
Intergenerational transmission of maternal childhood maltreatment, prenatal substance exposure, and internalizing and externalizing symptoms in early adolescence at age 12
Abstract
Background:
Few studies have examined the intergenerational impact of maternal childhood maltreatment (MCM) in the context of prenatal substance exposure (PSE). This study investigates whether PSE is part of the pathway of MCM or an independent risk factor affecting offspring psychopathology.
Methods:
Participants were 284 birth mother–child (44% male) dyads, primarily Black, low‐income, enrolled at birth. Exposure to alcohol, tobacco, marijuana, or cocaine in utero was assessed at 1 month postpartum. MCM was assessed at child age 4, and maternal psychological distress and offspring maltreatment at child age 10. Mother‐ and child‐reported internalizing and externalizing symptoms were assessed at child age 12 using the Child Behavior Checklist and the Youth Self‐Report. Structural equation modeling was conducted to test sequential mediation pathways examining the direct and indirect associations of MCM with child internalizing and externalizing symptoms via PSE, maternal psychological distress, and offspring maltreatment, adjusting for covariates.
Results:
MCM was directly related to adolescent‐reported internalizing and externalizing symptoms, whereas PSE was directly related to adolescent‐reported externalizing symptoms. MCM and PSE were indirectly related to mother‐reported internalizing and externalizing symptoms via maternal psychological distress. Only PSE was related to offspring maltreatment at 10 years, and offspring maltreatment was related to both mother‐ and adolescent‐reported internalizing and externalizing symptoms at 12 years.
Conclusions:
MCM and PSE may increase offspring vulnerability to psychopathology, highlighting the importance of evaluating historical risks that mothers may transmit from their own childhood maltreatment and prenatal substance use in assessing offspring psychopathology.
Article type: Research Article
Keywords: Intergenerational transmission of maltreatment, prenatal substance exposure, internalizing symptoms, externalizing symptoms, early adolescence
Affiliations: College of Social Work University of Utah Salt Lake City UT USA; Department of Social Work, College of Nursing and Professional Disciplines University of North Dakota Grand Forks ND USA; Jack, Joseph and Morton Mandel School of Applied Social Sciences Case Western Reserve University Cleveland OH USA; Department of Population and Quantitative Health Sciences, School of Medicine Case Western Reserve University Cleveland OH USA
License: © 2025 The Author(s). Journal of Child Psychology and Psychiatry published by John Wiley & Sons Ltd on behalf of Association for Child and Adolescent Mental Health. CC BY 4.0 This is an open access article under the terms of the http://creativecommons.org/licenses/by/4.0/ License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Article links: DOI: 10.1111/jcpp.70030 | PubMed: 40791072 | PMC: PMC12812793
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (314 KB)
Introduction
Child maltreatment is a pervasive and serious public health problem. In the United States, over 3 million children were subjects of child maltreatment reports in 2023; of those, 16% had evidence of maltreatment (US Department of Health & Human Services, ref. 2025). It is estimated that, before age 18, more than one third of all US children (37.4%) are the subjects of investigated child maltreatment reports (Kim, Wildeman, Jonson‐Reid, & Drake, ref. 2017), and 1 in 8 of those reported (12.5%) are substantiated by Child Protective Services (Wildeman et al., ref. 2014).
While the pernicious impact of child maltreatment has been extensively documented across multiple domains of mental (Danese & Widom, ref. 2023; McLaughlin, Colich, Rodman, & Weissman, ref. 2020; Min, Farkas, Minnes, & Singer, ref. 2007) and physical health (Grummitt et al., ref. 2021; Min, Minnes, Kim, & Singer, ref. 2013), its effects may also cut across generations (e.g., Buss et al., ref. 2017; Min, Singer, Minnes, Kim, & Short, ref. 2013; Moog et al., ref. 2023; Uy et al., ref. 2023). Children of mothers who had themselves experienced childhood maltreatment are at elevated risk of exposure to higher maternal psychological distress (Harris et al., ref. 2023; Humphreys et al., ref. 2020; Minnes et al., ref. 2008) and harsh discipline and maltreatment (Madigan et al., ref. 2019; Plant, Jones, Pariante, & Pawlby, ref. 2017), contributing to emotional and behavioral problems (Kim et al., ref. 2024; Ma et al., ref. 2022; Negriff, Palmer Molina, & Hackman, ref. 2020). However, few studies have examined the intergenerational impact of maternal childhood maltreatment (MCM) in the context of prenatal substance use, despite their well‐established association (Elliott et al., ref. 2014; Racine, McDonald, Chaput, Tough, & Madigan, ref. 2020). Only one cross‐sectional study to date (Warmingham et al., ref. 2024) has examined both MCM and prenatal substance (alcohol, tobacco, marijuana, and cocaine) exposure (PSE). That study reported that both MCM and PSE were associated with offspring maltreatment, which was associated with greater mother‐reported externalizing symptoms in adolescents. MCM was directly related to mother‐reported internalizing symptoms. However, this study was limited to girls, with less than 10% of mothers reporting prenatal substance use. Explicating the roles of PSE and the postnatal developmental environment as intergenerational risk processes of MCM is crucial for effective interventions and maximizing benefits for children.
Maternal childhood maltreatment, PSE, and risk processes to offspring psychopathology
Childhood maltreatment alters the structure and function of stress‐susceptible brain regions, such as the hypothalamic–pituitary–adrenal axis, affecting afflicted individuals’ ability to regulate stress and emotion (Teicher, Samson, Anderson, & Ohashi, ref. 2016); thus, increasing the risk of developing psychopathology and health‐compromising behaviors including substance use (Hughes et al., ref. 2017; Norman et al., ref. 2012; Rogers et al., ref. 2022). Childhood maltreatment has been associated with an earlier age of onset of alcohol and drug use (Hamburger, Leeb, & Swahn, ref. 2008; Kerr et al., ref. 2009), daily tobacco smoking at ages 22–24 (Topitzes, Mersky, & Reynolds, ref. 2010), and daily cannabis use and dependence at age 21 (Mills, Kisely, Alati, Strathearn, & Najman, ref. 2017). These substance‐using behaviors may continue during pregnancy (Chung et al., ref. 2010; Towers et al., ref. 2020). The 2023 National Survey on Drug Use and Health estimated that 9.4% of pregnant women used tobacco, 8.4% used alcohol, and 4.9% used illicit drugs including marijuana, opioids, and cocaine during the past month, with polysubstance use common among illicit drug‐using women (Substance Abuse and Mental Health Services Administration, ref. 2024).
PSE interferes with fetal brain development by altering neurotransmitter systems in the prefrontal cortex, affecting emotional and behavioral arousal and regulation and stress response (Ross, Graham, Money, & Stanwood, ref. 2015), which may increase vulnerability to psychopathology (Eiden, Perry, Ivanova, & Marcus, ref. 2023). Mounting evidence, although mixed, indicates a link between PSE and the development of psychopathology. Greater prenatal alcohol exposure was related to internalizing and externalizing symptoms in a meta‐analysis of six longitudinal cohorts (Jacobson et al., ref. 2021); prenatal tobacco exposure was associated with suboptimal developmental trajectories of internalizing symptoms in poly‐drug exposed children (Min et al., ref. 2021) and with conduct problems using meta‐analyses of 25 studies (Ruisch, Dietrich, Glennon, Buitelaar, & Hoekstra, ref. 2018); prenatal marijuana/cannabis exposure was associated with more aggressive behavior at age 5 (Keim et al., ref. 2024) and increased teacher‐ and child‐reported externalizing symptoms at ages 7–9 in a population‐based birth cohort (El Marroun et al., ref. 2019); and prenatal cocaine exposure was related to teacher‐ and caregiver‐rated externalizing symptoms at ages 7, 9, 11, and 13 years (Bada et al., ref. 2011) and to adolescents’ self‐rated externalizing symptoms at ages 12 and 15 years (Min, Minnes, Yoon, Short, & Singer, ref. 2014). It is important to note that the effects of PSE are highly variable depending on the specific dosage, chronicity, gestational timing of the exposure, and co‐exposure to other substances (Eiden et al., ref. 2023), contributing to the inconsistent findings.
Continuing substance use post pregnancy can also compromise parenting ability (Hatzis, Dawe, Harnett, & Loxton, ref. 2019). Substance use may offset reward systems in the brain, making parent–child interaction less rewarding and pleasant (Rutherford et al., ref. 2021). Maternal psychological functioning has been considered a main mechanism connecting MCM with children’s behavior (Cooke, Racine, Plamondon, Tough, & Madigan, ref. 2019). Maternal psychological distress may contribute to caregivers’ emotional unavailability, to a lack of consistent sensitive responses to children’s needs, and to the increased likelihood of coercive, maltreating parenting behaviors, elevating the risk for psychopathology in their children (Goodman et al., ref. 2011; Stith et al., ref. 2009). Multiple meta‐analyses have demonstrated that maternal psychological distress mediates the associations of MCM with offspring psychopathology (Loheide‐Niesmann, Riem, & Cima, ref. 2024; Zhang, Mersky, Gruber, & Kim, ref. 2023). Emerging evidence also suggests offspring maltreatment as a pathway linking MCM with offspring internalizing and externalizing symptoms in childhood (Plant et al., ref. 2017; Russotti, Warmingham, Handley, Rogosch, & Cicchetti, ref. 2021) and in adolescence (Kızıltepe & Irmak, ref. 2024; Warmingham et al., ref. 2024).
The current study
The current study examined associations among MCM, PSE, maternal psychological functioning, and adolescents’ internalizing and externalizing symptoms in an urban low‐income birth cohort of boys and girls. We modeled intergenerational risk processes that may elucidate pathways from MCM to offspring psychopathology, while specifying PSE as a potential mediator of MCM, directly and indirectly associated with offspring psychopathology through maternal psychological distress and parenting behavior. Our study examined the role of PSE in the context of intergenerational transmission of MCM, testing whether PSE is part of the pathway of MCM or an independent risk factor that increases child vulnerability to psychopathology. We utilized both maternal and adolescent reports to assess internalizing and externalizing symptoms more comprehensively given the well‐documented discrepancy across informants (De Los Reyes et al., ref. 2015; Khoury et al., ref. 2022). Relevant confounders of MCM and adolescents’ psychopathology were assessed, including maternal education (Min et al., ref. 2007), child sex (Endendijk et al., ref. 2017), and quality of home environment and ecological resources as markers characterizing the socio‐economic developmental context (Min et al., ref. 2024; St‐Laurent, Dubois‐Comtois, Milot, & Cantinotti, ref. 2019). We hypothesized that (1) more severe MCM would be associated with higher levels of PSE, (2) both MCM and PSE would be associated with increased maternal psychological distress and maltreating parenting behavior, and (3) these maternal factors would be related to greater internalizing and externalizing symptoms in their offspring.
Methods
Participants
The present study included 284 birth mother–child dyads from a birth cohort recruited between September 1994 and June 1996 at an urban teaching hospital in the Midwest USA for a prospective study on the developmental effects of prenatal cocaine exposure (Minnes et al., ref. 2014; Singer, Albert, Minnes, Min, & Kim, ref. 2024). Pregnant women at high risk for drug use (e.g., lack of prenatal care, behaviors suggesting intoxication, self‐admitted drug use) were given drug toxicology screenings per hospital policy. Mothers with severe mood disorders or schizophrenia, HIV positive status, chronic medical illness, or low intellectual functioning indicated in medical charts were excluded, as were infants with Down syndrome, fetal alcohol syndrome, or congenital heart defects. A total of 404 birth mothers and their newborns were enrolled at birth. Of the 404 mothers, 302 mothers were assessed for childhood maltreatment at 4 years postpartum, and 12 children died by the 12‐year assessment. The present study utilizes data from 284 birth mother–child dyads with complete data on MCM, PSE, and child behavioral assessment at age 12 years. Compared to the 120 mothers who were not included, the 284 participating mothers were more likely to have prenatal care visits (76% vs. 89%) and less likely to smoke cigarettes (75% vs. 62%) and to use cocaine (64% vs. 47%) during pregnancy; and their children were less likely to have low birth weight (<2,500 g; 35% vs. 23%), all p‘s ≤ .01. No other differences were found.
The 284 mothers and their biological children (130 boys, 154 girls) were primarily Black (n = 235, 83%) with low socioeconomic status (SES; n = 277, 98%). At delivery, the mean (SD) maternal age was 27.6 (5.30), range 18–41, with 13% (n = 38) being married. Thirty‐nine percent of mothers (n = 112) had not finished high school, with a mean (SD) of 11.74 (1.54) years of education. About one‐third of mothers (n = 95) reported sexual abuse; 29% (n = 81) physical abuse, 23% (n = 64) emotional abuse, 30% (n = 86) emotional neglect, and 28% (n = 80) physical neglect. More than half (n = 157) reported at least one type of maltreatment, 37% (n = 106) more than one type of maltreatment, and 7% (n = 13) all five types of maltreatment. Urine, infant meconium analyses, or self‐report indicated that 243 (85%) mothers used at least one substance during pregnancy: 134 (47%) used cocaine, 171 (60%) cigarettes, 212 (75%) alcohol, and 81 (28%) marijuana. Two‐thirds of the mothers (n = 186) used two or more substances during pregnancy, including most (96%) mothers who used cocaine.
Procedure
The Institutional Review Board of the participating hospital approved the study. The initial screenings and enrollment were conducted in the hospital. The follow‐up assessments were conducted at the university‐based research lab at 1, 6, and 12 months and 2, 4, 6, 9, 10, 11, and 12 years of age postpartum by separate examiners blind to PSE. Data in the present study were taken from assessments conducted when the children were 1 month (PSE), 4 (MCM), 10 (maternal psychological distress and offspring maltreatment), and 12 years of age (offspring psychopathology). Parental written informed consent was collected at each visit, with child assent beginning at age 9. A Certificate of Confidentiality (DA‐98‐91), exempting the study from legislative, judicial, or administrative attempts to obtain confidential information, was obtained from the Department of Health and Human Services. All participants were compensated with a monetary stipend, lunch, and/or transportation costs.
Measures
Maternal childhood maltreatment (MCM)
Maternal childhood abuse and neglect were assessed using the Childhood Trauma Questionnaire (CTQ; Bernstein & Fink, ref. 1998), a 28‐item self‐report inventory of emotional, physical, and sexual abuse, and emotional and physical neglect. Items were rated on a 5‐point scale according to frequency (1 = never true to 5 = very often true) and summed to yield a total score for each maltreatment, with higher scores indicating greater severity. For descriptive purposes, scores indicating moderate to severe levels of maltreatment (>12 in emotional abuse, >9 in physical abuse and neglect, >7 in sexual abuse, and >14 in emotional neglect; Bernstein & Fink, ref. 1998) were used to dichotomize the CTQ subscales. MCM was specified as a latent variable with the five continuous subscales, with the measurement errors of the two observed neglect variables being correlated given a substantial correlation between them.
Prenatal substance exposure (PSE)
At the newborn visit, birth mothers reported the amount and frequency of drug use for the month prior to and for each trimester of pregnancy using a Timeline Follow Back method (Singer et al., ref. 2002). For cocaine use, the number of rocks consumed and the amount of money spent on cocaine per day were recalled and computed to a standard unit of cocaine, equivalent to $20 worth of crack cocaine. The number of drinks of beer, wine, or hard liquor per week, with each drink equivalent to 0.5 oz. of absolute alcohol, was recorded. The number of tobacco cigarettes and marijuana joints smoked per day was collected. For each drug, the frequency of use was rated on a Likert‐type scale (0 = not at all to 7 = daily use) to indicate the average number of days per week of drug use, except for cigarettes computed as the number smoked per day. PSE was specified as a latent variable with four indicators reflecting the amount of alcohol, tobacco, marijuana, and cocaine used due to substantial correlations between them.
Maternal psychological distress
At the 10‐year visit, maternal psychological distress was assessed with the Brief Symptom Inventory (Derogatis, ref. 1992), a widely used 53‐item self‐report standardized assessment of psychological symptoms experienced in the past 7 days such as depression, anxiety, and hostility. Items were rated on a 5‐point scale, with higher scores indicating greater distress. The global severity index (GSI), the average rating of all 53 items, was used.
Maternal offspring maltreatment
At the 10‐year visit, offspring maltreatment was assessed with the Parent–Child Conflict Tactics Scale (PCCTS; Straus, Hamby, Finkelhor, Moore, & Runyan, ref. 1998), a parent‐report on parenting behaviors related to child maltreatment. The psychological aggression scale assesses verbal and emotional abuse (5 items, e.g., “shouted, yelled, screamed”). The physical assault scale includes corporal punishment (5 items, e.g., “spanked on the bottom with a bare hand”), severe assault (4 items, e.g., “Threw or knocked down”), and very severe assault (4 item, e.g., “grab around the neck and choked”). Items were rated on a 5‐point scale according to their frequency, 0 = never, 1 = once or twice in the past year, 2 = 3–10 times in the past year, 3 = 11 or more times in the past year, 4 = not in the past year, but it happened before, which was recoded to: 0 = never, 1 = not in the past year, but it happened before, 2 = once or twice in the past year, 6 = 3–10 times in the past year, 15 = 11 or more times in the past year, using the midpoint for the original category 2 and 3 (Straus et al., ref. 1998). The total score of physical assaults was calculated using weights to account for the severity by multiplying 2 for the severe assault and 3 for very severe assault (Straus et al., ref. 1998). Higher scores indicate greater maltreatment. It was specified as a latent variable with the two subscales.
Offspring internalizing and externalizing symptoms
At the 12‐year visit, child behaviors were assessed using the Child Behavior Checklist for ages 6–18 (CBCL) and the Youth Self‐Report (YSR; Achenbach & Rescorla, ref. 2001). The CBCL is a 112‐item parent rating, and the YSR is a 105‐item child self‐rating, both designed to assess emotional, behavioral, and social problems of children in the last 6 months. Standardized T‐scores of internalizing (i.e., withdrawn, somatic complaints, and anxious/depressed) and externalizing (i.e., aggression and delinquency) behaviors were used, with higher scores indicating greater symptoms.
Covariates
Maternal (age at delivery, race, and education) and child characteristics (sex, race, gestational age, and birth weight) were retrieved from hospital birth records and verified at the 1‐month postpartum visit. SES was assessed using the Hollingshead Two‐Factor Index (Hollingshead, ref. 1971) at the 1‐month postpartum visit. The quality of the caregiving environment was assessed at age 9 via the caregiver report using the Home Observation of the Environment (Caldwell & Bradley, ref. 1979). Ecological resources and support were assessed at age 12 using the External Assets subscale of the Developmental Assets Profile (Search Institute, ref. 2005), a youth self‐report (ages 12–18) with a possible range of 0–30. Higher scores indicate greater assets.
Data analysis
Data positively skewed were normalized using a log transformation (the four indicators of PSE and GSI) or square root transformation (physical aggression). Distributional characteristics were reported by the variables’ original distribution, with normalized data used in bivariate and multivariate analyses. Bivariate associations between study variables were assessed using zero‐order Pearson correlations.
Structural equation modeling was conducted using Mplus 8.4 to evaluate sequential mediation pathways examining the direct and indirect associations of MCM and PSE with child internalizing and externalizing symptoms at age 12. To account for commonalities among the endogenous variables representing maternal functioning (maternal psychological distress and maltreating parenting behavior) and child psychopathology (maternal and adolescent reports), all within‐time cross‐domain correlations were specified. Direct paths from MCM and PSE to offspring internalizing and externalizing symptoms were specified to indicate other unmeasured mediators of MCM and PSE. The maximum likelihood method was used to fit the models. Model fit was examined using the chi‐square (χ 2) goodness‐of‐fit test, the Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR) indices. Values ≥.95 for CFI and TLI, ≤.06 for RMSEA, and ≤.08 for SRMR indicate a good fit (Hu & Bentler, ref. 1998). Missing data on maternal psychological distress and parenting behavior (~21%) were estimated using full information maximum likelihood, allowing use of all available information from the observed data (Enders & Bandalos, ref. 2001). With no missing covariates, the analytical model was based on all 284 birth mother–child dyads. The significance of the indirect association was tested using a bootstrap method based on 1,000 resamples (Preacher & Hayes, ref. 2008). Model comparisons were conducted using the χ 2 difference (Δχ 2) test (Kline, ref. 1998). Two‐sided p < .05 indicated statistical significance. For ease of interpretation, parameter estimates are presented in standardized form.
Results
Table 1 provides descriptive statistics, internal consistency (α), and bivariate correlations between key observed variables. Maternal and adolescent ratings of internalizing and externalizing symptoms were only moderately correlated (r = .25 on internalizing and .34 on externalizing), supporting our analytical decision not to aggregate the maternal and adolescent ratings but to examine them separately.
Table 1: Descriptive statistics and correlations (r) among key observed variables in the path model
| Maternal | Child | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | |
| 1. Maternal education | – | −.19 | −.08 | −.10 | −.24 | −.21 | −.12 | −.21 | −.07 | −.23 | −.11 | .08 | .12 | .09 | −.14 | −.02 | −.09 | .00 | −.06 |
| Maternal CTQ | |||||||||||||||||||
| 2. Emotional abuse | – | .74 | .52 | .61 | .52 | .06 | .18 | .15 | .09 | .32 | .11 | .10 | −.01 | .02 | .21 | .20 | .12 | .15 | |
| 3. Physical abuse | – | .52 | .49 | .50 | .07 | .14 | .12 | .06 | .19 | .12 | .15 | −.04 | −.00 | .15 | .12 | .12 | .15 | ||
| 4. Sexual abuse | – | .36 | .40 | .03 | .13 | .11 | .04 | .22 | .08 | .14 | −.04 | −.06 | .20 | .23 | .10 | .13 | |||
| 5. Emotional neglect | – | .62 | .05 | .11 | .05 | .10 | .22 | .04 | .08 | −.02 | −.01 | .15 | .21 | .07 | .11 | ||||
| 6. Physical neglect | – | −.02 | .10 | .14 | .04 | .09 | −.06 | −.04 | .00 | .02 | .04 | .04 | .03 | .06 | |||||
| PSE | |||||||||||||||||||
| 7. Alcohola | – | .48 | .15 | .55 | .19 | .12 | .12 | −.07 | −.05 | −.00 | .10 | .08 | .14 | ||||||
| 8. Tobaccoa | – | .25 | .47 | .24 | .06 | .04 | −.09 | .05 | .05 | .15 | −.03 | .10 | |||||||
| 9. Marijuanaa | – | .16 | .11 | .04 | .05 | .00 | .03 | .07 | −.05 | .03 | .12 | ||||||||
| 10. Cocainea | – | .19 | .16 | .06 | −.06 | −.05 | .02 | .14 | −.02 | .18 | |||||||||
| 11. Psychological distressa | – | .39 | .27 | −.00 | .04 | .45 | .39 | .13 | .10 | ||||||||||
| PCCTS | |||||||||||||||||||
| 12. Psychological | – | .69 | .17 | −.12 | .27 | .36 | .14 | .19 | |||||||||||
| 13. Physicalb | – | .13 | −.01 | .17 | .27 | .14 | .12 | ||||||||||||
| 14. Child sex | – | −.12 | .10 | .11 | .16 | .10 | |||||||||||||
| 15. DAP external assets | – | −.09 | −.13 | −.29 | .37 | ||||||||||||||
| 16. CBCL internalizing | – | .66 | .25 | .12 | |||||||||||||||
| 17. CBCL externalizing | – | .22 | .34 | ||||||||||||||||
| 18. YSR internalizing | – | .54 | |||||||||||||||||
| 19. YSR externalizing | – | ||||||||||||||||||
| Mean (n) | 11.74 | 9.45 | 8.75 | 8.89 | 11.73 | 8.25 | 5.83 | 7.52 | 0.97 | 9.90 | 0.36 | 11.97 | 5.37 | (130) | 21.37 | 48.00 | 49.96 | 53.18 | 49.04 |
| SD (%) | 1.54 | 5.08 | 4.80 | 6.20 | 5.49 | 3.99 | 14.61 | 10.42 | 3.65 | 26.87 | 0.46 | 10.95 | 7.96 | (45.8) | 4.49 | 10.68 | 12.18 | 9.93 | 10.16 |
| α | .85 | .84 | .94 | .85 | .70 | – | – | – | – | .95 | .68 | .69 | – | .90 | .88 | .93 | .86 | .87 | |
Bold indicates significance at p < .05; Skewed data were normalized for bivariate and multivariate analyses using alog transformation or bsquare root transformation, with raw data reported for mean and SD. CBCL, Child Behavioral Checklist; CTQ, Childhood Trauma Questionnaire; DAP, Developmental Asset Profile; PCCTS, Parent–Child Conflict Tactic Scale; PSE, Prenatal Substance Exposure; YSR, Youth Self‐Report.
Model estimation
The initial, saturated model included: (1) paths from MCM to all three mediators and the four indicators of mother‐ and adolescent‐reported internalizing and externalizing symptoms at age 12; (2) paths from PSE to the other two mediators and the four indicators of internalizing and externalizing symptoms; (3) paths from maternal psychological distress and offspring maltreatment to the four indicators of internalizing and externalizing symptoms; (4) correlations between maternal psychological distress and offspring maltreatment at age 10; (5) correlations ndbetween mother‐ and adolescent‐reported internalizing and externalizing symptoms; and (6) correlations between all exogenous (i.e., MCM and all covariates) variables. This initial model produced a good model fit, χ 2 (111) = 152.61, p = .005, CFI = 0.972, TLI = 0.958, RMSEA = 0.036 (90% CI = 0.020–0.050), SRMR = 0.044. To achieve a more parsimonious model, path coefficients with a significance level of p ≥.15 were set to zero (Hosmer, Lemeshow, & Sturdivant, ref. 2013), χ 2 (126) = 167.62, p = .008, CFI = 0.972, TLI = 0.963, RMSEA = 0.034 (90% CI = 0.018–0.047), SRMR = 0.047, yielding an insignificant difference in model fit, Δχ 2 (15) = 15.01, p = .45. This reduced model was accepted as the final model (Figure 1).
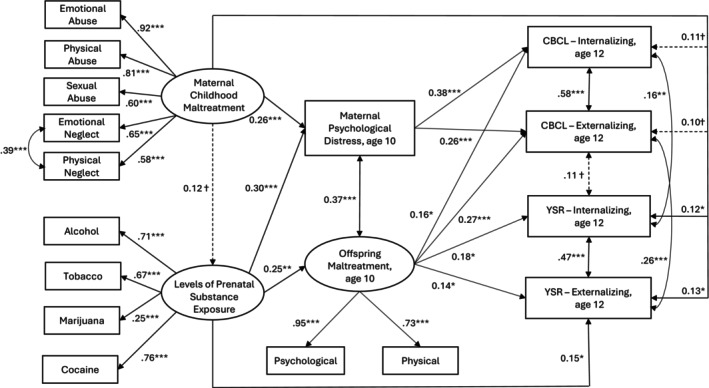
Figure 1 indicates the least marginally significant (p < .10) path coefficients. Adjusting for relevant covariates, MCM was related to maternal psychological distress at age 10 (β = .26, SE = .070, p < .001) but was not related to PSE (β = .12, SE = .073, p = .099) nor offspring maltreatment at age 10 (β = .13, SE = .089, p = .135). Maternal psychological distress was related to mother‐reported internalizing (β = .38, SE = .081, p < .001) and externalizing symptoms at age 12 (β = .26, SE = .078, p = .001). MCM was indirectly, via psychological distress, related to mother‐reported internalizing (indirect effect of MCM, β = .098, SE = .035, p = .005) and externalizing symptoms (indirect effect of MCM, β = .066, SE = .027, p = .012). MCM was also directly related to adolescent‐reported internalizing (β = .12, SE = .057, p = .036) and externalizing symptoms at age 12 (β = .13, SE = .054, p = .014). PSE was related to maternal psychological distress (β = .30, SE = .084, p < .001) and offspring maltreatment (β = .25, SE = .098, p = .011). Similar to MCM, PSE was indirectly, via maternal psychological distress, related to mother‐reported internalizing (indirect effect of PSE, β = .113, SE = .045, p = .012) and externalizing symptoms (indirect effect of PSE, β = .077, SE = .035, p = .027). Although individual paths from PSE to offspring maltreatment at age 10 and from offspring maltreatment to mother‐ and adolescent‐reported internalizing and externalizing symptoms at age 12 were all significant, the indirect effect of PSE via offspring maltreatment did not reach significance (p‘s ≥ .067). PSE was also directly related to higher adolescent‐reported externalizing symptoms (β = .15, SE = .062, p = .015). Offspring maltreatment was related to both mother‐ and adolescent‐reported internalizing (β = .16, SE = .082, p = .048 on the CBCL, β = .18, SE = .073, p = .015 on the YSR) and externalizing symptoms (β = .27, SE = .082, p = .001 on the CBCL, β = .14, SE = .068, p = .036 on the YSR). Maternal psychological distress and offspring maltreatment were correlated (r = .37, p < .001); the two indicators of internalizing symptoms were correlated (r = .16, p = .008) and so were the two indicators of externalizing symptoms (r = .26, p < .001). In terms of covariates, higher maternal education was related to both MCM (r = − .20, p < .001) and PSE (β = −.25, SE = .075, p = .001). Boys experienced greater maltreatment than girls (β = .174, SE = .067, p = .009). Greater external assets were related to fewer adolescent‐reported internalizing (β = −.26, SE = .057, p < .001) and externalizing symptoms (β = −.34, SE = .055, p < .001). Table 2 summarizes the direct and indirect associations of MCM, PSE, maternal psychological distress, and offspring maltreatment with offspring internalizing and externalizing symptoms.
Table 2: Decomposition of the standardized estimates of maternal childhood maltreatment on offspring psychopathology at age 12
| CBCL | YSR | |||||||
|---|---|---|---|---|---|---|---|---|
| Internalizing | Externalizing | Internalizing | Externalizing | |||||
| β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | |
| MCM | ||||||||
| Direct | .107 (.057) | .063 | .095 (.051) | .065 | .119 (.057) | .036 | .132 (.054) | .014 |
| Indirect | .122 (.040) | .002 | .124 (.039) | .002 | .024 (.022) | .287 | .041 (.023) | .069 |
| Total | .229 (.062) | <.001 | .219 (.055) | <.001 | .142 (.055) | .010 | .173 (.053) | .001 |
| Levels of PSE | ||||||||
| Direct | −.128 (.079) | .102 | .035 (.077) | .650 | −.041 (.071) | .564 | .150 (.062) | .015 |
| Indirect | .154 (.053) | .004 | .144 (.051) | .005 | .044 (.027) | .101 | .035 (.022) | .104 |
| Total | .024 (.072) | .735 | .179 (.073) | .014 | .003 (.069) | .966 | .185 (.064) | .004 |
| Maternal psychological distressjcpp70030-note-0004 | ||||||||
| Direct | .375 (.081) | <.001 | .255 (.078) | .001 | – | – | – | – |
| Indirect from MCM | .098 (.035) | .005 | .066 (.027) | .012 | – | – | – | – |
| Indirect from PSE | .113 (.045) | .012 | .077 (.035) | .027 | – | – | – | – |
| Indirect from MCM → PSE | .014 (.011) | .211 | .009 (.008) | .242 | – | – | – | – |
| Offspring maltreatment | ||||||||
| Direct | .163 (.082) | .048 | .269 (.082) | .001 | .177 (.073) | .015 | .142 (.068) | .036 |
| Indirect from MCM | .022 (.021) | .292 | .036 (.027) | .181 | .023 (.020) | .249 | .019 (.016) | .250 |
| Indirect from PSE | .040 (.028) | .146 | .067 (.036) | .067 | .044 (.101) | .101 | .035 (.022) | .104 |
| Indirect from MCM → PSE | .005 (.005) | .296 | .008 (.007) | .238 | .005 (.005) | .257 | .004 (.004) | .270 |
CBCL, Child Behavior Checklist; MCM, maternal childhood maltreatment; PSE, prenatal substance exposure; YSR, Youth Self‐Report.
Direct paths from maternal psychological distress to internalizing symptoms and to externalizing symptoms on the YSR were removed in the final model due to the lack of significance (p ≥ .15). Estimates were adjusted for maternal education on MCM and PSE, child sex on offspring maltreatment, and external assets on YSR internalizing and externalizing symptoms.
Discussion
This study demonstrated that both MCM and PSE increased offspring vulnerability to psychopathology directly and indirectly in a low‐income urban sample of prenatal cocaine/polydrug‐using mothers and their children. However, PSE was not a pathway underlying an intergenerational risk process of MCM to offspring psychopathology. Instead, independent of MCM, PSE was directly related to higher adolescent‐reported externalizing symptoms even after maternal psychological distress and maltreating parenting behavior were considered, supporting the long‐lasting teratologic effects of PSE (Ross et al., ref. 2015). MCM was related to greater internalizing and externalizing symptoms in offspring, directly when adolescents were informants but indirectly via maternal psychological distress when mothers were informants, demonstrating the intergenerational effect of MCM regardless of informant while suggesting pathways varied by informant. These core findings integrate two separate yet interrelated lines of inquiry toward a more nuanced understanding of the intergenerational risk process, where both the history of MCM and PSE are additively associated with increased risk for developing psychopathology in offspring. The present study is one of the few studies to document the role of PSE in the context of intergenerational transmission of MCM and, to our knowledge, the first using a prospective birth cohort of children of mothers with varying degrees of childhood maltreatment and prenatal substance use.
Contrary to our hypothesis, a non‐significant, yet marginal (p = .099) relationship was found between MCM and PSE. This could be due to the relative lack of variability in PSE in our sample where the majority reported some levels of PSE. Also, given that almost all mothers were categorized as low SES with limited educational obtainments, PSE might be highly confounded with poverty and its related psychosocial factors such as domestic violence and drug‐using partners and friends (Min, Tracy, & Park, ref. 2014). Replication studies with a more balanced distribution in PSE may clarify the relationship of MCM with PSE.
In our model of multiple mediators with two markers reflecting maternal psychological functioning, only psychological distress was a significant mediator of both MCM and PSE on mother‐reported offspring outcomes. It underscores the well‐recognized pivotal impact of maternal psychological distress, regardless of its antecedents, that confers an increased risk of developing psychopathology in offspring even after accounting for maltreating parenting behaviors (e.g., Plant et al., ref. 2017). Maternal offspring maltreatment was associated only with PSE, not with MCM, indicating that maltreatment was likely a function of PSE, rather than MCM, in this sample with high prevalence of both MCM and PSE. It is noteworthy that MCM was not related to PSE but was related to adolescent‐reported internalizing and externalizing symptoms with similar effect sizes (Cohen, ref. 1992), a finding that warrants replication. Despite the relationships of maternal offspring maltreatment with both mother‐ and adolescent‐reported internalizing and externalizing symptoms in offspring, offspring maltreatment did not emerge as a mediator of PSE. Given the frequent co‐occurrence of maternal psychological distress and offspring maltreatment, our simultaneous analysis of multiple associated pathways suggests that the intergenerational transmission of MCM can be better explained by maternal psychological distress, highlighting maternal psychological distress as a priority for interventions aimed at counteracting the intergenerational transmission of risk.
The direct relationship of MCM with adolescent‐reported internalizing and externalizing symptoms may imply other intermediary risk mechanisms. Additional adverse life events (Fereidooni, Daniels, & Lommen, ref. 2024), lack of social support (Bosquet Enlow, Englund, & Egeland, ref. 2018), poor mother–child attachment (Alto et al., ref. 2021), accumulations of such psychosocial risks (Racine et al., ref. 2018), or epigenetic methylation (Monk, Spicer, & Champagne, ref. 2012) may account for the direct relationship apparent in our study, areas of consideration in future studies.
The findings need to be considered in light of limitations. First, the generalizability of our findings is limited to the characteristics of our cohort, which is urban, low‐income, and predominantly Black adolescents, where about half of their mothers used cocaine and other substances during pregnancy. Second, MCM was constructed as a latent variable to capture high correlations among multiple types of abuse and neglect. Given that abuse versus neglect could be differentially associated with different developmental domains and thus, with later caregiving behaviors (e.g., abuse linked to aggression whereas neglect to health problems and cognitive abilities; Usacheva, Choe, Liu, Timmer, & Belsky, ref. 2022), the observed associations of MCM with PSE and maternal psychological functioning could reflect abuse experience rather than neglect, a hypothesis that should be tested in future studies. Third, although the time reference of the CTQ guided mothers to recall their childhood, the temporal precedence of MCM (assessed at 4‐year postpartum) to PSE (assessed at childbirth) could be ambiguous. The use of a retrospective self‐report to assess MCM might have compromised its reliability due to potential memory errors or suppression (Rucklidge, Brown, Crawford, & Kaplan, ref. 2006). Nonetheless, retrospective self‐reports of childhood maltreatment have been shown to be stronger correlates of psychosocial outcomes than objectively assessed measures (Danese & Widom, ref. 2023; Latham et al., ref. 2021). Fourth, the measure of offspring maltreatment overlooked neglect and might not fully capture the effects from MCM and PSE. We also relied on maternal reports assessing offspring maltreatment, subjective to social desirability bias. The insignificant relationship of MCM with offspring maltreatment could be due to the limited measurement of offspring maltreatment or/and mothers’ tendency to underreport their maltreating behavior. Lastly, the significant indirect relationship of MCM via maternal psychological distress with maternal report of offspring internalizing and externalizing behaviors could be due to biases associated with a single informant through shared method variance as well as mothers’ cognitive biases, as psychologically distressed mothers tend to perceive their childhood and their children’s behavior more negatively (Najman et al., ref. 2001). Yet, it is these maternal perceptions that shape maternal responses and parenting practice, and thus, offspring psychopathology.
The notable strength of the present study includes controlling for single‐source bias and shared method variance. By simultaneously assessing maternal and adolescent reports on offspring psychopathology, we disentangled informant‐specific pathways from MCM to offspring psychopathology. The use of the Timeline Follow Back method enhanced recall accuracy in assessing PSE (Robinson, Sobell, Sobell, & Leo, ref. 2014). Adjusting for multiple prenatal and postnatal socioeconomic markers such as maternal education and ecological resources, often considered common etiological factors of MCM, PSE, and offspring psychopathology (Belsky, ref. 1993; Dixon, Browne, & Hamilton‐Giachritsis, ref. 2009), increased confidence in the findings.
In conclusion, PSE was not a pathway underlying intergenerational transmission of MCM to offspring psychopathology; although PSE was related to greater adolescent‐reported externalizing symptoms. Our findings demonstrate the complexity of intergenerational maltreatment, PSE, and the postnatal caregiving environment, underscoring the importance of evaluating historical risks that mothers may transmit from their own childhood maltreatment and prenatal substance use in assessing offspring psychopathology.
Ethics statement
Parental written informed consent and child assent have been appropriately obtained. Study procedures were approved by the University Hospitals Institutional Review Board (UHCMC 10‐89‐206; the date of approval 05/26/2006).
Key points
- What’s known: The impact of childhood maltreatment may cut across generations, extending its long‐term implications. Few studies examined the intergenerational impact of maternal childhood maltreatment in the context of prenatal substance use.
- What’s new: Both maternal childhood maltreatment and prenatal substance use increased offspring vulnerability to psychopathology at age 12 directly and indirectly in a low‐income urban sample. Maternal prenatal substance use was not a pathway underlying intergenerational transmission of childhood maltreatment; although maternal prenatal substance use was related to greater adolescent‐reported externalizing symptoms.
- What’s relevant: The current study highlights the importance of evaluating historical risks that mothers may transmit from their own childhood maltreatment and prenatal substance use when assessing offspring psychopathology.
References
- Achenbach, T. , & Rescorla, L. (2001). Manual for the ASEBA school‐age forms & profiles: An integrated system of multi‐informant assessment. Burlington, VT: Research Center for Children, Youth & Families.
- Developmental pathways from maternal history of childhood maltreatment and maternal depression to toddler attachment and early childhood behavioral outcomes.. Attachment & Human Development,, 2021. [PubMed]
- Preadolescent behavior problems after prenatal cocaine exposure: Relationship between teacher and caretaker ratings (Maternal Lifestyle Study).. Neurotoxicology and Teratology,, 2011. [PubMed]
- Etiology of child maltreatment: A developmental‐ecological analysis.. Psychological Bulletin,, 1993. [PubMed]
- Bernstein, D.P. , & Fink, L. (1998). Childhood Trauma Questionnaire Manual. San Antonio: The Psychological Corporation.
- Maternal childhood maltreatment history and child mental health: Mechanisms in intergenerational effects.. Journal of Clinical Child & Adolescent Psychology,, 2018. [PubMed]
- Intergenerational transmission of maternal childhood maltreatment exposure: Implications for fetal brain development.. Journal of the American Academy of Child & Adolescent Psychiatry,, 2017. [PubMed]
- Caldwell, B.M. , & Bradley, R.H. (1979). Home observation for measurement of the environment. Little Rock, AR: University of Arkansas at Little Rock.
- Risky health behaviors among mothers‐to‐be: The impact of adverse childhood experiences.. Academic Pediatrics,, 2010. [PubMed]
- A power primer.. Psychological Bulletin,, 1992. [PubMed]
- Maternal adverse childhood experiences, attachment style, and mental health: Pathways of transmission to child behavior problems.. Child Abuse & Neglect,, 2019. [PubMed]
- Associations between objective and subjective experiences of childhood maltreatment and the course of emotional disorders in adulthood.. JAMA Psychiatry,, 2023. [PubMed]
- The validity of the multi‐informant approach to assessing child and adolescent mental health.. Psychological Bulletin,, 2015. [PubMed]
- Derogatis, L.R. (1992). The Brief Symptom Inventory, Administration, Scoring & Procedures Manual‐II. Baltimore, MD: Clinical Psychometric Research, Inc.
- Patterns of risk and protective factors in the intergenerational cycle of maltreatment.. Journal of Family Violence,, 2009
- Prenatal substance exposure.. Annual Review of Developmental Psychology,, 2023
- Preconception and prenatal cannabis use and the risk of behavioural and emotional problems in the offspring; a multi‐informant prospective longitudinal study.. International Journal of Epidemiology,, 2019. [PubMed]
- The risk for persistent adult alcohol and nicotine dependence: The role of childhood maltreatment.. Addiction,, 2014. [PubMed]
- Gender differences in child aggression: Relations with gender‐differentiated parenting and parents’ gender‐role stereotypes.. Child Development,, 2017. [PubMed]
- The relative performance of full information maximum likelihood estimation for missing data in structural equation models.. Structural Equation Modeling: A Multidisciplinary Journal,, 2001
- Childhood maltreatment and revictimization: A systematic literature review.. Trauma, Violence & Abuse,, 2024
- Maternal depression and child psychopathology: A meta‐analytic review.. Clinical Child and Family Psychology Review,, 2011. [PubMed]
- Association of childhood adversity with morbidity and mortality in US adults: A systematic review.. JAMA Pediatrics,, 2021. [PubMed]
- Childhood maltreatment and early alcohol use among high‐risk adolescents.. Journal of Studies on Alcohol and Drugs,, 2008. [PubMed]
- Maternal childhood maltreatment history and child behavior problems: Developmental patterns and mediation via maternal depressive symptoms and parenting behavior.. Child Maltreatment,, 2023. [PubMed]
- An investigation of the impact of childhood trauma on quality of caregiving in high risk mothers: Does maternal substance misuse confer additional risk?. Child Psychiatry & Human Development,, 2019. [PubMed]
- Commentary on “the indiscrimination state of social class measurement”.. Social Forces,, 1971
- Hosmer, D.W. , Lemeshow, S. , & Sturdivant, R.X. (2013). Applied logistic regression. Hoboken: John Wiley & Sons, Inc.
- Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification.. Psychological Methods,, 1998
- The effect of multiple adverse childhood experiences on health: A systematic review and meta‐analysis.. The Lancet Public Health,, 2017. [PubMed]
- Child maltreatment and depression: A meta‐analysis of studies using the Childhood Trauma Questionnaire.. Child Abuse & Neglect,, 2020. [PubMed]
- Effects of prenatal alcohol exposure on cognitive and behavioral development: Findings from a hierarchical meta‐analysis of data from six prospective longitudinal US cohorts.. Alcoholism, Clinical and Experimental Research,, 2021. [PubMed]
- Prenatal cannabis exposure and executive function and aggressive behavior at age 5 years.. JAMA Pediatrics,, 2024. [PubMed]
- Childhood trauma and injection drug use among high‐risk youth.. Journal of Adolescent Health,, 2009
- Examining the unique contributions of parental and youth maltreatment in association with youth mental health problems.. Child Abuse & Neglect,, 2022. [PubMed]
- Lifetime prevalence of investigating child maltreatment among US children.. American Journal of Public Health,, 2017. [PubMed]
- Maternal childhood trauma and children’s developmental course of aggressive behavior from ages 4 to 12.. Psychology of Violence,, 2024. [DOI | PubMed]
- Intergenerational transmission of childhood maltreatment and offspring behavioral adjustment problems and competence.. Child Abuse & Neglect,, 2024. [PubMed]
- Kline, R.B. (1998). Principles and practice of structural equation modeling. New York: Guilford Press.
- Childhood maltreatment and poor functional outcomes at the transition to adulthood: A comparison of prospective informant‐and retrospective self‐reports of maltreatment.. Social Psychiatry and Psychiatric Epidemiology,, 2021. [PubMed]
- The impact of maternal childhood maltreatment on child externalizing behaviour and the mediating factors underlying this association: A three‐level meta‐analysis and systematic review.. European Child & Adolescent Psychiatry,, 2024. [PubMed]
- Mediators and moderators in the relationship between maternal childhood adversity and children’s emotional and behavioural development: A systematic review and meta‐analysis.. Psychological Medicine,, 2022. [PubMed]
- Testing the cycle of maltreatment hypothesis: Meta‐analytic evidence of the intergenerational transmission of child maltreatment.. Development and Psychopathology,, 2019. [PubMed]
- Mechanisms linking childhood trauma exposure and psychopathology: A transdiagnostic model of risk and resilience.. BMC Medicine,, 2020. [PubMed]
- Child maltreatment and cannabis use in young adulthood: A birth cohort study.. Addiction,, 2017. [PubMed]
- Prenatal substance exposure and developmental trajectories of internalizing symptoms: Toddlerhood to preadolescence.. Drug and Alcohol Dependence,, 2021. [PubMed]
- Prenatal cocaine exposure and self‐reported behavioral adjustments from ages 12 to 21: Environmental pathways.. Psychological Medicine,, 2024. [PubMed]
- Impact of childhood abuse and neglect on substance use and psychological distress in adulthood.. Journal of Traumatic Stress,, 2007. [PubMed]
- Pathways linking childhood maltreatment and adult physical health.. Child Abuse & Neglect,, 2013. [PubMed]
- Self‐reported adolescent behavioral adjustment: Effects of prenatal cocaine exposure.. Journal of Adolescent Health,, 2014
- Mediating links between maternal childhood trauma and preadolescent behavioral adjustment.. Journal of Interpersonal Violence,, 2013
- Impact of trauma symptomatology on personal networks among substance using women.. Drug and Alcohol Dependence,, 2014. [PubMed]
- The association of prenatal cocaine use and childhood trauma with psychological symptoms over 6 years.. Archives of Women’s Mental Health,, 2008
- Comparison of 12‐year‐old children with prenatal exposure to cocaine and non‐exposed controls on caregiver ratings of executive function.. Journal of Youth and Adolescence,, 2014. [PubMed]
- Linking prenatal maternal adversity to developmental outcomes in infants: The role of epigenetic pathways.. Development and Psychopathology,, 2012. [PubMed]
- Intergenerational transmission of the effects of maternal exposure to childhood maltreatment in the USA: A retrospective cohort study.. The Lancet Public Health,, 2023. [PubMed]
- Bias influencing maternal reports of child behaviour and emotional state.. Social Psychiatry and Psychiatric Epidemiology,, 2001. [PubMed]
- Parental exposure to childhood maltreatment and offspring’s mental health: Investigating pathways through parental adversity and offspring exposure to maltreatment.. Child Maltreatment,, 2020. [PubMed]
- The long‐term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta‐analysis.. PLoS Medicine,, 2012. [PubMed]
- Association between maternal childhood trauma and offspring childhood psychopathology: Mediation analysis from the ALSPAC cohort.. The British Journal of Psychiatry,, 2017. [PubMed]
- Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models.. Behavior Research Methods,, 2008. [PubMed]
- Maternal psychosocial risk profiles in pregnancy: Associations with postpartum maternal health and child outcomes.. Clinical Psychological Science,, 2018
- Maternal substance use in pregnancy: Differential prediction by childhood adversity subtypes.. Preventive Medicine,, 2020. [PubMed]
- Reliability of the timeline followback for cocaine, cannabis, and cigarette use.. Psychology of Addictive Behaviors,, 2014. [PubMed]
- Effects of multiple adverse childhood experiences on substance use in young adults: A review of the literature.. Drug and Alcohol Dependence,, 2022. [PubMed]
- Developmental consequences of fetal exposure to drugs: What we know and what we still must learn.. Neuropsychopharmacology,, 2015. [PubMed]
- Retrospective reports of childhood trauma in adults with ADHD.. Journal of Attention Disorders,, 2006. [PubMed]
- Maternal substance use during pregnancy and offspring conduct problems: A meta‐analysis.. Neuroscience & Biobehavioral Reviews,, 2018. [PubMed]
- Child maltreatment: An intergenerational cascades model of risk processes potentiating child psychopathology.. Child Abuse & Neglect,, 2021. [PubMed]
- Parenting and addictions: Current insights from human neuroscience.. Current Addiction Reports,, 2021. [PubMed]
- Search Institute . (2005). Developmental assets profile: User manual. Minneapolis, MN: Author.
- Infant behaviors, prenatal cocaine exposure, and adult intelligence.. JAMA Network Open,, 2024. [PubMed]
- Effects of cocaine/polydrug exposure and maternal psychological distress on infant birth outcomes.. Neurotoxicology and Teratology,, 2002. [PubMed]
- Risk factors in child maltreatment: A meta‐analytic review of the literature.. Aggression and Violent Behavior,, 2009
- Intergenerational continuity/discontinuity of child maltreatment among low‐income mother–child dyads: The roles of childhood maltreatment characteristics, maternal psychological functioning, and family ecology.. Development and Psychopathology,, 2019. [PubMed]
- Identification of child maltreatment with the Parent‐Child Conflict Tactics Scales: Development and psychometric data for a national sample of American parents.. Child Abuse & Neglect,, 1998. [PubMed]
- 2023 National Survey of Drug Use and Health (NSDUH) .. 2024
- The effects of childhood maltreatment on brain structure, function and connectivity.. Nature Reviews Neuroscience,, 2016. [PubMed]
- Child maltreatment and adult cigarette smoking: A long‐term developmental model.. Journal of Pediatric Psychology,, 2010. [PubMed]
- Psychosocial background history of pregnant women with opioid use disorder: A prospective cohort study.. American Journal of Perinatology,, 2020. [PubMed]
- Child Maltreatment 2023 . Available from:. 2025
- Testing the empirical integration of threat‐deprivation and harshness‐unpredictability dimensional models of adversity.. Development and Psychopathology,, 2022. [PubMed]
- Effects of maternal childhood trauma on child emotional health: Maternal mental health and frontoamygdala pathways.. Journal of Child Psychology and Psychiatry,, 2023. [PubMed]
- Investigating the associations between prenatal exposure to substances and intergenerational maltreatment and symptoms of psychopathology for adolescent girls from families with low income.. Child Abuse & Neglect,, 2024. [PubMed]
- The prevalence of confirmed maltreatment among US children, 2004 to 2011.. JAMA Pediatrics,, 2014. [PubMed]
- Intergenerational transmission of parental adverse childhood experiences and children’s outcomes: A scoping review.. Trauma, Violence & Abuse,, 2023