| McCoy et al. (ref. 2023) | United States, Colorado | To explore rural pregnant and non-pregnant childbearing aged women’s perceptions and experiences related to maternal cannabis use | Semi-structured interviews, Thematic Analysis | N = 9, demographics unavailable |
| Vanstone et al. (ref. 2021) | Canada | To explore why pregnant and breastfeeding women’s use cannabis and changes in motivations across perinatal periods | Semi-structured virtual or phone interviews | N = 52 (30 pregnant; 22 breastfeeding), 69% white, 75% 19–34 years, all self-reported using cannabis before pregnancy |
| Popoola et al. (ref. 2023) * | Canada | To explore pregnant and breastfeeding women’s perceptions of perinatal cannabis use risks and mitigation strategies | Semi-structured virtual or phone interviews, Content Analysis | N = 52 (30 pregnant; 22 breastfeeding), 69% white, 75% 19–34 years, all self-reported using cannabis before pregnancy |
| Taneja et al. (ref. 2023) * | Canada | To explore pregnant and breastfeeding women’s information-seeking behaviors about perinatal cannabis use | Semi-structured virtual interviews, Content Analysis | N = 52 (30 pregnant; 22 breastfeeding), 69% white, 75% 19–34 years, all self-reported using cannabis before pregnancy |
| Woodruff et al. (ref. 2021) | United States, California | To explore pregnant and postpartum women’s experiences about discussing their cannabis use with healthcare providers | Semi-structured interviews, Thematic Analysis | N = 33, 50% Black or Hispanic, mean age = 29 years, all self-reported using cannabis at least weekly before pregnancy |
| Young-Wolff et al. (ref. 2022) | United States, California | To explore pregnant women’s perceptions about recreational cannabis legalization and cannabis use behaviors | Semi-structured virtual focus groups, Thematic Analysis | N = 53, 57% white, mean age = 30 years, 70% self-reported using cannabis daily during pregnancy |
| Young-Wolff et al. (ref. 2024b) * | United States, California | To examine cannabis-using pregnant women’s opinions and experiences regarding their intentions to use cannabis in the postpartum period | Semi-structured virtual focus groups, Thematic Analysis | N = 53, 57% white, mean age = 30 years, 70% self-reported using cannabis daily during pregnancy |
| Mian et al. (ref. 2023) * | United States, California | To examine pregnant women’s perceptions and patterns of cannabis use, including modes of administration | Semi-structured virtual focus groups, Thematic Analysis | N = 53, 57% white, mean age = 30 years, 70% self-reported using cannabis daily during pregnancy |
| Foti et al. (ref. 2023) * | United States, California | To explore pregnant women’s perceptions of cannabis use during pregnancy and healthcare experiences | Semi-structured virtual focus groups, Thematic Analysis | N = 53, 57% white, mean age = 30 years, 70% self-reported using cannabis daily during pregnancy |
| Barbosa-Leiker et al. (ref. 2025) | United States, California, Oregon, Washinton | To explore pregnant and postpartum American Indian women’s perceptions of risks and benefits of perinatal cannabis use | Semi-structured virtual or in-person interviews, Thematic Analysis | N = 10 (5 pregnant; 5 postpartum), 100% American Indian, mean age = 29 years, 90% self-reported using cannabis regularly during pregnancy and 10% only during postpartum |
| Denson et al. (ref. 2025) | United States,illinois | To examine postpartum and future pregnant women’s beliefs and perceptions of perinatal cannabis use | Semi-structured virtual interviews or focus groups, Thematic Analysis | N = 20, 50% Black or African American, 50% White, 10% Hispanic or Latina, mean age = 30 years, 4.4% self-reported current daily or weekly use of cannabis |
| Odgen et al. (ref. 2025) | United States,California | To explore postpartum women’s motivations for perinatal cannabis use and desire for interventions | Semi-structured interviews, Thematic analysis | N = 17, 53% White, 23.5% Black, 23.5% Hispanic, mean age = 26 years, 71% self-reported daily cannabis use during postpartum and 59% during breastfeeding |
*Secondary analysis
Identified Themes
Eight primary themes impacting decision-making about perinatal cannabis use were identified and are detailed below.
Recreational Cannabis Legalization
The nuances surrounding recreational cannabis legalization, such as the applicability of the policy and legal implications for this population, resulted in both uncertainty and acceptance of perinatal cannabis use. Several women discussed disparities in public health messaging about the policy of legal recreational cannabis use for those who are pregnant or breastfeeding (Barbosa-Leiker et al., ref. 2020; English & Greyson, ref. 2022; McCoy et al., ref. 2023). For example, women expressed concerns about whether the legal status of cannabis was similar to that of alcohol and tobacco or if it was still considered an illicit substance because it remains illegal federally (English & Greyson, ref. 2022). Conversely, some women were more open to discussing their perinatal cannabis use following legalization, under the misconception that it was an indicator that cannabis was permitted and safe to consume (Young-Wolff et al., ref. 2022). Cannabis retailers (e.g., cannabis dispensaries) and budtenders (i.e., people who work at dispensaries) were frequently relied on as a source for cannabis information and products (Mian et al., ref. 2023; Young-Wolff et al., ref. 2022). Women believed cannabis products from retailers were better regulated (i.e., safer) and that budtenders were knowledgeable (i.e., trained) (Barbosa-Leiker et al., ref. 2020; Gould et al., ref. 2024a; Macario & Thomas, ref. 2022).
Clinical Policies and Practices
Women expressed concerns about routine drug testing policies and the possibility of their infant being tested at birth (English & Greyson, ref. 2022; Greene et al., ref. 2023; Woodruff et al., ref. 2021). Most women shared fears of being reported to child protection services (CPS) if their perinatal cannabis use was discovered (Barbosa-Leiker et al., ref. 2020; English & Greyson, ref. 2022; Foti et al., ref. 2023; Greene et al., ref. 2023; Macario & Thomas, ref. 2022; Popoola et al., ref. 2023; Woodruff et al., ref. 2021; Young-Wolff et al., ref. 2022). Women believed CPS involvement would increase their risk of surveillance or having their infant removed from the home (English & Greyson, ref. 2022; Macario & Thomas, ref. 2022; Woodruff et al., ref. 2021). Low-income and racial and ethnic minority women were particularly concerned about legal repercussions, with many indicating that their identity put them at higher risk for drug testing and CPS involvement (Foti et al., ref. 2023; Greene et al., ref. 2023).
Stigma and Discrimination
Many women perceived various sources and forms of stigma (e.g., health care clinicians, social, and anticipated stigma) regarding their perinatal cannabis use. Stigma from clinicians was commonly reported, and women believed that recommendations were based on the clinicians’ personal biases rather than medical expertise. Some women suggested up-to-date knowledge and training about perinatal cannabis use are needed to destigmatize discussions and promote patient-centered care (English & Greyson, ref. 2022; McCoy et al., ref. 2023). Anticipated stigma or preconceived notions also affected women’s decisions and limited their disclosure of perinatal cannabis use (Foti et al., ref. 2023; Gould et al., ref. 2024a; Odgen et al., ref. 2025; Vanstone et al., ref. 2021). Some women from historically marginalized populations reported discrimination by clinicians and social workers, refraining them from inquiring for information and increasing punitive fears (English & Greyson, ref. 2022; Foti et al., ref. 2023; Greene et al., ref. 2023).
Access and Desire for Information
Most women emphasized the importance and need for evidence-based information about the safety, risks, and effects of using cannabis during the perinatal period (Denson et al., ref. 2025; Popoola et al., ref. 2023; Taneja et al., ref. 2023; Young-Wolff et al., ref. 2024b). Women expressed that current scientific research and medical information provided little guidance about the safety of perinatal cannabis use and lacked conclusive results on its effects (Denson et al., ref. 2025; Foti et al., ref. 2023; Macario & Thomas, ref. 2022; McCoy et al., ref. 2023). This inconsistency contributed to the predominant concern of being misinformed (Greene et al., ref. 2023). As a result, women searched for their own information online or asked others about their beliefs and experiences with perinatal cannabis use (English & Greyson, ref. 2022; Foti et al., ref. 2023; Gould et al., ref. 2024a; Kiel et al., ref. 2023; Macario & Thomas, ref. 2022; McCoy et al., ref. 2023; Odgen et al., ref. 2025; Taneja et al., ref. 2023; Woodruff et al., ref. 2021).
Clinician-Patient Relationships
Clinicians provided varied levels of perinatal health care and support to their patients. Most women experienced feelings of distrust and were uncomfortable bringing up perinatal cannabis use with their clinician (English & Greyson, ref. 2022; Greene et al., ref. 2023; McCoy et al., ref. 2023; Woodruff et al., ref. 2021). Some women reported wanting to engage in open conversations about their cannabis use and reasons for consumption, but only a few did (English & Greyson, ref. 2022; Foti et al., ref. 2023; Odgen et al., ref. 2025; Taneja et al., ref. 2023; Woodruff et al., ref. 2021). Women engaging in conversations with clinicians noticed the focus often shifted from their health as pregnant/parenting patients toward educating about the negative effects on the developing fetus or infant, leading them to feel unheard and uncared for (Barbosa-Leiker et al., ref. 2020; Gould et al., ref. 2024b; Young-Wolff et al., ref. 2024b). Clinicians generally encouraged abstinence over harm reduction approaches designed to reduce negative health outcomes (Barbosa-Leiker et al., ref. 2020, ref. 2025; Denson et al., ref. 2025; Greene et al., ref. 2023). Women received mixed messages and insufficient information about perinatal cannabis use, leading some to question their clinician’s medical expertise (English & Greyson, ref. 2022; Kiel et al., ref. 2023; Odgen et al., ref. 2025; Taneja et al., ref. 2023; Woodruff et al., ref. 2021). Others experienced a complete lack of communication, with several women claiming that their clinicians did not ask them about or follow up on their perinatal cannabis use at all (Barbosa-Leiker et al., ref. 2025; Gould et al., ref. 2024b; Woodruff et al., ref. 2021). Women from historically marginalized populations expressed a significant lack of support and cultural incompetence from clinicians altogether, creating a desire for services from people with similar backgrounds (Foti et al., ref. 2023; Greene et al., ref. 2023; Odgen et al., ref. 2025).
Most Trusted Sources: Family and Friends
Women frequently turned to family and friends to ask for information about their personal experiences with perinatal cannabis use (Denson et al., ref. 2025; Foti et al., ref. 2023; Macario & Thomas, ref. 2022; Taneja et al., ref. 2023; Woodruff et al., ref. 2021). Women made decisions based on these personal narratives because they were valid firsthand experiences from people who had been in the same situation (Denson et al., ref. 2025; Mian et al., ref. 2023; Taneja et al., ref. 2023). Some described valuing their partners’ input and support in their decisions to use cannabis perinatally (Kiel et al., ref. 2023; Mian et al., ref. 2023; Popoola et al., ref. 2023). Other women concealed their use from friends or family out of fear of stigma or judgment (English & Greyson, ref. 2022; Taneja et al., ref. 2023).
Perceptions and Experiences
Decisions were primarily influenced by their perceptions of the benefits and risks of cannabis, as well as the potential effects on fetal or infant health. The subthemes below provide a full description of the key factors driving decision-making.
Cannabis Benefits and Risks
Many women weighed the risks and benefits of perinatal cannabis use, particularly as they sought to mitigate their own needs against potential harm to their fetus/infant. They generally perceived cannabis as a ‘natural’ medicine or plant that was more effective in treating their symptoms compared to prescription medications (Foti et al., ref. 2023; Greene et al., ref. 2023; Kiel et al., ref. 2023; Macario & Thomas, ref. 2022; Odgen et al., ref. 2025; Vanstone et al., ref. 2021). Cannabis was perceived as a ‘safer’ alternative with fewer harmful risks for their fetus/infant, and for themselves. Some women drew comparisons between cannabis and other substances with well-established risks (e.g., alcohol, tobacco, opioids, etc.) to justify their beliefs and decisions to use cannabis perinatally (Barbosa-Leiker et al., ref. 2020, ref. 2025; Denson et al., ref. 2025; Foti et al., ref. 2023; Greene et al., ref. 2023; Kiel et al., ref. 2023; Macario & Thomas, ref. 2022; McCoy et al., ref. 2023; Young-Wolff et al., ref. 2024b). Other women shared using cannabis as a harm reduction strategy or substitute to decrease their use of higher-risk substances, such as methamphetamine, heroin, or opioids (Barbosa-Leiker et al., ref. 2025; Greene et al., ref. 2023; Kiel et al., ref. 2023). Ultimately, most believed that the benefits of cannabis for managing their symptoms outweighed the known harmful risks to their fetus/infant.
Impact on Fetal/Infant Health
Primary concerns about using perinatal cannabis included the effects that it could have on fetal/infant health (Barbosa-Leiker et al., ref. 2020; Denson et al., ref. 2025; Gould et al., ref. 2024b; Kiel et al., ref. 2023; McCoy et al., ref. 2023; Mian et al., ref. 2023; Popoola et al., ref. 2023; Taneja et al., ref. 2023; Vanstone et al., ref. 2021; Young-Wolff et al., ref. 2024b). Women observed the impact of their cannabis use during their pregnancy or after giving birth by looking for specific symptoms or signs of harm. They perceived miscarriage, premature delivery, LBW, asthma, ADHD, and neurodevelopmental issues as risks of perinatal cannabis use (Kiel et al., ref. 2023; Popoola et al., ref. 2023). To these women, the absence of these adverse outcomes indicated that their infant was not affected by their use. Others turned to the well-established harmful effects of tobacco use during pregnancy on fetal development to understand the potential risks of smoking cannabis (Mian et al., ref. 2023). Several women also perceived that cannabis use during breastfeeding was more dangerous than cannabis use during pregnancy because they believed THC could more directly reach the infant through breast milk (Barbosa-Leiker et al., ref. 2020; Kiel et al., ref. 2023; Young-Wolff et al., ref. 2024b). However, there were also mixed perceptions about the effects of consuming cannabis during breastfeeding (Barbosa-Leiker et al., ref. 2025; Odgen et al., ref. 2025).
Managing Consumption and Safety
Due to the possible risks associated with cannabis on fetal/infant health, many women changed their cannabis use during the perinatal period as a precautionary measure (Barbosa-Leiker et al., ref. 2025; Foti et al., ref. 2023; Kiel et al., ref. 2023; Popoola et al., ref. 2023; Taneja et al., ref. 2023; Vanstone et al., ref. 2021; Woodruff et al., ref. 2021; Young-Wolff et al., ref. 2022; Young-Wolff, Green, Young-Wolff et al., ref. 2024b). While some described ceasing their cannabis use upon learning about their pregnancy, others reduced their frequency to mitigate risks (Foti et al., ref. 2023; Popoola et al., ref. 2023; Vanstone et al., ref. 2021; Woodruff et al., ref. 2021; Young-Wolff, Green, Young-Wolff et al., ref. 2024b). Women who stopped during pregnancy typically planned to resume use after birth or breastfeeding (Odgen et al., ref. 2025; Popoola et al., ref. 2023; Vanstone et al., ref. 2021; Young-Wolff, Green, Young-Wolff et al., ref. 2024b). Most who continued to use cannabis throughout pregnancy or breastfeeding changed their mode of consumption, such as from inhalation to edible products, opted for using tobacco-free papers to smoke cannabis, or managed levels of THC (Barbosa-Leiker et al., ref. 2025; Gould et al., ref. 2024b; McCoy et al., ref. 2023; Mian et al., ref. 2023; Popoola et al., ref. 2023). They also expressed preferences on purchasing cannabis, with many turning to dispensaries they trusted or family members who grew their own cannabis (Gould et al., ref. 2024b; Mian et al., ref. 2023; Young-Wolff et al., ref. 2022). Breastfeeding women described switching to formula feeding or ‘pumping and dumping’ breast milk (i.e., pumping breast milk after consuming cannabis and throwing it away instead of feeding it to their infant) to continue using cannabis (Kiel et al., ref. 2023; Young-Wolff, Green, Young-Wolff et al., ref. 2024b). Other breastfeeding women increased their hygiene (i.e., washing hands or body and changing their clothes before coming into contact with their infant, smoking cannabis outside or at work instead of at home, etc.) or managing time between cannabis use and breastfeeding (i.e., using cannabis well before or shortly after breastfeeding) (Odgen et al., ref. 2025; Popoola et al., ref. 2023; Young-Wolff, Green, Young-Wolff et al., ref. 2024b).
Self-management
Most women described using cannabis to self-medicate perinatal mental health symptoms including stress, anxiety, trauma, and depression (Barbosa-Leiker et al., ref. 2020, ref. 2025; Denson et al., ref. 2025; English & Greyson, ref. 2022; Foti et al., ref. 2023; Gould et al., ref. 2024a; Gould, Ganesh, Nguyen, Gould et al., ref. 2024a, ref. b; Greene et al., ref. 2023; Kiel et al., ref. 2023; Macario & Thomas, ref. 2022; Mian et al., ref. 2023; Odgen et al., ref. 2025; Vanstone et al., ref. 2021; Woodruff et al., ref. 2021; Young-Wolff et al., ref. 2024). Cannabis was also used to self-manage pregnancy-related symptoms, such as nausea and vomiting, loss of appetite, pain, weight gain, and difficulty sleeping (Barbosa-Leiker et al., ref. 2025; Denson et al., ref. 2025; Foti et al., ref. 2023; Macario & Thomas, ref. 2022; Mian et al., ref. 2023; Vanstone et al., ref. 2021; Woodruff et al., ref. 2021), as well as symptoms from chronic conditions, like fibromyalgia or chronic pain (Kiel et al., ref. 2023; Macario & Thomas, ref. 2022). While most continued to use cannabis for its symptom management benefits, others discontinued use due to concerns about the effects on fetal/infant health (Foti et al., ref. 2023; Popoola et al., ref. 2023; Vanstone et al., ref. 2021; Young-Wolff et al., ref. 2022). However, some women experienced negative effects and believed cessation worsened their symptoms, resulting in cannabis reuptake (English & Greyson, ref. 2022). Women who previously used cannabis perinatally and whose children had not developed any health problems felt more comfortable using it again (Kiel et al., ref. 2023; Macario & Thomas, ref. 2022; Popoola et al., ref. 2023; Young-Wolff et al., ref. 2022). Concurrently, those who experienced pregnancy or birth complications questioned whether this was a result of their perinatal cannabis use (Kiel et al., ref. 2023; Popoola et al., ref. 2023).
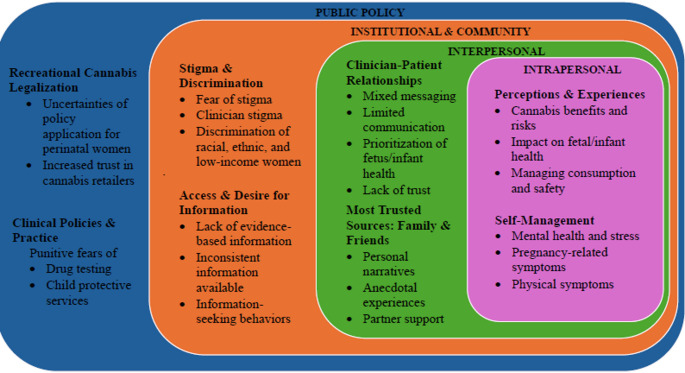
Perinatal Cannabis Use Decision-Making Model
Our findings resulted in eight primary themes and subthemes that served as constructs of the perinatal cannabis use decision-making model (Fig. 2). Based on Bronfenbrenner at al.‘s (ref. 1977) original Socio-Ecological Model, our model emphasizes the interdependencies of critical public policy, institutional and community, interpersonal, and intrapersonal factors that influence women’s decision-making. Specifically, our model identifies factors that require both public health (e.g., clear cannabis messaging for pregnant/parenting women, perinatal cannabis use education, etc.) and clinical interventions (e.g., non-stigmatizing and patient-centered care conversations, evidence-based and up-to-date information, etc.) to help women make better, more informed decisions when considering using cannabis perinatally.
Discussion
Legalization implications have led to an increased perception of safety due to its regulation, resulting in a potential higher likelihood of perinatal cannabis use. Our findings support quantitative studies demonstrating that women are more likely to use cannabis during the perinatal period in US states where cannabis is legal recreationally compared to US states where cannabis is not legal recreationally (Skelton et al., ref. 2020; Sood et al., ref. 2022; Vachhani et al., ref. 2022). The reliance on cannabis retailers for products and information is concerning because there is no consistent legislation for licensing across states that legalized recreational cannabis use, resulting in both licensed and unlicensed facilities (Unger et al., ref. 2020). There is also contradicting evidence that dispensaries are counseling pregnant women about using cannabis to treat pregnancy-related symptoms, such as nausea and vomiting, in places with legalized recreational use (Dickson et al., ref. 2018; Vastis et al., ref. 2021). We acknowledge that recreational legalization is for the general adult population and that legalizing cannabis has broader benefits, including for societal (e.g., justice decriminalization, taxation, and product regulation) and therapeutic purposes (e.g., anti-emesis, pain relief, appetite stimulation, etc.).
On the other hand, limited studies have examined attitudes toward cannabis during pregnancy in places where recreational use is not legalized. For example, Ramseyer et al.’s (ref. 2024) cross-sectional survey study indicates pregnant cannabis users and nonusers’ share permissive legalization attitudes, minimal perceived risks, lack of counseling, and desire for more information about risks. Other survey-based studies suggest women’s mixed attitudes toward legalization (Mark et al., ref. 2017) and beliefs of slight to no risk of harm (Ko et al., ref. 2015). Moreover, Keyhani et al.’s (ref. 2018) survey study indicates that the general US adult population believed cannabis was beneficial for managing pain, anxiety, stress, and depression. Although these attitudes emerged in settings without recreational legalization, their findings closely reflect the themes identified in our qualitative meta-synthesis, suggesting broader societal or cultural patterns. Regardless of legalization, policymakers, public health, and clinicians should provide clearer communications about perinatal cannabis use and its potential medical or legal consequences to better support informed decision-making among pregnant and parenting women.
A strong need for evidence-based information about the safety, risks, and effects of perinatal cannabis use was emphasized by women in our study, similar to prior research (Jarlenski et al., ref. 2016; Jarlenski & Spencer, ref. 2022). Most information available was perceived as unclear and inconsistent, which did not help guide decision-making about perinatal cannabis use. This resulted in the same information-seeking behaviors (i.e., online searching and reliance on family and friends’ personal experiences) that women reported in Jarlenski et al.‘s (ref. 2016) study nearly a decade ago, before medicinal cannabis legalization. Consistent with recent studies, women described turning to online posts on forums, discussion boards, or social media (Lebron et al., ref. 2022; Micalizzi et al., ref. 2024; Oram et al., ref. 2018). Our study aligns with Chang et al.‘s (ref. 2019) findings suggesting that women base their perinatal cannabis use decisions on their knowledge about other substances (e.g., tobacco and alcohol) due to the lack of information about the effects of cannabis.
Most importantly, our findings raised the issue of how pregnant and parenting women perceive cannabis use risks in the absence of negative effects or even when effects are present, they doubt it is due to their use. Based on limited research (Goodin et al., ref. 2025; McKenzie et al., ref. 2022; Satti et al., ref. 2022😉 and our own findings, we speculate the benefits gained from using cannabis perinatally at that point in time are driving factors shaping risk perceptions and continued use. This may be particularly relevant for women who are experiencing higher volumes of stress (Satti et al., ref. 2022), pregnancy-related symptoms (McKenzie et al., ref. 2022), and uncertainty about the risks of using cannabis during the perinatal period (Goodin et al., ref. 2025). As such, our findings warrant further investigation and the development of public health campaigns and evidence-based educational materials to clearly inform women about perinatal cannabis use effects, risks, and safety.
Clinicians play a critical role in perinatal cannabis use decision-making, specifically when providing care and delivering health messages to their pregnant or parenting patients. Our findings indicate that clinician’s engagement in delivering perinatal health care and discussing cannabis use varied substantially, similar to other studies (Bayrampour et al., ref. 2019). Most women didn’t disclose their cannabis use or engage in conversations with clinicians due to fears of being reported to CPS, supporting Jarlenski and colleagues (ref. 2016) findings. Additionally, limited or unclear communications decreased women’s trust in clinicians and generated feelings of being unheard as patients, similar to women who misused opioids perinatally (Morton et al., ref. 2023). Others reported not receiving any type of care at all, as highlighted by other women in Bayrampour et al.‘s (ref. 2019) review. Further, an ethical issue raised in some of our findings is the notion that cannabis may be safer than other substances, especially for people who have a history of using higher-risk substances (e.g., methamphetamine, heroin, opioids) (Barbosa-Leiker et al., ref. 2025; Greene et al., ref. 2023; Kiel et al., ref. 2023). Future work could focus on examining whether cannabis is a better alternative for people who use higher-risk substances, particularly during the perinatal period.
There are social issues to consider. Several women described experiencing stigma and discrimination from clinicians for their cannabis use during pregnancy or breastfeeding, like a review examining the effects of stigma on substance-using pregnant people to improve perinatal care (Weber et al., ref. 2021). Additionally, discrimination and inadequate culturally competent care were highlighted by women from historically marginalized populations, consistent with Murphy et al.’s (ref. 2022) review exploring perinatal experiences among Black women. These experiences can inflict a significant lack of trust in clinicians, resulting in women searching for information on their own, relying on friends and family, and self-medication practices. Consistent with other quantitative studies, our findings capture an uptake in self-medication practices to manage mental health and pregnancy-related symptoms (Vanstone et al., ref. 2022). Now is a seemingly pivotal time for clinicians, including nurses, to focus on building trusted relationships with women to screen for and discuss perinatal cannabis use in a non-stigmatizing and culturally competent manner. Nurse-patient communication interactions are well-documented and can be leveraged to improve perinatal and cannabis healthcare delivery (Höglander et al., ref. 2023).
Limitations
Relevant research reports may have been overlooked due to limitations in the search terms, databases, and inclusion and exclusion criteria used. Five research reports conducted secondary qualitative analyses of primary research reports were included, potentially skewing results because they used the same sample. We focused on locations where recreational cannabis use is legalized and on women of childbearing age living there, potentially limiting the applicability of these findings to different populations and settings. Finally, the sensitive and frequently stigmatized nature of perinatal cannabis use may have influenced participant responses, limiting the richness of qualitative findings we analyzed. These limitations should be considered when interpreting our study’s findings and implications.
Conclusion
Our QMS highlights the complex interactions of social and contextual factors that influence women’s perceptions and experiences with perinatal cannabis use. Our findings provide insight into decision-making about whether to use cannabis during the perinatal period and are consistent with available empirical evidence. Through targeted public health interventions and clinical support strategies, we can move closer to addressing the complexities of cannabis use during the perinatal period, especially in a time of expanding recreational cannabis legalization and social acceptance.
References
- T Baker, P Datta, K Rewers-Felkins, H Thompson, RR Kallem, TW Hale. Transfer of inhaled cannabis into human breast milk. Obstetrics and Gynecology, 2018. [DOI | PubMed]
- C Barbosa-Leiker, O Brooks, CL Smith, SC Reid, GL Fatima, KA Hirchak, R Arias-Losado, M Cabell. American Indian women’s perceptions of perinatal cannabis use. American Journal of Drug and Alcohol Abuse, 2025. [DOI | PubMed]
- C Barbosa-Leiker, E Burduli, CL Smith, O Brooks, M Orr, M Gartstein. Daily cannabis use during pregnancy and postpartum in a state with legalized recreational cannabis. Journal of Addiction Medicine, 2020. [DOI | PubMed]
- H Bassalov, N Yakirevich-Amir, I Reuveni, C Monk, S Florentin, O Bonne, I Matok. Prenatal cannabis exposure and the risk for neuropsychiatric anomalies in the offspring: A systematic review and meta-analysis. American Journal of Obstetrics and Gynecology, 2024. [DOI | PubMed]
- H Bayrampour, M Zahradnik, S Lisonkova, P Janssen. Women’s perspectives about cannabis use during pregnancy and the postpartum period: An integrative review. Preventive Medicine, 2019. [DOI | PubMed]
- KA Bertrand, NJ Hanan, G Honerkamp-Smith, BM Best, CD Chambers. Marijuana use by breastfeeding mothers and cannabinoid concentrations in breast milk. Pediatrics, 2018. [DOI | PubMed]
- U Bronfenbrenner. Toward an experimental ecology of human-development. American Psychologist, 1977. [DOI]
- Centers for Disease Control and Prevention. (2014). CDC’s division of reproductive health works to improve mental health among women of reproductive age. https://www.cdc.gov/ccindex/pdf/mentalhealthamongwomenofreproductiveage_vb.pdf
- JC Chang, JA Tarr, CL Holland, NM De Genna, GA Richardson, KL Rodriguez, J Sheeder, KL Kraemer, NL Day, D Rubio, M Jarlenski, RM Arnold. Beliefs and attitudes regarding prenatal marijuana use: Perspectives of pregnant women who report use. Drug and Alcohol Dependence, 2019. [DOI | PubMed]
- RK Denson, M Guerrero, W Bond, A Patterson, G May, T Polatsek, RJ Mermelstein. Beliefs and perceived benefits and harms of perinatal cannabis use among pre- and post-pregnancy women. Drug and Alcohol Dependence Reports, 2025. [DOI | PubMed]
- B Dickson, C Mansfield, M Guiahi, AA Allshouse, LM Borgelt, J Sheeder, RM Silver, TD Metz. Recommendations from cannabis dispensaries about first-trimester cannabis use. Obstetrics and Gynecology, 2018. [DOI | PubMed]
- DISA Global Solutions (2025). Marijuana legality by state – updated January 1, 2025. https://disa.com/marijuana-legality-by-state
- F English, D Greyson. You still have that fear: Policy constraints on informed decision making about legalized cannabis use during pregnancy and lactation. International Journal of Drug Policy, 2022. [DOI | PubMed]
- D Finfgeld-Connett. A guide to qualitative meta-synthesis, 2018
- TR Foti, A Green, A Altschuler, E Iturralde, MB Does, M Jackson-Morris, SR Adams, N Goler, D Ansley, A Conway, KC Young-Wolff. Patient perceptions of prenatal cannabis use and implications for clinicians. Obstetrics and Gynecology, 2023. [DOI | PubMed]
- A Goodin, DS Varma, K Dhillon, S Kaleem, S Dubare, A Jennings, BA Goldberger, K Roussos-Ross. Perception of risks of cannabis and cannabidiol use during pregnancy: A multi-methods study. Medical Cannabis and Cannabinoids, 2025. [DOI | PubMed]
- EE Gould, SS Ganesh, RC Ceasar. I don’t need my kid to be high”: Prioritizing harm reduction when using cannabis during pregnancy. Harm Reduction Journal, 2024. [DOI | PubMed]
- EE Gould, SS Ganesh, RM Nguyen, CV Breton, TM Bastian, GF Dunton, RC Ceasar. The unseen patient: Competing priorities between patients and providers when cannabis is used in pregnancy, a qualitative study. Frontiers in Global Women’s Health, 2024. [DOI | PubMed]
- S Greene, M Vaccaro, A Bernier, G Griffith, A Ion, R Maurice, C Gabel, M Blake. Digging in: Stigma and surveillance in the lives of pregnant and breastfeeding mothers who consume cannabis. Critical Public Health, 2023. [DOI]
- J. Van Höglander, I. K. Holmström, A. Lövenmark, S. Dulmen, H. Eide, A. J. Sundler. Registered nurse-patient communication research: An integrative review for future directions in nursing research. Journal of Advanced Nursing, 2023. [DOI | PubMed]
- M Jarlenski, N Spencer. Perceptions of safety around use of cannabis and nicotine/tobacco in pregnancy. Clinical Obstetrics and Gynecology, 2022. [DOI | PubMed]
- M Jarlenski, JA Tarr, CL Holland, D Farrell, JC Chang. Pregnant women’s access to information about perinatal marijuana use: A qualitative study. Women’s Health Issues, 2016. [DOI | PubMed]
- S Keyhani, S Steigerwald, J Ishida, M Vali, M Cerdá, D Hasin, C Dollinger, SR Yoo, BE Cohen. Risks and benefits of marijuana use: A National Survey of U.S. Adults. Annals of Internal Medicine, 2018. [DOI | PubMed]
- L Kiel, C Hsu, PD Wartko, L Albertson-Junkans, J Ewing, GT Lapham. Perspectives from women who engaged in prenatal and postpartum cannabis use in a U.S. state with legal non-medical use. Preventive Medicine Reports, 2023. [DOI | PubMed]
- JY Ko, KC Coy, SC Haight, TM Haegerich, L Williams, S Cox, R Njai, AM Grant. Characteristics of marijuana use during pregnancy—Eight states, pregnancy risk assessment monitoring system, 2017. MMWR. Morbidity and Mortality Weekly Report, 2020. [DOI | PubMed]
- JY Ko, SL Farr, VT Tong, AA Creanga, WM Callaghan. Prevalence and patterns of marijuana use among pregnant and nonpregnant women of reproductive age. American Journal of Obstetrics and Gynecology, 2015. [DOI | PubMed]
- CN Lebron, V Morales, S Saenz, DC Vidot. “Ganja mamas”: Online discussions about cannabis use in pregnancy. Drug and Alcohol Dependence, 2022. [DOI | PubMed]
- JO Lo, B Shaw, S Robalino, CK Ayers, S Durbin, MC Rushkin, A Olyaei, D Kansagara, CS Harrod. Cannabis use in pregnancy and neonatal outcomes: A systematic review and meta-analysis. Cannabis and Cannabinoid Research, 2024. [DOI | PubMed]
- HA Long, DP French, JM Brooks. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Research Methods in Medicine & Health Sciences, 2020. [DOI]
- E Macario, RM Thomas. Reasons Washington state women use marijuana during pregnancy/breastfeeding, their trusted information sources, and communication strategies for informed decision-making. The Journal of Perinatal & Neonatal Nursing, 2022. [DOI | PubMed]
- K Mark, J Gryczynski, E Axenfeld, RP Schwartz, M Terplan. Pregnant women’s current and intended cannabis use in relation to their views toward legalization and knowledge of potential harm. Journal of Addiction Medicine, 2017. [DOI | PubMed]
- L McCoy, S Newman Carroll, K Walters. It’s so natural it goes hand in hand”: A qualitative study of maternal perceptions of cannabis use during pregnancy. Journal of Psychoactive Drugs, 2023. [DOI | PubMed]
- LB McKenzie, SA Keim, MA Klebanoff. Risk perceptions about cannabis use and receipt of health-related information during pregnancy. American Journal of Health Promotion, 2022. [DOI | PubMed]
- MN Mian, TR Foti, A Green, E Iturralde, A Altschuler, MB Does, M Jackson-Morris, SR Adams, DD Satre, D Ansley, KC Young-Wolff. Exploring preferences for different modes of cannabis use during early pregnancy: A qualitative study. Addictive Behaviors, 2023. [DOI | PubMed]
- L Micalizzi, ER Aston, J Nesi, D Price, RL Gunn. A descriptive analysis of a popular pregnancy forum: Comments on the developmental consequences of cannabis use on offspring. Journal of Studies on Alcohol and Drugs, 2024. [DOI | PubMed]
- J Morton, J Vignato, AB Anbari. Stigma experienced by perinatal women with opioid dependency in the United States: A qualitative meta-synthesis. Western Journal of Nursing Research, 2023. [DOI | PubMed]
- L Murphy, F Liu, R Keele, B Spencer, K Kistner Ellis, D Sumpter. An integrative review of the perinatal experiences of Black women. Nursing for Women’s Health, 2022. [DOI | PubMed]
- Office of the Surgeon General. (2019). U.S. Surgeon general’s advisory: Marijuana use and the developing brain. U.S. Department of Health and Human Services.
- SN Ogden, TR Foti, MB Does, A Altschuler, E Iturralde, SA Sterling, D Ansley, C Castellanos, KC Young-Wolff. Cannabis use behaviors and desired interventions among postpartum individuals with frequent cannabis use in early pregnancy: A qualitative study. Journal of Addiction Medicine, 2025. [DOI | PubMed]
- D Oram, G Tzilos Wernette, LP Nichols, VGV Vydiswaran, X Zhao, T Chang. Substance use among young mothers: An analysis of Facebook posts. JMIR Pediatrics and Parenting, 2018. [DOI | PubMed]
- MJ Page, JE McKenzie, PM Bossuyt, I Boutron, TC Hoffmann, CD Mulrow, L Shamseer, JM Tetzlaff, EA Akl, SE Brennan, R Chou, J Glanville, JM Grimshaw, A Hróbjartsson, MM Lalu, T Li, EW Loder, E Mayo-Wilson, S McDonald, D Moher. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ (Clinical Research Ed.), 2021. [DOI | PubMed]
- SE Paul, AS Hatoum, JD Fine, EC Johnson, I Hansen, NR Karcher, AL Moreau, E Bondy, Y Qu, EB Carter, CE Rogers, A Agrawal, DM Barch, R Bogdan. Associations between prenatal cannabis exposure and childhood outcomes: Results from the ABCD study. JAMA Psychiatry, 2021. [DOI | PubMed]
- A Popoola, J Panday, S Taneja, D Greyson, SD McDonald, T Patel, E Darling, M Vanstone. Pregnant and lactating people’s strategies to mitigate the risk of cannabis consumption. Women’s Health (London, England), 2023. [DOI | PubMed]
- A Ramseyer, S Kennon-McGill, LL Miron, CH Wells, K Davis, S Ray-Griffith. Perceptions about marijuana use in pregnancy among pregnant users and nonusers in a state without legalized recreational cannabis [ID 2683513]. Obstetrics and Gynecology, 2024. [DOI]
- MA Satti, EG Reed, ES Wenker, SL Mitchell, J Schulkin, ML Power, DA Mackeen. Factors that shape pregnant women’s perceptions regarding the safety of cannabis use during pregnancy. Journal of Cannabis Research, 2022. [DOI | PubMed]
- KR Skelton, AA Hecht, SE Benjamin-Neelon. Recreational cannabis legalization in the US and maternal use during the preconception, prenatal, and postpartum periods. International Journal of Environmental Research and Public Health, 2020. [DOI | PubMed]
- S Sood, L Trasande, SS Mehta-Lee, SG Brubaker, A Ghassabian, MH Jacobson. Maternal cannabis use in the perinatal period: Data from the pregnancy risk assessment monitoring system marijuana supplement, 2016–2018. Journal of Addiction Medicine, 2022. [DOI | PubMed]
- Substance Abuse and Mental Health Services Administration (2022). 2020 National survey on drug use and health: Women. https://www.samhsa.gov/data/report/2020-nsduh-women
- S Taneja, J Panday, A Popoola, D Greyson, SD McDonald, T Patel, M Vanstone. Making informed choices about cannabis use during pregnancy and lactation: A qualitative study of information use. Birth (Berkeley, Calif.), 2023. [DOI | PubMed]
- Committee opinion 722: Marijuana use during pregnancy and lactation. Obstetrics and Gynecology, 2017. [DOI | PubMed]
- JB Unger, RO Vos, JS Wu, K Hardaway, AYL Sarain, DW Soto, C Rogers, J Steinberg. Locations of licensed and unlicensed cannabis retailers in California: A threat to health equity?. Preventive Medicine Reports, 2020. [DOI | PubMed]
- K Vachhani, AN Simpson, DN Wijeysundera, H Clarke, KS Ladha. Cannabis use among pregnant women under different legalization frameworks in the United States. American Journal of Drug and Alcohol Abuse, 2022. [DOI | PubMed]
- M Vanstone, J Panday, A Popoola, S Taneja, D Greyson, SD McDonald, R Pack, M Black, B Murray-Davis, E Darling. Pregnant people’s perspectives on cannabis use during pregnancy: A systematic review and integrative mixed-methods research synthesis. Journal of Midwifery & Women’s Health, 2022. [DOI]
- M Vanstone, S Taneja, A Popoola, J Panday, D Greyson, R Lennox, SD McDonald. Reasons for cannabis use during pregnancy and lactation: A qualitative study. CMAJ: Canadian Medical Association Journal = Journal De l’Association Medicale Canadienne, 2021. [DOI | PubMed]
- V Vastis, S Vincent, TD Metz, AK Shea. Are Canadian cannabis dispensaries counselling pregnant women appropriately. Journal of Obstetrics and Gynaecology Canada, 2021. [DOI | PubMed]
- Venditti, B. (2024). Mapped: Countries where recreational cannabis is legal. Visual Capitalist. https://www.visualcapitalist.com/mapped-countries-where-recreational-cannabis-is-legal/
- A Weber, B Miskle, A Lynch, S Arndt, L Acion. Substance use in pregnancy: Identifying stigma and improving care. Substance Abuse Rehabilitation, 2021. [DOI | PubMed]
- K Woodruff, KA Scott, SCM Roberts. Pregnant people’s experiences discussing their cannabis use with prenatal care providers in a state with legalized cannabis. Drug and Alcohol Dependence, 2021. [DOI | PubMed]
- KC Young-Wolff, SR Adams, SE Alexeeff, Y Zhu, E Chojolan, NE Slama, MB Does, LD Silver, D Ansley, CL Castellanos, LA Avalos. Prenatal cannabis use and maternal pregnancy outcomes. JAMA Internal Medicine, 2024. [DOI | PubMed]
- KC Young-Wolff, TR Foti, A Green, A Altschuler, MB Does, M Jackson-Morris, SR Adams, D Ansley, A Conway, N Goler, MN Mian, E Iturralde. Perceptions about cannabis following legalization among pregnant individuals with prenatal cannabis use in California. JAMA Network Open, 2022. [DOI | PubMed]
- KC Young-Wolff, A Green, A Altschuler, MB Does, M Jackson-Morris, SR Adams, D Ansley, A Conway, N Goler, K Skelton, TR Foti. Intentions to use cannabis postpartum: A qualitative study of pregnant individuals who used cannabis during early pregnancy. Journal of Women’s Health, 2024. [DOI | PubMed]