Demographic Profiles, Etiological Spectrum, and Anatomical Locations of the Post-Hepatic Obstructive Jaundice in Adult Population in Hadhramout Region in Yemen
Abstract
Background: Obstructive jaundice is a common health challenge in daily clinical practice caused by a heterogeneous group of benign and malignant conditions in or around extrahepatic bile ducts. This study aimed to investigate the causes of obstructive jaundice, analyze the age and sex distribution, and report the locations of obstruction. Methods: This was a retrospective study of electronic records of patients diagnosed with obstructive jaundice in the Hadhramout region in Yemen. Results: This study analyzed the data of 303 patients (mean age: 57 ± 17.99 years; range: 18–95 years); 60.40% (n = 183) were female, and 39.60% (n = 120) were male. The highest prevalence was found in middle-aged adults (n = 112, 36.96%), followed by the old (n = 101, 33.33%). Common bile duct (CBD) stones were the most common cause of obstructive jaundice (n = 175, 57.8%), followed by CBD stricture (n = 58, 19.1%), carcinoma of the head of the pancreas (n = 35, 11.6%), cholangiocarcinoma (n = 21, 6.9%), and external compression of the CBD (n = 2, 0.7%). CBD stones, cholangiocarcinoma, and ampulla of Vater masses were more prevalent in females (30.9%, 3.8%, and 2.2%, respectively) than in males (25.8%, 2.9%, and 1.7%, respectively). In contrast, CBD stricture and carcinoma of the pancreas were more frequent in males, occurring in 12.1% and 7.1% of male patients, respectively, compared to 7.9% and 4.9% in female patients. The primary obstruction site was the CBD (n = 254, 83.8%), followed by the head of the pancreas (n = 30, 9.9%), and the ampulla of Vater (n = 13, 4.3%). Conclusions: Obstructive jaundice predominantly affects middle-aged adults followed by the old-aged patients predominantly in females. The most common cause of obstructive jaundice was CBD stones, followed by CBD stricture, while carcinoma of the head of the pancreas was the most common malignant cause, followed by cholangiocarcinoma. Distal CBD is the most common anatomical location of obstructive jaundice.
Article type: Research Article
Keywords: obstructive jaundice, common bile duct (CBD), choledocholithiasis, CBD stricture, carcinoma of the pancreas, cholangiocarcinoma, Mirizzi syndrome
Affiliations: Department of Diagnostic Radiology, College of Applied Medical Sciences, Taibah University, Al-Madinah Al-Munawwarah 41477, Saudi Arabia; Department of Specialized Surgery, Radiology Section, Faculty of Medicine, Hadhramout University, Hadhramaut, Yemen; Department of Internal Medicine, Dr. Suliman Al Habib Hospital Altakhasosi, Riyadh 12344, Saudi Arabia; Radiology Department, Rush University Medical Center, Chicago, IL 60612, USA
License: © 2024 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.3390/diseases12120333 | PubMed: 39727663 | PMC: PMC11727093
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (1.4 MB)
1. Introduction:
Jaundice (hyperbilirubinemia) is a yellow discoloration of body tissues resulting from excessive accumulation of bilirubin due to increased production or impaired excretion [ref. 1]. The etiology of jaundice can be broadly divided into pre-hepatic, hepatic, and post-hepatic categories [ref. 2]. The pathogenesis of post-hepatic jaundice involves obstruction of the biliary drainage (obstructive jaundice) which blocks the passage of bile through the extrahepatic bile ducts outside the liver before entry into the duodenum via the ampulla of Vater [ref. 3,ref. 4]. Obstructive jaundice is caused by a heterogeneous group of benign and malignant conditions, which vary among individuals. The morbidity and mortality associated with obstructive jaundice depend on the cause of obstruction. These causes include choledocholithiasis, common bile duct (CBD) stricture, cholangiocarcinoma, carcinoma of the pancreas or gallbladder, periampullary carcinoma, and Mirizzi syndrome [ref. 5].
Transabdominal ultrasound imaging (TAUS) is the most commonly used screening modality, offering the advantages of being non-invasive, widely available, and inexpensive [ref. 6]. However, TAUS has limitations owing to its high operator dependence, which requires substantial knowledge and skills. Additionally, hepatobiliary artifacts may reduce the accuracy in CBD lesion diagnosis [ref. 7]. Endoscopic retrograde cholangiopancreatography (ERCP) provides rapid access to the bile ducts, facilitating optimal management of extra-hepatic bile duct stones and tumors [ref. 8]. Currently, ERCP is an established diagnostic and therapeutic method for CBD [ref. 9].
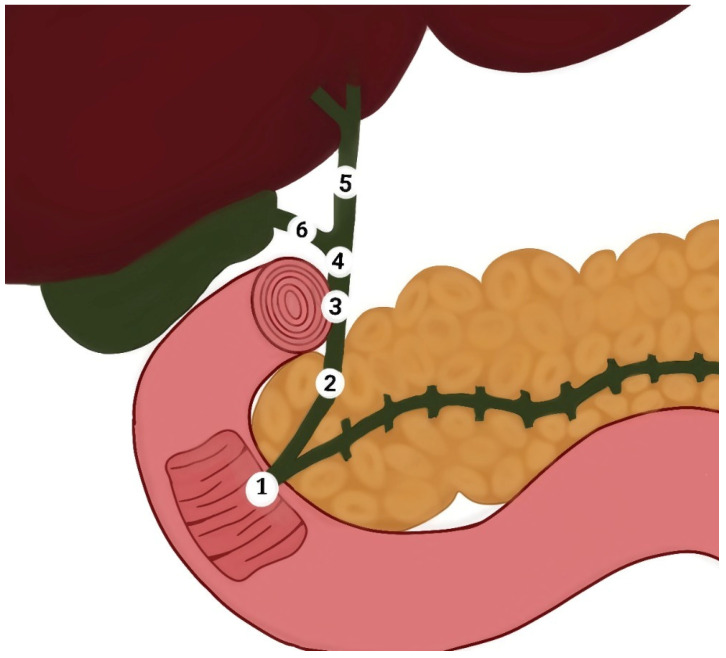
Obstructive jaundice is a common health challenge in daily practice and may lead to severe complications and adverse health outcomes. Management of this condition poses substantial diagnostic and therapeutic challenges for surgeons [ref. 10]. In the literature, there is a notable gap regarding the causes of obstructive jaundice in our region. This study aimed to investigate the most common causes of obstructive jaundice, analyze age and sex distributions, and identify the locations of obstruction in the extrahepatic bile ducts. This study reported common causes of obstructive jaundice in patients, including bile duct stone, bile duct stricture, cholangiocarcinoma, pancreatic carcinoma, mass at the ampulla of Vater, and external compression. We also identified the frequent anatomical locations of these causes in the extrahepatic bile ducts, such as the CBD, ampulla of Vater, head of the pancreas, and external compression. (Figure 1). To the best of our knowledge, this is the first study to explore these aspects of the Hadhramout region of the Republic of Yemen.
2. Materials and Methods
2.1. Study Design
This was a retrospective cross-sectional study of electronic records of patients diagnosed with obstructive jaundice between August 2017 and November 2023. This study was conducted at the Alsafwa Consultative Medical Center (ACMC) in Almukalla City, Hadhramout, Republic of Yemen. This study was approved by the Research Ethics Committee of ACMC in Almukalla City, Hadramout, Republic of Yemen (Approval Number: ACMC-11-23, 1 November 2023). All procedures were performed in accordance with the Declaration of Helsinki and all applicable standards and laws.
2.2. Sample Size
After ethical approval was obtained, this study involved 303 (n = 303) patients with clinically diagnosed obstructive jaundice who underwent TAUS and ERCP to identify the underlying cause.
2.3. Inclusion Criteria
This study included all of the patients clinically diagnosed with obstructive jaundice (n = 303) who underwent TAUS and ERCP to detect the cause of obstructive jaundice.
2.4. Exclusion Criteria
This study excluded the following categories:
- Patients with jaundice caused by pre-hepatic factors.
- Patients with obstructive jaundice caused by hepatic factors.
- Patients in whom the causes of obstructive jaundice were not definitively determined by ERCP (n = 88).
2.5. Data Acquisition
All patients underwent TAUS performed by a highly qualified radiologist with 13 years of postdoctoral experience in general ultrasound imaging. A Mindray DC30 ultrasound Machine with a deep curved transducer of 3.5 MHz was used to assess the CBD and biliary ducts in all patients. Following this, ERCP was conducted on all patients to confirm the diagnoses.
2.5.1. Ultrasound Imaging Procedure
After fasting for at least six hours, patients underwent TAUS scanning. Scanning was performed in the supine position with or without the left lateral decubitus position to scan the biliary tree. After the gel application, the ultrasound probe was wrapped around the right subcostal region. The right upper quadrant region was scanned in the sagittal, coronal, and axial planes.
2.5.2. ERCP Technique
After optimal preparation, written informed consent was obtained. According to the revised guidelines of the American Society of Gastrointestinal Endoscopy (ASGE) were reported by Jacob et al. [ref. 11], each patient involved in this study underwent ERCP for diagnostic and therapeutic purposes. The procedures were performed to ensure the consensus guidelines for perioperative management of patients undergoing ERCP reported by Azimaraghi et al. [ref. 12].
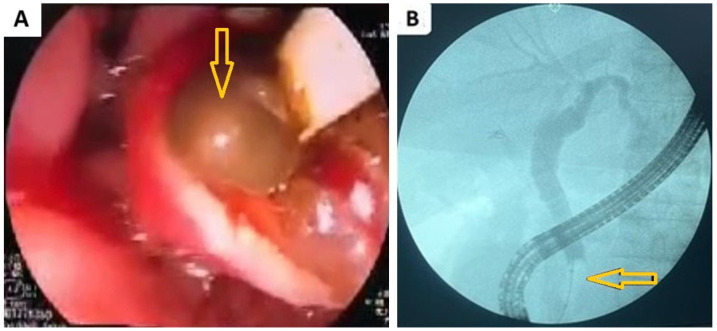
In the current study, the cause of obstructive jaundice was confirmed using ERCP in all patients. In our work, we present images of ERCP showing distal CBD stones obstructing it (Figure 2).
2.6. Statistical Analysis
The collected data were analyzed using the Statistical Package for Social Sciences (SPSS) version 25 (IBM, Armonk, NY, USA), and DATAtab Team (2023), (DATAtab: Online Statistics Calculator (DATAtab e.U. Graz, Austria)). This study reported common causes of obstructive jaundice in patients. Also, we compared demographic characteristics, such as sex and age groups, among the patients. Furthermore, this study analyzed the distribution of causes and locations according to patients’ sex and age groups. Categorical variables are expressed as frequencies and percentages, whereas continuous variables are presented as means with standard deviations. A chi-square test (X2) was used to compare the variables between the groups, with p-values considered significant when less than 0.05.
3. Results
3.1. Demographic Data
This study included 303 patients with an average age of 57 ± 17.99 years (range: 18–95). Of those, 60.40% (n = 183) were female, and 39.60% (n = 120) were male. The most commonly affected age group was the middle-aged adults (n = 112, 36.96%), followed by the old (n = 101, 33.33%) (Table 1). Boxplots show females were affected more than males across different age groups, with a notably smaller number of affected patients in the younger age group (<20 years) (Figure 3).
Table 1: Sociodemographic features of the involved patients.
| Variable | Categories | Number | Percentage |
|---|---|---|---|
| Patient’s gender | Male | 120 | 39.60% |
| Female | 183 | 60.40% | |
| Patient’s age groups | Young (<20 years) | 4 | 1.32% |
| Young adults (21–40 years) | 61 | 20.13% | |
| Middle-aged adults (41–60 years) | 112 | 36.96% | |
| Old (61–80 years) | 101 | 33.33% | |
| Very old (>80 years) | 25 | 8.25% |
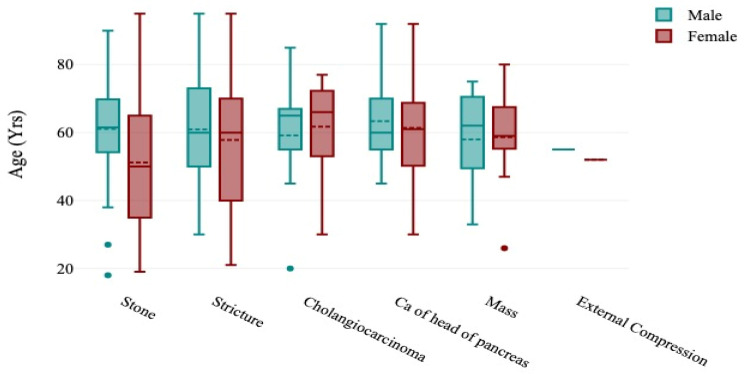
The boxplots show that females had a wider range of age than males in different causes of obstructed jaundice, except in masses where males had a wider age range and in external compression where there was no significant difference (Figure 3).
3.2. Etiological Data
The study findings indicated that CBD stones were the most common cause of obstructive jaundice (n = 175, 57.8%), followed by CBD stricture (n = 58, 19.1%), carcinoma of the pancreatic head (n = 35, 11.6%), cholangiocarcinoma (n = 21, 6.9%), and external compression of the CBD (n = 2, 0.7%) (Table 2).
Table 2: The common causes of post-hepatic obstructive jaundice.
| Causes of Obstructive Jaundice | Number | Percentage |
|---|---|---|
| Common bile duct stone | 175 | 57.8% |
| Common bile duct stricture | 58 | 19.1% |
| Cholangiocarcinoma | 21 | 6.9% |
| Carcinoma of the pancreas | 35 | 11.6% |
| Mass at the ampulla of Vater | 12 | 4.0% |
| External compression | 2 | 0.7% |
| Total | 303 | 100% |
The results indicated that CBD stones were the cause in 30.9% of females and 25.8% of males, cholangiocarcinoma was the cause in 3.8% of females and 2.9% of males, and masses in the ampulla of Vater were the cause in 2.2% of females and 1.7% of males. In contrast, CBD strictures were the cause in 12.1% of males compared to 7.9% of females, and pancreatic carcinoma was the cause in 7.1% of males against 4.9% of females (Figure 4). However, this study revealed no significant difference in the overall nature of the causes of obstructive jaundice between males and females (p = 0.336) (Table 3).
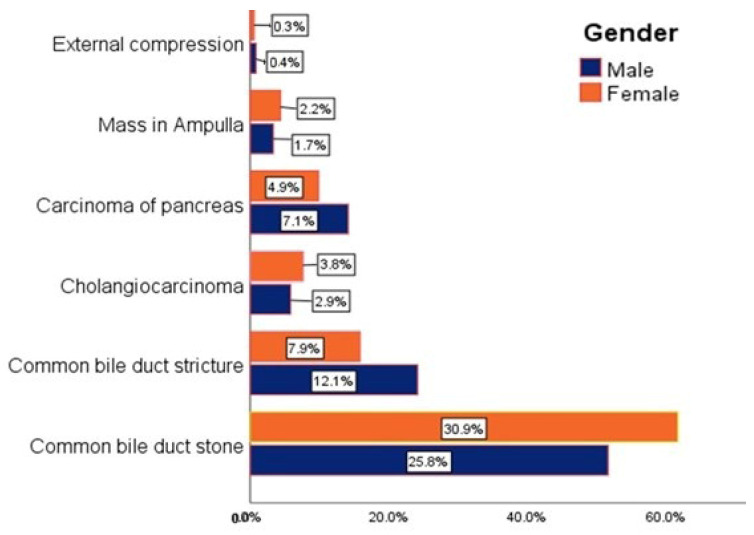
Table 3: The common causes of obstructive jaundice in males and females.
| Causes of Obstructive Jaundice | Male | Female | Total | p-Value |
|---|---|---|---|---|
| Common bile duct stone | 62 | 113 | 175 (57.8%) | 0.336 |
| Common bile duct stricture | 29 | 29 | 58 (19.1%) | |
| Cholangiocarcinoma | 7 | 14 | 21 (6.9%) | |
| Carcinoma of the pancreas | 17 | 18 | 35 (11.6%) | |
| Mass at the ampulla of Vater | 4 | 8 | 12 (4.0%) | |
| Compression | 1 | 1 | 2 (0.7%) | |
| Total | 120 | 183 | 303 (100%) |
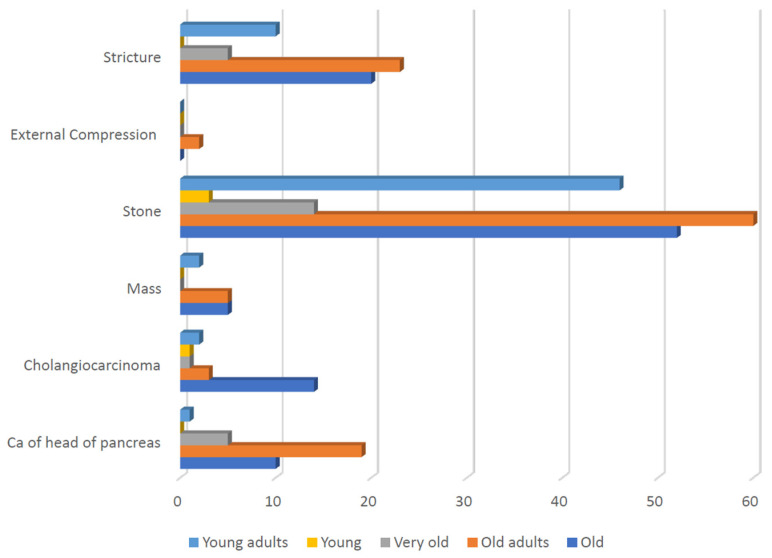
The current study demonstrated significant variation in the nature of the causes of obstructive jaundice across different age groups. CBD stones were most prevalent in middle-aged adults (n = 60, 34.29%), followed by the old (n = 52, 29.71%), and young adults (n = 46, 26.28%). Cholangiocarcinoma was more prevalent in old patients (n = 14, 66.66%); however, it was less common in the other age groups. Carcinoma of the head of the pancreas was predominantly observed in middle-aged adults (n = 19, 54.28%), followed by the old (n = 10, 28.57%); however, it was less common in the other age groups (X2 = 34.21, p = 0.025) (Table 4, Figure 5).
Table 4: The common causes of obstructive jaundice in different age groups.
| Causes of Obstructive Jaundice | Young | Young Adults | Middle-Aged Adults | Old | Very Old | Total | p-Value |
|---|---|---|---|---|---|---|---|
| Common bile duct stone | 3 | 46 | 60 | 52 | 14 | 175 (57.8%) | 0.025 |
| Common bile duct stricture | 0 | 10 | 23 | 20 | 5 | 58 (19.1%) | |
| Cholangiocarcinoma | 1 | 2 | 3 | 14 | 1 | 21 (6.9%) | |
| Carcinoma of the pancreas | 0 | 1 | 19 | 10 | 5 | 35 (11.6%) | |
| Mass at the ampulla of Vater | 0 | 2 | 5 | 5 | 0 | 12 (4.0%) | |
| External compression | 0 | 0 | 2 | 0 | 0 | 2 (0.7%) | |
| Total | 4 | 61 | 112 | 101 | 25 | 303 (100%) |
3.3. Anatomical Locations Data
Our results showed that the CBD was the most common location of obstructive jaundice caused by the CBD (n = 254, 83.8%), followed by the head of the pancreas (n = 30, 9.9%), the ampulla of Vater (n = 13, 4.3%), and external compression of the CBD (n = 6, 2.0%) (Table 5). Additionally, when comparing the different parts of the CBD, our results found that the distal CBD was the most common site of obstructive jaundice (n = 126, 41.6%), followed by the proximal part (n = 23, 7.6%), and the middle part (n = 4, 1.3%) (Table 6).
Table 5: The common locations of obstruction in the extrahepatic bile ducts.
| Locations of Cause of Obstructive Jaundice | Number | Percentage |
|---|---|---|
| Common bile duct (CBD) | 254 | 83.8% |
| Head of pancreas | 30 | 9.9% |
| Ampulla of Vater | 13 | 4.3% |
| Liver mass causing compression | 6 | 2.0% |
| Total | 303 | 100% |
Table 6: The common locations of obstruction in the CBD and extrahepatic bile ducts.
| Locations of Cause of Obstructive Jaundice | Number | Percentage |
|---|---|---|
| CBD stone (No determined part) | 101 | 33.3% |
| CBD stone in the distal part | 126 | 41.6% |
| CBD stone in the middle part | 4 | 1.3% |
| CBD stone in the proximal part | 23 | 7.6% |
| Head of pancreas | 30 | 9.9% |
| Ampulla of Vater | 13 | 4.3% |
| Liver mass causing compression | 6 | 2.0% |
| Total | 303 | 100% |
CBD: common bile duct.
4. Discussion
An accurate diagnosis of the cause of post-hepatic obstructive jaundice is the cornerstone for optimal management planning at different ages. A higher prevalence was obtained in females (60.40%) compared to males (39.60%). This finding aligns with the results of several studies: Chalya et al. reported 1.3:1 female-to-male ratio [ref. 13], Bhutia et al. found a 1:0.35 female-to-male ratio [ref. 5], Gameraddin et al. reported 65.33% females to 34.66% males [ref. 14], and Shukla et al. noted a 2:3 male-to-female ratio [ref. 15]. The predominance of females in these cases has been attributed to a higher incidence of gallbladder stones in women, which is a known risk factor for choledocholithiasis and benign biliary obstruction [ref. 13,ref. 16]
Our results showed that the mean age of the patients affected by obstructive jaundice was 57 ± 17.99 years, consistent with the findings of Khan ZA, who reported a mean age of 56.68 ± 23.34 years [ref. 17]. The most commonly affected age groups were middle-aged adults (36.96%) and the old (33.33%), which partially aligns with Hasan’s study, indicating that half of the patients undergoing ERCP for obstructive jaundice were aged 41–60 [ref. 18]. Notably, the clinical presentation of choledocholithiasis may vary with age [ref. 19]. The current study included only patients presenting with obstructive jaundice, which might explain the age groups involved compared to other studies.
It is important to note that the causes of post-hepatic obstructive jaundice include a range of benign and malignant lesions. CBD stones are the most common benign cause of CBD obstruction [ref. 5]. These findings confirm our findings, in which CBD stones were identified as the most prevalent cause of obstructive jaundice (57.8%). In our study, CBD strictures accounted for 19.1% of cases, although their nature (i.e., benign or malignant) was not determined. Aljahdli reported that while the majority of CBD strictures are considered malignant, up to 30% can be benign, presenting a diagnostic and management challenge [ref. 20]. CBD strictures can arise from various etiologies including iatrogenic postcholecystectomy or liver transplantation; primary sclerosing cholangitis; chronic pancreatitis; autoimmune pancreatitis, autoimmune cholangitis, Mirizzi syndrome, tuberculous, viral, or parasitic infections; HIV cholangiopathy; ischemia; vasculitis; trauma; and post-radiation therapy. On the malignant side, strictures may result from pancreatic carcinoma, cholangiocarcinoma, or metastatic disease with external compression by lymph nodes [ref. 21].
Obstructive jaundice is a common clinical manifestation of pancreatic head and neck cancer [ref. 22]. Clinically, 90% of pancreatic neoplasms are malignant ductal adenocarcinomas. Bornman noted that two thirds of pancreatic carcinoma develop in the head of the pancreas, with many patients presenting with progressive obstructive jaundice [ref. 23]. In line with these observations, in the current study, we found that carcinoma of the head of the pancreas was the most common malignant cause of obstructive jaundice and the third most common cause of obstructive jaundice, accounting for 11.6% of all cases.
Cholangiocarcinoma encompasses a group of malignancies originating from different locations in the bile ducts, including the intrahepatic, hilar/perihilar (Klatskin tumor), and distal CBD [ref. 24]. Its peak incidence is observed during the sixth to the seventh decade of life, with a slight male predominance [ref. 25]. Contrary to these trends, cholangiocarcinoma emerged as the fourth most common cause of obstructive jaundice in our study and was more frequently observed in females. This deviation may be attributed to our specific focus on cholangiocarcinoma as a sole cause of obstructive jaundice.
The epidemiology, pathogenesis, and classification of biliary stones differ according to the stone location in intrahepatic and/or extrahepatic bile ducts. The primary bile duct stones are mostly brown-pigment (calcium bilirubin) stones and more common in East Asian countries than in Western countries. Gallbladder stones are primarily cholesterol or black pigment stones and common in western countries and Japan [ref. 26]. In our study, CBD stones were the cause of obstructive jaundice in 57.8% of the study population, followed by CBD stricture (19.1%), carcinoma of the pancreatic head (11.6%), cholangiocarcinoma (6.9%), and external compression of the CBD (0.7%). These results reflected significant variation from the results of a similar study in the Sikkim state of India where CBD stones were the cause of obstructive jaundice in 84.93% of all patients, followed by gallbladder carcinoma (6.85%), followed by CBD stricture (2.74%), and pancreatic carcinoma (1.37%), cholangiocarcinoma (1.37%), periampullary carcinoma (1.37%), and Mirizzi syndrome (1.37%) [ref. 5].
Finally, Mirizzi syndrome, a rare condition in which obstructive jaundice is caused by external compression of the CBD or common hepatic duct due to gallstones impacted in Hartman’s pouch, is a notable cause [ref. 27]. Other mechanical causes of external compression of the bile ducts include non-Hodgkin lymphoma [ref. 28], hepatic artery aneurysm [ref. 29], pancreaticoduodenal artery aneurysm [ref. 30], portal vein thrombosis [ref. 31], and diaphragmatic hernia [ref. 32]. Interestingly, a recent case report suggested that cocaine is a potential cause of biliary tree obstruction [ref. 33]. In our study, we found two cases of obstructive jaundice due to external compression of the CBD, one caused by an enlarged hilar lymph node, and the other caused by a liver mass. This highlights that, while some causes are well-established, others may emerge in future research.
5. Limitations
This study is limited by the inability to precisely determine the locations of obstructive jaundice causes in different parts of the CBD in 101 (33.3%) patients. This lack of specific location data was a drawback, particularly when comparing the locations of CBD stones between those within the CBD. Despite this, we found that the distal CBD was the most common location for CBD stones.
6. Conclusions
Post-hepatic obstructive jaundice predominantly affects old adults followed by old-aged patients, with a higher incidence in females. The most common cause of obstructive jaundice was CBD stones followed by CBD stricture, which can be benign or malignant. Among the malignant causes, carcinoma of the head of the pancreas was the most common, followed by cholangiocarcinoma. The most common location for obstructive jaundice was identified as the CBD, particularly its distal part.
References
- A. Joseph, H. Samant. Jaundice. StatPearls, 2023
- Y.Y. Chee, P.H. Chung, R.M. Wong, K.K. Wong. Jaundice in infants and children: Causes, diagnosis, and management. Hong Kong Med. J., 2018. [DOI | PubMed]
- A. Pavlovic Markovic, M. Stojkovic Lalosevic, D.D. Mijac, T. Milovanovic, S. Dragasevic, A. Sokic Milutinovic, M.N. Krstic. Jaundice as a Diagnostic and Therapeutic Problem: A General Practitioner’s Approach. Dig. Dis., 2022. [DOI | PubMed]
- R. Shah, S. John. Cholestatic Jaundice. StatPearls, 2023
- K.D. Bhutia, T. Lachungpa, S.C. Lamtha. Etiology of obstructive jaundice and its correlation with the ethnic population of Sikkim. J. Family Med. Prim. Care, 2021. [DOI | PubMed]
- M.L. Freitas, R.L. Bell, A.J. Duffy. Choledocholithiasis: Evolving standards for diagnosis and management. World J. Gastroenterol., 2006. [DOI | PubMed]
- H.I. Alsaedi, A.M. Krsoom, S.A. Alshoabi, W.M. Alsharif. Investigation Study of Ultrasound Practitioners’ Awareness about Artefacts of Hepatobiliary Imaging in Almadinah Almunawwarah. Pak. J. Med. Sci., 2022. [DOI | PubMed]
- E. van Sonnenberg, R. Panchanathan. Percutaneous Transcholecystic Management of Choledocholithiasis: A Next Horizon for Interventional Radiologists?. Radiology, 2019. [DOI | PubMed]
- W.G. Zhang, N.L. Chai, B. Zhang, X. Li, J.F. Wang, H. Dong, Y.J. Feng, E.Q. Linghu. Cholangioscopy-assisted extraction through novel papillary support for small-calibre and sediment-like common bile duct stones. World J. Gastroenterol., 2023. [DOI | PubMed]
- J.J. Liu, Y.M. Sun, Y. Xu, H.W. Mei, W. Guo, Z.L. Li. Pathophysiological consequences and treatment strategy of obstructive jaundice. World J. Gastrointest. Surg., 2023. [DOI | PubMed]
- J.S. Jacob, M.E. Lee, E.Y. Chew, A.P. Thrift, R.J. Sealock. Evaluating the Revised American Society for Gastrointestinal Endoscopy Guidelines for Common Bile Duct Stone Diagnosis. Clin. Endosc., 2021. [DOI | PubMed]
- O. Azimaraghi, M. Bilal, S. Amornyotin, M. Arain, M. Behrends, T.M. Berzin, J.L. Buxbaum, C. Choice, P. Fassbender, M.S. Sawhney. Consensus guidelines for the perioperative management of patients undergoing endoscopic retrograde cholangiopancreatography. Br. J. Anaesth., 2023. [DOI | PubMed]
- P.L. Chalya, E.S. Kanumba, M. McHembe. Etiological spectrum and treatment outcome of Obstructive jaundice at a University teaching Hospital in northwestern Tanzania: A diagnostic and therapeutic challenges. BMC Res. Notes, 2011. [DOI | PubMed]
- M. Gameraddin, S. Omer, S. Salih, S. Elsayed, A. Alshaikh. Sonographic Evaluation of Obstructive Jaundice. Open J. Med. Imaging, 2015. [DOI]
- S. Shukla, P.R. Kharat, N. Patbamniya, K. Kumar. Clinicopathological study on patients presenting with obstructive jaundice. Int. Surg. J., 2018. [DOI]
- E.M. Coucke, H. Akbar, A. Kahloon, P.P. Lopez. Biliary Obstruction. StatPearls [Internet], 2022
- Z.A. Khan. Clinical profile of patients with obstructive jaundice: A surgeon’s perspectives. Int. Surg. J., 2019. [DOI]
- M.S. Hasan. Factors Affecting Morbidity and Mortality after ERCP for Obstructive Jaundice. Mymensingh Med. J., 2021. [PubMed]
- K.C. Hu, C.H. Chu, H.Y. Wang, W.H. Chang, S.C. Lin, C.C. Liu, W.C. Liao, C.J. Liu, M.S. Wu, S.C. Shih. How Does Aging Affect Presentation and Management of Biliary Stones?. J. Am. Geriatr. Soc., 2016. [DOI | PubMed]
- E.S. Aljahdli. Management of distal malignant biliary obstruction. Saudi J. Gastroenterol., 2018. [DOI | PubMed]
- A. Singh, A. Gelrud, B. Agarwal. Biliary strictures: Diagnostic considerations and approach. Gastroenterol. Rep., 2015. [DOI]
- Z. Shen, L. Tian, X. Wang. Treatment of pancreatic head cancer with obstructive jaundice by endoscopy ultrasonography-guided gastrojejunostomy: A case report and literature review. Medicine, 2018. [DOI | PubMed]
- P.C. Bornman, I.J. Beckingham. ABC of diseases of liver, pancreas, and biliary system. Pancreatic tumours. BMJ, 2001. [DOI | PubMed]
- M. Ledenko, S.O. Antwi, S. Arima, J. Driscoll, J. Furuse, H.J. Klümpen, F.O. Larsen, D.K. Lau, A. Maderer, A. Markussen. Sex-related disparities in outcomes of cholangiocarcinoma patients in treatment trials. Front. Oncol., 2022. [DOI | PubMed]
- N. Guedj. Pathology of Cholangiocarcinomas. Curr. Oncol., 2022. [DOI | PubMed]
- S. Tazuma. Gallstone disease: Epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best. Pract. Res. Clin. Gastroenterol., 2006. [DOI | PubMed]
- S. Jesani, A.L. Romero, S.B. Bozkurt, A.A. Abu Samak, J. Romero, J. Sookdeo, A. Naik. Mirizzi Syndrome: An Unusual Complication of Cholelithiasis. J. Community Hosp. Intern. Med. Perspect., 2022. [DOI | PubMed]
- L. Yuan, X. Shi, H. Shan, D. Xiao, X. Wang, F. Wang. Treatment of obstructive jaundice induced by non-hodgkin lymphoma with EUS-guided transgastric anterograde common bile duct stenting: Technical case report and literature review. Front. Surg., 2023. [DOI | PubMed]
- A. Julianov, Y. Georgiev. Hepatic artery aneurysm causing obstructive jaundice. Quant. Imaging Med. Surg., 2014. [DOI | PubMed]
- T. Yin, Z. Wan, H. Chen, X. Mao, Y. Yi, D. Li. Obstructive jaundice caused by pancreaticoduodenal artery aneurysms associated with celiac axis stenosis: Case report and review of the literature. Ann. Vasc. Surg., 2015. [DOI]
- A. Gebreselassie, M. Bukhari, M. Khashab. Recurrent Biliary Obstruction Secondary to Portal Vein Thrombosis with Cavernous Transformation and the Role of Cholangioscopy in Diagnosis: Case Report: 1301. Am. J. Gastroenterol., 2017. [DOI]
- H. Hoang, T. Norris. A Twisted Case of Jaundice. Cureus, 2020. [DOI | PubMed]
- K. Alexandre, O. Hassan, J. Hebden, J.M. Barnwell. Cocaine Induced Biliary Tree Obstruction in a Middle-Aged Male. Cureus, 2021. [DOI | PubMed]