
Chronic Pain in Dogs and Cats: Is There Place for Dietary Intervention with Micro-Palmitoylethanolamide?
Abstract
Simple Summary:
Chronic pain is being increasingly recognized and addressed in small animal practice. The recent recognition that inability to communicate does not negate the possibility to experience pain requires veterinarians to actively recognize, assess and manage animal pain. In order to successfully treat pain while limiting side effects, a combination of different therapeutic weapons (e.g., analgesic drugs, acupuncture, physiotherapy and dietary interventions) is currently preferred. In this perspective, the endocannabinoid-like palmitoylethanolamide represents a promising option, since it is naturally occurring in food sources and animal tissues, addresses the mechanisms of chronic pain (i.e., immune cell hyperactivity) and is presently used in complementary feeds for dogs and cats in highly absorbable micronized formulations (i.e., micro-palmitoylethanolamide). In the present paper, the role of immune non-neuronal cells in chronic pain is reviewed. Moreover, the function of body-own palmitoylethanolamide in controlling pain through non-neuronal cell modulation is discussed. Finally, data on pain-relieving effects provided by dietary supplementation with micro-palmitoylethanolamide are presented. The critical mass of data here reviewed might help veterinary practitioners in the process of evidence-based decision-making regarding the management of chronic pain in cats and dogs.
Abstract:
The management of chronic pain is an integral challenge of small animal veterinary practitioners. Multiple pharmacological agents are usually employed to treat maladaptive pain including opiates, non-steroidal anti-inflammatory drugs, anticonvulsants, antidepressants, and others. In order to limit adverse effects and tolerance development, they are often combined with non-pharmacologic measures such as acupuncture and dietary interventions. Accumulating evidence suggests that non-neuronal cells such as mast cells and microglia play active roles in the pathogenesis of maladaptive pain. Accordingly, these cells are currently viewed as potential new targets for managing chronic pain. Palmitoylethanolamide is an endocannabinoid-like compound found in several food sources and considered a body’s own analgesic. The receptor-dependent control of non-neuronal cells mediates the pain-relieving effect of palmitoylethanolamide. Accumulating evidence shows the anti-hyperalgesic effect of supplemented palmitoylethanolamide, especially in the micronized and co-micronized formulations (i.e., micro-palmitoylethanolamide), which allow for higher bioavailability. In the present paper, the role of non-neuronal cells in pain signaling is discussed and a large number of studies on the effect of palmitoylethanolamide in inflammatory and neuropathic chronic pain are reviewed. Overall, available evidence suggests that there is place for micro-palmitoylethanolamide in the dietary management of chronic pain in dogs and cats.
Article type: Review Article
Keywords: N-acylethanolamines, palmitoylethanolamide, chronic pain, small animals, micronization, endocannabinoids, microglia, mast cells
Affiliations: Department of Veterinary Medicine, Centro di Ricerca sul Dolore Animale (CeRiDA), Università degli Studi di Perugia, 06123 Perugia, Italy; Operational Unit of Anesthesia, Centro Veterinario Gregorio VII, 00165 Roma, Italy; davidegamba@mac.com; Freelance, DG Vet Pain Therapy, 24124 Bergamo, Italy
License: © 2021 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.3390/ani11040952 | PubMed: 33805489 | PMC: PMC8065429
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (2.5 MB)
1. Introduction
The revised definition of pain endorsed and approved by the International Association for the Study of Pain (IASP) defines pain as “An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage” [ref. 1]. An important change with respect to the previous definition (1979) consists in the recognition that verbally expressing pain is no more a prerequisite to experiencing pain. The IASP further explains that “Verbal description is only one of several behaviors to express pain; inability to communicate does not negate the possibility that a human or a nonhuman animal experiences pain” [ref. 1].
From a veterinary perspective, this represents a definitive recognition of animal pain and poses veterinary practitioners in an “algological position”, i.e., to play a proactive role in recognizing, assessing and managing animal pain. Indeed, many efforts have been made in this direction during the last decades and several European and US groups are moving toward the development of better protocols to detect [ref. 2,ref. 3,ref. 4,ref. 5,ref. 6,ref. 7], measure [ref. 8,ref. 9,ref. 10,ref. 11,ref. 12,ref. 13,ref. 14] and treat [ref. 7,ref. 15,ref. 16,ref. 17,ref. 18] animal pain accordingly. The ever-increasing availability of well-designed pain scales for acute and chronic pain in dogs and cats [ref. 19,ref. 20,ref. 21,ref. 22,ref. 23,ref. 24,ref. 25,ref. 26] and the Pain Management Guidelines [ref. 27,ref. 28] are good examples.
On the treatment side, one of the most up-to-date and clinically relevant issues consists in the multimodal approach to pain management, i.e., a combination of different therapeutic weapons, like analgesic drugs, acupuncture and physiotherapy techniques, as well as dietary interventions [ref. 29,ref. 30,ref. 31,ref. 32,ref. 33]. With regard to the last measure, calorie restriction and omega-3 fatty acids are the most investigated approaches to chronic pain in pets, particularly osteoarthritis pain [ref. 34,ref. 35].
Increasing evidence is accumulating on the beneficial effects of N-acylethanolamines (NAEs) in chronic pain. NAEs have been detected in several food sources of vegetable [ref. 36,ref. 37,ref. 38] and animal origin [ref. 39]. Moreover, chronic or subchronic high-fat diet, as well as deficient intake of essential fatty acids have been shown to profoundly affect NAE levels in animal body [ref. 40,ref. 41,ref. 42,ref. 43,ref. 44,ref. 45]. One of the most studied NAEs is the endocannabinoid-like mediator palmitoylethanolamide (PEA). Its levels in food sources and its pro-homeostatic role have been recently reviewed [ref. 46].
Interestingly, the autoprotective function of PEA was first suggested in dogs, when it was found that the canine myocardium produced PEA in response to ischemic injury [ref. 47] and canine brain possessed the biosynthetic and degradative machinery for PEA [ref. 48,ref. 49]. Since then, an increasing body of literature has emerged highlighting the importance of dietary intervention with micro-PEA—i.e., the bioavailable form of PEA—for pain relief [ref. 50,ref. 51,ref. 52,ref. 53].
The present paper outlines current information on the involvement of immune cells in chronic pain and reviews the role of endogenous PEA in pain control, as well as the experimental and clinical data on pain relieving effects provided by different PEA formulations.
Given that some micro-PEA-containing dietary supplements for dogs and cats are currently being available on the European market, this review wishes to provide scientific evidence to make informed decisions about the management of chronic pain in cats and dogs.
2. Pain Classification
Pain includes at least two dimensions, i.e., physical and emotional components. From a physical perspective, although pain is often conceived as a homogeneous sensory entity, several distinct types exist: transient, inflammatory, neuropathic and functional pain (Figure 1) [ref. 54].
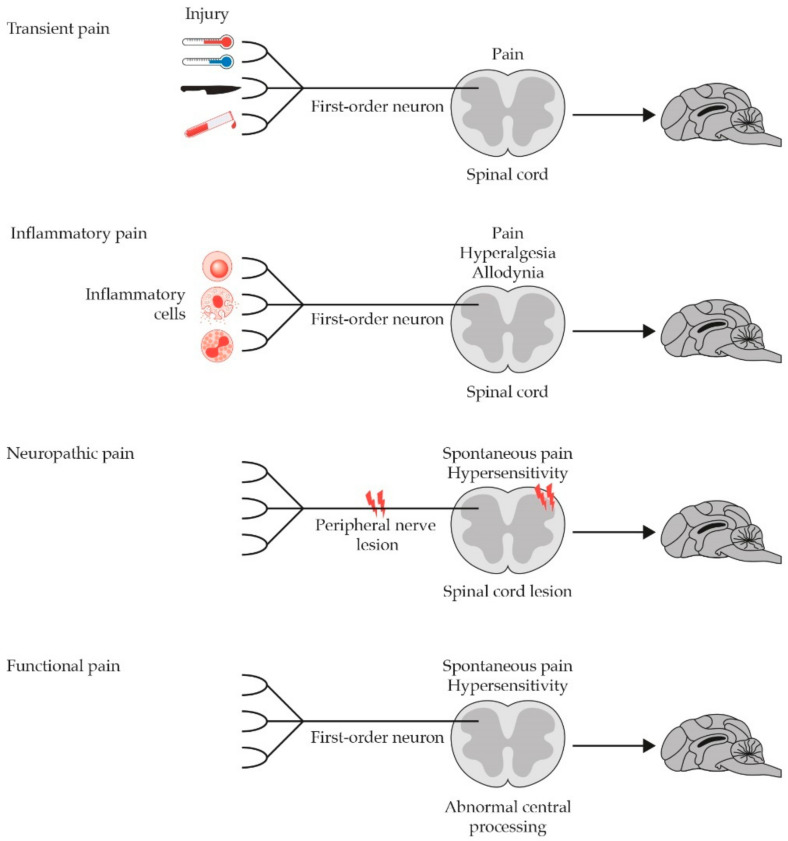
Transient pain develops when a potentially harmful insult is applied to a superficial or deep tissue (cutaneous/mucous or musculoskeletal/visceral, respectively) for such a short time that it does not cause tissue damage (potential damage). It develops rapidly and has a transient nature, disappearing with the end of the harmful stimulus or shortly thereafter. Transient pain acts like an alarm signal, capable of activating a sudden withdrawal reflex that protects the tissues from the noxious stimulus (adaptive pain). It develops thanks to the activation of the nociceptive system and the transduction, transmission, modulation and integration events that follow (nociceptive pain).
Inflammatory pain derives from damage-induced inflammation to somatic or visceral tissues (actual damage). It can be acute or chronic, depending on the nature of the underlying disease. While the former still has a protective purpose, as it limits movements and further damage until the repair is completed (adaptive pain), the latter lacks any biological purpose (maladaptive pain). Inflammatory pain is the result of nociceptor activation by inflammatory soup mediators released from immune cells, mainly mast cells. This leads to the development of neurogenic inflammation and brings about subsequent neurochemical changes, like wind-up and long-term potentiation, as well as translational and transcriptional modifications (e.g., lower activation threshold of nociceptors and increased expression of functional proteins involved in pain processing). The increased firing rate of the first and projection neuron (i.e., peripheral and central sensitization, respectively) is the main feature of inflammatory pain and leads to primary or secondary hyperalgesia (i.e., increased response to painful stimuli at the site of, or distant to the stimulus) and allodynia (i.e., painful response to harmless stimuli).
Neuropathic pain is defined by IASP as “pain that arises as a direct consequence of a lesion or disease affecting the somatosensitive system”. It results from an abnormal activation of the pain pathways, due to a dysfunction or damage to peripheral nerves and/or dorsal nerve roots (peripheral neuropathic pain) as well as spinal cord and/or brain (central neuropathic pain). Accordingly, it is considered disnociceptive, acquires a pathological, maladaptive nature and can be viewed as a disease itself rather than a symptom. Neuropathic pain can last for months to years or possibly even a lifetime, being thus considered a type of chronic pain. Possible mechanisms of peripheral neuropathic pain are (i) persistent hyperexcitability of nociceptors (even after damage repair), (ii) increased excitability of nociceptive fibers following nerve damage (e.g., after dysmyelinosis or neuroma formation), and (iii) structural/functional changes of spinal synapses following nerve degeneration. The resulting burst stimulation of afferent fibers may lead to central sensitization, a hallmark of several painful disorders like feline osteoarthritis [ref. 55]. Central neuropathic pain involves spinal cord and supramedullary neuronal structures and results from lesions affecting the central nervous system or increased activity of thalamic and cortical neurons due to neurochemical changes (e.g., imbalance of glutamatergic/GABAergic transmission).
Functional pain occurs spontaneously, in the total absence of tissue damage or evident dysfunction or damage to the nociceptive nervous system. It is probably supported by persistent plastic modifications of the central neuronal circuits induced by nociceptive or dysnociceptive algogenic lesions. As a consequence, originally activated central neuronal circuits remain active even when the lesion has resolved. A possible hypothesis is that mechanisms underlying the spontaneous processing of pain are similar to those that underlie memory: modifications of central neuronal circuits, initially induced by tissue or nerve damage, would remain in the CNS as traces of memory and can be “remembered” even after the lesion has resolved. Functional pain is therefore non-nociceptive, it can last months, years or forever, establishing its chronic nature. It has no biological function and is rather pathological (maladaptive). Like neuropathic pain, functional pain can thus be viewed as a disease itself [ref. 29,ref. 54,ref. 56].
3. Role of Non-Neuronal Cells in the Development and Resolution of Chronic Pain
As introduced above, chronic pain is an unpleasant experience outlasting the time of healing. Particular cells of the immune system intimately associated with or located within the nervous system, i.e., “non-neuronal cells”, are increasingly acknowledged as major contributors to the development and maintenance of chronic pain [ref. 51]. In particular, mast cells (within the nervous system and in the periphery) and microglia (at spinal and supraspinal level) interact with neurons under physiological and pathological conditions (Table 1).
Table 1: Mast cell and microglia ID chart.
| Mast Cells | Microglia | |
|---|---|---|
| Cell type | Resident long-lived immune-inflammatory cells [ref. 57,ref. 58] | Resident long-lived immune-inflammatory cells [ref. 59,ref. 60] |
| Location | PeripheryIn association with sensory nerves, forming synapse-like structures, in virtually any tissue, especially those exposed to the environmentPNSWithin nerves (endoneural mast cells) [ref. 61,ref. 62,ref. 63,ref. 64] | CNSThroughout the brain and spinal cord (largely outnumbering neurons), where they provide nourishment to neurons, regulate neural activity and generate innate immune responses [ref. 65] |
| CNSSpinal meninges; different brain parenchymal sites (e.g., hippocampus and thalamic, hypothalamic region); blood brain barrier (brain side), generally located near microglia [ref. 66,ref. 67,ref. 68] | ||
| Activation kinetics | Rapid release of prestored mediator in response to stimuli (e.g., sensory nerve activation), thanks to a wide range of receptorsRelease more than 50 mediators with vasoactive, neurosensitizing and pro-inflammatory effects [ref. 69,ref. 70,ref. 71,ref. 72] | Become activated in response to local stress (e.g., nerve injury), shifting their phenotype from a quiescent to an activated stateRelease pro-inflammatory cytokines and chemokines in the brain and spinal cord [ref. 73,ref. 74] |
| Type of pain involved in | Inflammatory and neuropathic pain, either visceral and somatic, e.g., osteoarthritis pain, discogenic pain, viscerovisceral hyperalgesia [ref. 75,ref. 76,ref. 77,ref. 78,ref. 79,ref. 80,ref. 81,ref. 82,ref. 83,ref. 84,ref. 85,ref. 86,ref. 87,ref. 88] | Neuropathic pain (e.g., canine intervertebral disk disease); also involved in allergic-induced neuropathic pain, acute inflammatory pain, paradoxical pain associated with long-term opioid administration [ref. 59,ref. 89,ref. 90,ref. 91,ref. 92,ref. 93] |
Abbreviations. CNS, central nervous system; PNS, peripheral nervous system.
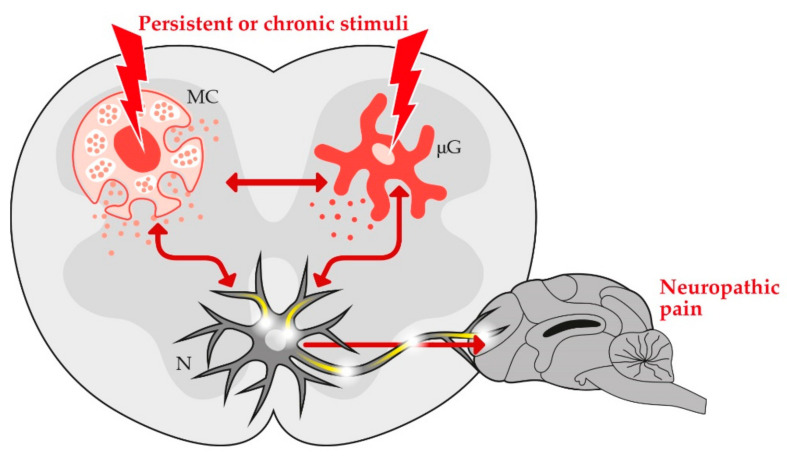
While in the first situation non-neuronal cells support the well-function of neurons (e.g., through releasing neurotrophic factors), in the latter they may become hyper-activated and may cause pain to continue after the original injury has healed [ref. 94,ref. 95]. In fact, prolonged activation of non-neuronal cells leads to uncontrolled release of pro-inflammatory mediators resulting in long-lasting plastic changes of synaptic connectivity, with enhanced transmission of nociceptive information, alterations of pain signaling pathways and chronic pain development [ref. 96,ref. 97].
It should also be considered that a bidirectional crosstalk between mast cells and microglia exists [ref. 98] and is currently acknowledged as a critical event in pain hypersensitivity [ref. 64,ref. 99]. Accordingly, non-neuronal cell hyper-activation—and the resulting neuroinflammation—is a key player of pain states (Figure 2) [ref. 100,ref. 101,ref. 102].
Interestingly, non-neuronal cells are also endowed with crucial protective functions in resolution of neuroinflammation and pain [ref. 59]. Indeed, mast cells and microglia are able to reduce sensitization by producing pro-resolution mediators, the so-called specialized pro-resolving lipid mediators [ref. 103,ref. 104,ref. 105].
In this framework, particular attention is currently devoted to endocannabinoids and related lipid compounds, such as NAEs and more particularly PEA [ref. 106,ref. 107,ref. 108,ref. 109]. As detailed below, PEA and similar endocannabinoids are locally released on demand during injury to counterbalance the effects of pro-algesic mediators [ref. 110,ref. 111].
4. Endogenous PEA and Pain Modulation
As briefly introduced above, non-neuronal cells not only dangerously boost pain signaling, but also exert crucial functions in resolution of neuroinflammation and pain, through pro-resolution mediators. Among them, endocannabinoids and related NAEs are increasingly being acknowledged to play key roles in pain modulation, with PEA being one of the most studied [ref. 112]. It has been repeatedly found in dozens of vegetable and animal food sources (in nanogram per gram level), from soy to carrots and from eggs to beef [ref. 39,ref. 46]. Moreover, PEA levels have also been detected in virtually any tissue and body fluid [ref. 46,ref. 51], where it is enzymatically produced “on demand” in response to actual or potential damage and enzymatically cleaved when it has served its purpose [ref. 51,ref. 52,ref. 113,ref. 114,ref. 115].
The late Nobel prize winner Rita Levi Montalcini first proposed that PEA acts as an Autacoid Local Injury Antagonist (ALIA), through down-modulating mast cell degranulation [ref. 116,ref. 117]. It was then found that PEA is synthesized by mast cells and microglia [ref. 118,ref. 119] and is able to keep cell reactivity within physiological boundaries [ref. 51], thereby controlling neuroinflammation and chronic pain [ref. 120,ref. 121,ref. 122].
It has also been demonstrated that PEA not only acts through non-neuronal cells, but may also directly influence neurons. Indeed, PEA was shown to (i) exert protective effects on cultured cortical and cerebellar neurons [ref. 123,ref. 124], (ii) control spontaneous GABAergic synaptic activity in striatal neurons [ref. 125], (iii) dose-dependently increase intracellular calcium concentration in sensory neurons thereby desensitizing pain receptors [ref. 126]; (iv) modulate the activity of dorsal root ganglion neurons [ref. 127].
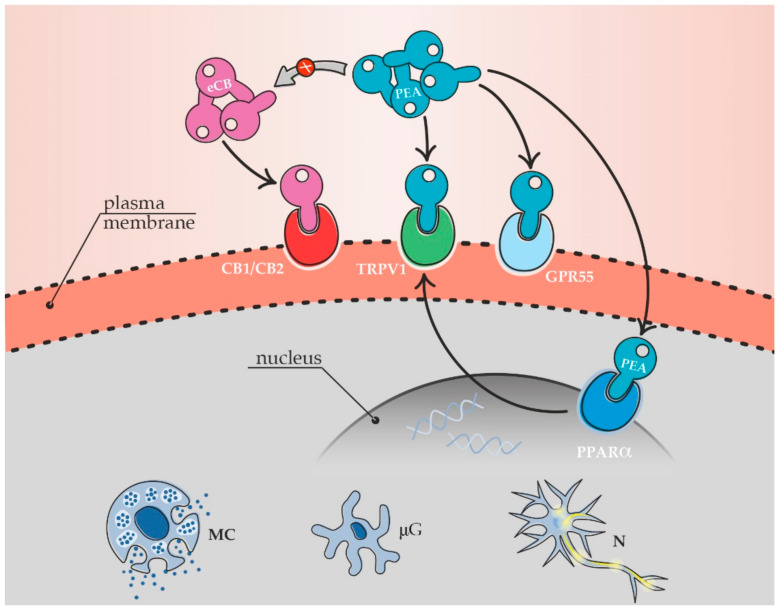
On the molecular side, PEA controls neuronal and non-neuronal cells through direct or indirect receptor targets, ranging from canonical to putative cannabinoid receptors, i.e., cannabinoid receptor type 1 and 2 (CB1 and CB2), peroxisome proliferator-activated receptor α (PPARα), transient receptor potential vanilloid 1 (TRPV1) and G protein-coupled receptors 55 and 119 (GPR55, GPR119) [ref. 65,ref. 126,ref. 127,ref. 128,ref. 129,ref. 130]. The indirect receptor agonism—i.e., a particular kind of entourage effect—depends on PEA ability to increase the local levels of the endocannabinoids anandamide (AEA) and/or 2-arachydonoylglycerol (2-AG) [ref. 52,ref. 125,ref. 131,ref. 132]. Different types of cannabinoid receptors have been recently localized in canine and feline central and peripheral organs. In particular, the target receptors of PEA have been found in canine and feline skin [ref. 133,ref. 134,ref. 135], along the gastrointestinal tract [ref. 136,ref. 137,ref. 138], in different brain areas [ref. 139,ref. 140,ref. 141,ref. 142], spinal cord and dorsal root ganglia [ref. 141,ref. 143]. The distribution of cannabinoid receptors in dogs and cats has been recently addressed by Gugliandolo et al. [ref. 46], to whose paper the reader is referred for more detailed information.
The multiple receptor mechanism(s) of PEA is responsible for innate pain control (Figure 3) [ref. 46,ref. 52] and provides PEA with a natural analgesic function, originally proposed in the late 1990s by Calignano and colleagues [ref. 144] and later even better designed by Piomelli and Sasso [ref. 145].
Currently, the role of body-own PEA in pain control is unquestionably proven by the recent case of a pain-insensitive woman who lacks the NAE degradative enzyme [ref. 146]. She feels almost no pain and has much higher levels of NAEs, with PEA levels being around 4-fold higher than normal.
In summary, PEA is an endogenous compound endowed with pain-relieving functions. It is locally produced on demand by non-neuronal cells and other cell types in response to an actual or potential damage, and acts as an endocannabinoid direct or indirect agonist to keep non-neuronal cell response within homeostatic boundaries.
5. Causes and Prevalence of Maladaptive Pain in Dogs and Cats
In the last decades, pets are becoming an increasingly important part of family life, being often considered real family members. Owners are more and more often seeking veterinary attention for various diseases affecting their pets, including pain. However, while most information on pain control in dogs and cats exists regarding peri-operative analgesic use, chronic pain conditions are still being undiagnosed and under-treated, especially in the feline species [ref. 147].
Indeed, many conditions may cause maladaptive pain in dogs and cats, as summarized in Table 2.
Table 2: Main causes of maladaptive pain in dogs and cats. From [ref. 148].
| Main Causes of Inflammatory Pain |
| Chronic lesions/inflammations affecting superficial tissues (skin, mucous membranes, teeth, some portions of the eye) and deep somatic tissues (bones, muscles, joints) |
| Chronic ulcers at skin, mucous, or corneal sites |
| Chronic inflammatory diseases |
| Gingivostomatitis Periodontitis Pulpits Otitis Conjunctivitis Keratitis Osteoarthritis |
| Myofascial trigger points |
| Discs herniation |
| Somatic cancers (skin, breast, osteosarcoma) |
| Chronic injury/inflammation affecting deep visceral tissues |
| Chronic inflammatory diseases Inflammatory bowel disease (IBD) Pancreatitis Cystitis (i.e., feline idiopathic cystitis) Prostatitis |
| Gastrointestinal ulcers |
| Cancers affecting visceral districts Primary visceral cancer Metastatic invasion of viscera |
| Main Causes of Neuropathic Pain |
| Peripheral and central nervous system disorders |
| Poliradiculoneuritis |
| Diabetic neuropathy |
| Disk compression radiculopathy with nerve damage |
| Tumor infiltration neuropathy |
| Paraneoplastic neuropathies |
| Myelin sheath cancer |
| Central nervous system (CNS) cancers |
| Chronic visceral pathologies with neuropathic component |
| Chronic pancreatitis |
| IBD |
| Feline interstitial cystitis |
| Visceral cancers |
The incidence of pain in dogs and cats has not received much attention so far. A cross-sectional study on 317 dogs and 112 cats admitted to an emergency service reported that 56% and 54% of dogs and cats respectively were painful, with most dogs suffering from deep somatic pain and most cats from visceral pain [ref. 149]. The percentage was lower in outpatients (1153 dogs and 652 cats), with 20% of dogs and 14% of cats showing evidence of pain [ref. 150]. Neuropathic pain was diagnosed in 7–8% of both species [ref. 150,ref. 151].
Among the causes listed in Table 2, one of the most frequent painful conditions in dogs and cats is osteoarthritis (OA), otherwise referred to as osteoarthrosis or degenerative joint disease. The prevalence of canine OA published so far varies widely. In the UK, estimates range from 6.6% in primary-care services [ref. 152,ref. 153] to 20% based on referral data [ref. 154]. Estimates from North America made on radiographic and clinical data from referral settings show the age-specific prevalence of canine OA, with values ranging from 20% in dogs older than one year to 80% in dogs over eight years [ref. 155]. A cross-sectional study on radiographic signs of feline OA showed an overall prevalence of 92% in randomly selected domestic cats (mean age of 9.9 years) [ref. 156,ref. 157].
Finally, it should be mentioned that recognizing and measuring pain in animals is anything but easy. Further complicating the issue is the discovery that people rate pain sensitivity differently based on breed-specific stereotypes or phenotypic traits and dog breed archetypes [ref. 158]. Many excellent review papers are available on pain assessment in companion animals, which the reader is referred to [ref. 22,ref. 23,ref. 24,ref. 159,ref. 160].
6. Management of Pain in Dogs and Cats
As previously discussed, chronic pain—regardless of the underlying cause—may become maladaptive, i.e., without any beneficial role. Neuropathic pain, functional pain and chronic inflammatory pain are all types of maladaptive pain. Any type of maladaptive pain is thus considered pathological and must be treated accordingly.
A full discussion on pain management in pets is behind the scope of this article. Briefly, non-steroidal anti-inflammatory drugs (NSAIDs), opioids and steroids alone or associated with adjuvant drugs such as gabapentinoids (gabapentin, pregabalin), NMDA-antagonists (amantadine, memantine), selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs) or tricyclic antidepressants (TCA, e.g., amitriptyline), among others, represent the mainstream pharmacologic treatment of pain [ref. 27,ref. 161,ref. 162]. However, when used alone or even in combination, these drugs may still fail to provide complete pain relief [ref. 149]. Moreover, they can lead to the occurrence of adverse effects, especially in the chronic use [ref. 163,ref. 164]. Chronic pain in pets thus still represents an unmet medical need.
The idea that multimodal analgesia tailored to the patient will have most chances of being effective is increasingly being acknowledged in veterinary practice [ref. 165,ref. 166,ref. 167]. In this view, dietary intervention with pro-resolving lipid compounds may represent an ideal adjunctive approach. PEA is currently one of the most promising options in this regard.
7. PEA and Formulation Challenges: A Size Issue
Before dealing with the effectiveness of PEA in chronic pain, a key formulation question must be addressed. PEA is a highly lipophilic compound and tends to aggregate in large particles (up to 2000 microns)—a big pharmaceutical issue since absorption rate is inversely related to particle size [ref. 46,ref. 108,ref. 168].
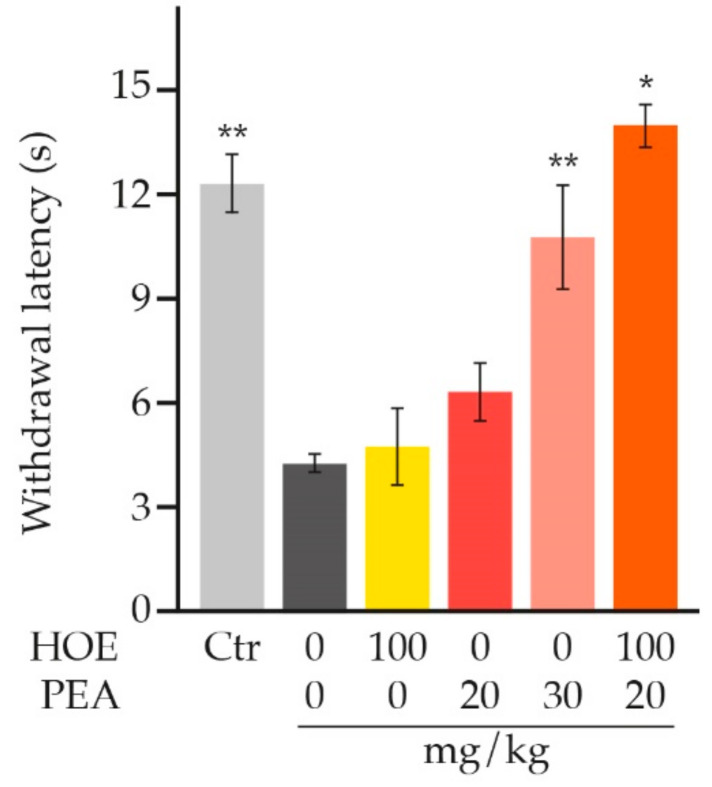
Particle size reduction through micronization techniques (down to 0.8 microns) importantly improves the dissolution and thus bioavailability (Figure 4A) [ref. 169]. This results in superior efficacy of orally administered PEA (Figure 4B) [ref. 170,ref. 171,ref. 172], while ensuring its safety [ref. 171]. Mainly for this reason, in clinical practice (in which oral route is preferred because of ease of administration) the micronized (PEA-m) and ultra-micronized (PEA-um) forms (collectively known as micro-PEA [ref. 158]) are privileged and are indeed the most investigated.
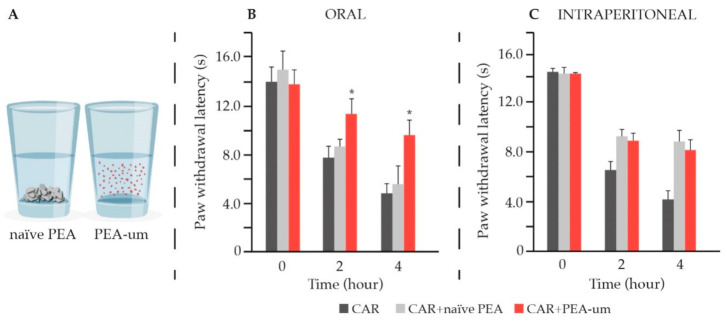
On the contrary, in laboratory animals, the intraperitoneal delivery is generally the easiest and most used administration route. Moreover, it results in faster and more complete absorption compared to oral route [ref. 173]. This is especially true if suspension in carboxymethyl cellulose is used [ref. 173], as it is usually the case with intraperitoneally administered PEA. Indeed, no difference was observed between PEA-um and naïve PEA in pain control, in the event of intraperitoneal delivery (Figure 4C), which is absolutely not the case if oral administration is used [ref. 172].
8. Preclinical Evidence for PEA in Pain Relief
The rationale to administer PEA for pain relief and wellbeing was brilliantly foreseen in the late nineties by the Nobel Prize Winner Rita Levi Montalcini, who stated that “the observed effects of Palmitoylethanolamide appear to reflect the consequences of supplying the tissue with a sufficient quantity of its physiological regulator of cellular homeostasis” [ref. 117].
Since then, several studies in preclinical pain models have been performed, with PEA being given mainly via intraperitoneal route, although intraplantar injection [ref. 144,ref. 174] and oral administration of micronised formulations [ref. 175] were also used. Interestingly, the concurrent administration of micro-PEA and morphine for 11 days attenuated the development of opioid tolerance [ref. 176], since micro-PEA strengthens morphine analgesia and allows prolonged and effective pain relief with low doses [ref. 177].
Moreover, a descending analgesic mechanism mediated by the serotonergic system has been suggested [ref. 178].
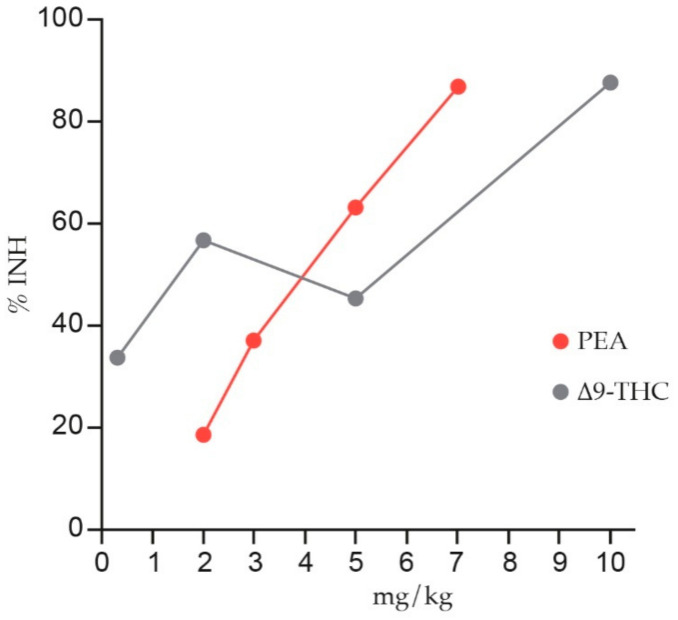
Table 3 and Table 4 summarize the main preclinical investigations. As shown, PEA exerts a clear anti-nociceptive effect in chronic pain models of either inflammatory [ref. 132,ref. 144,ref. 174,ref. 175,ref. 176,ref. 179,ref. 180,ref. 181,ref. 182,ref. 183,ref. 184,ref. 185,ref. 186,ref. 187,ref. 188,ref. 189,ref. 190,ref. 191], neuropathic [ref. 192,ref. 193,ref. 194,ref. 195,ref. 196,ref. 197,ref. 198] or mixed nature [ref. 199,ref. 200]. In particular, it has been found that the anti-nociceptive effect of PEA is comparable to synthetic or plant-derived cannabinoids used for chronic pain, like nabilone [ref. 181] and delta-9-tetrahydrocannabinol (Δ9-THC) (Figure 5) [ref. 190].
Table 3: Pain relieving effect of PEA—mainly given via intraperitoneal route—in animal models of chronic inflammatory pain. Summary of studies in chronological order.
| Animal Model | Main Behavioural Effect | Ref. |
|---|---|---|
| Somatic Inflammatory Pain | ||
| Carrageenan-induced hyperalgesia | Significant reduction of mechanical hyperalgesia | [ref. 179] |
| Formalin-induced persistent somatic pain | Significant inhibition of both early and late phasesof formalin-evoked pain behaviour | [ref. 144] |
| Formalin-induced persistent somatic pain | Significant reduction of the second phase behaviouralresponse (composite pain score) | [ref. 180] |
| Formalin-induced persistent somatic pain | Marked inhibition of pain behaviour | [ref. 174] |
| Carrageenan-induced hyperalgesia | Abolishment of hyperalgesic response | [ref. 181] |
| Intraplantar NGF-induced hyperalgesia | Significant reduction of hyperalgesia and neutrophilaccumulation | [ref. 189] |
| Carrageenan-induced hyperalgesia | Marked time-dependent reduction of mechanical hyperalgesia | [ref. 183] |
| Carrageenan-induced hyperalgesia (s.c. sponge implant) | Significant reduction of new nerve formation anddecrease of granuloma-associated hyperalgesia | [ref. 184] |
| Carrageenan-induced hyperalgesia | Significant increased mechanical and thermal thresholds (anti-hyperalgesic effect) | [ref. 202] |
| Formalin-inducednociception | Dose-dependent reduction of nocifensive behaviour in both early and late phases | [ref. 202] |
| Formalin-inducedneuropathic-like behaviour | Significant and dose-dependent decrease of mechanical allodynia and thermal hyperalgesia | [ref. 185] |
| Oxaliplatin-inducedneuropathic pain | Significant decrease of hyperalgesia and allodynia andimprovement in motor coordination | [ref. 176] |
| Streptozotocin-induceddiabetic neuropathy | Dose-dependent and significant relief of mechanical allodynia | [ref. 186] |
| Formalin-induced persistent somatic pain | Significant attenuation of the first andearly second phases of nociceptive behaviour | [ref. 132] |
| Carrageenan-induced hyperalgesia | Significant reduction of thermal hyperalgesia by 57%(superior effect compared to meloxicam) | [ref. 187] |
| CFA-induced joint pain | Significant decrease of extravasation and mechanical allodynia | [ref. 175] |
| Formalin-evoked persistent somatic pain | Significant attenuation of mechanical allodynia and heat hyperalgesia (over 90%) | [ref. 201] |
| Visceral Inflammatory Pain | ||
| Turpentine inflammation ofthe urinary bladder | Significant attenuation of the vesical hyper-reflexicresponse | [ref. 180] |
| Acetic acid-evoked writhing | Dose-dependent attenuation of the writhing response | [ref. 174] |
| Turpentine inflammation ofthe urinary bladder | Dose-dependent attenuation of referred hyperalgesia | [ref. 188] |
| Kaolin-evoked writhing | Potent inhibition of the nocifensive response | [ref. 174] |
| Magnesium sulphate-evoked writhing | Dose-dependent inhibition of the nocifensive response | [ref. 174] |
| NGF-induced inflammationof the urinary bladder | Significant increase of micturition threshold | [ref. 182] |
| PPQ-induced persistent visceral pain | Dose dependent inhibition of visceral pain measured as stretching movement inhibition | [ref. 190] |
| Cyclophosphamide-inducedcystitis | Significant decrease of the pain score | [ref. 191] |
Abbreviations. CFA, Complete Freund’s adjuvant; MIA, monosodium iodoacetate; NGF, nerve growth factor; OA, osteoarthritis; PPQ, phenyl-p-quinone.
Table 4: Pain relieving effect of PEA—mainly given via intraperitoneal route—in animal models of neuropathic and mixed pain. Summary of studies in chronological order.
| Animal Model | Main Behavioural Effect | Ref. |
|---|---|---|
| Neuropathic Pain | ||
| Partial sciatic nerve injury | Reduction of hyperalgesia (−79.4%) | [ref. 192] |
| Spinal cord injury | Significant reduction of the severity of spinal cord trauma | [ref. 193] |
| Chronic constriction injury | Significant relief of thermal hyperalgesia andmechanical allodynia | [ref. 194] |
| Chronic constriction injury | Significant and time-dependent relief of thermal hyperalgesia and mechanical allodynia (alreadyafter two administrations) | [ref. 120] |
| Partial sciatic nerve injury | Restored thermal and mechanical thresholds.Decrease of pain-induced memory deficits | [ref. 195] |
| Diabetic neuropathic pain | Significant antinociceptive effect. Significantly increased thresholds to mechanical stimuli | [ref. 196] |
| Sciatic nerve injury | Reduced nerve edema and inflammatory infiltrate (sub-optimal doses of PEA combined with acetaminophen) | [ref. 197] |
| Partial sciatic nerve injury | Restored cognitive behaviour and reduced cognitivedecline associated with neuropathic pain | [ref. 198] |
| Chronic constriction injury | Strong dose-dependent suppression of mechanical allodynia and heat hyperalgesia upon single and repeated (7 consecutive days) administration | [ref. 201] |
| Chronic mixed pain | ||
| MIA-induced OA pain | Significant decrease of mechanical allodynia andimproved locomotor function | [ref. 187] |
| MIA-induced OA pain | Significantly restored paw withdrawal thresholdand weight-bearing compared to the vehicle-treated controls in a dose-dependent fashion | [ref. 199] |
| Vitamin Ddeficiency-inducedchronic pain | Significant reduction of allodynia and neuronalsensitization | [ref. 200] |
Abbreviations. MIA, monosodium iodoacetate; OA, osteoarthritis.
Interestingly, an in-press study by Tagne and collaborators has just shown that hemp oil extract with 9.3% cannabidiol by weight has little or no effect when administered alone but synergizes with PEA to produce a greater-than-additive alleviation of neuropathic pain, upon single-dose administration (Figure 6) [ref. 201]. According to the authors, a possible explanation for the observed synergistic interaction lies in the ability of hemp oil extract to improve pharmacokinetic profile of PEA [ref. 201].
Two particularly interesting issues arise from the above findings. First, PEA is not analgesic sensu stricto since it does not modify the physiological pain threshold of control animals and rather electively normalizes conditions of hypersensitivity [ref. 176,ref. 185]. Second, PEA not only relieves pain itself but also improves pain-induced cognitive impairments [ref. 198].
As far as mechanism of action are concerned, reduced mast cell hyperplasia—even in endoneural sites—and decreased spinal microglia activation were the main observed events [ref. 120,ref. 185]. At the molecular level, the reduction of markers of pain pathway activation (e.g., Fos) and inflammatory mediators (e.g., cytokines, nerve growth factor) as well as modulation of extracellular signal-regulated kinase (ERK) and nuclear pro-inflammatory factors (e.g., NF-kB) were detected in the spinal cord [ref. 120,ref. 132,ref. 182,ref. 193,ref. 195,ref. 197]. Restoration of the glutamatergic synapses homeostasis in the prefrontal cortex and the involvement of de novo neurosteroid synthesis (i.e., allopregnanolone) in the spinal cord were also suggested to mediate PEA-induced analgesia [ref. 198,ref. 202]. Moreover, electrophysiological signs of decreased neuronal hyper-excitability were reported at the spinal cord level of PEA-um treated neuropathic animals [ref. 176,ref. 185,ref. 200]. Finally, the involvement of cannabinoid receptor(s) (e.g., CB2, CB1, PPARα) in the pain-relieving effect of PEA was repeatedly confirmed [ref. 186,ref. 192,ref. 194,ref. 199,ref. 202,ref. 203]. The up-regulation of CB2 expression by microglia through PPARα activation has also been suggested as a possible mechanism underlying the pain-relieving effect of PEA [ref. 204].
According to an impressive meta-analysis by IASP Presidential Taskforce on Cannabis and Cannabinoid Analgesia, PPARα agonists and, more specifically, PEA, are effective in attenuating pain-associated behaviors in a broad range of inflammatory or neuropathic pain models [ref. 205].
9. Clinical Evidence for Micro-PEA Dietary Supplementation in Pain Relief
On the clinical side, micro-PEA (i.e., micronized, ultramicronized or co-micronized PEA) has been orally administered as a dietary food for special medical purposes to human patients, either singly [ref. 206,ref. 207,ref. 208,ref. 209,ref. 210,ref. 211,ref. 212,ref. 213,ref. 214,ref. 215,ref. 216,ref. 217,ref. 218,ref. 219,ref. 220,ref. 221,ref. 222,ref. 223,ref. 224,ref. 225] or in combination with (i.e., add-on dietary intervention to) opioids, gabapentenoids or NSAIDs [ref. 226,ref. 227,ref. 228,ref. 229,ref. 230,ref. 231,ref. 232,ref. 233,ref. 234,ref. 235,ref. 236,ref. 237,ref. 238,ref. 239,ref. 240,ref. 241,ref. 242,ref. 243,ref. 244,ref. 245,ref. 246,ref. 247,ref. 248], as well as antioxidant compounds (e.g., luteolin, quercetin, polydatin) [ref. 249,ref. 250,ref. 251,ref. 252,ref. 253,ref. 254,ref. 255,ref. 256,ref. 257,ref. 258,ref. 259,ref. 260,ref. 261] in several painful conditions [ref. 53,ref. 262].
Altogether, nearly 5000 patients have been clinically investigated so far in dozens of published trials, showing an important overall effect in chronic pain, either neuropathic (Table 5), mixed (Table 6) or pelvic pain (Table 7).
Table 5: Pain relieving effect of micro-PEA (i.e., PEA-m or PEA-um) on chronic neuropathic pain: overview of human trials in chronological order.
| Diagnosis(Trial Design) | No. ofPts | Dose | Main Result | Ref. |
|---|---|---|---|---|
| Peripheral neuropathic pain | ||||
| Sciatic pain due to radicular and/or core compression of the sciatic nerve and discopathy(Double-blind, randomized, two doses of micro-PEA vs. placebo) | 636 | 300 mg/die or 300 mg/bid for three weeks | Significant decrease of pain on VAS (from 7 to 2) | [ref. 206] |
| Diabetic neuropathy pain associated with carpal tunnel syndrome(Group-controlled, randomized,micro-PEA treatment vs. standard care) | 50 | 600 mg/bid for two months | Significant relief of pain. Significant improvement of neurophysiologic parameters | [ref. 207] |
| Painful neuropathies(Open-label study) | 27 | 300 mg/bid for three weeks, followed by 300 mg/die for four weeks | Significant reduction of pain and improvement of electrophysiological parameters | [ref. 208] |
| Sciatic pain(Double-blind, randomized, two doses of micro-PEA vs. placebo(as an add-on therapy)) | 111 | 300 mg/die or 300 mg/bid for three weeks | Significant decrease in pain severity and duration of treatment with anti-inflammatory and analgesic drugs | [ref. 226] |
| Neuropathic chronic pain (diabetic neuropathy and postherpetic neuralgia)(Open, combination therapy with GBPs) | 30 | 600 mg/bid for 45 days | Significant decrease of pain on VAS (from 7.6 to 1.8) | [ref. 227] |
| Low back pain(Group-controlled (add-on therapy to standard analgesics)) | 81 | 600 mg/bid for three weeks followed by 600 mg/die for four weeks | Significant reduction of pain intensity compared to control group | [ref. 228] |
| Sciatic pain(Group-controlled, randomized, add-on therapy to standard analgesics) | 85 | 300 mg/bid for 30 days | Significant reliefof pain (scored both on VAS and Oswestry Low Back Pain Scale) compared to the analgesic-only group | [ref. 229] |
| Diabetic neuropathic pain(Open-label study) | 30 | 300 mg/bid for two months | Significant reduction of pain, burning, paraesthesia and numbness | [ref. 209] |
| Carpal tunnel syndrome in diabeticpts(Group-controlled, randomized vs. non-treated pts) | 40 | 600 mg/bid for two months | Significant reduction of pain and improvement of functional status and neurophysiologic parameters | [ref. 210] |
| Pain associated with carpal tunnelsyndrome(Group-controlled, randomized, two doses of micro-PEA vs. non-treatedpts) | 26 | 1st arm: 300 mg/bid for 30 days2nd arm: 600 mg/bid for 30 days | Significant dose-dependent reduction of pain and improvement of neurophysiologic parameters compared with control group | [ref. 211] |
| Chemotherapy-induced painfulneuropathy(Open-label study) | 20 | 300 mg/bid for two months | Significant pain reduction on NRS and significantly increased conduction velocity of myelinated fibers on neurophysiological assessment | [ref. 212] |
| Low back pain(Open, combination therapywith OPI) | 20 | 600 mg/bid for 30 days | Significant decrease of pain on VAS (from 7 to 2.5) | [ref. 230] |
| Various chronic pain-associated disorders(Open, combination therapywith GBPs and OPI) | 517 | 600 mg/bid for three weeks followed by 600 mg/die for four weeks | 61% decrease of mean pain score on NRS | [ref. 231] |
| Diabetic neuropathic pain(Group-controlled (micro-PEA + GBPs vs. GBPs)) | 74 | 600 mg/bid for the first 10 days, then 600 mg/die for 20 days, followed by 300 mg/die for 30 days | Significantly higher rate of responders (i.e., >60% decrease in pain score) compared to GBP group | [ref. 232] |
| Chronic neuropathic pain from lumbosciatica(Multicentral prospective, group-controlled study (add-on therapy to standard analgesics vs. standardanalgesics)) | 118 | 300 mg/bid for 30 days | Significantly larger improvements in VAS and QoL compared to standard therapy alone | [ref. 233] |
| Chronic pain associated to different pathological conditions(Observational study (add-on to poorly effective standard analgesics)) | 610 | 600 mg/bid for three weeks + 600 mg/die for the following four weeks | Significant decrease of the mean score of pain on NRS (even in pts without concomitant analgesics) | [ref. 234] |
| Diabetic neuropathy(Open-label study) | 30 | 300 mg/bid for two months | Significant decrease of pain severity and related symptoms evaluated by Michigan Neuropathy Screening instrument and NPSI | [ref. 213] |
| Diabetic or traumatic chronic neuropathic pain, with VAS greater than 6 in spite of the best therapeutic regimen with GBPs and/or OPI(Open-label study (add-on)) | 30 | 1200 mg/die for 40 days | Significant and time dependent decrease of pain on VAS and NPSI, as well as QoL on EQ-5D | [ref. 235] |
| Pain associated to fibromyalgia syndrome(Retrospective + prospective study (SNRI + GBPs vs. SNRI + GBPs +micro-PEA)) | 80 | 600 mg/bid in the first month and 300 mg/bid in the next two months | Further reduction in the number of positive tender points and significant reduction in pain, compared to SNRI + GBPs only | [ref. 236] |
| Low back pain(Case report (combined to low dose SNRI)) | 2 | 600–1200 mg/bid for two months | Significant decrease of pain on NRS | [ref. 237] |
| Failed back surgery syndrome (caused by laminectomy, discectomy, or vertebral stabilization)(Observational study (add-on to 1-month standard analgesic treatment, i.e., OPI + GBPs)) | 35 | 1200 mg/die for the first month and 600 mg/die for the second month | Further and significant decrease in pain intensity compared to the first month of standard analgesics | [ref. 238] |
| Chronic, non-cancer, non-ischemic pain in the back, joints or limbs in elderly pts (≥ 65 years)(Series of N-of-1 randomized trials) | 10 | 600 mg/bid | Statistically significant favorable impact on either pain intensity or function impairment in some of the three of the pts | [ref. 239] |
| Chronic low back pain(Two arm (prospective and retrospective), pilot observational study (add-on to OPI compared to OPI only)) | 55 | 600 mg/bid for six months | Significantly higher reduction in: | [ref. 240] |
| Neuropathic pain associated with nonsurgical lumbar radiculopathies(Retrospective study (add-on to 4-day treatment with ACT + OPI)) | 100 | 600 mg/bid for 30 days followed by 600 mg/die for 30 days | Significant pain relief in pts with mild, moderate and severe baseline painful symptoms | [ref. 241] |
| Neuropathic pain associated with nonsurgical lumbar radiculopathies with X-ray signs of spondylosis and CT/MRI signs of IVD protrusion or dehydration(Prospective single-blind (add-on to 7-day treatment with fixed combination ACT + OPI)) | 155 | 1200 mg/die for 30 days.If unsuccessful, further 30 days with 600 mg/die followed, if needed, by a second cycle of ACT + OPI for 30 days | Significant improvement of pain and disability after 30 or 60 days depending on the baseline pain severity (VAS 3–8). In pts with baseline VAS ≥9 the second ACT + OPI cycle was needed. | [ref. 242] |
| Carpal tunnel syndrome(Open, controlled study (PEA-um + surgery vs. surgery only)) | 42 | 600 mg/bid for 2 months before and 2 months after surgery + 600 mg/die for 30 days | Significant improvement in painful symptoms and overall sleep quality on PSQI | [ref. 243] |
| Burning mouth syndrome(Case report (add-on to poorly effective GBPs)) | 1 | 600 mg/bid for three months | Significant decrease of pain on VAS (from 9 to 5). Great reduction of the frequency of episodes | [ref. 244] |
| Chronic orofacial neuropathic pain (post-traumatic neuropathy)(Open-label clinical trial) | 22 | 300 mg/tidfor six weeks | Overall reduction in ongoing pain on VAS. Normalized activity patterns in the ascending pain pathway | [ref. 214] |
| Burning mouth syndrome(Preliminary randomized double-blind controlled trial) | 35 | 600 mg/bid for two months | Statistically significant higher reduction of burning mouth sensation on NRS compared to placebo | [ref. 215] |
| Fibromyalgia Syndrome(Retrospective observational study (add-on to concomitant pharmacological therapy, i.e., SSRI (n = 71), SNRI (n = 66), GBPs (n = 41), TCA (n = 40), BZD (n = 94),OPI (n = 78), NSAIDs (n = 87), MR (n = 35), ACT (n = 45)) | 407 | 600 mg/tid for 10 days followed by 600 mg/bid for 20 days followed by 600 mg/die for 125 months | Statistically significant decrease of pain on VAS and statistically significant improved QoL on FIQ | [ref. 246] |
| Low back pain—sciatica(Post-hoc analysis of a placebo-controlled study) | 600 | 600 mg/die | NNT of 1.7 (1.4–2) for the effect on pain and 1.5 (1.4–1.7) for the effect on function | [ref. 216] |
| Chronic low back pain(i.e., lumbo-sciatica and lumbo-cruralgia due to multiple herniated discs in the lumbar spine)(Open, add-on to standard analgesics + functional rehabilitation session) | 120 | 600 mg/bid for 20 days, followed by 600 mg/die for 40 days | Significant decrease of pain intensity scores (from 6.3 ± 0.1 at baseline to 3.7 ± 0.09 and 2 ± 0.09 at 30 and 60 days, respectively) | [ref. 245] |
| Central neuropathic pain | ||||
| Neuropathic pain associated with multiple sclerosis(Open-label study) | 20 | 300 mg/bid for two months | Significant decrease of neuropathic pain | [ref. 217] |
| Neuropathic pain and spasticity in post-stroke pts(Open, controlled micro-PEA + Pvs. PT only) | 20 | 600 mg/bid for two months followed by600 mg/die for 30 days | Significant decrease of pain and spasticity | [ref. 247] |
| Pain associated with stroke(Observational study(co-um PEA-Lut in association with the stroke therapy, e.g., thrombolytics)) | 250 | 700 mg + 70 mg for two months | Pain on NRS halved after 30 days | [ref. 249] |
| Migraine without aura—at least 6 months’ duration(Open-label study) | 50 | 600 mg/bid for three months | Significant decrease ofReduction of hypothermia and response to trigger factors (thermography) | [ref. 218] |
| Nummular headache(Case report (add-on todecreasing topiramate dose)) | 1 | 600 mg/die | Improvement in pain symptomsand on pain measuring scales | [ref. 219] |
| Occipital Neuralgia(Case report]) | 1 | 1200 mg/die | Significant improvement of pain, after around 2 weeks of treatment | [ref. 220] |
| Migraine with Aura(Single blind study (add-on to acute NSAIDs, i.e., ibuprofen, diclofenac sodium, or nimesuilde for about 2 days during acute migraine attack)) | 20 | 1200 mg/die for three months | Statistically significant and time-dependent pain relief, already evident at 60 days and lasting until the end of the study | [ref. 221] |
| Migraine without aura in a pediatric population(Open-label pilot study) | 70 | 600 mg/die for three months | Significant decrease of | [ref. 222] |
Abbreviations. ACT, Acetaminophen; bid, bis in die = twice daily; BZD, benzodiazepines; co-um PEA-Lut, co-ultramicronized palmitoylethanolamide and luteolin; CT, computed tomography scans; die, daily; EQ-5D, Health Questionnaire Five Dimensions; FIQ, Fibromyalgia Impact Questionnaire on quality of life; GBPs, gabapentinoids; IVD, intervertebral disk; MR = muscle relaxants; MRI, magnetic resonance imaging; NNT, Number Needed to Treat; NPSI, Neuropathic Pain Symptom Inventory; NRS, Numeric Rating Scale; NSAIDs, non-steroidal anti-inflammatory drugs; OPI, opiates; PSQI, Pittsburgh Sleep Quality Index; PT, physiotherapy; pts, patients; QoL, quality of life; tid, ter in die = three times daily; SSRI, serotonin selective reuptake inhibitors; SNRI, serotonin noradrenaline selective inhibitors; TCA, tricyclic antidepressants; VAS, visual analogue pain scale.
Table 6: Pain relieving effect of micro-PEA (i.e., PEA-m or PEA-um) on chronic mixed pain: overview of clinical trials in chronological order.
| Diagnosis[Trial Design] | No. ofPts | Dose | Main Result | Ref. |
|---|---|---|---|---|
| TMJ pain caused by OA(Double-blind randomized vs. NSAIDs) | 24 | 300 mg in the morning+ 600 mg in the eveningfor 7 days; followed by 300 mg/bid for 7 days | Significant decrease of pain on VAS (from 7 to 0.7) and significantly improved maximum mouth opening compared to NSAIDs | [ref. 223] |
| OA-induced TMJ arthralgia(Case series(initially combined with NSAIDs)) | 12 | 600 mg/die(together with NSAIDs for the first 4 days, then singly for the following 10 days) | Significant pain reduction after 4 days. Significant improvement of maximum mouth opening | [ref. 248] |
| Knee OA pain(Double-blind randomized placebo-controlled study (two doses)) | 111 | 300 mg/die or600 mg/die | Significant reduction ofWOMAC, pain on NRS and anxiety | [ref. 224] |
| Pain in arthrogenic TMJ dysfunction and similar disorders(Systematic review of 5 studies (4 RCTs + 1 retrospective cohort study)) | 227 | 300 mg/die and over | Effective in arthrogenic TMJ dysfunction and related disorders, with a superior analgesic effect to some NSAIDs and a low rate of adverse events | [ref. 225] |
Abbreviations. bid, bis in die = twice daily; die, daily; NSAIDs, non-steroidal anti-inflammatory drugs; pts, patients; OA, osteoarthritis; RCTs, randomized clinical trials; TMJ, temporomandibular joint; VAS, visual analogue pain scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Table 7: Pain relieving effect of PEA-Pol (i.e., PEA co-micronized with the antioxidant polydatin in 10:1 ratio) on chronic pelvic pain: overview of clinical trials in chronological order.
| Diagnosis[Trial Design] | No. ofPts | Dose | Main Result | Ref. |
|---|---|---|---|---|
| Chronic pelvic pain associated with endometriosis/dysmenorrhea/interstitial cystitis(Open-label study) | 25 | (200 + 20) mg/tid for 40 days | Significant reduction of pain on VAS (from 6.8 to 1.7); significant decrease in the use of NSAIDs. | [ref. 250] |
| Adolescent primarydysmenorrhea(Open-label study) | 20 | (400 + 40) mg/bidfor six months | 70% decrease in pelvic pain | [ref. 251] |
| Chronic pelvic pain and dyspareunia associated withendometriosis(Open (case series)) | 4 | (200 + 20) mg/bid forthree months | Significant decrease of pelvic pain and dyspareunia; significant reduction in the use of analgesics. | [ref. 252] |
| Pudendal neuralgia(Case report) | 1 | PEA-um300 mg/tid gradually decreased to 300 mg/die for one year | Resolution of chronic pelvic pain | [ref. 253] |
| Chronic pelvic pain associated with endometriosis(Double-blind, randomized parallel-group (celecoxib), placebo-controlled) | 61 | (400 + 40) mg/tid for three months | Significant decrease of chronic pelvic pain, dysmenorrhea and dyspareunia | [ref. 254] |
| Endometriosis associated with severe pelvic pain(Open-label study) | 24 | (400 + 40) mg/bid for three months | Statistically significant decrease of pain, dysmenorrhea and dyspareunia and improved QoL, as well as decreased assumption of NSAIDs | [ref. 255] |
| Pain related to endometriosis(Prospective study) | 47 | (400 + 40) mg/bid for three months | Significant decrease of chronic pelvic pain, dyspareunia and dysmenorrhea on VAS since the first visit (day 30) | [ref. 256] |
| Vestibulodynia(Randomized, placebo-controlled, combined with TENS) | 20 | (400 + 40) mg/bid for two months | Significant decrease of pain on VAS in both groups. Superior decrease of current perception threshold for C fibers in treated (40%) compared to placebo group (4.6%) | [ref. 257] |
| Primary dysmenorrhea(Randomized placebo-controlled with follow-up) | 220 | (400 + 40) mg/die for 10 days (from the 24th day ofcycle) | Improvement of pelvic pain in 98% of cases in the treated group vs. 56% in the placebo group. Statistically superior effect compared to placebo | [ref. 258] |
| Irritable bowel syndrome(Randomized double-blindplacebo-controlled) | 54 | (200 + 20) mg/bid for 12 weeks | Reduction of abdominal pain and discomfort | [ref. 259] |
| Symptomatic women withlaparoscopic diagnosis ofendometriosis(Single-arm, open-label) | 30 | (400 + 40) mg/bid for 80 days, after 10 days PEA-um 600 mg/bid | Significant decrease of symptoms (pain on VAS, dysmenorrhea, dyspareunia, and dyschezia, dysuria); increased QoL and psychological well-being; significant reduction in the use of the analgesics | [ref. 260] |
| Interstitial cystitis/bladder pain syndrome (IC/BPS)(Pilot, open-label bicentric study) | 32 | (400 + 40) mg/tid for three monthsfollowed by (400 + 40) mg/die for three months | Significant decrease of pelvic pain intensity on VAS from 6.9 ± 0.4 to 4.6 ± 0.4 (the effect persisting up to two months after treatment withdrawal);PUF significantly and progressively decreased; significant reduction in urinary frequency | [ref. 261] |
Abbreviations. bid, bis in die = twice daily; die, daily; NSAIDs, non-steroidal anti-inflammatory drugs; PUF, Pelvic Pain and Urgency/Frequency Symptom Scale; Pts, patients; QoL, quality of life; tid, ter in die = three times daily; TENS, transcutaneous electrical nerve stimulation therapy; VAS, visual analogue pain scale.
One of the most interesting findings comes from the neurophysiological assessment of 20 patients with chemotherapy-induced painful neuropathy, with daily administered micro-PEA 300 mg/bid for two months. Besides significant pain reduction, increased conduction velocity of myelinated fibers was recorded, with sensory nerve action potentials from sural and ulnar nerves, compound motor action potentials from peroneal and ulnar nerves and laser-evoked potentials for Aδ fibers being significantly improved [ref. 212].
A further striking finding comes from the so-called “number needed to treat” (NNT), i.e., a measure depicting the effectiveness of an intervention (the lower the NNT, the more effective the intervention). The calculation was elegantly made by researchers from the Department of Human Neurosciences, “Sapienza” University of Rome [ref. 216]. In particular, the percentage of patients who manifested at least 50% pain relief in response to a daily supplementation of micro-PEA 600 mg/die was calculated based on data from a multicenter, double-blind, placebo-controlled, randomized study on 636 patients with low back pain. NNT was found to be 1.7 [ref. 216]. It must be pointed out that it is a remarkable NNT value within the broad panorama of treatments for low back pain in human patients. A systematic review on first-line treatments for neuropathic pain has indeed shown that NNT for 50% pain relief ranges from around 4 to 10 across most positive trials (Table 8) [ref. 263]. The much lower NNT for micro-PEA (i.e., 1.7) emphasizes the good outcome for neuropathic pain relief. The relevance of the data is further strengthened by the non-significant (and indeed infinite) number needed to harm [ref. 216], that is, how many patients must receive a particular treatment for one additional patient to experience a particular adverse outcome.
Table 8: NNTs for micro-PEA and the main first-line treatments for neuropathic pain (i.e., the number of patients to treat in order to obtain one patient with at least 50% pain relief) [ref. 216,ref. 263].
| Intervention | NNT |
|---|---|
| Micro-PEA | 1.7 |
| TTAs | 3.6 |
| SNRIs | 6.4 |
| Gabapentin | 6.3 |
| Pregabalin | 7.7 |
Abbreviations. TTAs, tricyclic antidepressants; SNRIs, serotonin-norepinephrine reuptake inhibitors.
Overall, micro-PEA has shown a very favorable treatment profile in the management of chronic pain in human patients.
As far as privately owned animals are concerned, two trials have recently dealt with micro-PEA dietary administration for pain relief. The first is a case series in four jumping horses orally supplemented with PEA-um for non-responsive lameness and significant impairment of athletic performance [ref. 264]. In particular, the diagnoses were the following: navicular syndrome of the left forelimb (1 case), complicated case of chronic navicular syndrome and OA of the distal interphalangeal joint of the right forelimb (1 case), and OA of the distal intertarsal joint of the right hindlimb (2 cases). Horses were fed daily with PEA-um (2.5 g) mixed with a regular mixture of cereals for four months. At the end of the first month of supplementation, lameness on the AAEP scale (American Association of Equine Practitioners 0–5 scale, with zero indicating no perceptible lameness, and five being most extreme) showed improvement in all horses. Three months later, lameness was graded zero, allowing successful return to showjumping without disease recurrence [ref. 264].
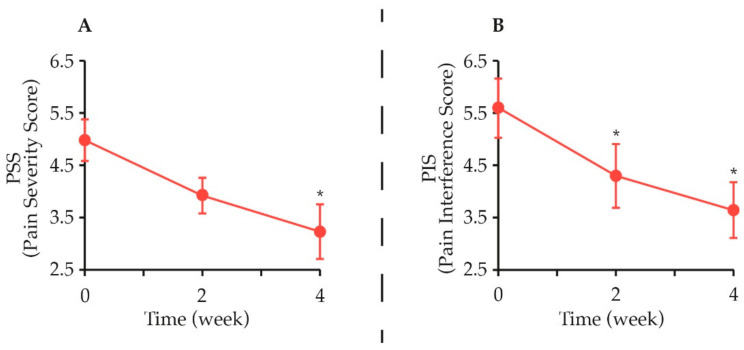
The second study is an open-field trial performed in 13 medium-to-large-breed client-owned adult dogs, with chronic OA and persistent lameness longer than one month. All dogs were supplemented for 4 weeks with a complementary feed containing PEA co-ultramicronized with the natural antioxidant quercetin (i.e., PEA-q, 24 mg/kg body weight). The Canine Brief Pain Inventory (CBPI) questionnaire was used to assess the severity of chronic pain (PSS, Pain Severity Score) and how it interfered with the dog’s normal functioning (PIS, Pain Interference Score). With success defined as a reduction of ≥1 in PSS and PIS, treatment was classified as successful in 54.5% dogs as early as week 2 and CBPI scores significantly decreased throughout the study (Figure 7). Moreover, lameness (either scored by the veterinarian on a 0–4 clinical scale or objectively assessed through a dynamic gait analysis) was found to significantly improve during the treatment period [ref. 265].
The findings of the trials summarized above provide clinical evidence on PEA-um (eventually co-micronized with quercetin) as a promising treatment option for chronic pain and related functional disability in horses, as well as dogs.
10. Conclusions
The management of chronic pain is the burden of veterinary practitioners. Multiple pharmacological agents have been employed to treat diverse pathological pain states, including opiates, NSAIDs, anticonvulsants, antidepressants, and others [ref. 29]. However, adverse effects could limit dosing and therapeutic efficacy [ref. 163,ref. 164].
The recent understanding of the role of non-neuronal cells in pain processing is uncovering potential new targets for managing chronic pain [ref. 104]. Furthermore, it is becoming increasingly clear that enhancing endocannabinoid signalling may prevent patients from developing persistent or chronic pain states mainly through non-neuronal cell modulation [ref. 266,ref. 267,ref. 268,ref. 269]. One such strategy is the dietetic use of the endocannabinoid-like PEA in bioavailable formulations (i.e., micro-PEA). As reviewed here, there is now strong evidence supporting the dietary supplementation with micro-PEA (either as alternative or add-on to conventional treatment) in the management of chronic pain. Such a critical mass of data is being generated that PEA is currently listed among the novel nonopioid interventions to chronic pain [ref. 270].
Although clinical studies in veterinary patients are warranted, the reviewed findings lay the foundations for a scientific and rational use of micro-PEA in the dietary management of chronic pain in dogs and cats.
References
- S.N. Raja, D.B. Carr, M. Cohen, N.B. Finnerup, H. Flor, S. Gibson, F.J. Keefe, J.S. Mogil, M. Ringkamp, K.A. Sluka. The Revised International Association for the Study of Pain Definition of Pain: Concepts, Challenges, and Compromises. Pain, 2020. [DOI | PubMed]
- M.L. Wiseman-Orr, E.M. Scott, J. Reid, A.M. Nolan. Validation of a Structured Questionnaire as an Instrument to Measure Chronic Pain in Dogs on the Basis of Effects on Health-Related Quality of Life. Am. J. Vet. Res., 2006. [DOI | PubMed]
- A. Tomas, D.J. Marcellin-Little, S.C. Roe, A. Motsinger-Reif, B.D.X. Lascelles. Relationship between Mechanical Thresholds and Limb Use in Dogs with Coxofemoral Joint Oa-Associated Pain and the Modulating Effects of Pain Alleviation from Total Hip Replacement on Mechanical Thresholds. Vet. Surg. VS, 2014. [DOI | PubMed]
- P.V. Steagall, B.P. Monteiro, H.L.M. Ruel, G. Beauchamp, G. Luca, J. Berry, S. Little, E. Stiles, S. Hamilton, D. Pang. Perceptions and Opinions of Canadian Pet Owners about Anaesthesia, Pain and Surgery in Small Animals. J. Small Anim. Pract., 2017. [DOI | PubMed]
- K.N. Davis, P.W. Hellyer, E.C.J. Carr, J.E. Wallace, L.R. Kogan. Qualitative Study of Owner Perceptions of Chronic Pain in Their Dogs. J. Am. Vet. Med. Assoc., 2019. [DOI | PubMed]
- D.S. Mills, I. Demontigny-Bédard, M. Gruen, M.P. Klinck, K.J. McPeake, A.M. Barcelos, L. Hewison, H. Van Haevermaet, S. Denenberg, H. Hauser. Pain and Problem Behavior in Cats and Dogs. Amimals, 2020. [DOI]
- S.M. Fox. Chronic Pain in Small Animal Medicine, 2018
- C.M. Morton, J. Reid, E.M. Scott, L.L. Holton, A.M. Nolan. Application of a Scaling Model to Establish and Validate an Interval Level Pain Scale for Assessment of Acute Pain in Dogs. Am. J. Vet. Res., 2005. [DOI | PubMed]
- M.B. Walton, E. Cowderoy, D. Lascelles, J.F. Innes. Evaluation of Construct and Criterion Validity for the “Liverpool Osteoarthritis in Dogs” (LOAD) Clinical Metrology Instrument and Comparison to Two Other Instruments. PLoS ONE, 2013. [DOI | PubMed]
- M. Freire, D. Knazovicky, B. Case, A. Thomson, B.D.X. Lascelles. Comparison of Thermal and Mechanical Quantitative Sensory Testing in Client-Owned Dogs with Chronic Naturally Occurring Pain and Normal Dogs. Vet. J. Lond. Engl. 1997, 2016. [DOI]
- L.K. Harris, H.R. Whay, J.C. Murrell. An Investigation of Mechanical Nociceptive Thresholds in Dogs with Hind Limb Joint Pain Compared to Healthy Control Dogs. Vet. J. Lond. Engl. 1997, 2018. [DOI]
- E.H. Hofmeister, M. Barletta, M. Shepard, B.M. Brainard, C.M. Trim, J. Quandt. Agreement among Anesthesiologists Regarding Postoperative Pain Assessment in Dogs. Vet. Anaesth. Analg., 2018. [DOI | PubMed]
- J. Hunt, D. Knazovicky, B.D.X. Lascelles, J. Murrell. Quantitative Sensory Testing in Dogs with Painful Disease: A Window to Pain Mechanisms?. Vet. J. Lond. Engl. 1997, 2019. [DOI | PubMed]
- B.D.X. Lascelles, D.C. Brown, M. Conzemius, M. Gill, M.L. Oshinsky, M. Sharkey. Measurement of Chronic Pain in Companion Animals: Priorities for Future Research and Development Based on Discussions from the Pain in Animals Workshop (PAW) 2017. Vet. J. Lond. Engl. 1997, 2019. [DOI | PubMed]
- G. Della Rocca, E. Olivieri, A. Di Salvo, J. Malvisi, M. Gogny. Attitude and Concern of Italian Veterinary Practitioners toward Management of Pain in Dogs and Cats. J. Vet. Pharmacol. Ther., 2009
- A. Catanzaro, A. Di Salvo, P.V. Steagall, D. Zampini, A. Polisca, G. Della Rocca. Preliminary Study on Attitudes, Opinions and Knowledge of Italian Veterinarians with Regard to Abdominal Visceral Pain in Dogs. Vet. Anaesth. Analg., 2016. [DOI | PubMed]
- C. Bradbrook, L. Clark. State of the Art Analgesia-Recent Developments Pharmacological Approaches to Acute Pain Management in Dogs and Cats: Part 2. Vet. J. Lond. Engl. 1997, 2018. [DOI]
- A. Baker-Meuten, T. Wendland, S.K. Shamir, A.M. Hess, F.M. Duerr. Evaluation of Acupuncture for the Treatment of Pain Associated with Naturally-Occurring Osteoarthritis in Dogs: A Prospective, Randomized, Placebo-Controlled, Blinded Clinical Trial. BMC Vet. Res., 2020. [DOI | PubMed]
- D.C. Brown, R.C. Boston, J.T. Farrar. Comparison of Force Plate Gait Analysis and Owner Assessment of Pain Using the Canine Brief Pain Inventory in Dogs with Osteoarthritis. J. Vet. Intern. Med., 2013. [DOI | PubMed]
- D.C. Brown, R.C. Boston, J.C. Coyne, J.T. Farrar. Ability of the Canine Brief Pain Inventory to Detect Response to Treatment in Dogs with Osteoarthritis. J. Am. Vet. Med. Assoc., 2008. [DOI | PubMed]
- A.K. Hielm-Björkman, H. Rita, R.-M. Tulamo. Psychometric Testing of the Helsinki Chronic Pain Index by Completion of a Questionnaire in Finnish by Owners of Dogs with Chronic Signs of Pain Caused by Osteoarthritis. Am. J. Vet. Res., 2009. [DOI | PubMed]
- J. Reid, A.M. Nolan, E.M. Scott. Measuring Pain in Dogs and Cats Using Structured Behavioural Observation. Vet. J. Lond. Engl. 1997, 2018. [DOI]
- Z. Belshaw, J. Yeates. Assessment of Quality of Life and Chronic Pain in Dogs. Vet. J. Lond. Engl. 1997, 2018. [DOI]
- I. Hernandez-Avalos, D. Mota-Rojas, P. Mora-Medina, J. Martínez-Burnes, A. Casas Alvarado, A. Verduzco-Mendoza, K. Lezama-García, A. Olmos-Hernandez. Review of Different Methods Used for Clinical Recognition and Assessment of Pain in Dogs and Cats. Int. J. Vet. Sci. Med., 2019. [DOI | PubMed]
- M. Enomoto, B.D.X. Lascelles, M.E. Gruen. Development of a Checklist for the Detection of Degenerative Joint Disease-Associated Pain in Cats. J. Feline Med. Surg., 2020. [DOI | PubMed]
- M.C. Evangelista, R. Watanabe, V.S.Y. Leung, B.P. Monteiro, E. O’Toole, D.S.J. Pang, P.V. Steagall. Facial Expressions of Pain in Cats: The Development and Validation of a Feline Grimace Scale. Sci. Rep., 2019. [DOI | PubMed]
- M. Epstein, I. Rodan, G. Griffenhagen, J. Kadrlik, M. Petty, S. Robertson, W. Simpson. 2015 AAHA/AAFP Pain Management Guidelines for Dogs and Cats. J. Am. Anim. Hosp. Assoc., 2015. [DOI | PubMed]
- K. Mathews, P.W. Kronen, D. Lascelles, A. Nolan, S. Robertson, P.V. Steagall, B. Wright, K. Yamashita. Guidelines for Recognition, Assessment and Treatment of Pain: WSAVA Global Pain Council Members and Co-Authors of This Document. J. Small Anim. Pract., 2014. [DOI | PubMed]
- G. Della Rocca, A. Bufalari. Terapia del Dolore Negli Animali da Compagnia, 2016
- D. Gamba. Il Dolore nel Cane. Valutazione, Diagnosi e Trattamento, 2020
- S.M. Fox. Multimodal Management of Canine Osteoarthritis, 2017
- L.M. Fry, S.M. Neary, J. Sharrock, J.K. Rychel. Acupuncture for Analgesia in Veterinary Medicine. Top. Companion Anim. Med., 2014. [DOI | PubMed]
- D.M. Lane, S.A. Hill. Effectiveness of Combined Acupuncture and Manual Therapy Relative to No Treatment for Canine Musculoskeletal Pain. Can. Vet. J., 2016. [PubMed]
- R. Gupta, A. Srivastava, R. Lall. Nutraceuticals in Veterinary Medicine, 2019
- J.-M. Vandeweerd, C. Coisnon, P. Clegg, C. Cambier, A. Pierson, F. Hontoir, C. Saegerman, P. Gustin, S. Buczinski. Systematic Review of Efficacy of Nutraceuticals to Alleviate Clinical Signs of Osteoarthritis. J. Vet. Intern. Med., 2012. [DOI | PubMed]
- A. Kilaru, E.B. Blancaflor, B.J. Venables, S. Tripathy, K.S. Mysore, K.D. Chapman. The N-Acylethanolamine-Mediated Regulatory Pathway in Plants. Chem. Biodivers., 2007. [DOI | PubMed]
- B.J. Venables, C.A. Waggoner, K.D. Chapman. N-Acylethanolamines in Seeds of Selected Legumes. Phytochemistry, 2005. [DOI | PubMed]
- K.D. Chapman. Occurrence, Metabolism, and Prospective Functions of N-Acylethanolamines in Plants. Prog. Lipid Res., 2004. [DOI | PubMed]
- L. De Luca, R. Ferracane, P. Vitaglione. Food Database of N-Acyl-Phosphatidylethanolamines, N-Acylethanolamines and Endocannabinoids and Daily Intake from a Western, a Mediterranean and a Vegetarian Diet. Food Chem., 2019. [DOI | PubMed]
- T.A. Diep, A.N. Madsen, B. Holst, M.M. Kristiansen, N. Wellner, S.H. Hansen, H.S. Hansen. Dietary Fat Decreases Intestinal Levels of the Anorectic Lipids through a Fat Sensor. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol., 2011. [DOI | PubMed]
- S. Lacroix, F. Pechereau, N. Leblanc, B. Boubertakh, A. Houde, C. Martin, N. Flamand, C. Silvestri, F. Raymond, V. Di Marzo. Rapid and Concomitant Gut Microbiota and Endocannabinoidome Response to Diet-Induced Obesity in Mice. mSystems, 2019. [DOI]
- L. Lin, T. Rideout, N. Yurkova, H. Yang, P. Eck, P.J.H. Jones. Fatty Acid Ethanolamides Modulate CD36-MRNA through Dietary Fatty Acid Manipulation in Syrian Golden Hamsters. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab., 2013. [DOI]
- K. Kleberg, H.A. Hassing, H.S. Hansen. Classical Endocannabinoid-like Compounds and Their Regulation by Nutrients. BioFactors Oxf. Engl., 2014. [DOI | PubMed]
- G. Carta, E. Murru, R. Vargiu, M. Collu, M. Carta, S. Banni, R. Stancampiano. Essential Fatty Acids Deficient Diet Modulates N-Acylethanolamide Profile in Rat’s Tissues. Prostaglandins Leukot. Essent. Fatty Acids, 2020. [DOI | PubMed]
- A. Artmann, G. Petersen, L.I. Hellgren, J. Boberg, C. Skonberg, C. Nellemann, S.H. Hansen, H.S. Hansen. Influence of Dietary Fatty Acids on Endocannabinoid and N-Acylethanolamine Levels in Rat Brain, Liver and Small Intestine. Biochim. Biophys. Acta, 2008. [DOI | PubMed]
- E. Gugliandolo, A.F. Peritore, C. Piras, S. Cuzzocrea, R. Crupi. Palmitoylethanolamide and Related ALIAmides: Prohomeostatic Lipid Compounds for Animal Health and Wellbeing. Vet. Sci., 2020. [DOI]
- D.E. Epps, P.C. Schmid, V. Natarajan, H.H. Schmid. N-Acylethanolamine Accumulation in Infarcted Myocardium. Biochem. Biophys. Res. Commun., 1979. [DOI | PubMed]
- V. Natarajan, P.C. Schmid, P.V. Reddy, M.L. Zuzarte-Augustin, H.H. Schmid. Biosynthesis of N-Acylethanolamine Phospholipids by Dog Brain Preparations. J. Neurochem., 1983. [DOI | PubMed]
- V. Natarajan, P.C. Schmid, P.V. Reddy, H.H. Schmid. Catabolism of N-Acylethanolamine Phospholipids by Dog Brain Preparations. J. Neurochem., 1984. [DOI | PubMed]
- G. Re, R. Barbero, A. Miolo, V. Di Marzo. Palmitoylethanolamide, Endocannabinoids and Related Cannabimimetic Compounds in Protection against Tissue Inflammation and Pain: Potential Use in Companion Animals. Vet. J. Lond. Engl. 1997, 2007. [DOI | PubMed]
- S. Petrosino, A. Schiano Moriello. Palmitoylethanolamide: A Nutritional Approach to Keep Neuroinflammation within Physiological Boundaries-A Systematic Review. Int. J. Mol. Sci., 2020. [DOI | PubMed]
- S. Petrosino, V. Di Marzo. The Pharmacology of Palmitoylethanolamide and First Data on the Therapeutic Efficacy of Some of Its New Formulations. Br. J. Pharmacol., 2017. [DOI | PubMed]
- A.F. Peritore, R. Siracusa, R. Crupi, S. Cuzzocrea. Therapeutic Efficacy of Palmitoylethanolamide and Its New Formulations in Synergy with Different Antioxidant Molecules Present in Diets. Nutrients, 2019. [DOI]
- C.J. Woolf. American College of Physicians; American Physiological Society. Pain: Moving from Symptom Control toward Mechanism-Specific Pharmacologic Management. Ann. Intern. Med., 2004. [DOI | PubMed]
- B.P. Monteiro, C. Otis, J.R.E. Del Castillo, R. Nitulescu, K. Brown, L. Arendt-Nielsen, E. Troncy. Quantitative Sensory Testing in Feline Osteoarthritic Pain—A Systematic Review and Meta-Analysis. Osteoarthr. Cartil., 2020. [DOI]
- G. Orlandini. Orlandini, La Semeiotica Del Dolore, 2016
- D. Elieh Ali Komi, S. Wöhrl, L. Bielory. Mast Cell Biology at Molecular Level: A Comprehensive Review. Clin. Rev. Allergy Immunol., 2020. [DOI | PubMed]
- S.J. Galli, N. Gaudenzio, M. Tsai. Mast Cells in Inflammation and Disease: Recent Progress and Ongoing Concerns. Annu. Rev. Immunol., 2020. [DOI | PubMed]
- G. Chen, Y.-Q. Zhang, Y.J. Qadri, C.N. Serhan, R.-R. Ji. Microglia in Pain: Detrimental and Protective Roles in Pathogenesis and Resolution of Pain. Neuron, 2018. [DOI | PubMed]
- R.-D. Gosselin, M.R. Suter, R.-R. Ji, I. Decosterd. Glial Cells and Chronic Pain. Neurosci. Rev. J. Bringing Neurobiol. Neurol. Psychiatry, 2010. [DOI | PubMed]
- J. Bienenstock, G. MacQueen, P. Sestini, J.S. Marshall, R.H. Stead, M.H. Perdue. Mast Cell/Nerve Interactions in Vitro and in Vivo. Am. Rev. Respir. Dis., 1991. [DOI | PubMed]
- Y. Zuo, N.M. Perkins, D.J. Tracey, C.L. Geczy. Inflammation and Hyperalgesia Induced by Nerve Injury in the Rat: A Key Role of Mast Cells. Pain, 2003. [DOI | PubMed]
- H. Xu, X. Shi, X. Li, J. Zou, C. Zhou, W. Liu, H. Shao, H. Chen, L. Shi. Neurotransmitter and Neuropeptide Regulation of Mast Cell Function: A Systematic Review. J. Neuroinflamm., 2020. [DOI]
- S.D. Skaper, L. Facci, M. Zusso, P. Giusti. An Inflammation-Centric View of Neurological Disease: Beyond the Neuron. Front. Cell. Neurosci., 2018. [DOI | PubMed]
- S. Marinelli, B. Basilico, M.C. Marrone, D. Ragozzino. Microglia-Neuron Crosstalk: Signaling Mechanism and Control of Synaptic Transmission. Semin. Cell Dev. Biol., 2019. [DOI | PubMed]
- I. Matsumoto, Y. Inoue, T. Shimada, T. Aikawa. Brain Mast Cells Act as an Immune Gate to the Hypothalamic-Pituitary-Adrenal Axis in Dogs. J. Exp. Med., 2001. [DOI | PubMed]
- T.L. Yaksh, J.W. Allen, S.L. Veesart, K.A. Horais, S.A. Malkmus, M. Scadeng, J.J. Steinauer, S.S. Rossi. Role of Meningeal Mast Cells in Intrathecal Morphine-Evoked Granuloma Formation. Anesthesiology, 2013. [DOI | PubMed]
- J.K. Sandhu, M. Kulka. Decoding Mast Cell-Microglia Communication in Neurodegenerative Diseases. Int. J. Mol. Sci., 2021. [DOI | PubMed]
- D.P. Green, N. Limjunyawong, N. Gour, P. Pundir, X. Dong. A Mast-Cell-Specific Receptor Mediates Neurogenic Inflammation and Pain. Neuron, 2019. [DOI | PubMed]
- J. Kalesnikoff, S.J. Galli. New Developments in Mast Cell Biology. Nat. Immunol., 2008. [DOI | PubMed]
- R. Silver, J.P. Curley. Mast Cells on the Mind: New Insights and Opportunities. Trends Neurosci., 2013. [DOI | PubMed]
- J. Pastwińska, P. Żelechowska, A. Walczak-Drzewiecka, E. Brzezińska-Błaszczyk, J. Dastych. The Art of Mast Cell Adhesion. Cells, 2020. [DOI]
- V. Coraggio, F. Guida, S. Boccella, M. Scafuro, S. Paino, D. Romano, S. Maione, L. Luongo. Neuroimmune-Driven Neuropathic Pain Establishment: A Focus on Gender Differences. Int. J. Mol. Sci., 2018. [DOI]
- H. Zhao, A. Alam, Q. Chen, M.A. Eusman, A. Pal, S. Eguchi, L. Wu, D. Ma. The Role of Microglia in the Pathobiology of Neuropathic Pain Development: What Do We Know?. Br. J. Anaesth., 2017. [DOI | PubMed]
- A. Héron, D. Dubayle. A Focus on Mast Cells and Pain. J. Neuroimmunol., 2013. [DOI | PubMed]
- T. Iuvone, G. Affaitati, D. De Filippis, M. Lopopolo, G. Grassia, D. Lapenna, L. Negro, R. Costantini, M. Vaia, F. Cipollone. Ultramicronized Palmitoylethanolamide Reduces Viscerovisceral Hyperalgesia in a Rat Model of Endometriosis plus Ureteral Calculosis: Role of Mast Cells. Pain, 2016. [DOI | PubMed]
- F. Giancola, U. Volta, R. Repossi, R. Latorre, D. Beeckmans, F. Carbone, K. Van den Houte, F. Bianco, E. Bonora, A. Gori. Mast Cell-Nerve Interactions Correlate with Bloating and Abdominal Pain Severity in Patients with Non-Celiac Gluten/Wheat Sensitivity. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc., 2020. [DOI | PubMed]
- B. Frossi, M. De Carli, A. Calabrò. Coeliac Disease and Mast Cells. Int. J. Mol. Sci., 2019. [DOI | PubMed]
- R.J. Miller, A.-M. Malfait, R.E. Miller. The Innate Immune Response as a Mediator of Osteoarthritis Pain. Osteoarthr. Cartil., 2020. [DOI | PubMed]
- J. Richards, S. Tang, G. Gunsch, P. Sul, M. Wiet, D.C. Flanigan, S.N. Khan, S. Moore, B. Walter, D. Purmessur. Mast Cell/Proteinase Activated Receptor 2 (PAR2) Mediated Interactions in the Pathogenesis of Discogenic Back Pain. Front. Cell. Neurosci., 2019. [DOI | PubMed]
- D. Kempuraj, S. Mentor, R. Thangavel, M.E. Ahmed, G.P. Selvakumar, S.P. Raikwar, I. Dubova, S. Zaheer, S.S. Iyer, A. Zaheer. Mast Cells in Stress, Pain, Blood-Brain Barrier, Neuroinflammation and Alzheimer’s Disease. Front. Cell. Neurosci., 2019. [DOI | PubMed]
- P. Forsythe. Mast Cells in Neuroimmune Interactions. Trends Neurosci., 2019. [DOI | PubMed]
- L. Zhang, J. Song, T. Bai, R. Wang, X. Hou. Sustained Pain Hypersensitivity in the Stressed Colon: Role of Mast Cell-Derived Nerve Growth Factor-Mediated Enteric Synaptic Plasticity. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc., 2018. [DOI]
- K. Gupta, I.T. Harvima. Mast Cell-Neural Interactions Contribute to Pain and Itch. Immunol. Rev., 2018. [DOI | PubMed]
- A. Ioan-Facsinay. Initiating Pain in Osteoarthritis (OA): Is It the Mast Cell?. Osteoarthr. Cartil., 2018. [DOI]
- M.G. Wiet, A. Piscioneri, S.N. Khan, M.N. Ballinger, J.A. Hoyland, D. Purmessur. Mast Cell-Intervertebral Disc Cell Interactions Regulate Inflammation, Catabolism and Angiogenesis in Discogenic Back Pain. Sci. Rep., 2017. [DOI | PubMed]
- G. Kaur, N. Singh, A.S. Jaggi. Mast Cells in Neuropathic Pain: An Increasing Spectrum of Their Involvement in Pathophysiology. Rev. Neurosci., 2017. [DOI | PubMed]
- M. Fusco, S.D. Skaper, S. Coaccioli, G. Varrassi, A. Paladini. Degenerative Joint Diseases and Neuroinflammation. Pain Pract. Off. J. World Inst. Pain, 2017. [DOI | PubMed]
- S.A. Moore. Managing Neuropathic Pain in Dogs. Front. Vet. Sci., 2016. [DOI | PubMed]
- L. Cao, C.D. Palmer, J.T. Malon, J.A. De Leo. Critical Role of Microglial CD40 in the Maintenance of Mechanical Hypersensitivity in a Murine Model of Neuropathic Pain. Eur. J. Immunol., 2009. [DOI | PubMed]
- M. Costigan, J. Scholz, C.J. Woolf. Neuropathic Pain: A Maladaptive Response of the Nervous System to Damage. Annu. Rev. Neurosci., 2009. [DOI | PubMed]
- I. Spitzbarth, P. Bock, V. Haist, V.M. Stein, A. Tipold, K. Wewetzer, W. Baumgärtner, A. Beineke. Prominent Microglial Activation in the Early Proinflammatory Immune Response in Naturally Occurring Canine Spinal Cord Injury. J. Neuropathol. Exp. Neurol., 2011. [DOI | PubMed]
- R. Yamasaki, T. Fujii, B. Wang, K. Masaki, M.A. Kido, M. Yoshida, T. Matsushita, J.-I. Kira. Allergic Inflammation Leads to Neuropathic Pain via Glial Cell Activation. J. Neurosci. Off. J. Soc. Neurosci., 2016. [DOI]
- R.D. Fields. New Culprits in Chronic Pain. Sci. Am., 2009. [DOI | PubMed]
- S.D. Skaper, L. Facci, P. Giusti. Mast Cells, Glia and Neuroinflammation: Partners in Crime?. Immunology, 2014. [DOI | PubMed]
- F. Marchand, M. Perretti, S.B. McMahon. Role of the Immune System in Chronic Pain. Nat. Rev. Neurosci., 2005. [DOI | PubMed]
- R. Ferreira, L. Bernardino. Dual Role of Microglia in Health and Disease: Pushing the Balance toward Repair. Front. Cell. Neurosci., 2015. [DOI | PubMed]
- H. Yuan, X. Zhu, S. Zhou, Q. Chen, X. Zhu, X. Ma, X. He, M. Tian, X. Shi. Role of Mast Cell Activation in Inducing Microglial Cells to Release Neurotrophin. J. Neurosci. Res., 2010. [DOI | PubMed]
- T.C. Theoharides, I. Tsilioni, M. Bawazeer. Mast Cells, Neuroinflammation and Pain in Fibromyalgia Syndrome. Front. Cell. Neurosci., 2019. [DOI | PubMed]
- A. Ellis, D.L.H. Bennett. Neuroinflammation and the Generation of Neuropathic Pain. Br. J. Anaesth., 2013. [DOI | PubMed]
- R.-R. Ji, Z.-Z. Xu, Y.-J. Gao. Emerging Targets in Neuroinflammation-Driven Chronic Pain. Nat. Rev. Drug Discov., 2014. [DOI | PubMed]
- M. Matsuda, Y. Huh, R.-R. Ji. Roles of Inflammation, Neurogenic Inflammation, and Neuroinflammation in Pain. J. Anesth., 2019. [DOI | PubMed]
- V. Chiurchiù, A. Leuti, M. Maccarrone. Bioactive Lipids and Chronic Inflammation: Managing the Fire Within. Front. Immunol., 2018. [DOI | PubMed]
- K. Ren, R. Dubner. Interactions between the Immune and Nervous Systems in Pain. Nat. Med., 2010. [DOI | PubMed]
- S.D. Skaper, L. Facci, M. Barbierato, M. Zusso, G. Bruschetta, D. Impellizzeri, S. Cuzzocrea, P. Giusti. N-Palmitoylethanolamine and Neuroinflammation: A Novel Therapeutic Strategy of Resolution. Mol. Neurobiol., 2015. [DOI | PubMed]
- R. Lerner, D. Pascual Cuadrado, J.M. Post, B. Lutz, L. Bindila. Broad Lipidomic and Transcriptional Changes of Prophylactic PEA Administration in Adult Mice. Front. Neurosci., 2019. [DOI | PubMed]
- A. Paladini, M. Fusco, T. Cenacchi, C. Schievano, A. Piroli, G. Varrassi. Palmitoylethanolamide, a Special Food for Medical Purposes, in the Treatment of Chronic Pain: A Pooled Data Meta-Analysis. Pain Physician, 2016. [PubMed]
- S.D. Skaper, L. Facci, M. Fusco, M.F. Della Valle, M. Zusso, B. Costa, P. Giusti. Palmitoylethanolamide, a Naturally Occurring Disease-Modifying Agent in Neuropathic Pain. Inflammopharmacology, 2014. [DOI | PubMed]
- D. Piomelli, L. Scalvini, Y. Fotio, A. Lodola, G. Spadoni, G. Tarzia, M. Mor. N-Acylethanolamine Acid Amidase (NAAA): Structure, Function, and Inhibition. J. Med. Chem., 2020. [DOI | PubMed]
- D. Piomelli. A Thickening Network of Lipids. Pain, 2012. [DOI | PubMed]
- D. Piomelli, A.G. Hohmann, V. Seybold, B.D. Hammock. A Lipid Gate for the Peripheral Control of Pain. J. Neurosci. Off. J. Soc. Neurosci., 2014. [DOI | PubMed]
- R. D’Amico, D. Impellizzeri, S. Cuzzocrea, R. Di Paola. ALIAmides Update: Palmitoylethanolamide and Its Formulations on Management of Peripheral Neuropathic Pain. Int. J. Mol. Sci., 2020. [DOI | PubMed]
- F. Piscitelli. Chapter 9—Endocannabinoidomics: “Omics” Approaches Applied to Endocannabinoids and Endocannabinoid-Like Mediators. The Endocannabinoidome, 2015. [DOI]
- S. Petrosino, V.D. Marzo. Anandamide and Other Acylethanolamides. Handbook of Neurochemistry and Molecular Neurobiology: Neural Lipids, 2009. [DOI]
- S. Kallendrusch, C. Hobusch, A. Ehrlich, S. Ziebell, N. Ueda, G. Geisslinger, M. Koch, F. Dehghani. Site-Specific and Time-Dependent Activation of the Endocannabinoid System after Transection of Long-Range Projections. PLoS ONE, 2012. [DOI | PubMed]
- L. Aloe, A. Leon, R. Levi-Montalcini. A Proposed Autacoid Mechanism Controlling Mastocyte Behaviour. Agents Actions, 1993. [DOI | PubMed]
- R. Levi-Montalcini, S.D. Skaper, R. Dal Toso, L. Petrelli, A. Leon. Nerve Growth Factor: From Neurotrophin to Neurokine. Trends Neurosci., 1996. [DOI | PubMed]
- T. Bisogno, S. Maurelli, D. Melck, L. De Petrocellis, V. Di Marzo. Biosynthesis, Uptake, and Degradation of Anandamide and Palmitoylethanolamide in Leukocytes. J. Biol. Chem., 1997. [DOI | PubMed]
- G.G. Muccioli, N. Stella. Microglia Produce and Hydrolyze Palmitoylethanolamide. Neuropharmacology, 2008. [DOI | PubMed]
- I. Bettoni, F. Comelli, A. Colombo, P. Bonfanti, B. Costa. Non-Neuronal Cell Modulation Relieves Neuropathic Pain: Efficacy of the Endogenous Lipid Palmitoylethanolamide. CNS Neurol. Disord. Drug Targets, 2013. [DOI | PubMed]
- S.D. Skaper, L. Facci, P. Giusti. Glia and Mast Cells as Targets for Palmitoylethanolamide, an Anti-Inflammatory and Neuroprotective Lipid Mediator. Mol. Neurobiol., 2013. [DOI | PubMed]
- A. Sayd, M. Antón, F. Alén, J.R. Caso, J. Pavón, J.C. Leza, F. Rodríguez de Fonseca, B. García-Bueno, L. Orio. Systemic Administration of Oleoylethanolamide Protects from Neuroinflammation and Anhedonia Induced by LPS in Rats. Int. J. Neuropsychopharmacol., 2014. [DOI | PubMed]
- S.D. Skaper, A. Buriani, R. Dal Toso, L. Petrelli, S. Romanello, L. Facci, A. Leon. The ALIAmide Palmitoylethanolamide and Cannabinoids, but Not Anandamide, Are Protective in a Delayed Postglutamate Paradigm of Excitotoxic Death in Cerebellar Granule Neurons. Proc. Natl. Acad. Sci. USA, 1996. [DOI | PubMed]
- M. Portavella, N. Rodriguez-Espinosa, P. Galeano, E. Blanco, J.I. Romero, M.I. Holubiec, F. Rodriguez de Fonseca, E. Fernández-Espejo. Oleoylethanolamide and Palmitoylethanolamide Protect Cultured Cortical Neurons Against Hypoxia. Cannabis Cannabinoid Res., 2018. [DOI | PubMed]
- A. Musella, D. Fresegna, F.R. Rizzo, A. Gentile, S. Bullitta, F. De Vito, L. Guadalupi, D. Centonze, G. Mandolesi. A Novel Crosstalk within the Endocannabinoid System Controls GABA Transmission in the Striatum. Sci. Rep., 2017. [DOI | PubMed]
- P. Ambrosino, M.V. Soldovieri, C. Russo, M. Taglialatela. Activation and Desensitization of TRPV1 Channels in Sensory Neurons by the PPARα Agonist Palmitoylethanolamide. Br. J. Pharmacol., 2013. [DOI | PubMed]
- I.A. Khasabova, Y. Xiong, L.G. Coicou, D. Piomelli, V. Seybold. Peroxisome Proliferator-Activated Receptor α Mediates Acute Effects of Palmitoylethanolamide on Sensory Neurons. J. Neurosci. Off. J. Soc. Neurosci., 2012. [DOI]
- M. Koch, S. Kreutz, C. Böttger, A. Benz, E. Maronde, C. Ghadban, H.-W. Korf, F. Dehghani. Palmitoylethanolamide Protects Dentate Gyrus Granule Cells via Peroxisome Proliferator-Activated Receptor-α. Neurotox. Res., 2011. [DOI | PubMed]
- J. LoVerme, R. Russo, G. La Rana, J. Fu, J. Farthing, G. Mattace-Raso, R. Meli, A. Hohmann, A. Calignano, D. Piomelli. Rapid Broad-Spectrum Analgesia through Activation of Peroxisome Proliferator-Activated Receptor-Alpha. J. Pharmacol. Exp. Ther., 2006. [DOI | PubMed]
- D.-S. Im. GPR119 and GPR55 as Receptors for Fatty Acid Ethanolamides, Oleoylethanolamide and Palmitoylethanolamide. Int. J. Mol. Sci., 2021. [DOI | PubMed]
- M.I. Herrera, R. Kölliker-Frers, G. Barreto, E. Blanco, F. Capani. Glial Modulation by N-Acylethanolamides in Brain Injury and Neurodegeneration. Front. Aging Neurosci., 2016. [DOI]
- B.N. Okine, M.K. Madasu, F. McGowan, C. Prendergast, J.C. Gaspar, B. Harhen, M. Roche, D.P. Finn. N-Palmitoylethanolamide in the Anterior Cingulate Cortex Attenuates Inflammatory Pain Behaviour Indirectly via a CB1 Receptor-Mediated Mechanism. Pain, 2016. [DOI | PubMed]
- L. Campora, V. Miragliotta, E. Ricci, L. Cristino, V. Di Marzo, F. Albanese, M. Federica Della Valle, F. Abramo. Cannabinoid Receptor Type 1 and 2 Expression in the Skin of Healthy Dogs and Dogs with Atopic Dermatitis. Am. J. Vet. Res., 2012. [DOI | PubMed]
- V. Miragliotta, P.L. Ricci, F. Albanese, A. Pirone, D. Tognotti, F. Abramo. Cannabinoid Receptor Types 1 and 2 and Peroxisome Proliferator-Activated Receptor-α: Distribution in the Skin of Clinically Healthy Cats and Cats with Hypersensitivity Dermatitis. Vet. Dermatol., 2018. [DOI | PubMed]
- F. Mercati, C. Dall’Aglio, L. Pascucci, C. Boiti, P. Ceccarelli. Identification of Cannabinoid Type 1 Receptor in Dog Hair Follicles. Acta Histochem., 2012. [DOI | PubMed]
- G. Polidoro, G. Galiazzo, F. Giancola, S. Papadimitriou, M. Kouki, S. Sabattini, A. Rigillo, R. Chiocchetti. Expression of Cannabinoid and Cannabinoid-Related Receptors in the Oral Mucosa of Healthy Cats and Cats with Chronic Gingivostomatitis. J. Feline Med. Surg., 2020. [DOI | PubMed]
- A. Stanzani, G. Galiazzo, F. Giancola, C. Tagliavia, M. De Silva, M. Pietra, F. Fracassi, R. Chiocchetti. Localization of Cannabinoid and Cannabinoid Related Receptors in the Cat Gastrointestinal Tract. Histochem. Cell Biol., 2020. [DOI | PubMed]
- G. Rossi, G. Gioacchini, G. Pengo, J.S. Suchodolski, A.E. Jergens, K. Allenspach, A. Gavazza, S. Scarpona, S. Berardi, L. Galosi. Enterocolic Increase of Cannabinoid Receptor Type 1 and Type 2 and Clinical Improvement after Probiotic Administration in Dogs with Chronic Signs of Colonic Dysmotility without Mucosal Inflammatory Changes. Neurogastroenterol. Motil. Off. J. Eur. Gastrointest. Motil. Soc., 2020. [DOI]
- A. Pirone, C. Cantile, V. Miragliotta, C. Lenzi, E. Giannessi, B. Cozzi. Immunohistochemical Distribution of the Cannabinoid Receptor 1 and Fatty Acid Amide Hydrolase in the Dog Claustrum. J. Chem. Neuroanat., 2016. [DOI | PubMed]
- J. Freundt-Revilla, F. Heinrich, A. Zoerner, F. Gesell, M. Beyerbach, M. Shamir, A. Oevermann, W. Baumgärtner, A. Tipold. The Endocannabinoid System in Canine Steroid-Responsive Meningitis-Arteritis and Intraspinal Spirocercosis. PLoS ONE, 2018. [DOI | PubMed]
- J. Freundt-Revilla, K. Kegler, W. Baumgärtner, A. Tipold. Spatial Distribution of Cannabinoid Receptor Type 1 (CB1) in Normal Canine Central and Peripheral Nervous System. PLoS ONE, 2017. [DOI | PubMed]
- M. Fernández-Trapero, F. Espejo-Porras, C. Rodríguez-Cueto, J.R. Coates, C. Pérez-Díaz, E. de Lago, J. Fernández-Ruiz. Upregulation of CB2 Receptors in Reactive Astrocytes in Canine Degenerative Myelopathy, a Disease Model of Amyotrophic Lateral Sclerosis. Dis. Model. Mech., 2017. [DOI | PubMed]
- R. Chiocchetti, G. Galiazzo, C. Tagliavia, A. Stanzani, F. Giancola, M. Menchetti, G. Militerno, C. Bernardini, M. Forni, L. Mandrioli. Cellular Distribution of Canonical and Putative Cannabinoid Receptors in Canine Cervical Dorsal Root Ganglia. Front. Vet. Sci., 2019. [DOI | PubMed]
- A. Calignano, G. La Rana, A. Giuffrida, D. Piomelli. Control of Pain Initiation by Endogenous Cannabinoids. Nature, 1998. [DOI | PubMed]
- D. Piomelli, O. Sasso. Peripheral Gating of Pain Signals by Endogenous Lipid Mediators. Nat. Neurosci., 2014. [DOI | PubMed]
- A.M. Habib, A.L. Okorokov, M.N. Hill, J.T. Bras, M.-C. Lee, S. Li, S.J. Gossage, M. van Drimmelen, M. Morena, H. Houlden. Microdeletion in a FAAH Pseudogene Identified in a Patient with High Anandamide Concentrations and Pain Insensitivity. Br. J. Anaesth., 2019. [DOI | PubMed]
- D. Adrian, M. Papich, R. Baynes, J. Murrell, B.D.X. Lascelles. Chronic Maladaptive Pain in Cats: A Review of Current and Future Drug Treatment Options. Vet. J., 2017. [DOI | PubMed]
- G. Della Rocca, M.B. Conti. Terapie Palliative E Cure Di Fine Vita In Medicina Veterinaria, 2018
- A.J. Wiese, W.W. Muir, T.E. Wittum. Characteristics of Pain and Response to Analgesic Treatment in Dogs and Cats Examined at a Veterinary Teaching Hospital Emergency Service. J. Am. Vet. Med. Assoc., 2005. [DOI | PubMed]
- W.W. Muir, A.J. Wiese, T.E. Wittum. Prevalence and Characteristics of Pain in Dogs and Cats Examined as Outpatients at a Veterinary Teaching Hospital. J. Am. Vet. Med. Assoc., 2004. [DOI | PubMed]
- M.E. Epstein. Feline Neuropathic Pain. Vet. Clin. N. Am. Small Anim. Pract., 2020. [DOI | PubMed]
- D.G. O’Neill, D.B. Church, P.D. McGreevy, P.C. Thomson, D.C. Brodbelt. Prevalence of Disorders Recorded in Dogs Attending Primary-Care Veterinary Practices in England. PLoS ONE, 2014. [DOI | PubMed]
- K.L. Anderson, D.G. O’Neill, D.C. Brodbelt, D.B. Church, R.L. Meeson, D. Sargan, J.F. Summers, H. Zulch, L.M. Collins. Prevalence, Duration and Risk Factors for Appendicular Osteoarthritis in a UK Dog Population under Primary Veterinary Care. Sci. Rep., 2018. [DOI | PubMed]
- R.A. Pettitt, A.J. German. Investigation and Management of Canine Osteoarthritis. Practice, 2015. [DOI]
- S.A. Johnston. Osteoarthritis: Joint Anatomy, Physiology, and Pathobiology. Vet. Clin. N. Am. Small Anim. Pract., 1997. [DOI]
- B.D.X. Lascelles, Y.-H. Dong, D.J. Marcellin-Little, A. Thomson, S. Wheeler, M. Correa. Relationship of Orthopedic Examination, Goniometric Measurements, and Radiographic Signs of Degenerative Joint Disease in Cats. BMC Vet. Res., 2012. [DOI | PubMed]
- B.D.X. Lascelles, J.B. Henry, J. Brown, I. Robertson, A.T. Sumrell, W. Simpson, S. Wheeler, B.D. Hansen, H. Zamprogno, M. Freire. Cross-Sectional Study of the Prevalence of Radiographic Degenerative Joint Disease in Domesticated Cats. Vet. Surg. VS, 2010. [DOI | PubMed]
- M.E. Gruen, P. White, B. Hare. Do Dog Breeds Differ in Pain Sensitivity? Veterinarians and the Public Believe They Do. PLoS ONE, 2020. [DOI | PubMed]
- G. Della Rocca, A. Catanzaro, A.D. Salvo, M.E. Goldberg. Diagnosis of Pain in Small Companion Animals. Am. J. Anim. Vet. Sci., 2015. [DOI]
- B.P. Monteiro, P.V. Steagall. Chronic Pain in Cats: Recent Advances in Clinical Assessment. J. Feline Med. Surg., 2019. [DOI | PubMed]
- P.D. MacFarlane, A.S. Tute, B. Alderson. Therapeutic Options for the Treatment of Chronic Pain in Dogs. J. Small Anim. Pract., 2014. [DOI | PubMed]
- T. Grubb. Where Do We Go from Here? Future Treatment Strategies for Chronic Pain. Top. Companion Anim. Med., 2010. [DOI | PubMed]
- B.P. Monteiro-Steagall, P.V.M. Steagall, B.D.X. Lascelles. Systematic Review of Nonsteroidal Anti-Inflammatory Drug-Induced Adverse Effects in Dogs. J. Vet. Intern. Med., 2013. [DOI | PubMed]
- B. KuKanich. Outpatient Oral Analgesics in Dogs and Cats beyond Nonsteroidal Antiinflammatory Drugs: An Evidence-Based Approach. Vet. Clin. N. Am. Small Anim. Pract., 2013. [DOI | PubMed]
- T. Grubb, H. Lobprise. Local and Regional Anaesthesia in Dogs and Cats: Overview of Concepts and Drugs (Part 1). Vet. Med. Sci., 2020. [DOI | PubMed]
- M. Goich, A. Bascuñán, P. Faúndez, A. Valdés. Multimodal Analgesia for Treatment of Allodynia and Hyperalgesia after Major Trauma in a Cat. JFMS Open Rep., 2019. [DOI | PubMed]
- T.M. Fan. Pain Management in Veterinary Patients with Cancer. Vet. Clin. N. Am. Small Anim. Pract., 2014. [DOI | PubMed]
- S. Petrosino, M. Cordaro, R. Verde, A. Schiano Moriello, G. Marcolongo, C. Schievano, R. Siracusa, F. Piscitelli, A.F. Peritore, R. Crupi. Oral Ultramicronized Palmitoylethanolamide: Plasma and Tissue Levels and Spinal Anti-Hyperalgesic Effect. Front. Pharmacol., 2018. [DOI | PubMed]
- S. Sareen, G. Mathew, L. Joseph. Improvement in Solubility of Poor Water-Soluble Drugs by Solid Dispersion. Int. J. Pharm. Investig., 2012. [DOI]
- D. Impellizzeri, M. Campolo, R. Di Paola, G. Bruschetta, D. de Stefano, E. Esposito, S. Cuzzocrea. Ultramicronized Palmitoylethanolamide Reduces Inflammation an a Th1-Mediated Model of Colitis. Eur. J. Inflamm., 2015. [DOI]
- E.R. Nestmann. Safety of Micronized Palmitoylethanolamide (MicroPEA): Lack of Toxicity and Genotoxic Potential. Food Sci. Nutr., 2017. [DOI | PubMed]
- D. Impellizzeri, G. Bruschetta, M. Cordaro, R. Crupi, R. Siracusa, E. Esposito, S. Cuzzocrea. Micronized/Ultramicronized Palmitoylethanolamide Displays Superior Oral Efficacy Compared to Nonmicronized Palmitoylethanolamide in a Rat Model of Inflammatory Pain. J. Neuroinflamm., 2014. [DOI]
- A. Al Shoyaib, S.R. Archie, V.T. Karamyan. Intraperitoneal Route of Drug Administration: Should It Be Used in Experimental Animal Studies?. Pharm. Res., 2019. [DOI | PubMed]
- A. Calignano, G. La Rana, D. Piomelli. Antinociceptive Activity of the Endogenous Fatty Acid Amide, Palmitylethanolamide. Eur. J. Pharmacol., 2001. [DOI | PubMed]
- M.L. Bartolucci, I. Marini, F. Bortolotti, D. Impellizzeri, R. Di Paola, G. Bruschetta, R. Crupi, M. Portelli, A. Militi, G. Oteri. Micronized Palmitoylethanolamide Reduces Joint Pain and Glial Cell Activation. Inflamm. Res. Off. J. Eur. Histamine Res. Soc. Al, 2018. [DOI]
- L. Di Cesare Mannelli, F. Corti, L. Micheli, M. Zanardelli, C. Ghelardini. Delay of Morphine Tolerance by Palmitoylethanolamide. BioMed Res. Int., 2015. [DOI | PubMed]
- L. Di Cesare Mannelli, L. Micheli, E. Lucarini, C. Ghelardini. Ultramicronized N-Palmitoylethanolamine Supplementation for Long-Lasting, Low-Dosed Morphine Antinociception. Front. Pharmacol., 2018. [DOI | PubMed]
- A. González-Hernández, G. Martínez-Lorenzana, J. Rodríguez-Jiménez, G. Rojas-Piloni, M. Condés-Lara. Intracisternal Injection of Palmitoylethanolamide Inhibits the Peripheral Nociceptive Evoked Responses of Dorsal Horn Wide Dynamic Range Neurons. J. Neural Transm. Vienna Austria 1996, 2015. [DOI | PubMed]
- S. Mazzari, R. Canella, L. Petrelli, G. Marcolongo, A. Leon. N-(2-Hydroxyethyl)Hexadecanamide Is Orally Active in Reducing Edema Formation and Inflammatory Hyperalgesia by down-Modulating Mast Cell Activation. Eur. J. Pharmacol., 1996. [DOI | PubMed]
- S.I. Jaggar, F.S. Hasnie, S. Sellaturay, A.S. Rice. The Anti-Hyperalgesic Actions of the Cannabinoid Anandamide and the Putative CB2 Receptor Agonist Palmitoylethanolamide in Visceral and Somatic Inflammatory Pain. Pain, 1998. [DOI | PubMed]
- S. Conti, B. Costa, M. Colleoni, D. Parolaro, G. Giagnoni. Antiinflammatory Action of Endocannabinoid Palmitoylethanolamide and the Synthetic Cannabinoid Nabilone in a Model of Acute Inflammation in the Rat. Br. J. Pharmacol., 2002. [DOI | PubMed]
- W.P. Farquhar-Smith, S.I. Jaggar, A.S.C. Rice. Attenuation of Nerve Growth Factor-Induced Visceral Hyperalgesia via Cannabinoid CB(1) and CB(2)-like Receptors. Pain, 2002. [DOI | PubMed]
- G. D’Agostino, G. La Rana, R. Russo, O. Sasso, A. Iacono, E. Esposito, G. Mattace Raso, S. Cuzzocrea, J. Loverme, D. Piomelli. Central Administration of Palmitoylethanolamide Reduces Hyperalgesia in Mice via Inhibition of NF-KappaB Nuclear Signalling in Dorsal Root Ganglia. Eur. J. Pharmacol., 2009. [DOI | PubMed]
- D. De Filippis, L. Luongo, M. Cipriano, E. Palazzo, M.P. Cinelli, V. de Novellis, S. Maione, T. Iuvone. Palmitoylethanolamide Reduces Granuloma-Induced Hyperalgesia by Modulation of Mast Cell Activation in Rats. Mol. Pain, 2011. [DOI | PubMed]
- L. Luongo, F. Guida, S. Boccella, G. Bellini, L. Gatta, F. Rossi, V. de Novellis, S. Maione. Palmitoylethanolamide Reduces Formalin-Induced Neuropathic-like Behaviour through Spinal Glial/Microglial Phenotypical Changes in Mice. CNS Neurol. Disord. Drug Targets, 2013. [DOI | PubMed]
- G. Donvito, I. Bettoni, F. Comelli, A. Colombo, B. Costa. Palmitoylethanolamide Relieves Pain and Preserves Pancreatic Islet Cells in a Murine Model of Diabetes. CNS Neurol. Disord. Drug Targets, 2015. [DOI | PubMed]
- D. Britti, R. Crupi, D. Impellizzeri, E. Gugliandolo, R. Fusco, C. Schievano, V.M. Morittu, M. Evangelista, R. Di Paola, S. Cuzzocrea. A Novel Composite Formulation of Palmitoylethanolamide and Quercetin Decreases Inflammation and Relieves Pain in Inflammatory and Osteoarthritic Pain Models. BMC Vet. Res., 2017. [DOI | PubMed]
- W.P. Farquhar-Smith, A.S. Rice. Administration of Endocannabinoids Prevents a Referred Hyperalgesia Associated with Inflammation of the Urinary Bladder. Anesthesiology, 2001. [DOI | PubMed]
- W.P. Farquhar-Smith, A.S.C. Rice. A Novel Neuroimmune Mechanism in Cannabinoid-Mediated Attenuation of Nerve Growth Factor-Induced Hyperalgesia. Anesthesiology, 2003. [DOI | PubMed]
- V.L. Haller, D.L. Cichewicz, S.P. Welch. Non-Cannabinoid CB1, Non-Cannabinoid CB2 Antinociceptive Effects of Several Novel Compounds in the PPQ Stretch Test in Mice. Eur. J. Pharmacol., 2006. [DOI | PubMed]
- F. Pessina, R. Capasso, F. Borrelli, T. Aveta, L. Buono, G. Valacchi, P. Fiorenzani, V. Di Marzo, P. Orlando, A.A. Izzo. Protective Effect of Palmitoylethanolamide in a Rat Model of Cystitis. J. Urol., 2015. [DOI | PubMed]
- Z. Helyes, J. Németh, M. Thán, K. Bölcskei, E. Pintér, J. Szolcsányi. Inhibitory Effect of Anandamide on Resiniferatoxin-Induced Sensory Neuropeptide Release in Vivo and Neuropathic Hyperalgesia in the Rat. Life Sci., 2003. [DOI | PubMed]
- T. Genovese, E. Esposito, E. Mazzon, R. Di Paola, R. Meli, P. Bramanti, D. Piomelli, A. Calignano, S. Cuzzocrea. Effects of Palmitoylethanolamide on Signaling Pathways Implicated in the Development of Spinal Cord Injury. J. Pharmacol. Exp. Ther., 2008. [DOI | PubMed]
- B. Costa, F. Comelli, I. Bettoni, M. Colleoni, G. Giagnoni. The Endogenous Fatty Acid Amide, Palmitoylethanolamide, Has Anti-Allodynic and Anti-Hyperalgesic Effects in a Murine Model of Neuropathic Pain: Involvement of CB(1), TRPV1 and PPARgamma Receptors and Neurotrophic Factors. Pain, 2008. [DOI | PubMed]
- F. Guida, L. Luongo, F. Marmo, R. Romano, M. Iannotta, F. Napolitano, C. Belardo, I. Marabese, A. D’Aniello, D. De Gregorio. Palmitoylethanolamide Reduces Pain-Related Behaviors and Restores Glutamatergic Synapses Homeostasis in the Medial Prefrontal Cortex of Neuropathic Mice. Mol. Brain, 2015. [DOI | PubMed]
- D. Impellizzeri, A.F. Peritore, M. Cordaro, E. Gugliandolo, R. Siracusa, R. Crupi, R. D’Amico, R. Fusco, M. Evangelista, S. Cuzzocrea. The Neuroprotective Effects of Micronized PEA (PEA-m) Formulation on Diabetic Peripheral Neuropathy in Mice. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol., 2019. [DOI | PubMed]
- A.F. Peritore, R. Siracusa, R. Fusco, E. Gugliandolo, R. D’Amico, M. Cordaro, R. Crupi, T. Genovese, D. Impellizzeri, S. Cuzzocrea. Ultramicronized Palmitoylethanolamide and Paracetamol, a New Association to Relieve Hyperalgesia and Pain in a Sciatic Nerve Injury Model in Rat. Int. J. Mol. Sci., 2020. [DOI | PubMed]
- S. Boccella, I. Marabese, M. Iannotta, C. Belardo, V. Neugebauer, M. Mazzitelli, G. Pieretti, S. Maione, E. Palazzo. Metabotropic Glutamate Receptor 5 and 8 Modulate the Ameliorative Effect of Ultramicronized Palmitoylethanolamide on Cognitive Decline Associated with Neuropathic Pain. Int. J. Mol. Sci., 2019. [DOI | PubMed]
- M. Alsalem, M. Haddad, S.A. Aldossary, H. Kalbouneh, A. Altarifi, S.M. Jaffal, M.A. Abbas, N. Aldaoud, K. El-Salem. Role of Cannabinoid Receptor 1 and the Peroxisome Proliferator-Activated Receptor α in Mediating Anti-Nociceptive Effects of Synthetic Cannabinoids and a Cannabinoid-like Compound. Inflammopharmacology, 2019. [DOI | PubMed]
- F. Guida, S. Boccella, C. Belardo, M. Iannotta, F. Piscitelli, F. De Filippis, S. Paino, F. Ricciardi, D. Siniscalco, I. Marabese. Altered Gut Microbiota and Endocannabinoid System Tone in Vitamin D Deficiency-Mediated Chronic Pain. Brain. Behav. Immun., 2020. [DOI | PubMed]
- A.M. Tagne, Y. Fotio, L. Lin, E. Squire, F. Ahmed, T.I. Rashid, E.K. Azari, D. Piomelli. Palmitoylethanolamide and Hemp Oil Extract Exert Synergistic Anti-Nociceptive Effects in Mouse Models of Acute and Chronic Pain. Pharmacol. Res., 2021. [DOI | PubMed]
- O. Sasso, R. Russo, S. Vitiello, G.M. Raso, G. D’Agostino, A. Iacono, G. La Rana, M. Vallée, S. Cuzzocrea, P.V. Piazza. Implication of Allopregnanolone in the Antinociceptive Effect of N-Palmitoylethanolamide in Acute or Persistent Pain. Pain, 2012. [DOI | PubMed]
- L. Di Cesare Mannelli, G. D’Agostino, A. Pacini, R. Russo, M. Zanardelli, C. Ghelardini, A. Calignano. Palmitoylethanolamide Is a Disease-Modifying Agent in Peripheral Neuropathy: Pain Relief and Neuroprotection Share a PPAR-Alpha-Mediated Mechanism. Mediat. Inflamm., 2013. [DOI]
- F. Guida, S. Boccella, M. Iannotta, D. De Gregorio, C. Giordano, C. Belardo, R. Romano, E. Palazzo, M.A. Scafuro, N. Serra. Palmitoylethanolamide Reduces Neuropsychiatric Behaviors by Restoring Cortical Electrophysiological Activity in a Mouse Model of Mild Traumatic Brain Injury. Front. Pharmacol., 2017. [DOI | PubMed]
- N. Soliman, S. Haroutounian, A.G. Hohmann, E. Krane, J. Liao, M. Macleod, D. Segelcke, C. Sena, J. Thomas, J. Vollert. A Systematic Review and Meta-Analysis of Cannabis-Based Medicines, Cannabinoids and Endocannabinoid System Modulators Tested for Antinociceptive Effects in Animal Models of Injury-Related or Pathological Persistent Pain. Pain, 2021. [DOI | PubMed]
- G. Guida, M. de Martino, A. de Fabiani, L. Canteri, A. Alexandre, G. Vassallo, M. Rogai, F. Lanaia, S. Petrosino. La Palmitoiletanolamida (Normast®) En El Dolor Neuropático Crónico Por Lumbociatalgia de Tipo Compresivo: Estudio Clínico Multicéntrico. Dolor, 2010
- A. Assini, D. Laricchia, R. Pizzo, L. Pandolfini, M. Belletti, M. Colucci, S. Ratto. The Carpal Tunnel Syndrome in Diabetes: Clinical and Electrophysiological Improvement after Treatment with Palmitoylethanolamide. Eur. J. Neurol., 2010. [DOI | PubMed]
- A. Biasiotta, S.L. Cesa, C. Leone, G.D. Stefano, A. Truini, G. Cruccu. 265 Efficacy of Palmitoylethanolamide in Patients with Painful Neuropathy. A Clinical and Neurophysiological Open Study. Preliminary Results. Eur. J. Pain Suppl., 2010. [DOI]
- C. Schifilliti, L. Cucinotta, V. Fedele, C. Ingegnosi, G. Savoca, C. Leotta. Palmitoylethanolamide Reduces the Symptoms of Neuropathic Pain in Diabetic Patients. Shock, 2011. [PubMed]
- A. Assini, D. Laricchia, R. Pizzo. Tunnel Carpale Nel Paziente Diabetico Migliloramento Clinico Ed Elettrofisiologico Dopo Trattamento Con Palmitoiletanolamide. Carpal Tunnel Syndrome in the Diabetic Patient. Clinical and Electrophysiologic Improvement after Treatment with Palmitoylethanolamide. Proceedings of the 34th National Congress AISD—New Frontiers in Pain Medicine
- R. Conigliaro, V. Drago, P.S. Foster, C. Schievano, V. Di Marzo. Use of Palmitoylethanolamide in the Entrapment Neuropathy of the Median in the Wrist. Minerva Med., 2011. [PubMed]
- A. Truini, A. Biasiotta, G. Di Stefano, S. La Cesa, C. Leone, C. Cartoni, V. Federico, M.T. Petrucci, G. Cruccu. Palmitoylethanolamide Restores Myelinated-Fibre Function in Patients with Chemotherapy-Induced Painful Neuropathy. CNS Neurol. Disord. Drug Targets, 2011. [DOI | PubMed]
- C. Schifilliti, L. Cucinotta, V. Fedele, C. Ingegnosi, S. Luca, C. Leotta. Micronized Palmitoylethanolamide Reduces the Symptoms of Neuropathic Pain in Diabetic Patients. Pain Res. Treat., 2014. [DOI | PubMed]
- Z. Alshelh, E.P. Mills, D. Kosanovic, F. Di Pietro, P.M. Macey, E.R. Vickers, L.A. Henderson. Effects of the Glial Modulator Palmitoylethanolamide on Chronic Pain Intensity and Brain Function. J. Pain Res., 2019. [DOI | PubMed]
- G. Ottaviani, K. Rupel, M. Gobbo, A. Poropat, V. Zoi, M. Faraon, R. Di Lenarda, M. Biasotto. Efficacy of Ultramicronized Palmitoylethanolamide in Burning Mouth Syndrome-Affected Patients: A Preliminary Randomized Double-Blind Controlled Trial. Clin. Oral Investig., 2019. [DOI]
- G. Cruccu, G.D. Stefano, P. Marchettini, A. Truini. Micronized Palmitoylethanolamide: A Post Hoc Analysis of a Controlled Study in Patients with Low Back Pain—Sciatica. CNS Neurol. Disord. Drug Targets, 2019. [DOI | PubMed]
- G. Mancardi, M. Infante, E. Capello, M. Sormani, A. Uccelli. La Palmitoiletanolamide Allevia Il Dolore Neuropatico Associato Alla Sclerosi Multipla. Palmitoylethanolamide Relieves Neuropathic Pain Associated with Multiple Sclerosis. Proceedings of the XL Congress of the Italian Society of Neurology
- G. Dalla Volta, P. Zavarize, G.F. Ngonga, D. Carli. Ultramicronized Palmitoylethanolamide Reduces Frequency and Pain Intensity in Migraine. A Pilot Study. Int. J. Neurol. Brain Disord., 2016. [DOI]
- D. Chirchiglia, A. Della Torre, F. Signorelli, G. Volpentesta, G. Guzzi, C.A. Stroscio, F. Deodato, D. Gabriele, A. Lavano. Administration of Palmitoylethanolamide in Combination with Topiramate in the Preventive Treatment of Nummular Headache. Int. Med. Case Rep. J., 2016. [DOI | PubMed]
- R.S. Calabrò, P. Bramanti. Occipital Neuralgia Responding to Palmitoylethanolamide. Headache, 2017. [DOI | PubMed]
- D. Chirchiglia, E. Cione, M.C. Caroleo, M. Wang, G. Di Mizio, N. Faedda, T. Giacolini, S. Siviglia, V. Guidetti, L. Gallelli. Effects of Add-On Ultramicronized N-Palmitol Ethanol Amide in Patients Suffering of Migraine With Aura: A Pilot Study. Front. Neurol., 2018. [DOI | PubMed]
- L. Papetti, G. Sforza, G. Tullo, P. Alaimo di Loro, R. Moavero, F. Ursitti, M.A.N. Ferilli, S. Tarantino, F. Vigevano, M. Valeriani. Tolerability of Palmitoylethanolamide in a Pediatric Population Suffering from Migraine: A Pilot Study. Pain Res. Manag., 2020. [DOI | PubMed]
- I. Marini, M.L. Bartolucci, F. Bortolotti, M.R. Gatto, G.A. Bonetti. Palmitoylethanolamide versus a Nonsteroidal Anti-Inflammatory Drug in the Treatment of Temporomandibular Joint Inflammatory Pain. J. Orofac. Pain, 2012. [PubMed]
- E. Steels, R. Venkatesh, E. Steels, G. Vitetta, L. Vitetta. A Double-Blind Randomized Placebo Controlled Study Assessing Safety, Tolerability and Efficacy of Palmitoylethanolamide for Symptoms of Knee Osteoarthritis. Inflammopharmacology, 2019. [DOI | PubMed]
- I. Sani, Y. Hamza. A Systematic Review on the Effectiveness of Palmitoylethanolamide for the Treatment of Pain in Arthrogenic Temporomandibular Joint Dysfunction and Related Disorders. J. Dent. Maxillofac. Res., 2019. [DOI]
- L. Canteri, S. Petrosino, G. Guida. Reducción Del Consumo de Antiinflamatorios y Analgésicos En El Tratamiento Del Dolor Neuropático Crónico En Pacientes Afectados Por Lumbociatalgia de Tipo Compresivo y En Tratamiento Con Normast® 300 Mg. Dolor, 2010
- P. Desio. Associazione tra pregabalin e palmitoiletanolamide (PEA) per il trattamento del dolore neuropatico. Pathos, 2010
- R.A. Palomba, S. Adiletta, A. Candiello, M. Penimpede, P. Bonaccia, C.J. De Martino. Analgesia multimodale per il dolore cronico: Direttive future e razionale. Multimodal analgesia for chronic pain: Rationale and future directions. Proceedings of the 33rd National Congress of the Italian Association for the Study of Pain (AISD)
- C.M. Dominguez, A.A. Diaz Martin, F.G. Ferrer. Palmitoiletanolamida (PEA) En Lumbociatica En Asociacion al Tratamiento Habitual. Palmitoylethanolamide in Lumbosciatic Pain in Association with Standard Therapy. Proceedings of the 8th National Congress of the Sociedad Española Del Dolor
- P. Desio. Associazione Dell’ossicodone a Lenta Titolazione Con Palmitoiletanolamide per Il Trattamento Del Low Back Pain. Anest. E Med. Crit. AMC, 2011
- A. Di Paolo, V. Gianfelice, C. Silvestri. La Palmitoiletanolamide Nel Trattamento Del Dolore Attivato Dal Sistema Gliale: Nostra Esperienza. Palmitoylethanolamide in the Management of Glia-Activated Pain. Our Experience. Proceedings of the 34th National Congress of the Italian Association for the Study of Pain (AISD)
- S. Adiletta, A. Candiello, D. Arminio, S. Porcaro, M.M. Saporito, R. Palomba. Sinergismo Tra Pregabalin e Palmitoiletanolamide (PEA) Nel Trattamento Della Neuropatia Diabetica. Proceedings of the 34th National Congress of the Italian Association for the Study of Pain (AISD)
- C.M. Domínguez, A.D. Martín, F.G. Ferrer, M.I. Puertas, A.L. Muro, J.M. González, J.P. Prieto, I.R. Taberna. N-Palmitoylethanolamide in the Treatment of Neuropathic Pain Associated with Lumbosciatica. Pain Manag., 2012. [DOI | PubMed]
- A. Gatti, M. Lazzari, V. Gianfelice, A. Di Paolo, E. Sabato, A.F. Sabato. Palmitoylethanolamide in the Treatment of Chronic Pain Caused by Different Etiopathogenesis. Pain Med. Malden Mass, 2012. [DOI]
- D. Cocito, E. Peci, P. Ciaramitaro, A. Merola, L. Lopiano. Short-Term Efficacy of Ultramicronized Palmitoylethanolamide in Peripheral Neuropathic Pain. Pain Res. Treat., 2014. [DOI | PubMed]
- R. Del Giorno, S. Skaper, A. Paladini, G. Varrassi, S. Coaccioli. Palmitoylethanolamide in Fibromyalgia: Results from Prospective and Retrospective Observational Studies. Pain Ther., 2015. [DOI | PubMed]
- P. Desio. Aliamidi e duloxetina nel trattamento del low back pain Aliamides and duloxetina in the treatment of low back pain. Pathos, 2016
- A. Paladini, G. Varrassi, G. Bentivegna, S. Carletti, A. Piroli, S. Coaccioli. Palmitoylethanolamide in the Treatment of Failed Back Surgery Syndrome. Pain Res. Treat., 2017. [DOI | PubMed]
- F. Germini, A. Coerezza, L. Andreinetti, A. Nobili, P.D. Rossi, D. Mari, G. Guyatt, M. Marcucci. N-of-1 Randomized Trials of Ultra-Micronized Palmitoylethanolamide in Older Patients with Chronic Pain. Drugs Aging, 2017. [DOI | PubMed]
- M.B. Passavanti, M. Fiore, P. Sansone, C. Aurilio, V. Pota, M. Barbarisi, D. Fierro, M.C. Pace. The Beneficial Use of Ultramicronized Palmitoylethanolamide as Add-on Therapy to Tapentadol in the Treatment of Low Back Pain: A Pilot Study Comparing Prospective and Retrospective Observational Arms. BMC Anesthesiol., 2017. [DOI | PubMed]
- D. Chirchiglia, P. Chirchiglia, F. Signorelli. Nonsurgical Lumbar Radiculopathies Treated with Ultramicronized Palmitoylethanolamide (UmPEA): A Series of 100 Cases. Neurol. Neurochir. Pol., 2018. [DOI | PubMed]
- D. Chirchiglia, S. Paventi, P. Seminara, E. Cione, L. Gallelli. N-Palmitoyl Ethanol Amide Pharmacological Treatment in Patients With Nonsurgical Lumbar Radiculopathy. J. Clin. Pharmacol., 2018. [DOI | PubMed]
- M. Evangelista, V. Cilli, R. De Vitis, A. Militerno, F. Fanfani. Ultra-Micronized Palmitoylethanolamide Effects on Sleep-Wake Rhythm and Neuropathic Pain Phenotypes in Patients with Carpal Tunnel Syndrome: An Open-Label, Randomized Controlled Study. CNS Neurol. Disord. Drug Targets, 2018. [DOI | PubMed]
- D. Chirchiglia, P. Chirchiglia, R. Marotta, L. Gallelli. Add-on Administration of Ultramicronized Palmitoylethanolamide in the Treatment of New-Onset Burning Mouth Syndrome. Int. Med. Case Rep. J., 2019. [DOI | PubMed]
- D. Scaturro, C. Asaro, L. Lauricella, S. Tomasello, G. Varrassi, G. Letizia Mauro. Combination of Rehabilitative Therapy with Ultramicronized Palmitoylethanolamide for Chronic Low Back Pain: An Observational Study. Pain Ther., 2020. [DOI | PubMed]
- V. Schweiger, A. Martini, P. Bellamoli, K. Donadello, C. Schievano, G.D. Balzo, P. Sarzi-Puttini, M. Parolini, E. Polati. Ultramicronized Palmitoylethanolamide (Um-PEA) as Add-on Treatment in Fibromyalgia Syndrome (FMS): Retrospective Observational Study on 407 Patients. CNS Neurol. Disord. Drug Targets, 2019. [DOI | PubMed]
- M. Parabita, R.M.D. Amore, F. Marinosci, M.G. Matera, A. Izzo, G.A. Russo. Reduction of Post Stroke Spasticity with Palmitoylethanolamide Treatment. Shock, 2011
- I. Marini, M. Cavallaro, M. Bartolucci, A. Alessandri-Bonetti, M. Gatto, M. Cordaro, L. Checchi. Can Celecoxib Enhance Palmitoylethanolamide’s Effect in the Treatment of Temporo-Mandibular Arthralgia in Osteoarthritis Patients?. J. Transl. Sci., 2018. [DOI]
- C. Caltagirone, C. Cisari, C. Schievano, R. Di Paola, M. Cordaro, G. Bruschetta, E. Esposito, S. Cuzzocrea. Co-Ultramicronized Palmitoylethanolamide/Luteolin in the Treatment of Cerebral Ischemia: From Rodent to Man. Transl. Stroke Res., 2016. [DOI | PubMed]
- R. Palomba, M. De Simone, A. Giovannini, P. Bonaccia, D. Pinto. Use of Palmitoylethanolamide (PEA) + Polydatin in the Chronic Pelvic Pain. Proceedings of the 64th National Congress of the Italian Society of Anesthesia, Analgesia and Intensive Care (SIAARTI)
- A. Fulghesu, R. Magnini, S. Mazzella, A. Cappai, A. Orrù, M. Pisu. Treatment of Adolescent Dysmenorrhea by a New Inhibitor of Mast Cells-Induced Infiammation (Palmitoylethanolamide + Trans Polidatin). Proceedings of the 16th World Congress of Pediatric and Adolescent Gynecology
- U. Indraccolo, F. Barbieri. Effect of Palmitoylethanolamide-Polydatin Combination on Chronic Pelvic Pain Associated with Endometriosis: Preliminary Observations. Eur. J. Obstet. Gynecol. Reprod. Biol., 2010. [DOI | PubMed]
- R.S. Calabrò, G. Gervasi, S. Marino, P.N. Mondo, P. Bramanti. Misdiagnosed Chronic Pelvic Pain: Pudendal Neuralgia Responding to a Novel Use of Palmitoylethanolamide. Pain Med. Malden Mass, 2010. [DOI | PubMed]
- L. Cobellis, M.A. Castaldi, V. Giordano, E. Trabucco, P. De Franciscis, M. Torella, N. Colacurci. Effectiveness of the Association Micronized N-Palmitoylethanolamine (PEA)-Transpolydatin in the Treatment of Chronic Pelvic Pain Related to Endometriosis after Laparoscopic Assessment: A Pilot Study. Eur. J. Obstet. Gynecol. Reprod. Biol., 2011. [DOI | PubMed]
- G. Lo Monte, I. Soave, R. Marci. Administration of micronized palmitoylethanolamide (PEA)-transpolydatin in the treatment of chronic pelvic pain in women affected by endometriosis: Preliminary results. Minerva Ginecol., 2013. [PubMed]
- E. Giugliano, E. Cagnazzo, I. Soave, G. Lo Monte, J.M. Wenger, R. Marci. The Adjuvant Use of N-Palmitoylethanolamine and Transpolydatin in the Treatment of Endometriotic Pain. Eur. J. Obstet. Gynecol. Reprod. Biol., 2013. [DOI | PubMed]
- F. Murina, A. Graziottin, R. Felice, G. Radici, C. Tognocchi. Vestibulodynia: Synergy between Palmitoylethanolamide + Transpolydatin and Transcutaneous Electrical Nerve Stimulation. J. Low. Genit. Tract Dis., 2013. [DOI | PubMed]
- E. Tartaglia, M. Armentano, B. Giugliano, T. Sena, P. Giuliano, C. Loffredo, P. Mastrantonio. Effectiveness of the Association N-Palmitoylethanolamine and Transpolydatin in the Treatment of Primary Dysmenorrhea. J. Pediatr. Adolesc. Gynecol., 2015. [DOI | PubMed]
- C. Cremon, V. Stanghellini, M.R. Barbaro, R.F. Cogliandro, L. Bellacosa, J. Santos, M. Vicario, M. Pigrau, C. Alonso Cotoner, B. Lobo. Randomised Clinical Trial: The Analgesic Properties of Dietary Supplementation with Palmitoylethanolamide and Polydatin in Irritable Bowel Syndrome. Aliment. Pharmacol. Ther., 2017. [DOI | PubMed]
- E. Stochino Loi, A. Pontis, V. Cofelice, S. Pirarba, M.F. Fais, A. Daniilidis, I. Melis, A.M. Paoletti, S. Angioni. Effect of Ultramicronized-Palmitoylethanolamide and Co-Micronized Palmitoylethanolamide/Polydatin on Chronic Pelvic Pain and Quality of Life in Endometriosis Patients: An Open-Label Pilot Study. Int. J. Womens Health, 2019. [DOI | PubMed]
- M. Cervigni, L. Nasta, C. Schievano, N. Lampropoulou, E. Ostardo. Micronized Palmitoylethanolamide-Polydatin Reduces the Painful Symptomatology in Patients with Interstitial Cystitis/Bladder Pain Syndrome. BioMed Res. Int., 2019. [DOI | PubMed]
- B.B. Artukoglu, C. Beyer, A. Zuloff-Shani, E. Brener, M.H. Bloch. Efficacy of Palmitoylethanolamide for Pain: A Meta-Analysis. Pain Physician, 2017. [PubMed]
- N.B. Finnerup, N. Attal, S. Haroutounian, E. McNicol, R. Baron, R.H. Dworkin, I. Gilron, M. Haanpää, P. Hansson, T.S. Jensen. Pharmacotherapy for Neuropathic Pain in Adults: A Systematic Review and Meta-Analysis. Lancet Neurol., 2015. [DOI | PubMed]
- E. Gugliandolo, A. Barbagallo, A.F. Peritore, S. Cuzzocrea, R. Crupi. Oral Supplementation with Ultramicronized Palmitoylethanolamide for Joint Disease and Lameness Management in Four Jumping Horses: A Case Report. Amimals, 2020. [DOI]
- A. Vezzoni, F. Crupi, S. Boiocchi, S. Boano. Effect of Palmitoylethanolamide Co-Ultra Micronized with Quercetin in Dogs with Osteoarthritis by Means of Dynamic Gate Analysis and Canine Brief Pain Inventory Questionnaire. Proceedings of the 5th World Veterinary Orthopaedic Congress ESVOT-VOS
- M.S. Alkaitis, C. Solorzano, R.P. Landry, D. Piomelli, J.A. DeLeo, E.A. Romero-Sandoval. Evidence for a Role of Endocannabinoids, Astrocytes and P38 Phosphorylation in the Resolution of Postoperative Pain. PLoS ONE, 2010. [DOI | PubMed]
- R. Guerrero-Alba, P. Barragán-Iglesias, A. González-Hernández, E.E. Valdez-Moráles, V. Granados-Soto, M. Condés-Lara, M.G. Rodríguez, B.A. Marichal-Cancino. Some Prospective Alternatives for Treating Pain: The Endocannabinoid System and Its Putative Receptors GPR18 and GPR55. Front. Pharmacol., 2018. [DOI | PubMed]
- L. Luongo, S. Maione, V. Di Marzo. Endocannabinoids and Neuropathic Pain: Focus on Neuron-Glia and Endocannabinoid-Neurotrophin Interactions. Eur. J. Neurosci., 2014. [DOI | PubMed]
- S. Maione, B. Costa, V. Di Marzo. Endocannabinoids: A Unique Opportunity to Develop Multitarget Analgesics. Pain, 2013. [DOI | PubMed]
- A.D. Kaye, E.M. Cornett, B. Hart, S. Patil, A. Pham, M. Spalitta, K.F. Mancuso. Novel Pharmacological Nonopioid Therapies in Chronic Pain. Curr. Pain Headache Rep., 2018. [DOI | PubMed]