
Cannabis Use Among Older Adults
Abstract
Question:
What are the prevalence and correlates of cannabis use and cannabis use disorder (CUD) among older adults?
Findings:
In this cross-sectional study of 4503 respondents aged 65 to 84 years from the Veterans Health Administration (2020-2023), 10% reported past 30-day cannabis use, 36% of whom had CUD. Odds for CUD were higher among younger respondents, those reporting anxiety, those with 1 or more deficits in activities of daily living, those with past month illicit drug use, and those with frequent, inhaled, or recreational cannabis use.
Meaning:
Asking about cannabis use as part of routine health behavior screening in Veterans Health Administration clinical settings may help identify older adults with cannabis use or CUD.
Affiliations: Center for Data to Discovery and Delivery Innovation, San Francisco Veterans Affairs (VA) Health Care System, San Francisco, California; Northern California Institute for Research and Education, San Francisco; Center for Tobacco Control Research and Education, Cardiovascular Research Institute, University of California, San Francisco; School of Medicine, University of California, San Francisco; Division of Geriatrics, San Francisco VA Health Care System, San Francisco, California; Division of Geriatrics, Department of Medicine, University of California, San Francisco; Department of Psychiatry and Behavioral Sciences, University of California, San Francisco; Institute of Health Policy, Management and Evaluation, University of Toronto, Toronto, Ontario, Canada; Department of Psychiatry, Columbia University Medical Center, New York, New York; Addiction Recovery and Treatments Services, San Francisco VA Health Care System, San Francisco VA Medical Center, San Francisco, California
License: Copyright 2025 Pravosud V et al. JAMA Network Open. CC BY 4.0 This is an open access article distributed under the terms of the CC-BY License.
Article links: DOI: 10.1001/jamanetworkopen.2025.10173 | PubMed: 40366653 | PMC: PMC12079303
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (507 KB)
Introduction
Cannabis use has been increasing in the US,1,2,3 yet little is known about patterns and correlates of current cannabis use and cannabis use disorder (CUD) in older adults.4,5 Previous studies have suggested an increase in cannabis use among older people,4,5,6,7,8 with less than 1% (ranging from 0.4%6,8 to 0.7%7) of adults 65 years or older reporting past-year cannabis use in 2005 to 2006 compared with 8.4% in 2022.9 Smoking is the most common form of cannabis use among those 60 years or older4,5 and is perceived as less harmful than tobacco smoking.6,10 Expansion of state-directed legalization of medical and recreational cannabis, which leads to greater accessibility of cannabis products, has contributed to higher rates of cannabis use1,11,12,13,14,15 and CUD.13,16 Between 2017 and 2022, there was a significant increase in CUD-related encounters among Medicare beneficiaries 65 years or older, with the highest rates in states where recreational and medical cannabis was legal.17 Despite older adults generally holding more negative beliefs about cannabis, legalization might have shifted cannabis perceptions toward its social acceptance among this age group.18 Older people use cannabis for medical reasons, such as management of pain, mental health, and sleep, which can influence their risk perception and increase the frequency of use.19,20
Favorable views and increasing frequency of cannabis use among older adults warrant more research on patterns of consumption and correlates of CUD among this population. Older people are generally at higher risks for impairment of activities of daily living (ADLs),21 frailty and associated falls,22 as well as hospitalizations and mortality23 and thus may be particularly susceptible to adverse effects of cannabis, even if used for therapeutic purposes.24,25 Cannabis use increases the risk of neuropsychiatric disorders,26,27,28,29 respiratory symptoms,30 and cardiovascular outcomes31,32,33,34,35 that remain the leading causes of death in older adults.23 Another negative consequence of cannabis use is the risk of CUD, which has become one of the most prevalent substance use disorders in the US.3 Data from the early 1990s to mid-2000s indicate that approximately 20% to 30% of those who use cannabis may develop CUD,36 with higher risks for people who use cannabis daily.37,38 However, these data rely on reports largely from younger populations. In recent years, frequent cannabis use has increased in the general US population 12 years and older,39 but the frequency of current cannabis use and its association with CUD in older adults remains unclear.
Although some previous studies have examined cannabis use and CUD in middle to late life,7,40,41,42 to our knowledge, no recent study has focused on detailing the patterns and correlates of current cannabis use and CUD in adults 65 years or older at a national level. Older veterans are another understudied population in cannabis research. Unlike younger age groups (18-25 years), veterans 65 years or older are less likely to use recreational cannabis,43,44 are more likely to use medicinal cannabis recommended by a health care professional,45 and report use for pain management, insomnia, and mental health (eg, posttraumatic stress disorder [PTSD]).19,20,46 Overall, cannabis use and CUD among US veterans 18 years or older, including among patients of the Veterans Health Administration (VHA), have been increasing since the early 2000s,45,47 especially in states that have legalized cannabis.16,43,47 During the early and mid-2000s, past-year CUD estimates were 1.38% among VHA patients16 and 1.8% among US veterans in general.43 The most recent 2020 data of US veterans aged 22 to 99 years (mean [SD] age, 62.2 [15.7] years) showed a rate of 2.7% for past 6-month CUD diagnoses.48 In VHA patients 65 years or older, CUD prevalence has disproportionately increased between 2016 and 2019 among veterans with psychiatric disorders (from 1.3% to 2.0%) vs those without49 and among those with chronic or severe pain (from 0.6% to 1.0%) vs those without.46 However, rates of CUD among older veterans who engage in cannabis use are unknown.
The current Veterans Affairs (VA) Cannabis and Aging Study is the first analysis of a cohort of adults 65 years or older who have answered detailed survey questions on cannabis use and CUD. We used cross-sectional data from the baseline interview of this cohort to characterize cannabis use in late life, describing forms, frequency, reasons for cannabis use, and prevalence and correlates of CUD among a national sample of older adults who used the VA health care system. Prior research of older adults among veteran16,46,49 and nonveteran17 populations in health care settings provides data on CUD prevalence based on clinical diagnoses, which likely represent more severe CUD cases,50,51 whereas rates of mild CUD may remain underreported.52 Although the use of a VHA cohort in our study presents challenges for generalizability to other populations,53 this work provides important data on cannabis use in older veterans and offers benchmark data regarding patterns and correlates among the general population of adults 65 years or older—an age group that has been underrepresented in cannabis research.37,54
Methods
Study Design and Sample
This study is an analysis of cross-sectional interview and medical record data collected from participants in the VA Cannabis and Aging Cohort at study entry. It includes a national sample of community-dwelling adult VHA patients aged 65 to 84 years with at least 1 primary care visit in the 2 years before October 3, 2019, to ensure that we captured a population who would have baseline data available in the VHA records (n = 2 590 235). Using the Corporate Data Warehouse (CDW), we excluded 729 922 patients (22.0%) who were not in the age range of interest, deceased, or potentially at the end of life (eg, hospice or palliative care) (Figure 1). Participants provided verbal informed consent before the interview. The University of California, San Francisco Institutional Review Board provided a waiver for obtaining written consent. This study was approved by the University of California, San Francisco Institutional Review Board and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.
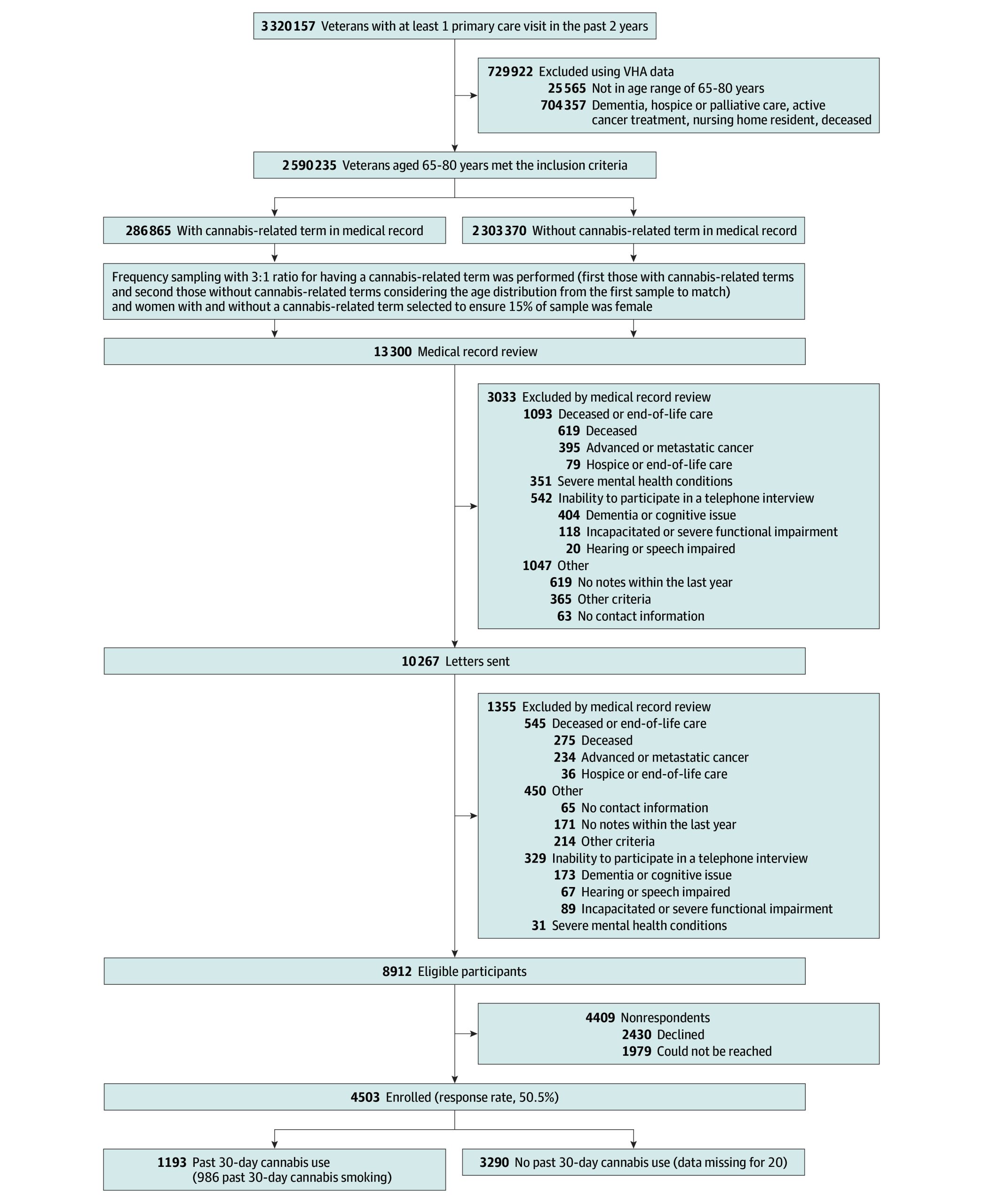
The VA Cannabis and Aging Study selected people with and without cannabis use by identifying adults with medical record documentation of prior cannabis use or nonuse by applying a previously developed text processing algorithm.55 We categorized potential participants into 2 groups: those with (n = 286 865) and without (n = 2 303 370) a term denoting cannabis use in their medical record in the past 6 months (eg, cannabis, marijuana, MJ). To recruit a mix of those initially identified from both groups (with and without cannabis-related terms), we randomly selected individuals who potentially engaged (3.6% sampled) and did not engage (0.1% sampled) in cannabis use. To ensure sufficient representation, we also oversampled female veterans to ensure that approximately 15% of the sample was female. We sampled participants until we met recruitment goals.
Once participants had been selected, we reviewed 13 300 medical records (eg, health professionals’ summaries) to identify those with exclusion criteria missed by VHA CDW data in the first round (eg, end-of-life care). We excluded 3033 participants (22.8%) in 4 categories using medical record reviews: (1) those deceased or receiving end-of-life care (n = 1093); (2) those with a severe mental health condition (eg, active suicidal ideation documented in a recent visit), for whom a phone call might have exacerbated the underlying mental health condition and who could not participate in an interview (n = 351); (3) those unable to participate in a telephone interview (eg, having a severe cognitive or speech impairment) (n = 542); and (4) other (eg, no contact information, lived outside the US, or incarcerated) (n = 1047). Eligible participants (n = 10 267) were mailed a letter and then telephoned after 2 weeks and invited to participate in a 30- to 45-minute telephone interview (the initial incentive of US $25 was later increased to US $35). At this stage, we identified an additional 1355 patients (13.2%) who met the 4 exclusion criteria before or during interviews. From the sample of eligible individuals (n = 8912), we recruited respondents from February 5, 2020, to August 29, 2023 (Figure 1; eTable 1 in Supplement 1). Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the VA.56
Assessment of Cannabis Use
The telephone interview asked about forms and frequency of lifetime, last-year, and past 30-day cannabis use and about duration (in years) of lifetime cannabis smoking (eTable 2 in Supplement 1). Respondents reported reasons for lifetime use of medical or recreational cannabis and specified for which health concerns they had ever used cannabis (eg, insomnia or pain) (eTable 3 in Supplement 1). Those who reported past 30-day cannabis use were asked about 11 CUD-related diagnostic criteria related to their experiences in the past 12 months (eTable 2 in Supplement 1) using a checklist derived from the CUD questions included in the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) (DSM-5)57: mild CUD, defined as reporting 2 to 3 criteria; moderate CUD, defined as reporting 4 to 5 criteria; and severe CUD, defined as reporting 6 criteria or more.
Assessments of Baseline Health
Sociodemographic Characteristics
Using data from the VHA CDW, we collected data regarding respondents’ age, race and ethnicity, employment status, and state of residence. During the survey interview, respondents provided data on their marital status, the highest level of educational attainment, and whether it was hard to pay for basic needs as a proxy for income. Race and ethnicity were included in the analysis because one of the primary goals of the study was to examine sociodemographic correlates of cannabis use and CUD among older veterans.
Health Behaviors
Respondents provided information on current and past tobacco use status, alcohol use, and past 30-day illicit drug use (eg, amphetamines or cocaine) (eTable 2 in Supplement 1). Using interview data on quantity and frequency of past-year alcohol use, we assessed the presence or absence of hazardous drinking with the Alcohol Use Disorders Identification Test–Consumption (AUDIT-C) (cutoff scores of ≥4 for men and ≥3 for women).58
Mental Health
Respondents self-reported feeling lonely vs not lonely based on a 3-item scale.59 We assessed dichotomized variables indicating PTSD (cutoff score >18 based on the 8-item Posttraumatic Stress Disorder Checklist for DSM-560), moderate-severe anxiety (>9 based on the 7-item Generalized Anxiety Disorder screener61), and clinically significant depressive symptoms (≥10 based on the 8-item Patient Health Questionnaire screener62).
Physical Health and Aging Relevant Variables
Using electronic health record (EHR) data, we examined the Care Assessment Need score (categorized into 3 groups: <50, 50 to <75, and ≥75), which is a VHA-specific measure where a higher score indicates higher hospitalization and mortality risk,63,64 and a dichotomized variable indicating an individual’s independence in ADLs based on the Katz Index of Independence in Activities of Daily Living.21,65 Respondents also reported experiencing falls in the past 12 months (yes or no).
Outcome Variables
We examined 2 main outcome variables. The first was a binary variable of self-reported past 30-day cannabis use, defined as use of inhaled (smoking, vaporizing or “vaping,” or dabbing) or edible cannabis because of higher health risk associated with these routes of administration vs topical use (ie, topicals were coded as no past 30-day use). The second was a binary variable indicating any past 12-month CUD (≥2 of the 11 CUD-related diagnostic criteria) (eTable 2 in Supplement 1) among those with past 30-day cannabis use.57 We descriptively reported the prevalence of cannabis use in the last year and in a lifetime (including and excluding topicals) and frequent past 30-day cannabis use (ie, ≥20 days, similar to prior surveys3).
Statistical Analysis
All analyses were conducted in SAS software, version 9.4 (SAS Institute Inc) from February to May 2024 using PROC SURVEY procedures with combined person-level analytic weights (sampling weights × nonresponse weights) to account for the sampling of our cohort from the larger population of VHA patients (our target population) and nonresponse to the patient survey. The denominator for our cohort sampling weights came from the full VHA patient population; sampling weights were computed using age, gender, race, ethnicity, US Census region, and presence of cannabis-related terms in medical notes. These sampling weights were applied to align the sample with the distribution of veterans aged 65 to 80 years who had met study inclusion criteria (n = 2 590 235) (Figure 1). Nonresponse weights were computed using the same factors to adjust for differences between respondents and nonrespondents. The final person-level weights, which were the product of sampling and nonresponse weights, were then normalized to ensure the weighted sample also summed to the total population of veterans aged 65 to 80 years who had met the inclusion criteria (n = 2 590 235).
For descriptive analysis, we reported weighted means with 95% CIs or medians with IQRs for continuous variables; for categorical variables, we reported unweighted numbers and weighted percentages together with 95% CIs for the total sample, by gender, by lifetime or past 30-day cannabis use, and by CUD status. We compared weighted percentages via the Rao-Scott χ2 tests by gender, past 30-day cannabis use, and CUD.
Our primary adjusted analysis assessed correlates of past 30-day cannabis use among all respondents and of CUD among those reporting past 30-day use. We used weighted multivariable logistic regression models, simultaneously including sociodemographic (age, gender, race and ethnicity, educational level, employment, economic hardship, marital status, and state of residents) and behavioral (alcohol, tobacco, and illicit drug use) characteristics, self-reported loneliness, and mental health concerns (anxiety, depression, or PTSD) as well as physical function or health-related factors (Care Assessment Need score, ADLs, or experiencing falls). The CUD model also included the frequency of past 30-day cannabis use as an independent variable.
Our secondary adjusted analysis assessed the odds of CUD with the forms of past 30-day cannabis use among those reporting past 30-day cannabis use (model 1: smoking, vaping, dabbing, and use of edibles separately; model 2: any inhaled cannabis use vs edibles only). We used weighted multivariable logistic regression models that controlled for age, gender, frequency of past 30-day cannabis use, and reasons for lifetime cannabis use. We then performed 2 sensitivity analyses. First, we reran models 1 to 2 without accounting for frequency of use to examine whether it was confounding associations between any CUD and forms of use. Second, we reran models 1 to 2 of the secondary adjusted analysis while defining CUD as reporting 4 or more CUD-related criteria (ie, any moderate or severe CUD).
Our collinearity diagnostics revealed no substantial collinearity among the included variables in the models (variance inflation factors were <1.82). In all analyses, we used listwise deletion of missing data; the combined proportion of missing values for the response and independent variables in each analysis was less than 2.5%. Two-tailed P < .05 was considered statistically significant.
Results
A total of 4503 respondents participated in the study (response rate, 50.5%; 51.3% among those with the cannabis term in the medical records and 48.2% among those without the cannabis term) (Figure 1). The study participants were not substantially different from the nonrespondents (eTable 1 in Supplement 1), and there were no significant differences by age, race, and ethnicity between respondents and nonrespondents when stratified by a cannabis term noted in the medical records. Among the 4503 respondents, the weighted mean age was 73.3 years (95% CI, 73.0-73.5 years). Of the respondents, 4.2% (95% CI, 3.1%-5.4%) were Hispanic, 13.3% (95% CI, 11.6%-15.0%) were non-Hispanic Black or African American, 78.4% (76.2%-80.6%) were non-Hispanic White, and 4.0% (95% CI, 2.9%-5.1%) were non-Hispanic other race (Asian, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, multiple races, or unknown or not reported). Most were men (85.4%; 95% CI, 83.6%-87.2%), retired (73.3%; 95% CI, 70.9%-75.8%), and married (62.6%; 95% CI, 59.9%-65.3%). Most had a high school degree or received some college education (66.7%; 95% CI, 64.0%-69.4%) and reported no hardship in paying for basic needs (81.5%; 95% CI, 79.4%-83.6%) (Table 1). The survey included residents of 50 states as well as Washington, DC, and Puerto Rico.
Table 1. : Characteristics of the Sample of US Veterans, 2020-2023a
| Characteristic | No. (weighted %) [95% CI] | P valuezoi250366t1n2 | ||
|---|---|---|---|---|
| Total (N = 4503) | Men (3689 [85.4%]) | Women (814 [14.6%]) | ||
| Age group, y | ||||
| 65-70 | 1695 (23.9) [21.9-25.8] | 1307 (20.8) [18.8-22.8] | 388 (42.1) [35.9-48.2] | <.001 |
| 71-75 | 2094 (49.2) [46.3-52.0] | 1801 (51.6) [48.5-54.7] | 293 (34.7) [28.6-40.8] | |
| 76-84 | 714 (27.0) [24-29.9] | 581 (27.6) [24.4-30.9] | 133 (23.2) [16.4-29.9] | |
| Race and ethnicityzoi250366t1n3 | ||||
| Black or African American, non-Hispanic | 844 (13.3) [11.6-15.0] | 663 (11.8) [10.1-13.6] | 181 (22.2) [16.9-27.5] | <.001 |
| Hispanic | 219 (4.2) [3.1-5.4] | 196 (4.7) [3.4-6.0] | 23 (1.6) [0.1-3.1] | |
| White, non-Hispanic | 3253 (78.4) [76.2-80.6] | 2688 (79.6) [77.3-81.9] | 565 (71.4) [65.6-77.2] | |
| Other race, non-Hispanic | 187 (4.0) [2.9-5.1] | 142 (3.9) [2.7-5.1] | 45 (4.8) [2.2-7.4] | |
| Marital status | ||||
| Married, partner, or engaged | 2326 (62.6) [59.9-65.3] | 2105 (67.6) [64.8-70.4] | 221 (33.2) [27-39.3] | <.001 |
| Other (eg, single, divorced) | 2177 (37.4) [34.7-40.1] | 1584 (32.4) [29.6-35.2] | 593 (66.8) [60.7-73] | |
| Educational level | ||||
| Bachelor’s degree and beyond | 1229 (30.7) [28.1-33.3] | 881 (28.6) [25.8-31.5] | 348 (42.8) [36.4-49.2] | <.001 |
| High school graduate, some college | 3100 (66.7) [64.0-69.4] | 2636 (68.4) [65.4-71.3] | 464 (57.1) [50.7-63.5] | |
| Less than high school graduate | 174 (2.6) [1.7-3.4] | 172 (3.0) [2.0-4.0] | 2 (0.1) [0.0-0.1] | |
| Employment (data missing for 2 [0.01%]) | ||||
| Employed | 438 (11.5) [9.7-13.2] | 368 (12.0) [10.1-14.0] | 70 (8.2) [4.9-11.4] | .11 |
| Retired | 2971 (73.3) [70.9-75.8] | 2437 (73.3) [70.6-76.0] | 534 (73.6) [68.1-79.1] | |
| Other | 1092 (15.2) [13.3-17.1] | 882 (14.7) [12.6-16.7] | 210 (18.2) [13.4-23.0] | |
| Hard to pay for basic needs (data missing for 9 [0.2%]) | 1167 (18.3) [16.2-20.4] | 906 (17.0) [14.8-19.2] | 261 (26.1) [20.4-31.8] | .001 |
| Not very hard | 3327 (81.5) [79.4-83.6] | 2776 (82.9) [80.7-85.1] | 551 (73.2) [67.4-79.0] | |
| Has ever used cannabis (data missing for 14 [0.4%])zoi250366t1n4 | 3420 (58.2) [55.3-61.0] | 2827 (58.0) [54.9-61.1] | 593 (59.3) [52.7-66.0] | .77 |
| Past 30-d cannabis usezoi250366t1n5 (data missing for 20 [0.4%]) | ||||
| Current (past 30 d) | 1193 (10.3) [8.9-11.7] | 1018 (10.2) [8.6-11.7] | 175 (11.1) [7.6-14.5] | .90 |
| No current (more than past 30 d) | 2221 (47.9) [45.1-50.7] | 1803 (47.8) [44.7-50.9] | 418 (48.3) [41.8-54.8] | |
| Never | 1069 (41.5) [38.6-44.3] | 849 (41.6) [38.5-44.7] | 220 (40.6) [34.0-47.3] | |
| Past 30-d forms of cannabis use | ||||
| Smoking (data missing for 18 [0.4%]) | 986 (7.4) [6.3-8.6] | 869 (7.7) [6.5-8.9] | 117 (5.9) [3.5-8.3] | .23 |
| Vaping (data missing for 20 [0.5%]) | 170 (1.2) [0.8-1.6] | 141 (1.1) [0.7-1.6] | 29 (1.4) [0.4-2.5] | .60 |
| Dabbing (data missing for 23 [0.6%]) | 32 (0.2) [0.1-0.3] | 28 (0.2) [0.1-0.3] | 4 (0.1) [0.0-0.2] | .33 |
| Edibles (data missing for 26 [0.5%]) | 339 (3.8) [2.8-4.7] | 257 (3.2) [2.2-4.2] | 82 (7.4) [4.3-10.5] | .001 |
| Frequent past 30-d cannabis use (≥20 d; data missing for 21 [0.4%]) | 753 (5.4) [4.4-6.4] | 650 (5.5) [4.4-6.6] | 103 (5.0) [2.9-7.0] | |
| Nonfrequent past 30-d use | 439 (4.9) [3.9-5.9] | 367 (4.7) [3.6-5.8] | 72 (6.1) [3.2-9.0] | .53 |
| No past 30-d use | 3290 (89.3) [87.9-90.8] | 2652 (89.4) [87.8-91] | 638 (88.9) [85.4-92.4] | |
| Any past 12-mo cannabis use disorder (≥2 criteria)zoi250366t1n6 | 546 (3.7) [3.0-4.4] | 490 (3.9) [3.1-4.7] | 56 (2.7) [1.1-4.4] | .23 |
| Past 12-mo cannabis use disorder criteria | ||||
| 0 | 433 (4.8) [3.7-5.9] | 343 (4.4) [3.3-5.6] | 90 (6.9) [4.0-9.9] | .25 |
| 1 | 211 (1.7) [1.2-2.3] | 182 (1.8) [1.1-2.5] | 29 (1.4) [0.4-2.4] | |
| 2-3 (Mild) | 336 (2.4) [1.8-2.9] | 306 (2.5) [1.8-3.1] | 30 (1.7) [0.3-3.2] | |
| 4-5 (Moderate) | 144 (1.1) [0.7-1.5] | 127 (1.2) [0.7-1.6] | 17 (0.8) [0.0-1.5] | |
| ≥6 (Severe) | 66 (0.3) [0.2-0.3] | 57 (0.3) [0.2-0.3] | 9 (0.2) [0.1-0.4] | |
| Not applicable | 3313 (89.7) [88.3-91.1] | 2674 (89.9) [88.3-91.4] | 639 (88.9) [85.5-92.4] | |
| Medical cannabis legalization status (vs not legal) | 3152 (66.1) [63.4-68.7] | 2620 (66.6) [63.7-69.5] | 532 (63.1) [56.8-69.4] | .32 |
| Recreational and medical cannabis legalization status (vs not legal) | 1694 (29.9) [27.3-32.4] | 1374 (29.3) [26.5-32.1] | 320 (33.4) [27.4-39.5] | .21 |
| State cannabis legalization status | ||||
| Nonlegal | 1351 (33.9) [31.3-36.6] | 1069 (33.4) [30.5-36.3] | 282 (36.9) [30.6-43.2] | .10 |
| Medical only | 1458 (36.2) [33.5-38.9] | 1246 (37.3) [34.3-40.3] | 212 (29.7) [23.6-35.8] | |
| Recreational and medical | 1694 (29.9) [27.3-32.4] | 1374 (29.3) [26.5-32.1] | 320 (33.4) [27.4-39.5] | |
| Any past 30-d tobacco use (any tobacco smoking or e-cigarette use; data missing for 5 [0.2%]) | ||||
| Current (>16 d in the past month) | 800 (11.7) [10.1-13.4] | 666 (11.6) [9.8-13.4] | 134 (12.6) [8.3-16.8] | <.001 |
| No current use | 2521 (56.8) [54.0-59.5] | 2173 (60.0) [56.9-63] | 348 (38.0) [31.7-44.2] | |
| Never | 1177 (31.3) [28.7-34.0] | 846 (28.3) [25.4-31.2] | 331 (49.1) [42.6-55.6] | |
| AUDIT-C (data missing for 9 [0.1%]) | ||||
| Negative | 3365 (75.5) [73.1-77.9] | 2707 (75.1) [72.4-77.7] | 658 (78.1) [72.9-83.3] | .34 |
| Positive | 1129 (24.4) [22.0-26.8] | 973 (24.8) [22.1-27.4] | 156 (21.9) [16.7-27.1] | |
| Past 30-d illicit drug use (data missing for 25 [0.3%])zoi250366t1n7 | 57 (0.3) [0.1-0.4] | 56 (0.3) [0.2-0.4] | 1 (0.0) [0.0-0.1] | .003 |
| ≥10 Symptoms based on GAD-7 (data missing for 3 [0.1%]) | 814 (11.7) [10.0-13.4] | 643 (10.5) [8.7-12.2] | 171 (19.1) [13.8-24.3] | <.001 |
| ≥10 Depressive symptoms based on PHQ-8 (data missing for 8 [0.1%]) | 986 (13.1) [11.3-14.9] | 772 (12.0) [10.1-13.9] | 214 (19.5) [14.4-24.7] | .002 |
| ≥19 Symptoms based on PCL-8 inventory (data missing for 7 [0.1%]) | 449 (6.0) [4.8-7.3] | 344 (5.3) [4.0-6.6] | 105 (10.3) [6.3-14.3] | .005 |
| Loneliness (data missing for 3 [0.01%]) | ||||
| Not lonely | 3285 (81.7) [79.6-83.8] | 2759 (83.1) [80.9-85.3] | 526 (73.4) [67.9-78.9] | <.001 |
| Lonely | 1215 (18.3) [16.2-20.3] | 927 (16.9) [14.7-19.1] | 288 (26.6) [21.1-32.1] | |
| Getting social support in COVID-19 (data missing for 14 [0.2%]) | ||||
| Extremely or very difficult | 167 (2.5) [1.6-3.3] | 134 (2.3) [1.4-3.3] | 33 (3.2) [1.1-5.2] | .44 |
| Other | 4322 (97.3) [96.4-98.2] | 3541 (97.4) [96.4-98.4] | 781 (96.8) [94.8-98.9] | |
| CAN score (data missing for 9 [0.5%]) | ||||
| <50 | 1274 (27.5) [25.1-29.8] | 892 (23.9) [21.4-26.3] | 382 (48.6) [42.1-55.1] | <.001 |
| 50 to <75 | 1953 (43.1) [40.3-45.8] | 1631 (43.5) [40.4-46.5] | 322 (40.6) [34.0-47.2] | |
| ≥75 | 1267 (29.0) [26.3-31.8] | 1161 (32.3) [29.2-35.4] | 106 (9.7) [5.6-13.8] | |
| ≥1 Deficit in activities of daily life support (data missing for 16 [0.4%]) | 1663 (32.3) [29.7-35.0] | 1176 (28.6) [25.7-31.4] | 487 (54.6) [48.1-61.0] | <.001 |
| Falls in the past 12 mo (data missing for 3 [0.01%]) | 1740 (34.4) [31.7-37.1] | 1338 (32.7) [29.7-35.6] | 402 (44.5) [38.1-51.0] | <.001 |
Data are unweighted numbers and weighted percentages together with the 95% CIs for the total sample (unless otherwise specified) and by gender.
P values shown are for comparisons that included 3 groups: (1) those who reported past 30-day cannabis use with cannabis use disorder (CUD), those who reported past 30-day cannabis use without CUD, and (3) not applicable (no use or missing). P values shown are for F statistics from Rao-Scott χ2 tests for categorical variables while excluding missing or noneligible respondents.
The White, non-Hispanic category also included respondents who identified as White of unknown ethnicity (n = 85 [1.2%]); the Black or African American, non-Hispanic category also included respondents who identified as Black or African American of unknown ethnicity (n = 13 [0.3%]). The other race, non-Hispanic category included respondents of another race (31 [0.8%] Asian, 50 [1.0%] American Indian or Alaska Native, and 43 [0.6%] Native Hawaiian or Other Pacific Islander), of multiple races (n = 1 [0.004%]), or of unknown or unreported race or ethnicity (62 [1.6%]).
Affirmative responses to the question, “Have you ever used marijuana in any form?” regardless of the form of use.
Smoking, vaping, dabbing, or use of edibles in the past 30 days.
Cannabis use disorder was defined as reporting any 2 or more of the following 11 criteria among those who reported past 30-day use: tolerance; withdrawal or high use; taken in larger amounts or during a longer period than intended; a great deal of time getting, using, or recovering from use; important activities given up; recurrent psychological or physical problems; hazardous use; recurrent social problems; failure to fulfill obligations; craving; and/or persistent desire to cut down.
Includes cocaine, heroin, amphetamines, or other illicit drugs.
Abbreviations: AUDIT-C, Alcohol Use Disorders Identification Test–Consumption; CAN, Care Assessment Need; GAD-7, 7-item Generalized Anxiety Disorder; PCL-8, 8-item Posttraumatic Stress Disorder Checklist for the Diagnostic and Statistical Manual of Mental Disorders; PHQ-8, 8-item Patient Health Questionnaire.
Lifetime Cannabis Use
More than half of the respondents (57.4%; 95% CI, 54.6%-60.3%) reported lifetime cannabis use in the form of smoking, vaping, dabbing, or edibles, and 14.1% (95% CI, 12.5%-15.8%) reported last-year use (eFigure 1 in Supplement 1). Smoking cannabis was the most common form (97.2%; 95% CI, 96.0%-98.4%), followed by the use of edibles (34.3%; 95% CI, 31.2%-37.4%) (eFigure 2 in Supplement 1).
Among those with available data on forms of lifetime cannabis use including topicals (n = 3409), 28.9% (95% CI, 26.0%-31.8%) reported any medical use: 16.7% (95% CI, 14.5%-18.8%) used cannabis for both medical and recreational purposes, and 12.3% (95% CI, 10.1%-14.5%) used medicinal cannabis only (eFigure 3 in Supplement 1). The most common reasons for any medical use were management of pain (any: 56.4%; 95% CI, 50.9%-61.9%; general or vascular: 33.4%; 95% CI, 28.1%-38.6%; muscle or skeletal: 24.8%; 95% CI, 19.9%-29.7%), sleep difficulties (16.0%; 95% CI, 11.9%-20.0%), arthritis (11.3%; 95% CI, 8.0%-14.6%), and mood or mental health concerns (any: 18.4%; 95% CI, 14.7%-22.1%; anxiety: 9.9%; 95% CI, 6.9%-13.0%; PTSD: 6.8%; 95% CI, 4.6%-9.0%; depression: 4.5%; 95% CI, 3.1%-5.9%) (eFigure 4 in Supplement 1).
Past 30-Day Use
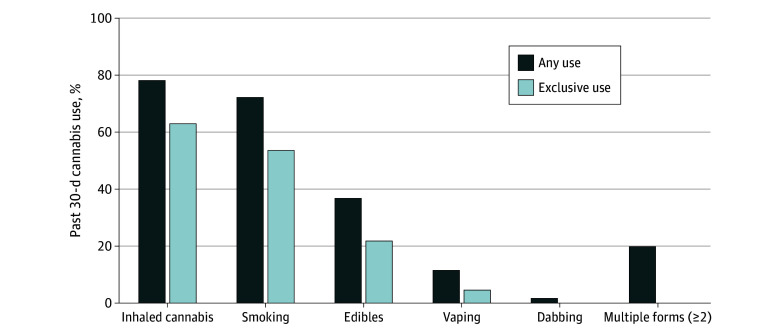
More than 1 in 10 respondents (10.3%; 95% CI, 8.9%-11.7%) reported past 30-day cannabis use (Table 1). More women than men used edibles in the past month (7.4% [95% CI, 4.3%-10.5%] vs 3.2% [95% CI, 2.2%-4.2%]; P = .001), whereas other forms of use did not differ by gender (Table 1). Among those with past 30-day cannabis use (n = 1193), smoking (72.4%; 95% CI, 65.4%-79.3%; median [IQR] years of daily cannabis smoking, 19.1 [1.3-39.4]) and use of edibles (36.9%; 95% CI, 29.8%-43.9%) were the most common, and 19.9% (95% CI, 14.9%-24.9%) reported 2 or more forms of use (Figure 2). Many of those who reported edible cannabis use also inhaled cannabis (41.2%; 95% CI, 29.4%-52.9%). More than half of those with past 30-day use (52.4%; 95% CI, 45.4%-59.4%) used cannabis frequently.
In the weighted multivariable logistic regression analysis, past 30-day cannabis use (vs no past 30-day use) was more likely reported among younger respondents (aged 65-70 vs 76-84 years: adjusted odds ratio [AOR], 2.86; 95% CI, 1.59-5.17; aged 71-75 vs 76-84 years: AOR, 2.04; 95% CI, 1.13-3.69); participants who were not (vs were) married or in a relationship (AOR, 1.85; 95% CI, 1.30-2.64); those who were not retired or employed vs retired (AOR, 1.55; 95% CI, 1.07-2.26); those who experienced economic hardships (vs those who did not) (AOR, 1.61; 95% CI, 1.05-2.45); those who reported current tobacco use (AOR, 2.78; 95% CI, 1.66-4.64) and past tobacco use (AOR, 1.92; 95% CI, 1.19-3.10) vs no lifetime use; those with any illicit drug use (vs none) in the past month (AOR, 2.72; 95% CI, 1.14-6.49); those who had a positive (vs negative) AUDIT-C score (AOR, 1.47; 95% CI, 1.04-2.06); and those who resided in states with recreational (vs nonlegal) cannabis status (AOR, 2.53; 95% CI, 1.71-3.75) (Table 2).
Table 2. : Correlates of Past 30-Day Cannabis Use for Respondents With Available Data on Cannabis Smoking, Vaping, Dabbing, and Use of Edibles in 4483 US Veterans, 2020-2023a
| Characteristic | No. (weighted %) [95% CI] | AOR (95% CI)zoi250366t2n3 | P valuezoi250366t2n3 | |
|---|---|---|---|---|
| Past 30-d use (n = 1193)zoi250366t2n2 | No past 30-d use (n = 3290) | |||
| Age group, y | ||||
| 65-70 | 558 (36.0) [30.0-41.9] | 1126 (22.5) [20.4-24.6] | 2.86 (1.59-5.17) | <.001 |
| 71-75 | 521 (49.2) [42.3-56.2] | 1565 (49.2) [46.1-52.2] | 2.04 (1.13-3.69) | .02 |
| 76-84 | 114 (14.8) [8.1-21.6] | 599 (28.4) [25.2-31.5] | 1 [Reference] | NA |
| Gender | ||||
| Men | 1018 (84.3) [79.6-89.1] | 2652 (85.5) [83.6-87.5] | 1.03 (0.62-1.71) | .90 |
| Women | 175 (15.7) [10.9-20.4] | 638 (14.5) [12.5-16.4] | 1 [Reference] | NA |
| Race and ethnicity | ||||
| Black or African American, non-Hispanic | 259 (18.0) [13.3-22.7] | 582 (12.8) [11.0-14.7] | 1.17 (0.79-1.75) | .43 |
| Hispanic | 53 (4.8) [1.9-7.8] | 166 (4.2) [3.0-5.4] | 0.98 (0.49-1.96) | .95 |
| White, non-Hispanic | 835 (73.6) [68.0-79.3] | 2402 (78.9) [76.5-81.2] | 1 [Reference] | NA |
| Other race, non-Hispaniczoi250366t2n4 | 46 (3.6) [1.3-5.9] | 140 (4.1) [2.9-5.3] | 0.82 (0.35-1.93) | .66 |
| Marital status | ||||
| Other | 669 (55.4) [48.4-62.3] | 1500 (35.4) [32.6-38.3] | 1.85 (1.30-2.64) | <.001 |
| Married, partner, or engaged | 524 (44.6) [37.7-51.6] | 1790 (64.6) [61.7-67.4] | 1 [Reference] | NA |
| Educational level | ||||
| Less than high school graduate | 53 (3.0) [1.4-4.5] | 121 (2.5) [1.6-3.5] | 0.77 (0.36-1.64) | .50 |
| High school graduate or some college | 858 (69.8) [63.3-76.2] | 2230 (66.5) [63.6-69.4] | 0.85 (0.56-1.28) | .43 |
| Bachelor’s degree and beyond | 282 (27.3) [20.9-33.7] | 939 (30.9) [28.1-33.8] | 1 [Reference] | NA |
| Employment (n = 4480) | ||||
| Employed | 91 (7.6) [4.0-11.1] | 343 (11.8) [9.9-13.7] | 0.56 (0.30-1.03) | .06 |
| Other | 332 (25.2) [19.4-31.1] | 755 (14.1) [12.0-16.1] | 1.55 (1.07-2.26) | .02 |
| Retired | 770 (67.2) [60.8-73.6] | 2190 (74.1) [71.5-76.7] | 1 [Reference] | NA |
| Hard to pay for basic needs (n = 4474)zoi250366t2n5 | 347 (28.8) [22.3-35.3] | 811 (17.2) [15.0-19.4] | 1.61 (1.05-2.45) | .03 |
| Not very hard | 844 (71.1) [64.6-77.6] | 2472 (82.7) [80.5-84.9] | 1 [Reference] | NA |
| State cannabis legalization status | ||||
| Nonlegal | 299 (24.1) [18.6-29.6] | 1046 (35.1) [32.2-38.0] | 1 [Reference] | NA |
| Medical only | 390 (33.5) [26.8-40.1] | 1062 (36.6) [33.6-39.6] | 1.43 (0.94-2.16) | .10 |
| Recreational and medical | 504 (42.4) [35.5-49.4] | 1182 (28.3) [25.6-31.0] | 2.53 (1.71-3.75) | <.001 |
| Any past 30-d tobacco use (n = 4479)zoi250366t2n6 | ||||
| Current (>16 d in the past month) | 347 (21.8) [16.9-26.7] | 451 (10.6) [8.9-12.4] | 2.78 (1.66-4.64) | <.001 |
| No current use | 674 (59.5) [52.7-66.2] | 1833 (56.4) [53.4-59.4] | 1.92 (1.19-3.10) | .007 |
| Never | 172 (18.7) [12.8-24.6] | 1002 (32.8) [29.9-35.7] | 1 [Reference] | NA |
| AUDIT-C (n = 4476) | ||||
| Positive | 415 (32.3) [26.1-38.6] | 706 (23.3) [20.8-25.9] | 1.47 (1.04-2.06) | .03 |
| Negative | 776 (67.6) [61.4-73.9] | 2579 (76.5) [73.9-79.1] | 1 [Reference] | NA |
| Past 30-d illicit drug use (n = 4463) | 32 (1.2) [0.7-1.6] | 25 (0.2) [0.0-0.3] | 2.72 (1.14-6.49) | .02 |
| ≥10 Symptoms based on the GAD-7 (n = 4480) | 187 (12.3) [7.9-16.7] | 625 (11.7) [9.8-13.5] | 0.73 (0.41-1.29) | .28 |
| ≥10 Depressive symptoms based on the PHQ-8 (n = 4475) | 251 (17.5) [12.4-22.6] | 730 (12.6) [10.7-14.5] | 1.44 (0.86-2.42) | .17 |
| ≥19 Symptoms based on PCL-8 inventory (n = 4476) | 99 (5.6) [3.2-8.0] | 348 (6.1) [4.7-7.5] | 0.69 (0.36-1.31) | .26 |
| Loneliness (n = 4480) | ||||
| Not lonely | 849 (77.2) [71.8-82.7] | 2423 (82.2) [80.0-84.4] | 1 [Reference] | NA |
| Lonely | 342 (22.7) [17.2-28.2] | 866 (17.8) [15.6-20.0] | 0.96 (0.64-1.43) | .83 |
| CAN score (n = 4474) | ||||
| <50 | 308 (27.7) [21.8-33.7] | 962 (27.5) [25.0-30.1] | 1 [Reference] | NA |
| 50 to <75 | 539 (42.7) [35.9-49.5] | 1405 (43.1) [40.1-46.1] | 1.12 (0.78-1.61) | .54 |
| ≥75 | 343 (29.4) [22.6-36.2] | 917 (28.9) [25.9-31.9] | 1.30 (0.84-2.02) | .23 |
| ≥1 Deficit in activities of daily life support (n = 4467) | 409 (32.3) [25.9-38.8] | 1248 (32.4) [29.5-35.3] | 0.96 (0.65-1.44) | .86 |
| Falls in the past 12 mo (n = 4480) | 420 (29.3) [23.4-35.1] | 1314 (34.9) [32.0-37.8] | 0.71 (0.50-1.03) | .07 |
Data are unweighted numbers and weighted percentages together with the 95% CIs by past 30-day cannabis use for respondents with available data on past 30-day cannabis use (n = 4483; data missing for 20 [0.4%]).
Smoking, vaping, dabbing, or use of edibles in the past 30 days.
Results obtained from adjusted logistic regression with all listed variables entered simultaneously; past 30-day use is the outcome variable: 4403 observations used (data missing for 100 [2.2%] of the total sample): 1166 reporting past 30-day cannabis use vs 3237 reporting no past 30-day use.
The other race, non-Hispanic category included respondents of another race (31 [0.8%] Asian, 50 [1.0%] American Indian or Alaska Native, and 42 [0.6%] Native Hawaiian or Other Pacific Islander), of multiple races (1 [0.004%]), or of unknown or not reported race or ethnicity (62 [1.6%]).
Reported very hard, hard, or somewhat hard to pay for basic needs or reported being homeless, living in a shelter, a mobile home, or in a single room in a building.
Smoking cigarettes, cigarillos, cigars, or pipes or using e-cigarettes for more than 16 days in the past month.
Abbreviations: AOR, adjusted odds ratio; AUDIT-C, Alcohol Use Disorders Identification Test–Consumption; CAN, Care Assessment Need; GAD-7, 7-item Generalized Anxiety Disorder; NA, not applicable; PCL-8, 8-item Posttraumatic Stress Disorder Checklist for the Diagnostic and Statistical Manual of Mental Disorders; PHQ-8, 8-item Patient Health Questionnaire.
Cannabis Use Disorder
Of 1190 respondents with past 30-day cannabis use and available data on CUD diagnostic criteria, 36.3% (95% CI, 30.1%-42.6%) met our past 12-month CUD definition (or 3.7% [95% CI, 3.0%-4.4%] in the total sample) (Table 1; eFigure 1 in Supplement 1), including 22.9% (95% CI, 17.7%-28.1%) with mild, 10.9% (95% CI, 7.0%-14.8%) with moderate, and 2.5% (95% CI, 1.8%-3.2%) with severe CUD (eFigure 5 in Supplement 1). In the weighted multivariable logistic regression analysis, men, respondents younger than 76 years, those who experienced anxiety, those who reported frequent cannabis use or any illicit drug use in the past month, and those who reported 1 or more deficits in ADLs were more likely to have any CUD (eTable 4 in Supplement 1). Lifetime cannabis use for exclusively medical reasons compared with any recreational use (recreational only or combined with medical use) was associated with lower odds of any CUD (≥2 criteria). Frequent past 30-day cannabis use was the highest among those who had ever used cannabis for both medical and recreational purposes (61.0%; 95% CI, 52.4%-69.6%), followed by those who used medical cannabis only (53.3%; 95% CI, 38.1%-68.6%), and was the lowest among respondents who only used recreational cannabis (30.4%; 95% CI, 15.9%-44.9%) (eFigure 6 in Supplement 1).
Secondary Analysis: Associations of CUD With Forms and Frequency of Cannabis Use
In the weighted multivariable logistic regression analysis, past 30-day use of any inhaled cannabis vs edibles only was associated with higher odds of any CUD (AOR, 3.56; 95% CI, 1.12-11.26) (Table 3) and vice versa: use of edibles only vs any inhaled cannabis was associated with lower odds of any CUD (model 3) (see eTable 5 in Supplement 1 for reciprocal results). Most respondents who used any inhaled cannabis reported daily or near-daily use (61.0%; 95% CI, 53.9%-68.1%), whereas those who exclusively consumed edibles were less likely to use cannabis frequently (21.5%; 95% CI, 7.3%-35.7%). Frequent past 30-day cannabis use was independently associated with higher odds of any CUD in all models (Table 3).
Table 3. : Association of Forms of Use With Any Past 12-Month CUD Among 1193 US Veterans Who Reported Any Past 30-Day Cannabis Use Adjusted by Age and Gender, 2020-2023a
| Characteristic | No. (weighted %) [95% CI] | CUD, No. (%) [95% CI] | Model 1 (CUD vs no CUD)zoi250366t3n2 | Model 2 (CUD vs no CUD)zoi250366t3n3 | ||
|---|---|---|---|---|---|---|
| AOR (95% CI)zoi250366t3n4 | P value | AOR (95% CI)zoi250366t3n4 | P value | |||
| Use | ||||||
| Any smoking | 986 (72.4) [65.4-79.3] | 494 (43.0) [35.8-50.2] | 2.08 (0.87-4.99) | .10 | NA | NA |
| Any vaping | 170 (11.5) [7.7-15.3] | 83 (43.2) [26.4-59.9] | 1.26 (0.47-3.40) | .65 | ||
| Any dabbing | 32 (1.7) [0.6-2.8] | 25 (56.7) [21.2-92.2] | 1.10 (0.18-6.79) | .91 | ||
| Any edibles | 339 (36.9) [29.8-43.9] | 132 (27.6) [17.4-37.7] | 1.05 (0.53-2.10) | .89 | ||
| Frequent past 30-d usezoi250366t3n5 | 753 (52.4) [45.4-59.4] | 392 (44.9) [36.2-53.7] | 2.14 (1.24-3.71) | .007 | 2.02 (1.16-3.51) | .01 |
| Form of use | ||||||
| Edibles only | 135 (21.7) [14.9-28.5] | 22 (10.2) [0.62-19.8] | NA | NA | 1 [Reference] | NA |
| Any inhaled use | 1058 (78.3) [71.5-85.1] | 524 (43.5) [36.5-50.5] | NA | NA | 3.56 (1.12-11.26) | .03 |
| Age group, y | ||||||
| 65-70 | 558 (36.0) [30.0-41.9] | 263 (43.6) [35.4-51.8] | 5.40 (2.11-13.82) | <.001 | 5.49 (2.15-14.02) | <.001 |
| 71-75 | 521 (49.2) [42.2-56.2] | 241 (38.4) [28.8-48.0] | 4.80 (1.80-12.75) | .002 | 4.96 (1.89-13.03) | .001 |
| 76-84 | 114 (14.8) [8.1-21.6] | 42 (11.5) [4.8-18.2] | 1.0 [Reference] | NA | 1 [Reference] | NA |
| Gender | ||||||
| Men | 1018 (84.3) [79.6-89.1] | 490 (38.4) [31.5-45.4] | 1.86 (0.81-4.24) | .14 | 1.63 (0.71-3.72) | .25 |
| Women | 175 (15.7) [10.9-20.4] | 56 (24.7) [11.6-37.9] | 1.0 [Reference] | NA | 1 [Reference] | NA |
| Reasons for lifetime cannabis use | ||||||
| Medical only | 278 (26.5) [19.9-33.2] | 80 (18.3) [9.3-27.3] | 0.35 (0.17-0.71) | .004 | 0.36 (0.18-0.73) | .005 |
| Recreational only or both | 912 (73.4) [66.7-80.0] | 465 (42.8) [35.4-50.2] | 1.0 [Reference] | NA | 1 [Reference] | NA |
Data are unweighted numbers, weighted percentages, and 95% CIs for forms of use (not mutually exclusive) and covariates among those who reported past 30-day cannabis use (n = 1193) and row percentages together with the 95% CIs (for CUD).
Model 1 variables were reporting smoking, vaping, dabbing, or use of edibles while adjusting for age, gender, frequency of past 30-day cannabis use, and reasons for lifetime cannabis use (n = 1182: 545 with CUD vs 637 without CUD).
Model 2 variables were a 2-level variable indicating forms of cannabis use (any inhaled cannabis use vs edibles only) while adjusting for age, gender, frequency of past 30-day cannabis use, and reasons for lifetime cannabis use (n = 1189: 545 with CUD vs 644 without CUD).
The AORs for forms of use are shown in associations with the outcome variable of CUD, which is defined as reporting any 2 of the following 11 criteria: tolerance; withdrawal; cannabis taken in larger amounts or during a longer period than intended; a great deal of time getting, using, or recovering from use; important activities given up; recurrent psychological or physical problems; hazardous use; recurrent social problems; failure to fulfill obligations; craving; and/or persistent desire to cut down.
Smoking, vaping, dabbing, or using edibles 20 or more days in the past 30 days.
Abbreviations: AOR, adjusted odds ratio; CUD, cannabis use disorder; NA, not applicable.
Sensitivity analyses revealed that before adjusting for frequency of use, cannabis smoking was associated with higher odds of any CUD (model 1) (eTable 5 in Supplement 1), whereas the association was nonsignificant after controlling for frequent use (model 1) (Table 3). The finding of lower odds of any CUD with exclusive use of edibles (reciprocally, higher odds of any CUD with any inhaled cannabis) were consistently significant before and after adjustments for frequency of use (models 2-3) (eTable 5 in Supplement 1).
Sensitivity analyses examining associations of forms of use with moderate to severe CUD (≥4 criteria: 13.4%; 95% CI, 9.4%-17.4%) among those with past 30-day cannabis use confirmed our primary findings indicating that inhaled (vs edibles only) cannabis use, especially smoking, was associated with moderate to severe CUD regardless of frequency of use (models 4-5) (eTable 5 in Supplement 1). Unlike our primary models with the overall CUD outcome (≥2 criteria), exclusive medical cannabis use compared with recreational use was no longer significantly associated with lower odds for moderate to severe CUD (models 4-5) (eTable 5 in Supplement 1).
Discussion
In this cross-sectional study of a nationally representative sample of older veterans 65 years and older who received treatment in the VHA, more than 1 in 10 reported past 30-day cannabis use, suggesting almost 2 times higher prevalence of cannabis use compared with their counterparts 65 years or older in the general population (5.2% in 20229). Cannabis consumption on a daily or near-daily basis among those currently using cannabis was common, and more than one-third of those with past 30-day use had at least mild CUD. Prevalence of past 30-day cannabis use was close to that of past 30-day tobacco use, supporting previous studies showing that increasing cannabis use among US adults is approaching tobacco use rates.1,15,66,67,68 Our findings highlight the importance of screening older veterans for frequent and disordered cannabis use and informing older veterans about the risks of developing CUD.
CUD was more prevalent among respondents of younger age (65-75 vs ≥76 years) and those who used illicit drugs, frequently used cannabis, or had anxiety or 1 or more deficits in ADLs. In line with prior research,41 respondents reporting lifetime cannabis use exclusively for medical reasons vs recreationally were less likely to report any CUD. However, the odds for moderate to severe CUD did not differ significantly among those who used cannabis recreationally vs for medical reasons only. A novel finding of our secondary analysis was that veterans who used inhaled cannabis had higher adjusted odds of CUD compared with those who used edibles only, independently of frequency of use. In contrast, those who exclusively used edibles were less likely to report CUD. Previous studies have shown that higher potency of cannabis products may increase the risk of CUD.69,70 Inhaled modes of cannabis administration, especially vaping and dabbing concentrates, can deliver high levels of tetrahydrocannabinol (THC), which may explain our finding that inhaled forms of cannabis are associated with higher odds of CUD.71,72,73
It is concerning that the weighted percentage of CUD among veterans 65 years or older engaging in past 30-day cannabis use (36.3%) was at the higher end of the CUD prevalence reported among people who use cannabis in the general US population.54,74,75 Besides differences in the nature of our study being based on VHA patients vs the general population in prior research,54,74,75 the comparisons with past observational studies may be complicated by variations in the time interval of cannabis use chosen (ie, lifetime, past-year, or past-month use) and discrepancies in the CUD definition, which was based on the DSM-557 in our survey compared with Diagnostic and Statistical Manual of Mental Disorders (Third or Fourth Edition) diagnostic criteria or International Statistical Classification of Diseases, Tenth Revision codes used in prior studies.54 The weighted CUD prevalence (3.7%) in the total sample of our study, which is representative of the VHA patients aged 65 to 80 years who met the eligibility criteria, was higher but still comparable with a study in veterans (mean [SD] age, 62.2 [15.7] years) in 2019 to 2020, which reported 2.7% of past 6-month CUD based on the Cannabis Use Disorder Identification Test–Revised (CUDIT-R).48 Another study in VHA patients (mean [SD] age, 57 [14.4] years) also showed similar CUD prevalence in 2019 while using clinician-based CUD diagnostic codes: 2.25% in states with nonlegal cannabis, followed by states with medical (2.54%) and recreational (2.56%) cannabis laws.16
The weighted prevalence of past-year cannabis use among the VHA patients in our study was higher compared with 2022 estimates for their counterparts 65 years or older in the civilian population: 14.1% vs 8.4%.9 However, the patterns and correlates of past 30-day cannabis use were consistent with findings in the general population.3,42,76 Smoking was the most common form of cannabis use in our sample, and use of edibles was higher in women vs men, similar to what has been observed in the general population of adults 60 years or older.5 Frequency of past 30-day cannabis use was independently associated with higher odds of any CUD, similar to prior research linking frequent cannabis use to increased CUD risk.37,38 Sociodemographic correlates of past 30-day cannabis use in older veterans were similar to those reported in past research of civilian populations42,76 and indicated socioeconomic disparities in cannabis use, which was higher among those who were younger (65-75 vs ≥76 years), unemployed or experiencing financial hardships, and unmarried or unpartnered. In line with previous studies in veterans 18 years or older,43,44,45,77 our findings showed higher cannabis use among respondents who resided in states with cannabis legalization (also in line with studies of non-VHA clinical populations17) and those reporting alcohol, tobacco, and illicit drug use, suggesting the need for cannabis use screening among veterans with these characteristics.
Compared with the general population, veterans are more likely to report mental health issues53,78,79 and substance use disorders80 and have higher suicide risk.81 It was expected that 1 of the top 3 reasons for lifetime medical cannabis use among the VHA patients in our study was management of mental health concerns, including anxiety, depression, and PTSD. Although anxiety was associated with higher odds of CUD, there were no differences by depression or PTSD status. This finding may reflect VHA patients’ greater access to evidence-based therapy and treatment options recommended by VHA clinicians as alternatives to cannabis use.82
Given rapid cannabis legalization affecting rates of use1 and CUD16 and increasing social acceptance of cannabis use,10,18 more focus is needed on negative health consequences of cannabis use in older veterans, such as higher risk for cardiovascular31,32,33,34 and respiratory health outcomes,30 neuropsychiatric disorders,26,27,28,29 and development of CUD.36 Older veterans may be at risk for THC intoxication, not tolerating cannabis potency that has increased in recent years83,84,85 or latent THC components found in products that are being marketed as cannabidiol only.24 Prevention of problematic cannabis use and CUD is also crucial in older veterans due to the elevated risk of suicide ideation48 and exacerbation of mental health concerns86 experienced by aging populations.
Findings from past research and our study highlight a potential need to include screening for cannabis use in clinical settings and to reinforce efforts to prevent CUD among veterans 65 years or older. Although the US Preventive Services Task Force87 recommends screening for any unhealthy substance use,88 the VA has opted not to engage in universal drug screening or screening for cannabis use at this juncture. The common and frequent cannabis use among older veterans in our study is concerning and suggests that this decision may need to be reconsidered. Past and emerging studies emphasize the importance of integrating cannabis screening and assessment for CUD in the primary care setting,89,90,91 which can be implemented via the Alcohol Substance Involvement Screening Test,91 Drug Abuse Screening Test 10,92 and Single-item Screen-Cannabis,93 with a follow-up assessment of CUD via DSM-557 or Substance Use Symptom Checklist (a scaled measure of DSM-5)90 or CUDIT-R.48 Improved identification of patients at risk or with CUD can also help with linkage to care or referrals.90,91 Current VA guidelines recommend that patients with CUD be offered referral to mental health services for evidence-based treatments, including motivational interviews,94 contingency management,95 and cognitive behavioral therapy.96 However, if unidentified, patients cannot be offered existing evidence-based treatments. Despite increasing cannabis use among older adults, there is an inadequate evidence base on therapeutic benefits and potential harms from cannabis use among older people.25,97 Screening and informing older veterans about risks of cannabis use is critical because cannabis use may confer more health risks25,26,27,28,29,30,31,32,33,34,98 than benefits.99,100,101
Limitations
This study has some limitations. First, this was a cross-sectional study, which precludes prospective examination of associations between patient characteristics and patterns of cannabis use. Second, this was an EHR-based cohort of US veterans 65 years or older; thus, results may not generalize to nonveteran or non-VHA populations53 or women. However, we oversampled women to ensure representation in the study. Third, these were self-reported data, provided via telephone interviews, regarding lifetime substance use behaviors; thus, recall and social desirability biases may have occurred. Responses about cannabis use could have varied by cannabis legalization status of the state of residence. It is possible that some participants did not accurately report their cannabis use. However, self-report is considered an accepted and valid method of assessing substance use used in many cohort studies102,103 and in national surveys.3,5,76 Furthermore, participants in this study were provided a National Institutes of Health Certificate of Confidentiality to reassure them that their data responses would remain private. Although self-administered online questionnaires can mitigate social-report biases for collection of sensitive data,104,105 telephone interviews used in the study may be a more effective method for data collection among older adults, as in our study.
Conclusions
To our knowledge, this was the first large national study that used combined EHR and participant interview data to examine factors associated with current cannabis use and CUD among older veterans. Cannabis use was common and similar to estimates reported in younger populations; more than one-third of the participants with past 30-day use had any CUD. Anxiety, use of illicit drugs, frequent past 30-day cannabis use, and use of inhaled vs edible cannabis were associated with higher odds of any CUD. Given high rates of frequent cannabis use and CUD among older veterans, screening for cannabis use in clinical settings may be necessary, alongside referrals to appropriate specialty treatment.
References
- US adult illicit cannabis use, cannabis use disorder, and medical marijuana laws: 1991-1992 to 2012-2013.. JAMA Psychiatry., 2017. [DOI | PubMed]
- 2SAMHSA. Results from the 2013 National Survey on Drug Use and Health: summary of national findings. 2014. Accessed March 26, 2025. https://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.pdf
- 3SAMHSA. Results from the 2023 National Survey on Drug Use and Health: detailed tables. HHS Publication No. PEP24-07-021-006, NSDUH Series H-59. 2024. Accessed October 16, 2024. https://www.samhsa.gov/data/sites/default/files/reports/rpt47095/National%20Report/National%20Report/2023-nsduh-annual-national.pdf
- Marijuana use among adults 50 years or older in the 21st century.. Gerontol Geriatr Med. Published online June 21,, 2018. [DOI | PubMed]
- 5SAMHSA. Behavioral health among older adults: results from the 2021 and 2022 National Surveys on Drug Use and Health. SAMHSA Publication No. PEP24-07-018. 2024. Accessed May 23, 2024. https://www.samhsa.gov/data/report/older-adult-behavioral-health-report-2021-2022
- Demographic trends among older cannabis users in the United States, 2006-13.. Addiction., 2017. [DOI | PubMed]
- The epidemiology of substance use and disorders among middle aged and elderly community adults: national survey on drug use and health.. Am J Geriatr Psychiatry., 2009. [DOI | PubMed]
- Trends in cannabis use among older adults in the United States, 2015-2018.. JAMA Intern Med., 2020. [DOI | PubMed]
- 9SAMHSA. Key substance use and mental health indicators in the united states: results from the 2022 National Survey on Drug Use and Health. Table 1.7B. Marijuana Use in Lifetime, Past Year, and Past Month: Among People Aged 12 or Older; by Detailed Age Category, Percentages, 2021 and 2022. Accessed March 26, 2025. https://www.samhsa.gov/data/sites/default/files/reports/rpt42728/NSDUHDetailedTabs2022/NSDUHDetailedTabs2022/NSDUHDetTabsSect1pe2022.htm
- Perceptions of safety of daily cannabis vs tobacco smoking and secondhand smoke exposure, 2017-2021.. JAMA Netw Open., 2023. [DOI | PubMed]
- Impacts of recreational cannabis legalization on cannabis use: a longitudinal discordant twin study.. Addiction., 2023. [DOI | PubMed]
- Racial and ethnic differences in cannabis use following legalization in US states with medical cannabis laws.. JAMA Netw Open., 2021. [DOI | PubMed]
- Association between recreational marijuana legalization in the United States and changes in marijuana use and cannabis use disorder from 2008 to 2016.. JAMA Psychiatry., 2020. [DOI | PubMed]
- The effect of medical marijuana laws on adolescent and adult use of marijuana, alcohol, and other substances.. J Health Econ., 2015. [DOI | PubMed]
- Cannabis legalization and changes in cannabis and tobacco/nicotine use and co-use in a national cohort of U.S. adults during 2017-2021.. Int J Drug Policy., 2024. [DOI | PubMed]
- State cannabis legalization and cannabis use disorder in the US Veterans Health Administration, 2005 to 2019.. JAMA Psychiatry., 2023. [DOI | PubMed]
- State cannabis legalization and trends in cannabis-related disorders in US older adults, 2017 to 2022.. JAMA Netw Open., 2024. [DOI | PubMed]
- Older adults experiences of using recreational cannabis for medicinal purposes following legalization.. Int J Drug Policy., 2022. [DOI | PubMed]
- Factors associated with having a medical marijuana card among veterans with recent substance use in VA outpatient treatment.. Addict Behav., 2016. [DOI | PubMed]
- Self-reported medicinal cannabis use as an alternative to prescription and over-the-counter medication use among US military veterans.. Clin Ther., 2023. [DOI | PubMed]
- 21Edemekong PF, Bomgaars DL, Sukumaran S, . Activities of daily living. In: StatPearls [Internet]. Updated June 26, 2023. Accessed March 26, 2025. https://www.ncbi.nlm.nih.gov/books/NBK470404/
- Frailty in elderly people.. Lancet., 2013. [DOI | PubMed]
- Surveillance for morbidity and mortality among older adults–United States, 1995-1996.. MMWR CDC Surveill Summ., 1999. [PubMed]
- Cannabis-induced acute encephalopathy in a 94-year-old woman due to family administration of cannabidiol (CBD) products: a case report.. Cureus., 2023. [DOI | PubMed]
- Impacts of medical and non-medical cannabis on the health of older adults: findings from a scoping review of the literature.. PLoS One., 2023. [DOI | PubMed]
- Causal association between cannabis and psychosis: examination of the evidence.. Br J Psychiatry., 2004. [DOI | PubMed]
- Cannabis and schizophrenia: a longitudinal study of Swedish conscripts.. Lancet., 1987. [DOI | PubMed]
- Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study.. BMJ., 2002. [DOI | PubMed]
- Long-term consequences of adolescent cannabinoid exposure in adult psychopathology.. Front Neurosci., 2014. [DOI | PubMed]
- Marijuana use, respiratory symptoms, and pulmonary function.. Ann Intern Med., 2018. [DOI | PubMed]
- What is the current knowledge about the cardiovascular risk for users of cannabis-based products? a systematic review.. Curr Atheroscler Rep., 2017. [DOI | PubMed]
- Association of cannabis use with cardiovascular outcomes among US adults.. J Am Heart Assoc., 2024. [DOI | PubMed]
- One minute of marijuana secondhand smoke exposure substantially impairs vascular endothelial function.. J Am Heart Assoc., 2016. [DOI | PubMed]
- Increased vulnerability to atrial and ventricular arrhythmias caused by different types of inhaled tobacco or marijuana products.. Heart Rhythm., 2023. [DOI | PubMed]
- Adverse cardiovascular outcomes in young cannabis users: a nationwide analysis.. Hearts (Basel)., 2024. [DOI]
- Cannabis use, cannabis use disorder, and comorbid psychiatric illness: a narrative review.. J Clin Med., 2020. [DOI | PubMed]
- Identifying risk-thresholds for the association between frequency of cannabis use and development of cannabis use disorder: a systematic review and meta-analysis.. Drug Alcohol Depend., 2022. [DOI | PubMed]
- Probability and correlates of dependence among regular users of alcohol, nicotine, cannabis, and cocaine: concurrent and prospective analyses of the National Epidemiologic Survey on Alcohol and Related Conditions.. J Clin Psychiatry., 2016. [DOI | PubMed]
- Changes in self-reported cannabis use in the United States from 1979 to 2022.. Addiction., 2024. [DOI | PubMed]
- Nonmedical versus medical marijuana use among three age groups of adults: associations with mental and physical health status.. Am J Addict., 2017. [DOI | PubMed]
- Prevalence of cannabis use disorder and reasons for use among adults in a US state where recreational cannabis use is legal.. JAMA Netw Open., 2023. [DOI | PubMed]
- Prevalence and frequency of cannabis use among adults ages 50-80 in the United States.. Cannabis Cannabinoid Res., 2024. [DOI | PubMed]
- Prevalence and correlates of cannabis use and cannabis use disorder among U.S. veterans: results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC-III).. Am J Psychiatry., 2022. [DOI | PubMed]
- Recent cannabis use among Veterans in the United States: results from a national sample.. Addict Behav., 2018. [DOI | PubMed]
- National trends in past-year marijuana use among veterans in the United States, 2013-2019.. Subst Use Misuse., 2023. [DOI | PubMed]
- Increasing risk of cannabis use disorder among U.S. veterans with chronic pain: 2005-2019.. Pain., 2023. [DOI | PubMed]
- Prevalence of cannabis use disorder diagnoses among veterans in 2002, 2008, and 2009.. Psychol Serv., 2012. [DOI | PubMed]
- Comparative associations of problematic alcohol and cannabis use with suicidal behavior in U.S. military veterans: a population-based study.. J Psychiatr Res., 2021. [DOI | PubMed]
- Trends in prevalence of cannabis use disorder among U.S. veterans with and without psychiatric disorders between 2005 and 2019.. Am J Psychiatry., 2024. [DOI | PubMed]
- Using electronic health records for population health research: a review of methods and applications.. Annu Rev Public Health., 2016. [DOI | PubMed]
- The epidemiology of substance use disorders in US Veterans: a systematic review and analysis of assessment methods.. Am J Addict., 2016. [DOI | PubMed]
- Comparison of medical cannabis use reported on a confidential survey vs documented in the electronic health record among primary care patients.. JAMA Netw Open., 2022. [DOI | PubMed]
- US veterans who do and do not utilize Veterans Affairs health care services: demographic, military, medical, and psychosocial characteristics.. Prim Care Companion CNS Disord., 2019. [DOI | PubMed]
- What is the prevalence and risk of cannabis use disorders among people who use cannabis? a systematic review and meta-analysis.. Addict Behav., 2020. [DOI | PubMed]
- A search algorithm for identifying likely users and non-users of marijuana from the free text of the electronic medical record.. PLoS One., 2018. [DOI | PubMed]
- Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support.. J Biomed Inform., 2009. [DOI | PubMed]
- DSM-5 criteria for substance use disorders: recommendations and rationale.. Am J Psychiatry., 2013. [DOI | PubMed]
- Validation of the AUDIT and AUDIT-C for hazardous drinking in community-dwelling older adults.. Int J Environ Res Public Health., 2021. [DOI | PubMed]
- A short scale for measuring loneliness in large surveys: results from two population-based studies.. Res Aging., 2004. [DOI | PubMed]
- PTSD-8: a short PTSD inventory.. Clin Pract Epidemiol Ment Health., 2010. [DOI | PubMed]
- Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population.. Med Care., 2008. [DOI | PubMed]
- The PHQ-8 as a measure of current depression in the general population.. J Affect Disord., 2009. [DOI | PubMed]
- Predicting risk of hospitalization or death among patients receiving primary care in the Veterans Health Administration.. Med Care., 2013. [DOI | PubMed]
- Insights from advanced analytics at the Veterans Health Administration.. Health Aff (Millwood)., 2014. [DOI | PubMed]
- 65Wallace M, Shelkey M. Katz Index of Independence in Activities of Daily Living (ADL). The Hartford Institute for Geriatric Nursing; 2007. Accessed May 22, 2024. https://www.alz.org/careplanning/downloads/katz-adl.pdf
- Tobacco product use among adults—United States, 2021.. MMWR Morb Mortal Wkly Rep., 2023. [DOI | PubMed]
- Young adult cannabis use disorder treatment admissions declined as past month cannabis use increased in the U.S.: an analysis of states by year, 2008-2017.. Addict Behav., 2021. [DOI | PubMed]
- Tobacco, alcohol, cannabis, and other drug use in the US before and during the early phase of the COVID-19 pandemic.. JAMA Netw Open., 2023. [DOI | PubMed]
- Association of cannabis potency with mental ill health and addiction: a systematic review.. Lancet Psychiatry., 2022. [DOI | PubMed]
- Higher average potency across the United States is associated with progression to first cannabis use disorder symptom.. Drug Alcohol Depend., 2019. [DOI | PubMed]
- Acute effects of smoked and vaporized cannabis in healthy adults who infrequently use cannabis: a crossover trial.. JAMA Netw Open., 2018. [DOI | PubMed]
- Cannabis vaporisation: understanding products, devices and risks.. Drug Alcohol Rev., 2024. [DOI | PubMed]
- Associations between cannabis consumption methods and cannabis risk perception.. Int J Environ Res Public Health., 2024. [DOI | PubMed]
- Prevalence of marijuana use disorders in the United States between 2001-2002 and 2012-2013.. JAMA Psychiatry., 2015. [DOI | PubMed]
- Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: basic findings from the National Comorbidity Survey.. Exp Clin Psychopharmacol., 1994. [DOI]
- Sociodemographic characteristics associated with and prevalence and frequency of cannabis use among adults in the US.. JAMA Netw Open., 2021. [DOI | PubMed]
- Cannabis use among U.S. military veterans following residential substance use disorder treatment.. Mil Med., 2023. [DOI | PubMed]
- Bringing the war back home: mental health disorders among 103,788 US veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs facilities.. Arch Intern Med., 2007. [DOI | PubMed]
- Comparing mental and physical health of U.S. veterans by VA healthcare use: implications for generalizability of research in the VA electronic health records.. BMC Health Serv Res., 2022. [DOI | PubMed]
- Substance use disorders among veterans in a nationally representative sample: prevalence and associated functioning and treatment utilization.. J Stud Alcohol Drugs., 2018. [DOI | PubMed]
- Mental and physical health conditions in US combat veterans: results from the National Health and Resilience in Veterans Study.. Prim Care Companion CNS Disord., 2017. [DOI | PubMed]
- 82VA/DoD clinical practice guideline for the management of posttraumatic stress disorder and acute stress disorder 2023. Accessed March 26, 2025. https://www.healthquality.va.gov/guidelines/mh/ptsd/
- Changes in cannabis potency over the last 2 decades (1995-2014): analysis of current data in the United States.. Biol Psychiatry., 2016. [DOI | PubMed]
- The effects of medical marijuana laws on potency.. Int J Drug Policy., 2014. [DOI | PubMed]
- A comprehensive review of cannabis potency in the United States in the last decade.. Biol Psychiatry Cogn Neurosci Neuroimaging., 2021. [DOI | PubMed]
- Depression in older adults.. Annu Rev Clin Psychol., 2009. [DOI | PubMed]
- 87US Preventive Services Task Force. Unhealthy drug use: screening. Accessed October, 21, 2024. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/drug-use-illicit-screening
- Screening for drug use in primary care: practical implications of the new USPSTF recommendation.. JAMA Intern Med., 2020. [DOI | PubMed]
- Integration of screening, assessment, and treatment for cannabis and other drug use disorders in primary care: an evaluation in three pilot sites.. Drug Alcohol Depend., 2019. [DOI | PubMed]
- Association between cannabis use disorder symptom severity and probability of clinically-documented diagnosis and treatment in a primary care sample.. Drug Alcohol Depend., 2023. [DOI | PubMed]
- Cannabis use reported by patients receiving primary care in a large health system.. JAMA Netw Open., 2024. [DOI | PubMed]
- A comprehensive review of the psychometric properties of the Drug Abuse Screening Test.. J Subst Abuse Treat., 2007. [DOI | PubMed]
- Validity of the Single-Item Screen-Cannabis (SIS-C) for cannabis use disorder screening in routine care.. JAMA Netw Open., 2022. [DOI | PubMed]
- Motivational interviewing for cannabis use disorders: a systematic review and meta-analysis.. Eur Addict Res., 2021. [DOI | PubMed]
- Contingency management for treatment of cannabis use disorder in co-occurring mental health disorders: a systematic review.. Brain Sci., 2022. [DOI | PubMed]
- Cannabis use and cannabis use disorder.. Nat Rev Dis Primers., 2021. [DOI | PubMed]
- Medical cannabis for older patients-treatment protocol and initial results.. J Clin Med., 2019. [DOI | PubMed]
- Trends in emergency department visits associated with cannabis use among older adults in California, 2005-2019.. J Am Geriatr Soc., 2023. [DOI | PubMed]
- Cannabinoids, cannabis, and cannabis-based medicine for pain management: a systematic review of randomised controlled trials.. Pain., 2021. [DOI | PubMed]
- Systematic review of systematic reviews for medical cannabinoids: pain, nausea and vomiting, spasticity, and harms.. Can Fam Physician., 2018. [PubMed]
- Efficacy and adverse event profile of cannabidiol and medicinal cannabis for treatment-resistant epilepsy: systematic review and meta-analysis.. Epilepsy Behav., 2020. [DOI | PubMed]
- Persistent cannabis users show neuropsychological decline from childhood to midlife.. Proc Natl Acad Sci U S A., 2012. [DOI | PubMed]
- Marijuana use, diet, body mass index, and cardiovascular risk factors (from the CARDIA study).. Am J Cardiol., 2006. [DOI | PubMed]
- Asking sensitive questions: the impact of data collection mode, question format, and question context.. Public Opin Q., 1996. [DOI]
- Disclosure of sensitive behaviors across self-administered survey modes: a meta-analysis.. Behav Res Methods., 2015. [DOI | PubMed]