The use of antibiotics during pregnancy: A cross‐sectional study of knowledge, attitude, and practices among antenatal care attendees in Northern Ghana
Abstract
Background and aims:
The promotion of rational use of antibiotics among pregnant women is eminent not only for the risk of teratogenicity in the developing fetus but also the risk of drug resistance with its concomitant high cost of health care. Studies on antibiotic self‐medication among pregnant women in Northern Ghana are rare. Improving the knowledge and awareness among the vulnerable groups about the appropriate use of antibiotics can help in limiting the antibiotic resistance menace. We, therefore, conducted this study to assess the knowledge, attitude, and practice (KAP) toward antibiotic use among pregnant women attending an antenatal clinic at a primary health care in Tolon, Northern Region, Ghana.
Method:
We conducted a cross‐sectional study using an interviewer‐administered questionnaire to assess the KAP of 702 pregnant women on antibiotic use. This study was conducted in the Tolon Health Center (THC) from March 2021 and ended in October 2021.
Results:
In this study, 55.6% of pregnant women had good knowledge and 45.3% of them had engaged in self‐medication with antibiotics while pregnant. There were statistically significant associations between participants’ background and obstetric characteristics and knowledge of antibiotic use and antibiotic resistance, except for age, marital status, and parity. Also, there was a significant association between pregnant women’s knowledge and self‐medication or over‐the‐counter purchase of antibiotics.
Conclusion:
We concluded that higher education level, monthly income, good practice, and good knowledge were significantly associated with a reduced likelihood of self‐medication with antibiotics. A well‐structured education that could be easily accepted and understood by pregnant women on the risks of antibiotic self‐medication should be included in the routine education at the antenatal clinics.
Article type: Research Article
Keywords: antibiotics, Ghana, knowledge, pregnancy, self‐medication
Affiliations: Department of Clinical Microbiology University for Development Studies Tamale Ghana; Department of Midwifery and Women’s Health, School of Nursing and Midwifery University for Development Studies Tamale Ghana; Department of Human Anatomy University for Development Studies Tamale Ghana; Department of General Nursing, School of Nursing and Midwifery University for Development Studies Tamale Ghana; Department of Pediatrics and Child Health Tamale Teaching Hospital Tamale Ghana
License: © 2024 The Authors. Health Science Reports published by Wiley Periodicals LLC. CC BY 4.0 This is an open access article under the terms of the http://creativecommons.org/licenses/by/4.0/ License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Article links: DOI: 10.1002/hsr2.2111 | PubMed: 38779221 | PMC: PMC11109041
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (1.2 MB)
INTRODUCTION
Antibiotic resistance has become a worldwide health challenge associated with the rise in antibiotic prescription and consumption worldwide.ref. hsr22111-bib-0001 This challenge has a serious consequence on humans, as diseases that were easily treatable will be difficult to treat.ref. hsr22111-bib-0002 Among many, self‐medication is a major contributor to the development of human pathogen resistance to antibiotic drugs.ref. hsr22111-bib-0002, ref. hsr22111-bib-0003 Pregnant women are one of the vulnerable population groups who practice self‐medication frequently and repeatedly for the prevention of abortion and treatment of pregnancy‐related morbidities.ref. hsr22111-bib-0004 During pregnancy, many physiological and hormonal changes occur, which make these women susceptible to infection,ref. hsr22111-bib-0005 which if not managed timely and well, may lead to some complications that may be fatal to the mother or fetus.ref. hsr22111-bib-0006, ref. hsr22111-bib-0007 To bring quick relief from these pregnancy‐related symptoms, pregnant women may resort to using medicines. Because of inefficient health care system and easy access to medicine from several channels, many pregnant women in developing countries easily practice self‐medication.ref. hsr22111-bib-0008, ref. hsr22111-bib-0009, ref. hsr22111-bib-0010
Self‐medication during pregnancy presents a serious maternal and fetal health threat that cannot be overemphasized.ref. hsr22111-bib-0011, ref. hsr22111-bib-0012 It may lead to fetal toxicity, low birth weight, preterm delivery, and also other teratogenic effects.ref. hsr22111-bib-0010, ref. hsr22111-bib-0013 Sub‐Saharan Africa accounted for ~66% of the estimated global maternal deaths in 2017.ref. hsr22111-bib-0014 Many studies have indicated high rates of self‐medication during pregnancy,ref. hsr22111-bib-0004, ref. hsr22111-bib-0009, ref. hsr22111-bib-0015, ref. hsr22111-bib-0016, ref. hsr22111-bib-0017, ref. hsr22111-bib-0018, ref. hsr22111-bib-0019 with self‐medication with antibiotics among pregnant women reported as 1.9% in Tanzaniaref. hsr22111-bib-0016 and 9.6% in Nigeria.ref. hsr22111-bib-0019 However, a study in Ghana reported that the prevalence of antibiotic exposure among pregnant women increased from 54.8% in 2013 to 77.8% in 2015.ref. hsr22111-bib-0012 Antibiotic exposures during pregnancy have been associated with both short‐term (e.g., congenital abnormalities) and long‐term effects (e.g., changes in the gut microbiome, asthma, atopic dermatitis) in the newborn. However, it is estimated that only 10% of medications have sufficient data related to safe and effective use by pregnant women.ref. hsr22111-bib-0020 Widespread irrational use of antibiotics and ignorance of people about the need to complete the course of antibiotics, their side effects, standard acceptable dosage limits, and antibiotic overdose issues can lead to microbial resistance issues.ref. hsr22111-bib-0002
The promotion of rational antibiotic use is imminent due to the risk of drug resistance with its concomitant high cost of health care and also the risk of teratogenicity in the developing fetus.ref. hsr22111-bib-0012 Even though there are many potential dangers associated with antibiotic self‐medication during pregnancy,ref. hsr22111-bib-0021, ref. hsr22111-bib-0022 many pregnant women are oblivious of them.ref. hsr22111-bib-0017 Improving the knowledge and awareness among the nonmedical population about the usage of antibiotics can help in limiting the antibiotic resistance menace.ref. hsr22111-bib-0002, ref. hsr22111-bib-0003
Report on pregnant women’s knowledge, attitudes, and antibiotic use is rare in Ghana, especially in the Northern Region. To speed up the antibiotic stewardship campaign in Northern Ghana and implementation of appropriate interventions, a potential knowledge gap concerning antibiotic use in pregnancy and associated factors must be identified. We, therefore, conducted this study to assess the knowledge, attitude, and practice (KAP) toward antibiotic use among pregnant women attending an antenatal clinic at a primary health care in Tolon, Northern region, Ghana.
METHOD
Study design and setting
This cross‐sectional study conducted among antenatal attendees at the Tolon Health Center (THC) within the Northern Region of Ghana. This was conducted between May 2021 to October 2021.
The district lies between latitudes 9° 15" and 10° 002′ North and Longitudes 0° 53′ and 1° 25′ West. Tolon has a population of 118,101, with 58,512 being males and 59,589 females.ref. hsr22111-bib-0023 The annual population change is 4.6% and a population density of 90.06/km2.ref. hsr22111-bib-0023
Study population and eligibility criteria
The study participants were all pregnant women receiving antenatal care (ANC) at THC during the study period. Only pregnant women who gave informed consent were included in the studies. For those below 18 years, their legal guardian or parent consented for them.
Sample size calculation
We used the Yamane’s formula to determine the minimum number of participants required for the study. The formula stated that n = N/1 + Ne 2; where n is the sample size required, N is the known population size, e represents the error (0.05) at a confidence level of 95%. Using a population size of 118,101, the minimum number of participants required for the study was 399.
Sampling methods
We used a simple random technique to select study participants. The facility was visited twice in a week. For each day of visit, a maximum of 15 pregnant women were recruited for the study. In all, we recruited 702 pregnant women over the 6‐month period.
Data collection instrument
We used an interviewer‐administered questionnaire, which was adapted from other studies,ref. hsr22111-bib-0015, ref. hsr22111-bib-0024 to establish the KAPs of pregnant women regarding antibiotic use. The questionnaire constitutes a section for socio‐demographic and obstetric characteristics, KAP. The internal consistency of questions for knowledge sections that were scored was assessed and Cronbach’s α value of 0.80 was obtained.
Three trained midwifery students with the supervision of a medical officer administered the questionnaires. The questionnaires were pretested before being used. Antenatal attendees who consented by signing or thumbprinting or through their guardian were recruited into the study. The questionnaire was translated to the respondent’s local dialect by a language competent midwife when necessary.
Variables
The variables of interest socio‐demographic and obstetric history, KAP regarding antibiotic use.
The main outcomes of interest were knowledge score, desired attitude, and desired practice of antibiotic use. Knowledge score was determined as the number of questions answered correctly out of the total questions. Knowledge score above the mean knowledge score was considered as good knowledge.ref. hsr22111-bib-0015 For attitude and practice, we calculated the total desired answers and reported them in frequencies. Purchase and use of antibiotics without prescription was considered as self‐medication.
Socio‐demographic and obstetric history, knowledge, and attitude were tested as the main predictors of antibiotic use among the pregnant women.
Data analysis
First, the data entry team checked for the completeness of the questionnaire. Incomplete questionnaires were excluded from analysis. Data were then entered into Microsoft Excel 2019, cleaned, and exported to SPSS version 26 for analysis. For descriptive statistics, frequencies and percentages were used. Logistic regression was used to detect predictors of antibiotic self‐medication and odds ratio, 95% confidence interval (CI), and p = 0.05 were used.
Ethical considerations
Permission for the study was obtained from the administrator of the facility. Ethical approval was obtained from University for Development Studies Institutional Review Board with reference UDS/RB/0006/21. The interviews were conducted in privacy and all information was kept confidential.
RESULTS
Demographic and obstetrics characteristics of participants
As seen in Table 1, participants’ age ranged from 16 to 45 years with a mean age of 25.2 ± 3.81 years. Most (54.7%) of the participants were from the age of 21 to 30 years and 660 (94.0%) were married. In terms of monthly income, 61.4% earned <Gh¢500.00 with 12.8% earning over Gh¢2000.00. Among the 702 pregnant women, 24.8% had no formal education and 29.9%, 32.5%, and 12.8% had completed primary, secondary, and tertiary school education, respectively.
Table 1: Analysis of knowledge level by background and obstetrics characteristics, attitude, and practice.
| Characteristics variable | Good knowledge | Poor knowledge | ||||||
|---|---|---|---|---|---|---|---|---|
| Total | N (%) | n | (%) | n | (%) | χ2, df | p | |
| Age (years) | ||||||||
| 16–20 | 102 | (14.5) | 60 | (8.5) | 42 | (6.0) | 4.846, 5 | 0.435 |
| 21–25 | 168 | (23.9) | 90 | (12.8) | 78 | (11.1) | ||
| 26–30 | 216 | (30.8) | 120 | (17.1) | 96 | (13.7) | ||
| 31–35 | 90 | (12.8) | 48 | (6.8) | 42 | (6.0) | ||
| 36–40 | 102 | (14.5) | 54 | (7.7) | 48 | (6.8) | ||
| ≥41 | 24 | (3.4) | 18 | (2.6) | 6 | (0.9) | ||
| Marital status | ||||||||
| Not married | 42 | (6.0) | 18 | (2.6) | 24 | (3.4) | 0.109 | |
| Married | 660 | (94.0) | 372 | (53.0) | 288 | (41.0) | ||
| Educational level | ||||||||
| None | 174 | (24.8) | 18 | (2.6) | 156 | (22.2) | 196.8, 3 | <0.001 |
| Primary | 210 | (29.9) | 138 | (19.7) | 72 | (10.3) | ||
| Secondary | 228 | (32.5) | 162 | (23.1) | 66 | (9.4) | ||
| Tertiary | 90 | (12.8) | 72 | (10.3) | 18 | (2.6) | ||
| Monthly income | ||||||||
| Less than 500 | 276 | (39.3) | 84 | (12.0) | 192 | (27.4) | 135.9, 4 | <0.001 |
| 500–999 | 150 | (21.4) | 90 | (12.8) | 60 | (8.5) | ||
| 1000–1499 | 72 | (10.3) | 48 | (6.8) | 24 | (3.4) | ||
| 1500–1999 | 114 | (16.2) | 90 | (12.8) | 24 | (3.4) | ||
| ≥2000 | 90 | (12.8) | 78 | (11.1) | 12 | (1.7) | ||
| Duration of pregnancy | ||||||||
| First trimester | 108 | (15.4) | 66 | (9.4) | 42 | (6.0) | 2.411, 2 | 0.300 |
| Second trimester | 318 | (45.3) | 168 | (23.9) | 150 | (21.4) | ||
| Third trimester | 276 | (39.3) | 156 | (22.2) | 120 | (17.1) | ||
| Gravidity | ||||||||
| First | 126 | (17.9) | 62 | (8.8) | 64 | (9.1) | 5.191, 4 | 0.261 |
| Second | 162 | (23.1) | 84 | (12.0) | 78 | (11.1) | ||
| Third | 180 | (25.6) | 106 | (15.1) | 74 | (10.5) | ||
| Fourth | 156 | (22.2) | 90 | (12.8) | 66 | (9.4) | ||
| Fifth or more | 78 | (11.1) | 48 | (6.8) | 30 | (4.3) | ||
| Parity | ||||||||
| Nulliparous | 138 | (19.7) | 78 | (11.1) | 60 | (8.5) | 3.998, 3 | 0.262 |
| Primiparous | 198 | (28.2) | 108 | (15.4) | 90 | (12.8) | ||
| Multiparous | 342 | (48.7) | 186 | (26.5) | 156 | (22.2) | ||
| Grand multiparous | 24 | (3.4) | 18 | (2.6) | 6 | (0.9) | ||
| Ever lost pregnancy | ||||||||
| No | 438 | (62.4) | 276 | (39.3) | 162 | (23.1) | <0.001 | |
| Yes | 264 | (37.6) | 114 | (16.2) | 150 | (21.4) | ||
| Number of pregnancies lost (n = 264) | ||||||||
| One | 216 | (30.8) | 84 | (12.0) | 132 | (18.8) | 10.10, 2 | 0.006 |
| Two | 42 | (6.0) | 18 | (2.6) | 24 | (3.4) | ||
| Three | 6 | (0.9) | 6 | (0.9) | 0 | (0.0) | ||
| Pregnant women should not accept antibiotics from family to treat an infection | ||||||||
| Disagree | 300 | (42.7) | 156 | (22.2) | 144 | (20.5) | 2.833, 2 | 0.243 |
| Agree | 312 | (44.4) | 180 | (25.6) | 132 | (18.8) | ||
| Neutral | 90 | (12.8) | 54 | (7.7) | 36 | (5.1) | ||
| Pregnant women must consult a doctor before taking antibiotic | ||||||||
| Disagree | 60 | (8.5) | 36 | (5.1) | 24 | (3.4) | 0.5979, 2 | 0.742 |
| Agree | 600 | (85.5) | 330 | (47.0) | 270 | (38.5) | ||
| Neutral | 42 | (6.0) | 24 | (3.4) | 18 | (2.6) | ||
| Pregnant women should not purchase antibiotics over the counter | ||||||||
| Disagree | 108 | (15.4) | 54 | (7.7) | 54 | (7.7) | 13.87, 2 | 0.001 |
| Agree | 528 | (75.2) | 312 | (44.4) | 216 | (30.8) | ||
| Neutral | 66 | (9.4) | 24 | (3.4) | 42 | (6.0) | ||
| Do you complete the course of regimen of antibiotic treatment | ||||||||
| No | 396 | (56.4) | 222 | (31.6) | 174 | (24.8) | 0.760 | |
| Yes | 306 | (43.6) | 168 | (23.9) | 138 | (19.7) | ||
| Do you take more than the prescribed amount of antibiotic when you do feel well | ||||||||
| No | 672 | (95.7) | 366 | (52.1) | 306 | (43.6) | 0.008 | |
| Yes | 30 | (4.3) | 24 | (3.4) | 6 | (0.9) | ||
| Do you keep non‐prescribed antibiotics at home in case you would need it | ||||||||
| No | 384 | (54.7) | 228 | (32.5) | 156 | (22.2) | 0.027 | |
| Yes | 318 | (45.3) | 162 | (23.1) | 156 | (22.2) | ||
| Do you purchase antibiotics from over‐the ‐counter for an infection? | ||||||||
| No | 384 | (54.7) | 294 | (41.9) | 90 | (12.8) | <0.001 | |
| Yes | 318 | (45.3) | 96 | (13.7) | 222 | (31.6) | ||
Also, in the study were 138(19.7%) nulliparous, 198(28.2%) were primiparous, 342(48.7%) multiparous, and 24(3.4%) grand multiparous women. Three hundred and eighteen (45.3%) of the pregnant women were in their second trimester with an average number of gravidae of 2.85 ± 1. 264 and 264 (37.6%) had lost a pregnancy.
Knowledge of antibiotic use among pregnant women
We used nine questions to assess participants’ knowledge of antibiotic usage during pregnancy and antibiotic resistance. The mean knowledge score was 6.5 ± 1.2., which was the minimum score for good knowledge. Three hundred and ninety (55.6%) had good knowledge. More than half of the participants, 54.7% and 66.7% knew that antibiotics are not used to treat headaches and cough, and antibiotics can be used to treat flu, respectively. Also, 91.5% knew that antibiotic resistance is when an antibiotic is unable to kill germs and 94.9% knew that resistance is a serious health issue (Figure 1).
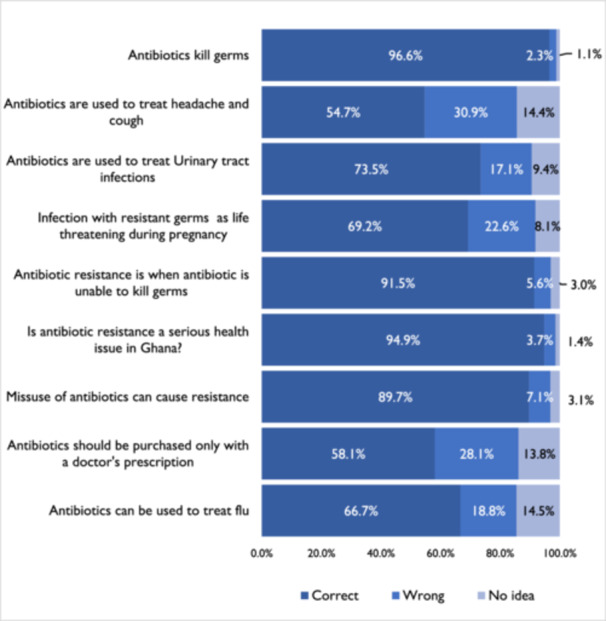
There were statistically significant associations between participants’ background and obstetric characteristics and knowledge of antibiotic use and antibiotic resistance, except for age (p = 0.435), marital status (p = 0.109), and parity (p = 0.262). Also, there was a significant association between pregnant women’s knowledge and self‐medication or over‐the‐counter purchase of antibiotics (Table 1 and Figure 1).
Attitudes of pregnant women towards antibiotic use
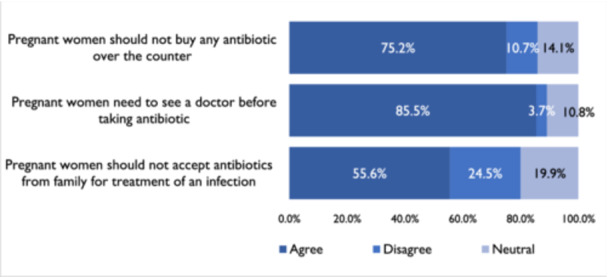
Six hundred (85.5%) participants agreed that pregnant women need to consult a doctor before taking antibiotics. However, only 75.2% agreed that pregnant women should not buy any antibiotics over the counter. Also, 55.6% agreed it is not good to accept antibiotics from family members to treat infection (Figure 2).
Practices of pregnant women regarding antibiotics
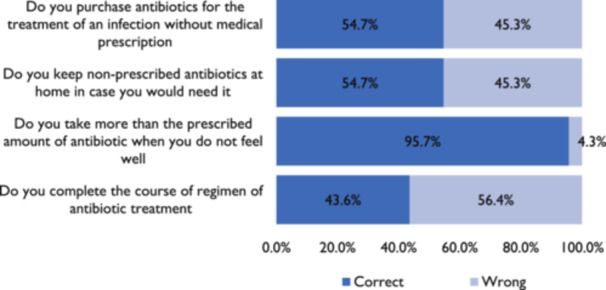
In this study, 45.3% of the women reported having engaged in self‐medication through the purchase of unprescribed antibiotics over the counter whiles pregnant. Only 43.6%, completed the course of antibiotic regimen for treatment and 54.7% do not keep antibiotics at home (Figure 3).
Predictors of knowledge of antibiotic use and resistance among pregnant women
To identify the predictors of knowledge among pregnant women, we performed a logistic regression analysis to compare participants’ demography and knowledge score (Table 2.) The regression model analysis reveals that pregnant women who have had primary secondary and tertiary education were 16.61 (CI: 9.523–29.46; p < 0.001), 21.27 (CI: 12.19–37.45; p < 0.001), and 34.67 (CI: 16.99–71.94; p < 0.001) times likely to be knowledgeable than those who had never had formal education. Also, we found out that increased monthly income is associated with an increased likelihood to have good knowledge as those who earned between Gh¢500–999, Gh¢1000–1499, Gh¢1500–1999, and Gh¢2000 or more were 3.429 (CI: 2.257–5.186; p < 0.001), 4.571 (CI: 2.588–7.962; p < 0.001), 8.571 (5.112–14.06; p < 0.001), and 14.86 (7.594 to 28.22; p < 0.001) times likely to have good knowledge that those that earn <Gh¢500. We also detected that good knowledge is associated with a 40% decrease in the odds of keeping nonprescribed drugs at home.
Table 2: Logistic regression analysis of predictors of knowledge among study participants.
| Characteristics | OR | 95% CI | p |
|---|---|---|---|
| Marital status | |||
| Not married | 1 | ||
| Married | 1.722 | 0.9324–3.163 | 0.109 |
| Educational Level | |||
| None | 1 | ||
| Primary | 16.61 | 9.523–29.46 | <0.001 |
| Secondary | 21.27 | 12.19–37.45 | <0.001 |
| Tertiary | 34.67 | 16.99–71.94 | <0.001 |
| Monthly income | |||
| <500 | 1 | ||
| 500–999 | 3.429 | 2.257–5.186 | <0.001 |
| 1000–1499 | 4.571 | 2.588–7.962 | <0.001 |
| 1500–1999 | 8.571 | 5.112–14.06 | <0.001 |
| ≥2000 | 14.86 | 7.594–28.22 | <0.001 |
| Pregnant women should not buy antibiotics over the counter | |||
| Disagree | 1 | ||
| Agree | 1.444 | 0.9614–2.170 | 0.088 |
| Neutral | 0.5714 | 0.3008–1.093 | 0.086 |
| Do you keep non‐prescribed antibiotics at home in case you would need it | |||
| No | 1 | ||
| Yes | 1.407 | 1.039–1.888 | 0.027 |
| Do you purchase antibiotics from over‐the‐counter for an infection? | |||
| No | 1 | ||
| Yes | 7.554 | 5.366–10.55 | <0.001 |
Abbreviations: 95% CI, 95% confidence interval; OR, odds ratio.
Predictors of antibiotic self‐medication in pregnant women
As indicated in Table 3, education, monthly income, good practice, and good knowledge were significantly associated with a reduced likelihood to self‐medicate. Pregnant women who have had primary, secondary and tertiary had 0.2679 (CI: 0.1707–0.4152; p < 0.001), 0.1296 (CI: 0.08330–0.2039; p < 0.001), and 0.1157 (CI: 0.06585–0.2070; p < 0.001) reduced odd of self‐medicating with antibiotics. Also, we found out that an increase in monthly income is associated with decreased odds of self‐medication. Those who earned Gh¢1000–1499, Gh¢1500–1999, and Gh¢2000, or more had reduced odds of 0.05329 (CI: 0.02415–0.1279; p < 0.001), 0.1563 (CI: 0.09444–0.2591; p < 0.001), 0.04187 (CI: 0.01918–0.09848; p < 0.001), respectively. We realized that desired practice of completing the course of the regimen of antibiotics for treatment was associated with a 58.4% decrease in the odds of self‐medication with antibiotics. Those who keep unprescribed antibiotics at home were 2.69 (CI: 1.989–3.672; p < 0.001) times more likely to engage in self‐medication with antibiotics. Those who had good knowledge were associated with an 86.8% decrease in odds of self‐medication.
Table 3: Logistic regression analysis of predictors of antibiotic self‐medication among study participants.
| Characteristics | OR | 95% CI | p |
|---|---|---|---|
| Age (years) | |||
| 16–20 | 1 | ||
| 21–25 | 0.5752 | 0.3529–0.9587 | 0.032 |
| 26–30 | 0.5625 | 0.3468–0.9126 | 0.025 |
| 31–35 | 0.5625 | 0.3090–0.9945 | 0.057 |
| 36–40 | 1.607 | 0.9246–2.838 | 0.123 |
| 41–45 | 0.375 | 0.1397–1.042 | 0.050 |
| Educational level | |||
| None | 1 | ||
| Primary | 0.2679 | 0.1707–0.4152 | <0.001 |
| Secondary | 0.1296 | 0.08330–0.2039 | <0.001 |
| Tertiary | 0.1157 | 0.06585–0.2070 | <0.001 |
| Monthly Income | |||
| <500 | 1 | ||
| 500–999 | 1.507 | 0.9870–2.322 | 0.069 |
| 1000–1499 | 0.05329 | 0.02415–0.1279 | <0.001 |
| 1500–1999 | 0.1563 | 0.09444–0.2591 | <0.001 |
| ≥2000 | 0.04187 | 0.01918–0.09848 | <0.001 |
| Gravidity | |||
| First | 1 | ||
| Second | 1.436 | 0.8871–2.281 | 0.154 |
| Third | 0.8889 | 0.5546–1.401 | 0.638 |
| Fourth | 1.556 | 0.9807–2.494 | 0.073 |
| Fifth or more | 0.5926 | 0.3308–1.060 | 0.103 |
| Parity | |||
| Nulliparous | 1 | ||
| Primiparous | 1.296 | 0.8246–2.010 | 0.249 |
| Multiparous | 1.502 | 1.014–2.267 | 0.047 |
| Grand multiparous | 0.5185 | 0.1980–1.384 | 0.186 |
| How many lost pregnancy | |||
| None | 1 | ||
| One | 1.55 | 1.111–2.140 | 0.008 |
| Two | 1.387 | 0.6979–2.754 | 0.344 |
| Three | 0.2312 | 0.02003–1.418 | 0.141 |
| Pregnant women should not accept antibiotics from a family member for treatment of an infection | |||
| Disagree | 1 | ||
| Agree | 0.531 | 0.3835–0.7304 | <0.001 |
| Neutral | 0.2125 | 0.1098–0.4059 | <0.001 |
| Pregnant women should not buy antibiotics over the counter | |||
| Disagree | 1 | ||
| Agree | 0.5804 | 0.3823–0.8894 | 0.010 |
| Neutral | 0.96 | 0.5319–1.747 | 0.900 |
| Do you complete the course of regimen of antibiotic treatment | |||
| No | 1 | ||
| Yes | 0.4167 | 0.3074–0.5659 | <0.001 |
| Do you keep nonprescribed antibiotics at home in case you would need it | |||
| No | 1 | ||
| Yes | 2.69 | 1.989–3.672 | <0.001 |
| Knowledge score | |||
| Poor knowledge | 1 | ||
| Good knowledge | 0.1324 | 0.09478–0.1864 | <0.001 |
Abbreviations: 95% CI, 95% confidence interval; OR, odds ratio.
DISCUSSION
This study was conducted to assess the KAP of antibiotic use and the prevalence of antibiotic self‐medication among pregnant women receiving ANC in a primary health facility in Northern Ghana.
In this study, 55.6% of pregnant women had good knowledge of antibiotic use and resistance, which is however lower than the 80% reported among pregnant women in South Africa.ref. hsr22111-bib-0015 Studies in different parts of the world indicate different levels of self‐medication among pregnant women.ref. hsr22111-bib-0008, ref. hsr22111-bib-0017, ref. hsr22111-bib-0024, ref. hsr22111-bib-0025, ref. hsr22111-bib-0026 In this study, 45.3% of the women reported having purchased antibiotics over the counter without a prescription while pregnant. This rate is in contrast to the 16.6% in South Africa,ref. hsr22111-bib-0015 12.5%, and 25.1% in Ethiopia,ref. hsr22111-bib-0027, ref. hsr22111-bib-0028 and 37% in Nigeriaref. hsr22111-bib-0009 that has been reported among pregnant women. Reasons attributed to self‐medication include the urge for self‐care, feeling of sympathy toward family members in sickness, lack of time, lack of health services, financial constraint, ignorance, misbelieves, extensive advertisement, and availability of drugs in informal channels are responsible for the growing trend of self‐medication.ref. hsr22111-bib-0008, ref. hsr22111-bib-0029
The antibiotic resistance crisis is not only a health threat to the healthcare industry but also an economic burden for both developed and developing economies. The consequences of antibiotic resistance on patient care is dire and cannot be estimated especially in resource limited countries including Ghana.ref. hsr22111-bib-0011, ref. hsr22111-bib-0030 A major reason responsible for the antibiotic resistance crisis is overdosage and self‐medication.ref. hsr22111-bib-0030 Self‐medication is influenced by many factors.ref. hsr22111-bib-0004, ref. hsr22111-bib-0017, ref. hsr22111-bib-0018, ref. hsr22111-bib-0031, ref. hsr22111-bib-0032, ref. hsr22111-bib-0033 In this study, we report that high education level, monthly income, good practice, and good knowledge were significantly associated with a reduced likelihood to self‐medicate. Pregnant women who have had primary, secondary, and tertiary had reduced odds of self‐medicating with antibiotics. In a study conducted in Lebanon by Jamhour et al.,ref. hsr22111-bib-0034 self‐medication significantly correlated with a lower educational level. This may be because better medication knowledge is associated with higher educational levelsref. hsr22111-bib-0035 and also increase the odds of maintaining excellent or very good health.ref. hsr22111-bib-0036
Also, we found out that an increased monthly income is associated with decreased odds of self‐medication. Those who earned Gh¢1000–1499, Gh¢1500–1999, and Gh¢2000 or more had reduced odds of self‐medicating, in contrast to KAP studies among the South African cohort of pregnant women where women with higher purchasing power were more likely to self‐medicate.ref. hsr22111-bib-0015 This may be because high earners can afford the cost of medical care and the cost of drugs that can be purchased with prescription.ref. hsr22111-bib-0037, ref. hsr22111-bib-0038
We realized pregnant women who had good knowledge of antibiotics completed the course of the regimen of antibiotics for treatment and had reduced odds of practicing self‐medication with antibiotics. A similar situation was detected by Jamhour et al.,ref. hsr22111-bib-0034 where those with poor knowledge about antibiotics stopped antibiotics at the inappropriate time and were involved in self‐medication. Also, a study in South Africa reported that participants with good knowledge were six times more likely to have good practice regarding antibiotic use.ref. hsr22111-bib-0015 Pregnant women who had poor knowledge kept unprescribed antibiotics at home and were more likely to engage in self‐medication with antibiotics. Such poor practices regarding antibiotic use have been reported in many countries in Africaref. hsr22111-bib-0003, ref. hsr22111-bib-0009, ref. hsr22111-bib-0012, ref. hsr22111-bib-0015, ref. hsr22111-bib-0016, ref. hsr22111-bib-0025, ref. hsr22111-bib-0027, ref. hsr22111-bib-0038, ref. hsr22111-bib-0039 and Europe.ref. hsr22111-bib-0021, ref. hsr22111-bib-0024
The lack of knowledge about self‐medication among the study participant may be contributing to the antibiotic resistance tragedy.ref. hsr22111-bib-0003 There is therefore the need for community education about antibiotics, their use, and side effects, and to discourage them from self‐medication and misuse of antibioticsref. hsr22111-bib-0003 as the Antibiotic resistance crisis is not just a concern related to the health care industry, but can impact a country’s economic growth as well.ref. hsr22111-bib-0040
CONCLUSION
Even though 55.6% of the pregnant women demonstrated good knowledge, the prevalence of self‐medication is significantly high. We report that high education level, monthly income, good practice, and good knowledge were significantly associated with a reduced likelihood of self‐medication with antibiotics. An increase in knowledge among pregnant women about antibiotics has the potential of reducing the odds of antibiotic self‐medication by 87%. The results of this study underscore the need for effective measures and interventions to discourage self‐medication among this group. A well‐structured education that could be easily accepted and understood by pregnant women on the risks of antibiotic self‐medication should be included in the routine education at the antenatal clinics.
AUTHOR CONTRIBUTIONS
Ezekiel K. Vicar contributed to study conceptualization, design, data analysis, drafting, and revision of the manuscript. Williams Walana contributed to study conceptualization, data analysis, drafting and revision of the manuscript. Rosemond A. Fordjour contributed to methodology, investigation, drafting, and revision of the manuscript. Christiana Benneh contributed to methodology, investigation, drafting, and revision of the manuscript. Rosemond E. Bentil contributed to study design, data collection, analysis, and revision of the manuscript. Gifty M. Wuffelle contributed to the conceptualization, study supervision, and revision of the manuscript. Emmanuel K. Osabutey contributed to formal analysis, supervision, and revision of the manuscript. Gilbert Nachinab contributed to the data analysis, interpretation, drafting and revision of the manuscript. Mauvina Obeng‐Bempong contributed to study conceptualization, design, drafting and revision of the manuscript. All authors read and approved the final draft of the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
TRANSPARENCY STATEMENT
The lead author Ezekiel K. Vicar affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
References
- Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data.. Lancet Infect Dis., 2014. [PubMed]
- The antimicrobial resistance crisis: causes, consequences, and management.. Front Public Health., 2014. [PubMed]
- Self‐medication and antibiotic resistance: crisis, current challenges, and prevention.. Saudi J Biol Sci., 2017. [PubMed]
- Prevalence and causes of self‐medication in pregnant women referring to health centers in Southern of Iran.. Int J Pharm Sci Res., 2015
- Pregnancy and pregnancy‐associated hormones alter immune responses and disease pathogenesis.. Horm Behav., 2012. [PubMed]
- Anatomical and physiological alterations of pregnancy.. J Pharmacokinet Pharmacodyn., 2020. [DOI | PubMed]
- Physiological and anatomical changes of pregnancy: implications for anaesthesia.. Indian J Anaesth., 2018. [PubMed]
- Self‐medication: a current challenge.. J Basic Clin Pharm., 2014. [DOI]
- Self‐medication: potential risks and hazards among pregnant women in Uyo, Nigeria.. Pan Afr Med J., 2012
- Self‐medication practice and associated factors among pregnant women in Addis Ababa, Ethiopia.. Trop Med Health., 2018. [DOI | PubMed]
- Self‐medication practice in pregnant women from central Mexico.. Saudi Pharm J., 2018. [PubMed]
- Antibiotic use during pregnancy: a retrospective study of prescription patterns and birth outcomes at an antenatal clinic in rural Ghana.. J Pharm Policy., 2017
- Pharmacokinetics and pharmacogenetics of selective serotonin reuptake inhibitors during pregnancy: an observational study.. Ther Drug Monit., 2017. [PubMed]
- 14 World Health Organization . Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA. World Bank Group and the United Nations Population Division; 2019.
- Antibiotic use in pregnancy: knowledge, attitudes and practices among pregnant women in Cape Town, South Africa.. J Antimicrob Chemother., 2020. [PubMed]
- Self‐medication among pregnant women attending antenatal clinic at Makongoro health centre in Mwanza, Tanzania: a challenge to health systems.. BMC Pregnancy Childbirth., 2018. [PubMed]
- Prevalence and reasons of self‐medication in pregnant women: a systematic review and meta‐analysis.. Int J Community Based Nurs Midwifery., 2018. [PubMed]
- Self‐medication and associated factors among pregnant women attending antenatal care at Kemisie General Hospital, North East Ethiopia.. Patient Prefer Adherence., 2020. [PubMed]
- Determinants of self medication practices among pregnant women in Ibadan, Nigeria.. Int J Clin Pharmacy., 2011
- A review of antibiotic use in pregnancy.. Pharmacotherapy., 2015. [PubMed]
- Perception of risk regarding the use of medications and other exposures during pregnancy.. Eur J Clin Pharmacol., 2010. [PubMed]
- Substance use and self‐medication during pregnancy and associations with socio‐demographic data: a cross‐sectional survey.. Int J Nurs Sci., 2015
- 23Tolon: A District in Ghana. 2021. Accessed Novemver 24, 2021. https://www.citypopulation.de/en/ghana/admin/northern/0807__tolon/
- Attitudes, beliefs and knowledge concerning antibiotic use and self‐medication: a comparative European study.. Pharmacoepidemiol Drug Safety., 2007
- Self‐medication among pregnant women attending ante‐natal clinics in Jos‐North, Nigeria.. Int J Trop Dis Health., 2017
- Comparing the self‐medication and supplement therapy in pregnant women in Kashan rural and urban areas.. J Mazandaran Univ Med Sci., 2014
- Factors associated with self medication practice among pregnant mothers attending antenatal care at governmental health centers in Bahir Dar city administration, Northwest Ethiopia, a cross sectional study.. Pan African Med J., 2015. [DOI]
- Assessment of drug use among pregnant women in Addis Ababa, Ethiopia.. Pharmacoepidemiol Drug Safety., 2009. [DOI]
- Self‐medication practices in rural Maharashtra.. Ind J Commun Med., 2006
- Drivers of household antibiotic use in urban informal settlements in Northern Ghana: implications for antimicrobial resistance control.. Health Sci Rep., 2023. [DOI | PubMed]
- Self‐medication among pregnant women attending outpatients’ clinics in Northern Jordan‐a cross‐sectional study.. Pharmacol Res Perspect., 2021. [DOI | PubMed]
- Assessment of knowledge, attitude and behavior towards antibiotic use in primary health care patients in Fayoum Governorate, Egypt.. Alexandria J Med., 2018
- Pattern of antibiotic abuse–a population based study in Cairo.. Egypt J Chest Dis Tuberc., 2013
- Antibiotic knowledge and self‐medication practices in a developing country: a cross‐sectional study.. Am J Infect Control., 2017. [PubMed]
- Does the patients’ educational level and previous counseling affect their medication knowledge?. Ann Thorac Med., 2013. [PubMed]
- 36 Feinstein L , Sabates R , Anderson TM , Sorhaindo A , Hammond C . What are the Effects of Education on Health. Organisation for Economic Co‐operation and Development Paris; 2006:171‐354.
- Socioeconomic differences in self‐medication among middle‐aged and older people: data from the China health and retirement longitudinal study.. BMJ Open., 2017. [DOI]
- The prevalence and risks of antibiotic self‐medication in residents of a rural community in Accra, Ghana.. Sci African., 2021
- Public knowledge and attitudes regarding the use of antibiotics and resistance: findings from a cross‐sectional study among Palestinian adults.. Zoonoses Public Health., 2016. [PubMed]
- Global disease burden due to antibiotic resistance‐state of the evidence.. J Glob Health., 2016. [DOI | PubMed]