
CBD Disrupts Malme-3M Cell Metabolism via Glycolytic Shift and Redox Imbalance
Abstract
Background: Accumulating evidence suggests that cannabidiol (CBD) exerts variable effects on cancer cells that influence cellular activity, including growth. While anecdotal evidence abounds, mechanistic studies have lagged. Methods: Malme-3M cells derived from melanoma and less-aggressive BJ fibroblast cells were incubated with CBD. CE-MS mass spectroscopy was used to measure metabolite changes resulting from CBD treatment. Results: Data indicate a differential response between malignant Malme-3M cells and BJ fibroblasts with respect to metabolites critical for primary metabolic function. A significant reduction in TCA metabolites is seen with a corresponding increase in glycolytic output in the Malme-3M cell line. A similar reduction in TCA activity in BJ fibroblasts appears to differentially activate fatty acid oxidation. ATP is significantly reduced in the Malme-3M cells with a corresponding decrease in metabolites associated with redox maintenance. Conclusions: This is the first metabolomics analyses of malignant Malme-3M cells and less-aggressive BJ fibroblasts after pre-treatment with CBD. The data suggest that the CBD-induced metabolic perturbation could reprogram cellular metabolism and affect ATP production and redox maintenance of the more-aggressive Malme-3M cells.
Article type: Brief Report
Keywords: Malme-3M, BJ fibroblast, cannabidiol (CBD), redox, metabolism
Affiliations: Biome, Inc., Shinjuku 169-0051, Japan; Department of Medicine, University of Florida, 1600 SW Archer Rd., Gainesville, FL 32608, USA; xuyiling870@gmail.com (Y.X.); hans.ghayee@medicine.ufl.edu (H.G.); Human Metabolome Technologies, America, 24 Denby Road, Suite 217, Boston, MA 02134, USA; alex.buko@humanmetabolome.com
License: © 2025 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.3390/cimb47110928 | PubMed: 41296432 | PMC: PMC12651666
Relevance: Core topic: mentioned in title and keywords
Full text: PDF (1.1 MB)
1. Introduction
In recent years, the medical and scientific communities have witnessed a surge of interest in the potential therapeutic applications of cannabidiol (CBD), a non-psychoactive compound derived from the Cannabis sativa plant. Of the over 500 compounds in the C. sativa plant, 60 have been classified as cannabinoids (CBs) with 2, Delta-9-tetrahydrocannabinol (THC) and Cannabidiol (CBD), having been extensively tested in a research setting. However, interest has increased in the minor compounds found in the flower as well as the rest of the plant [ref. 1].
CBs have been experimented on as part of treatments for chemotherapy–toxicity-induced indications. CBs are effective in reducing nausea associated with chemotherapy and radiotherapy. However, CBs have also been shown to have anti-proliferative effects on several cancers including breast, colorectal, lung, paraganglioma, liver, melanoma, and brain, both in vitro and in vivo [ref. 2,ref. 3,ref. 4,ref. 5,ref. 6,ref. 7]. Evidence suggests that CBD may exert anticancer effects through multiple mechanisms, including apoptosis induction, cell cycle regulation, inhibition of angiogenesis, and attenuation of migration as well as invasion [ref. 2,ref. 8].
The effects of CBs are due in part to signaling through endogenous cannabinoid receptors (CB-Rs). These receptors are present on several cancer cell lines and directly correlate with aggressiveness [ref. 7,ref. 9]. These effects have been shown on both estrogen positive and negative breast cancer cell lines. In addition, effects have been seen in models of gliomas and neuroblastomas where Phase 1 clinical trials of combination temozolomide and CBD for the treatment of highly invasive brain cancer have shown promising results [ref. 1,ref. 10,ref. 11]. Interest lies not only in the correlation of CB-Rs with aggressiveness but also in the receptor activation of known cancer-inducing pathways, including the PI3K-AKT pathway [ref. 12]. CBD has also been found to have therapeutic potential in a model of gemcitabine-resistant cholangiocarcinoma, offering new potential therapies to drug-resistant cases [ref. 13]. Interestingly, recent evidence even shows a positive correlation among CBD usage and inhibition of viral replication of SARS-CoV-2 infections [ref. 11].
However, CB’s effect on cancer cell metabolism has yet to be examined. Cancer cell metabolism has been a heavily researched topic, often attributed to Otto Warburg’s work. Warburg postulated that all cancers suffered from an irreversible inhibition of mitochondrial metabolism, leaving cancer cells wholly dependent on glycolysis and sugar for energy production [ref. 14]. In recent years, however, we have seen the complexity of cancer cell metabolism; studies show that glutamine and fatty acids also play a role in cancer growth and survival. Glutamine plays a key role in the regulation and maintenance of redox potential as it is a key precursor for glutathione synthesis. However, this also relies heavily on glucose metabolism via the pentose phosphate pathway (PPP), which is responsible for the production of the reducing equivalent NADPH, critical for the recycling of oxidized glutathione (GSSSG) back to its reduced form (GSH) [ref. 15,ref. 16,ref. 17]. However, targeting cancer cell metabolism has remained an interesting yet elusive target for novel therapies. It has been suggested that CBs may exert their anti-proliferative effects partly through changes in mitochondrial membrane potential, suggesting a metabolic consequence of treatment with CBs [ref. 18].
Aside from their use in cancer therapy, CBs have been shown to influence pain and inflammation through their modulation of antioxidant enzymes such as superoxide dismutase and thioredoxin reductase, as well as its modulation of the inflammatory marker NFkB [ref. 19,ref. 20]. Application of CBs therefore reach wide from cancer to Parkinson’s, and even to chronic pain [ref. 21,ref. 22]. Furthermore, CBD has been shown to modulate several neuropsychiatric disorders with the potential to modulate psychotic, addictive, and depressive states [ref. 23].
Currently, the US Food and Drug Administration (FDA) has not approved any cannabis products for the treatment of diseases. However, it has approved several cannabis-derived and synthetic THC-like compounds for the treatment of seizures and AIDS-associated weight loss (Epidolex, Marinol, Syndros, and Cesamet). Research on large human cohorts is limited partly because important metabolic studies are lacking.
In this study, our aim was to understand the metabolic changes in malignant Malme-3M cells compared to less-aggressive BJ fibroblasts after treatment with CBD.
2. Materials and Methods
2.1. Cell Culture
The Malme-3M, (ATCC Catalog No. HTB-64, Manassas, VA, USA), were grown in an IMDM medium (Gibco, Catalog No.12440-053, Waltham, MA, USA) with 10% FBS. Immortalized BJ fibroblasts, gift from Jerry Shay at UT Southwestern (Dallas, TX, USA), were grown in a DMEM medium (Gibco, Catalog No. 11965-092, Waltham, MA, USA) with 10% FBS.
Cells were grown in T75 flasks until they reached logarithmic phase growth (80% confluency), then the cells were seeded into four replicate 60 mm dishes. The seeding density of BJ cells was 3 × 105 cells/dish and for Malme-3M was 1.2 × 106 cells/dish. The cells were incubated for 24 h before treatment. Cells were then treated with DMSO (vehicle, Sigma Catalog No. D2650-100ML, Burlington, MA, USA) or CBD (Cayman Chemical Catalog No. 90080, Ann Arbor, MI, USA) and incubated at 37 °C in a CO2 incubator for 72 h before metabolite extraction.
2.2. Dosing with CBD
BJ fibroblasts were dosed with 12.5 µM CBD, and Malme-3M cells were dosed with 16 µM CBD for 72 h, which represent their respective IC50 values as determined by cell viability assays at varying concentrations of CBD, as shown in Supplementary Figure S1.
2.3. Metabolite Measurements
Triplicate 60 mm dishes of cultured cells were used for the extraction of intracellular metabolites. The culture medium was aspirated from the dish and cells were washed twice by 5% mannitol solution (5 mL first and then 1 mL). The cells were then treated with 400 µL of methanol and left at rest for 30 s to inactivate enzymes. Next, the cell extract was treated with 275 µL of Milli-Q water containing internal standards (H3304-1002, Human Metabolome Technologies, Inc., Tsuruoka, Japan) and left at rest for another 30 s. The extract was obtained and centrifuged at 2300× g and 4 °C for 5 min and then 350 µL of the upper aqueous layer was centrifugally filtered through a Millipore 5 kDa cutoff filter at 9100× g and 4 °C for 180 min to remove proteins. The filtrate was centrifugally concentrated and re-suspended in 50 µL of Milli-Q water for CE-MS analysis.
The untargeted metabolome analysis with CE-TOF/MS was performed using an Agilent CE-TOFMS system (Agilent Technologies, Santa Clara, CA, USA) equipped with a fused silica capillary [50 µm (inner diameter) × 80 cm]. For measurements of cationic/anionic metabolites, running buffer, a solution composed of Cation Buffer Solution [H3301–1001; Human Metabolome Technologies (HMT), Tsuruoka, Japan] and Anion buffer solution (H3302–1021) were used, with CE voltage + 27 kV/+ 30 kV, MS ionization ESI positive/negative, MS capillary voltage 4000 V/3500 V, MS scan range 50–1000 m/z, and HMT Sheath Liquid (H3301–1020). Identification of metabolites and measurement of relative amounts were performed using MASTER HANDS (version 2.1.0.1, 2.9.0.9; Keio University, Tokyo, Japan) and the HMT metabolite database based on internal standards (HMT) [ref. 24]. Data are represented as the average of three independent samples +/− standard deviation. All metabolite measurements are represented as the relative area under the curve.
3. Results
In this study, we aimed to understand metabolic changes in the malignant Malme-3M cell line compared to the less-aggressive BJ fibroblast cell line when pre-treated with cannabidiol (CBD) for 72 h. We first interrogated cellular wide changes and their associated metabolic processes. BJ fibroblast and Malme-3M cell lines were treated with 12.5 and 16 μM CBD, which, respectively, represent the IC50 for each cell line. As shown in Table 1, we saw a larger number of differentially regulated metabolites in the Malme-3M cell line treated with CBD relative to BJ fibroblasts. Of note, we saw significant changes in several key metabolic pathways to include glycolysis, glutaminolysis, redox maintenance, the urea cycle, and the TCA cycle.
Table 1: Overall view of key metabolic changes observed in the Malme-3M cell line relative to the control BJ Fibroblasts. As shown in the table, several metabolites involved in primary metabolism, including choline regulation, glycolysis, and the TCA, were differentially regulated by CBD in the Malme cell line. The up-regulated cutoff, shown in red, was 1.2-fold or above, while the down-regulated cutoff, shown in green, was 0.8-fold or below. FC represents the fold change between the corresponding treated vs. control for the represented cell line. Black rows represent separators between major metabolic groups.
| Annotation | FC Fibro CBD/Control | FC Malme CBD/Control | Pathway |
|---|---|---|---|
| Malonyl CoA | 1.39 | 0.00 | Fatty acid synthesis |
| HMG CoA | 0.22 | 0.38 | CHOL synthesis |
| Glucose 6-phosphate | 0.54 | 0.46 | Glycolysis |
| Fructose 6-phosphate | 0.47 | 0.36 | Glycolysis |
| Fructose 1,6-diphosphate | 1.89 | 0.48 | Glycolysis |
| Dihydroxyacetone phosphate (DHAP) | 1.52 | 0.43 | Glycolysis |
| 2-Phosphoglyceric acid | 0.75 | 0.59 | Glycolysis |
| 3-Phosphoglyceric acid | 0.84 | 0.59 | Glycolysis |
| Phosphoenolpyruvic acid (PEP) | 0.70 | 0.38 | Glycolysis |
| Pyruvic acid | 0.86 | Glycolysis | |
| Lactic acid | 1.80 | 1.67 | Glycolysis |
| Lac/Pyr ratio | 1.97 | Glycolysis | |
| O-Acetylcarnitine (ALCAR) | 1.35 | 0.42 | Glycolysis |
| Acetyl CoA | 2.95 | 1.18 | Glycolysis |
| ALCAR/Acetyl CoA | 0.40 | 0.34 | Glycolysis |
| 3-Hydroxybutyric acid (3-HB) | 1.21 | 0.61 | Glycolysis |
| Met | 1.02 | 1.00 | Transulfuration |
| Cys | 1.71 | 0.83 | Transulfuration |
| Homocysteine | 0.34 | 0.42 | Transulfuration |
| S-Adenosylhomocysteine | 1.24 | 0.91 | Transulfuration |
| S-Adenosylmethionine | 1.00 | 2.19 | Transulfuration |
| Glutathione (GSSG) | 0.99 | 0.43 | Oxidative stress |
| Glutathione (GSH) | 0.59 | 0.41 | Oxidative stress |
| GSH/GSSG ratio | 0.61 | 0.96 | Oxidative stress |
| Cystathionine | 1.60 | 0.99 | Oxidative stress |
| Carnosine | 1.07 | 0.60 | Oxidative stress |
| NADH | 1.72 | 0.29 | NAD metabolism |
| NADPH | 1.39 | 0.18 | NAD metabolism |
| NADH/NADPH ratio | 1.42 | 1.63 | NAD metabolism |
| Phosphocreatine | 0.35 | 0.02 | Urea cycle |
| Ornithine | 0.90 | 1.31 | Urea cycle |
| Arg | 1.49 | 1.26 | Urea cycle |
| Citrulline | 1.18 | 1.07 | Urea cycle |
| Arg/Cit ratio | 1.27 | 1.17 | Urea cycle |
| Creatinine | 1.11 | 0.92 | Urea cycle |
| Creatine | 0.52 | 0.31 | Urea cycle |
| Spermine | 0.72 | 0.28 | polyamine |
| Spermidine | 1.08 | 0.11 | polyamine |
| N1,N12-Diacetylspermine | 100.63 | Polyamine | |
| N1-Acetylspermine | 5.28 | Polyamine | |
| N-Acetylputrescine | 0.81 | 1.46 | Polyamine |
| N1,N8-Diacetylspermidine | 4.33 | Polyamine | |
| N1-Acetylspermidine | 1.92 | 3.28 | Polyamine |
| Putrescine | 1.05 | 2.07 | polyamine |
| N-Methylputrescine | 1.47 | polyamine | |
| Inosine | 3.65 | 0.34 | purine |
| Adenosine | 1.96 | 0.20 | Purine synthesis |
| Guanosine | 8.44 | 0.20 | Purine synthesis |
| 6-Phosphogluconic acid | 0.89 | 0.68 | Purine synthesis |
| Hypoxanthine | 3.22 | 53.49 | Purine synthesis |
| IMP | 1.61 | 23.47 | Purine synthesis |
| Citric acid | 0.46 | 0.09 | TCA cycle |
| cis-Aconitic acid | 0.33 | 0.08 | TCA cycle |
| Isocitric acid | 0.00 | 0.00 | TCA cycle |
| 2-Oxoglutaric acid | 0.56 | 0.03 | TCA cycle |
| Succinic acid | 1.15 | 7.39 | TCA cycle, pyrimidine synthesis, urea cycle |
| Glutamic acid | 0.93 | 0.17 | TCA, Glutaminolysis, GSH synthesis |
| Glutamine | 2.02 | 1.03 | TCA, Glutaminolysis |
| Glu/Gln ratio | 0.70 | 0.17 | TCA cycle |
| Fumaric acid | 0.72 | 0.51 | TCA cycle |
| Malic acid | 0.72 | 0.55 | TCA cycle |
| FMN | 0.00 | 0.14 | TCA cycle |
| ATP | 0.87 | 0.44 | TCA cycle |
While both the less-aggressive BJ fibroblast cells and aggressive Malme-3M cells showed a significant decrease in citrate, as shown in Figure 1A, there was only a corresponding decrease in ATP in the Malme-3M cells. Glycolytic activity was correspondingly increased in the Malme-3M cell line in a likely attempt to maintain ATP levels, as shown by a significant increase in lactic acid production.
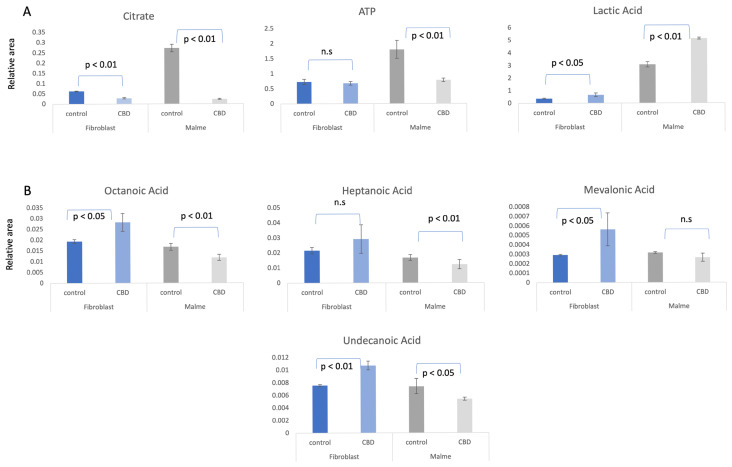
By examining the change in short and medium chain fatty acids, we observed that fatty acid metabolism is elevated in BJ fibroblasts because of CBD treatment, as shown in Figure 1B. This suggests that the BJ fibroblasts respond to reductions in TCA cycle activity with an increase in fatty acid oxidation to maintain constant ATP levels. In contrast, there is an overall significant decrease or no change in the Malme-3M cells, consistent with an inhibited TCA cycle.
We suggest that CBD results in potential oxidative stress—or greater susceptibility to oxidative stress—in malignant cells lines only. In Figure 2A, we show that glutamate was significantly reduced in the Malme-3M cells, resulting in a reduction in both GSH and GSSG, likely affecting de novo glutathione synthesis. NADPH, which is required for GSH regeneration, was also significantly reduced in Malme-3M.
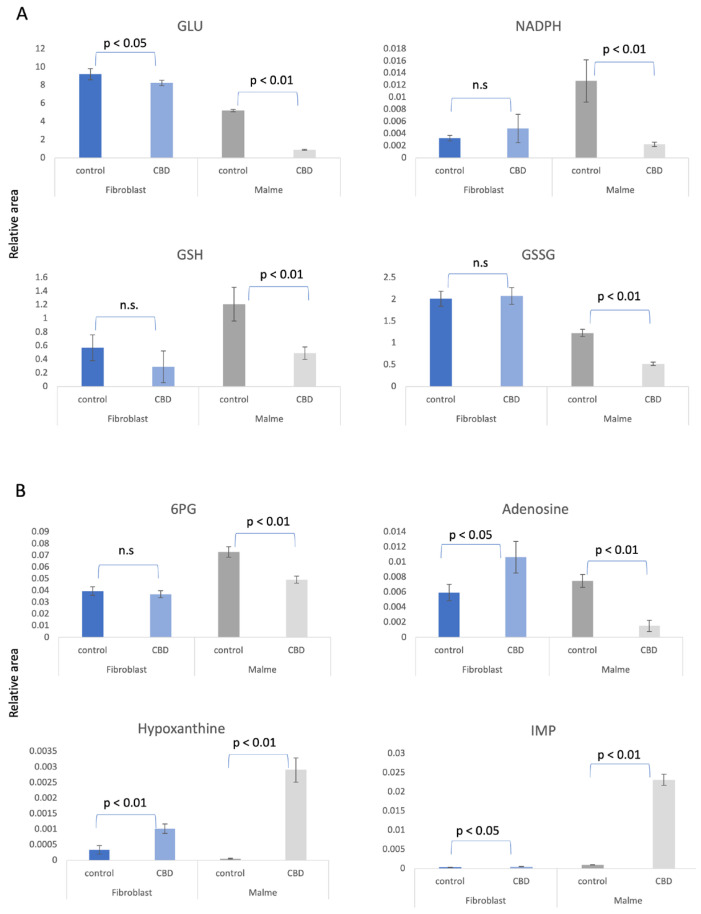
As shown in Figure 2B, the pentose phosphate pathway (PPP) and de novo purine synthesis are differentially regulated by CBD in BJ fibroblasts versus the Malme-3M cells. As a result of a likely increase in glycolytic activity in the Malme-3M cell line, glucose carbons are shunted away from the PPP to accommodate this increased demand for ATP. This results in an overall decrease in de novo purine synthesis, as shown by a dramatic decrease in both 6-phosphogluconate (6-PG), the first metabolite of the PPP, and adenosine levels, a key precursor for nucleotide synthesis. The nucleotide salvage pathway can potentially recycle purine bases to maintain some level of de novo purine synthesis. During this process of recycling nucleotides, hypoxanthine is a key intermediate. We see both hypoxanthine and inosine monophosphate (IMP), a product recycled from hypoxanthine, are dramatically elevated in Malme-3M + CBD with a 53× and 23× fold increase, respectively, suggesting nucleotide salvage is activated. The first committed step of the PPP also produces NADPH, which is essential for GSH regeneration. We see that in Malme-3M, this step seems to be reduced, resulting from less activity in the PPP and as a byproduct, less production of NADPH, as shown in Figure 2A. While we also see only a modest increase in IMP and hypoxanthine in BJ fibroblasts, we see an increase in adenosine as well, which may suggest that de novo purine synthesis might be up-regulated because of CBD treatment. This contrasts with the decrease in de novo purine synthesis we see in Malme cells.
4. Discussion
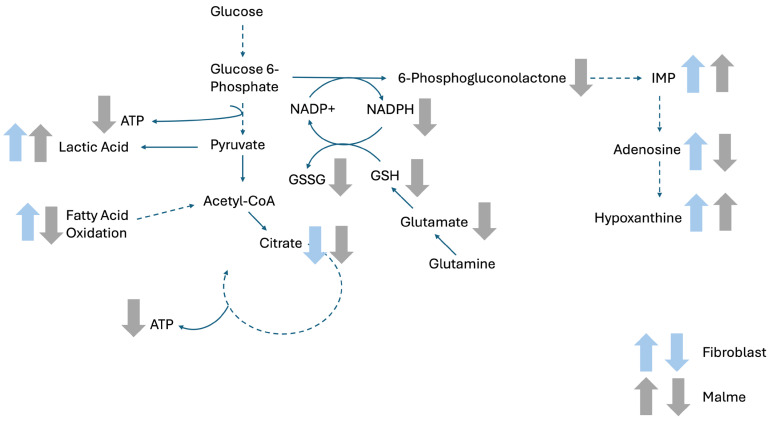
A detailed metabolic analysis of less-aggressive human BJ fibroblasts versus the malignant Malme-3M cell line was performed after 72 h of CBD treatment. CBD exerted a differential effect in the Malme-3M cell line, particularly affecting central energy metabolites, as highlighted in Figure 3. Specifically, there was a reduction of TCA cycle metabolites in the Malme-3M cells, and a corresponding increase in glycolytic output in the form of lactic acid. Consistent with an inhibited TCA cycle, reductions in ATP levels were seen. A potential consequence of an elevated glycolytic pathway is the diversion of glucose carbons away from de novo purine synthesis for the continued production of ATP for cell survival. However, because of reduced purine synthesis, the nucleotide salvage pathway appears to be elevated, as noted with dramatic increases in both hypoxanthine and IMP, key biomarkers of nucleotide salvage, in CBD treated Malme-3M cells. A major consequence of reduced carbon flow through the pentose phosphate pathway (PPP)—a key precursor pathway for de novo purine synthesis—is the reduction of NADPH, which is generated by the first committed step of the PPP. NADPH is critical for the recycling of oxidized glutathione during times of oxidative stress. Overall, in conjunction with a reduction of total glutathione levels in the Malme-3M cells, we suggest that this can further sensitize the cells to oxidative stress.
The reduction of total glutathione levels could be in part due to a reduction in de novo synthesis of glutathione as glutamate, a key glutathione precursor, could be re-directed to the TCA to compensate for the reduced TCA activity. A reduction in glutathione, in combination with reduced levels of NADPH, may result in an increased sensitivity to oxidative stress in the Malme-3M cells. Therefore, CBD treatment may result in synergistic effects when combined with other redox-inducing stress such as radiation therapy.
Interestingly, while the BJ fibroblasts also exhibited changes in some of the same key metabolic pathways, namely the TCA cycle and an increase in lactic acid production, there were key differences in the response by these cells. One key difference in the response to CBD treatment was the overall increase in short and medium chain fatty acids in the BJ cells, while either no change or a slight decrease in the Malme-3M cell line was seen. This differential response could be observed because of the inhibited TCA cycle. The less-aggressive cells may switch to fatty acid oxidation to maintain cellular ATP levels. Indeed, there was no change in ATP levels in the BJ cells, even in the presence of reduced citrate concentrations and a presumably reduced TCA cycle. On the other hand, Malme-3M cells were unable to maintain cellular ATP levels in a similar way. Instead, the attempt to maintain ATP levels was through an increase in glycolytic output, as evidenced by a larger increase in lactic acid in the Malme-3M cells.
The observed metabolic changes due to the mitochondria-related consequences of CBD treatment may be related to calcium maintenance. CBD has previously been shown to increase intracellular calcium levels and reduce cell viability [ref. 25,ref. 26]. These effects can be attributed to activation of the transmembrane ion channel TRPA1 by CBD, followed by activation of the mitochondrial outer membrane VDAC1 by increased calcium flux or direct interaction with CBD [ref. 27]. VDAC1 is an outer mitochondrial receptor that increases uptake of calcium into the mitochondria, leading to calcium overload and cell death. Studies have shown alterations of cancer cell mitochondrial membrane composition [ref. 28,ref. 29] could leave cancer cells more susceptible to calcium dysregulation because CBD exerts its effects through several potential signaling pathways. This can occur through the CB1/CB2, VDAC1, and TRPV1 receptors, which all regulate glycolysis, glutaminolysis, and oxidative stress markers. It is possible that future therapeutic strategies can take advantage of this differential response. For example, aggressive cancers treated with CBD may be more susceptible to therapies designed to increase oxidative stress, or other metabolic inhibitors used to synergistically weaken aggressive cancer cells.
5. Conclusions
For the first time, an analysis of metabolomics of both less-aggressive BJ fibroblasts and malignant Malme-3M cells after pre-treatment with CBD has been made. As a result of CBD treatment, there is reprogramming of key metabolic processes including the TCA cycle, redox maintenance, and fatty acid oxidation. While more studies are needed to fully elucidate the mechanistic effects of CBD treatment, there is a clear and differential cellular metabolic consequence of CBD treatment between these cell types.
References
- T.Q. Nguyen, H.S. Park, S.H. Choi, D.Y. Hong, J.Y. Cheon, Y.M. Lee, C.M. Kim, J.K. Hong, S.J. Oh, M.S. Cho. New Cannabinoids and Chlorin-Type Metabolites from the Flowers of Cannabis sativa L.: A Study on Their Neuroblastoma Activity. Pharmaceuticals, 2025. [DOI | PubMed]
- Y.M. Deng, C. Zhao, L. Wu, Z. Qu, X.Y. Wang. Cannabinoid Receptor-1 suppresses M2 macrophage polarization in colorectal cancer by downregulating EGFR. Cell Death Discov., 2022. [DOI | PubMed]
- V.N. Ivanov, J. Wu, T.J.C. Wang, T.K. Hei. Inhibition of ATM kinase upregulates levels of cell death induced by cannabidiol and gamma-irradiation in human glioblastoma cells. Oncotarget, 2019. [DOI | PubMed]
- M. Esmaeli, M. Dehghanpour Dehabadi. Cannabidiol (CBD) as a potential therapeutic agent for liver cancer: A comprehensive review of current evidence. Cancer Cell Int., 2025. [DOI | PubMed]
- G. Nahler. Cannabidiol and Other Phytocannabinoids as Cancer Therapeutics. Pharmaceut. Med., 2022. [DOI | PubMed]
- K. Wang, L. Schober, A. Fischer, N. Bechmann, J. Maurer, L. Peischer, A. Reul, C. Hantel, M. Reincke, F. Beuschlein. Opposing Effects of Cannabidiol in Patient-derived Neuroendocrine Tumor, Pheochromocytoma/Paraganglioma Primary Cultures. J. Clin. Endocrinol. Metab., 2024. [DOI | PubMed]
- S.S. Alghamdi, H.N. Albahlal, D.E. Aloumi, S. Bin Saqyah, A. Alsubait, J. Alamre, M. Alrashed, N. Alsuhabeny, A.E. Mohammed. Revealing the therapeutic potential of synthetic cannabinoids: A systematic review of cannabinoid receptor binding dynamics and their implications for cancer therapy. J. Cannabis Res., 2025. [DOI | PubMed]
- P. Massi, M. Solinas, V. Cinquina, D. Parolaro. Cannabidiol as potential anticancer drug. Br. J. Clin. Pharmacol., 2013. [DOI | PubMed]
- C.F. Almeida, N. Teixeira, G. Correia-da-Silva, C. Amaral. Cannabinoids in Breast Cancer: Differential Susceptibility According to Subtype. Molecules, 2021. [DOI | PubMed]
- M. Guzman, M.J. Duarte, C. Blazquez, J. Ravina, M.C. Rosa, I. Galve-Roperh, C. Sanchez, G. Velasco, L. Gonzalez-Feria. A pilot clinical study of Delta9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme. Br. J. Cancer, 2006. [DOI | PubMed]
- B. Bukowska. Current and Potential Use of Biologically Active Compounds Derived from Cannabis sativa L. in the Treatment of Selected Diseases. Int. J. Mol. Sci., 2024. [DOI | PubMed]
- C. Pagano, G. Navarra, L. Coppola, G. Avilia, M. Bifulco, C. Laezza. Cannabinoids: Therapeutic Use in Clinical Practice. Int. J. Mol. Sci., 2022. [DOI | PubMed]
- T. Pongking, P. Thongpon, K. Intuyod, S. Klungsaeng, R. Thanan, A. Chaidee, N. Charoenram, S. Kongsintaweesuk, C. Sakonsinsiri, K. Vaeteewoottacharn. Cannabidiol exhibits potent anti-cancer activity against gemcitabine-resistant cholangiocarcinoma via ER-stress induction in vitro and in vivo. BMC Complement. Med. Ther., 2024. [DOI | PubMed]
- O. Warburg. On the origin of cancer cells. Science, 1956. [DOI | PubMed]
- R.J. DeBerardinis, A. Mancuso, E. Daikhin, I. Nissim, M. Yudkoff, S. Wehrli, C.B. Thompson. Beyond aerobic glycolysis: Transformed cells can engage in glutamine metabolism that exceeds the requirement for protein and nucleotide synthesis. Proc. Natl. Acad. Sci. USA, 2007. [DOI | PubMed]
- T.N. Seyfried, L.M. Shelton. Cancer as a metabolic disease. Nutr. Metab., 2010. [DOI]
- L.M. Shelton, L.C. Huysentruyt, T.N. Seyfried. Glutamine targeting inhibits systemic metastasis in the VM-M3 murine tumor model. Int. J. Cancer, 2010. [DOI | PubMed]
- K. Sooda, S.J. Allison, F.A. Javid. Investigation of the cytotoxicity induced by cannabinoids on human ovarian carcinoma cells. Pharmacol. Res. Perspect., 2023. [DOI | PubMed]
- A. Jastrzab, A. Gegotek, E. Skrzydlewska. Cannabidiol Regulates the Expression of Keratinocyte Proteins Involved in the Inflammation Process through Transcriptional Regulation. Cells, 2019. [DOI | PubMed]
- W.J. Huang, W.W. Chen, X. Zhang. Endocannabinoid system: Role in depression, reward and pain control (Review). Mol. Med. Rep., 2016. [DOI | PubMed]
- S. Pisanti, A.M. Malfitano, E. Ciaglia, A. Lamberti, R. Ranieri, G. Cuomo, M. Abate, G. Faggiana, M.C. Proto, D. Fiore. Cannabidiol: State of the art and new challenges for therapeutic applications. Pharmacol. Ther., 2017. [DOI | PubMed]
- E.B. Russo. The Case for the Entourage Effect and Conventional Breeding of Clinical Cannabis: No “Strain,” No Gain. Front. Plant Sci., 2018. [DOI | PubMed]
- S. Elsaid, S. Kloiber, B. Le Foll. Effects of cannabidiol (CBD) in neuropsychiatric disorders: A review of pre-clinical and clinical findings. Prog. Mol. Biol. Transl. Sci., 2019. [DOI | PubMed]
- T. Soga, Y. Kakazu, M. Robert, M. Tomita, T. Nishioka. Qualitative and quantitative analysis of amino acids by capillary electrophoresis-electrospray ionization-tandem mass spectrometry. Electrophoresis, 2004. [DOI | PubMed]
- N. Rimmerman, D. Ben-Hail, Z. Porat, A. Juknat, E. Kozela, M.P. Daniels, P.S. Connelly, E. Leishman, H.B. Bradshaw, V. Shoshan-Barmatz. Direct modulation of the outer mitochondrial membrane channel, voltage-dependent anion channel 1 (VDAC1) by cannabidiol: A novel mechanism for cannabinoid-induced cell death. Cell Death Dis., 2013. [DOI | PubMed]
- J.Z. Chan, R.E. Duncan. Regulatory Effects of Cannabidiol on Mitochondrial Functions: A Review. Cells, 2021. [DOI | PubMed]
- A. de la Harpe, N. Beukes, C.L. Frost. CBD activation of TRPV1 induces oxidative signaling and subsequent ER stress in breast cancer cell lines. Biotechnol. Appl. Biochem., 2022. [DOI | PubMed]
- A. Musella, V. De Chiara, S. Rossi, C. Prosperetti, G. Bernardi, M. Maccarrone, D. Centonze. TRPV1 channels facilitate glutamate transmission in the striatum. Mol. Cell Neurosci., 2009. [DOI | PubMed]
- M.A. Kiebish, X. Han, H. Cheng, J.H. Chuang, T.N. Seyfried. Brain mitochondrial lipid abnormalities in mice susceptible to spontaneous gliomas. Lipids, 2008. [DOI | PubMed]