
Psychoactive Substance Use and Its Association with Mental Health Symptomatology Among Latvian Medical Students: A Cross-Sectional Study
Abstract
Medical students are at elevated risk for psychoactive substance use and mental health challenges due to academic pressures and environmental stressors. This study aimed to determine the prevalence and trends of psychoactive substance use among medical students at Riga Stradins University (RSU) and to examine associations with symptoms of anxiety, depression, and resilience to stress. A bilingual, anonymous cross-sectional study was conducted using a SurveyMonkey-hosted questionnaire. The survey included a socio-demographic questionnaire, the Generalized Anxiety Disorder Questionnaire-7 (GAD-7), the Patient Health Questionnaire-9 (PHQ-9), the Brief Resilience Scale (BRS), and the World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (WHO ASSIST V3.1). A total of 559 RSU medical students participated (response rate: 31.8%). Lifetime substance use prevalence was highest for caffeine 98.7%, alcohol 93.9%, tobacco 68.4%, and cannabis 50.9%. High-risk use was noted for tobacco 6.8%, inhalants 4.2%, cocaine 3.6%, and alcohol 1.4%. Significant differences in total substance use were observed by gender (p = 0.006) and depression symptom severity by PHQ-9 (p < 0.001), which were predictors of the total involvement score. The findings suggest that further attention to mental health and substance use patterns among medical students may be beneficial for student well-being and professional development.
Article type: Research Article
Keywords: psychoactive substances, medical students, resilience, anxiety, depression, intervention risk, mental health, medicine students, WHO ASSIST
Affiliations: Faculty of Medicine, Riga Stradiņš University, LV-1046 Riga, Latvia045161@rsu.edu.lv (N.C.);; Department of Psychosomatic Medicine and Psychotherapy, Riga Stradiņš University, LV-1046 Riga, Latvia; Department of Neuromedicine and Neurosciences, Faculty of Medicine and Life Sciences, University of Latvia, LV-1586 Riga, Latvia; Department of Psychiatry and Narcology, Riga Stradiņš University, LV-1005 Riga, Latvia; elmars.rancans@rsu.lv (E.R.); lubova.renemane@rsu.lv (L.R.)
License: © 2025 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.3390/ijerph22121806 | PubMed: 41464440 | PMC: PMC12732645
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (819 KB)
1. Introduction
Psychoactive substance use and associated attitudes among European medical students [ref. 1,ref. 2,ref. 3,ref. 4,ref. 5,ref. 6] and doctors in training are well documented [ref. 7]. The COVID-19 pandemic further intensified this concern, as a growing body of evidence indicates increased psychological distress among medical students [ref. 8,ref. 9,ref. 10]. Despite their medical knowledge, medical students are not immune to engaging in substance use. The demands of pre-clinical education, frequent exposure to human suffering during clinical training, and rigorous professional expectations throughout their careers contribute to elevated levels of psychological distress [ref. 11,ref. 12,ref. 13,ref. 14]. These factors may also erode resilience [ref. 15], which is broadly understood as the ability to bounce back or recover from stress [ref. 16].
A recent meta-analysis estimated anxiety symptom prevalence at 33.8% among medical students [ref. 13], compared with approximately 13% in the general European adult population before COVID-19 [ref. 17]. Similarly, depressive symptoms affect approximately 27.2–28.0% of medical students [ref. 12,ref. 14], far exceeding the 6.5% prevalence reported in the general European population [ref. 18]. Furthermore, inter-country variability has been documented both during and in the aftermath of the COVID-19 pandemic [ref. 18]. Although methodological differences such as sampling techniques persist, these symptom-based comparisons clearly highlight the disproportionate mental health burden among medical students.
Substance use has been documented as a maladaptive coping strategy among medical students and physicians in training [ref. 5,ref. 7,ref. 19,ref. 20]. A systematic review found that 24% of medical students reported risky or harmful alcohol use, with European populations at higher risk, and that 17.2% were current tobacco smokers [ref. 21]. Additional estimates included 11.8% past-month cannabis use, 9.9% past-month sedative use, and 7.7% stimulant use (mainly exam-related) [ref. 21]. Other psychoactive substances, such as cocaine, hallucinogens, and opioids (with the specific exception of Iran), generally remained below 3%. However, inhalant use varied regionally, with approximately 14.3% lifetime inhalant use concentrated in Latin America [ref. 21]. A more recent meta-analysis estimated lifetime cannabis use at 31.4% and past year use at 17.2%, with a singular European study reporting substantially higher rates [ref. 22].
Specific data on the use of stimulants, including for academic performance, is reported in 5.2–47.4% of medical students globally, with large regional variability [ref. 21,ref. 23,ref. 24]. Sedative and tranquilizer use also remains prevalent, with up to 25% of students reporting sedative use [ref. 21]. These trends reflect both recreational experimentation and maladaptive coping behaviors shaped by cultural and socioeconomic factors [ref. 25,ref. 26,ref. 27].
Latvia, a Baltic member state of the European Union (EU), provides internationally aligned and EU-accredited medical education programs within the Bologna framework [ref. 28]. Medical education is primarily delivered by Riga Stradins University (RSU) and the University of Latvia, both offering six-year Medical Doctor (M.D.) programs for domestic and international students, with admission being highly competitive and based on academic performance [ref. 28]. According to Eurostat data from the European Commission, Latvia ranks third among EU member states in the number of medical doctor graduates [ref. 29]. As such, RSU’s medical education program is internationally oriented and supported by global accreditation and certification frameworks [ref. 28,ref. 30].
Research on substance use trends among Latvian medical students is limited, particularly regarding associations with mental health outcomes across different psychoactive substances. These limitations have implications for student well-being and broader public health. Prior research conducted at RSU, while insightful and complementary to the present study, was constrained by a smaller sample size, selective recruitment, and a primary focus on mental health outcomes [ref. 31]. Addressing these knowledge gaps is particularly important, as today’s medical students represent potential future clinicians in a multitude of national and transnational healthcare systems. Consequently, the aim of the present study was to evaluate the relationships between psychoactive substance use, depressive and anxiety symptoms, resilience levels, and relevant sociodemographic factors in this population.
2. Materials and Methods
2.1. Study Design and Sampling
This observational, cross-sectional study was conducted among Latvian and international medical students in the Faculty of Medicine at RSU. A pilot study (n = 29) was carried out using convenience sampling via email invitation and included 14 international and 15 Latvian students from diverse academic disciplines. The pilot aimed to refine the questionnaire regarding clarity, length, usability, technical function, and data privacy based on structured feedback.
Data collection for the main study was conducted between June and October 2024 using SurveyMonkey, an online survey platform compliant with the General Data Protection Regulation (GDPR) and previously used in peer-reviewed healthcare research [ref. 32,ref. 33]. The final survey comprised a sociodemographic section and four standardized instruments: The World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (WHO ASSIST V3.1) for substance use, the Generalized Anxiety Disorder 7 (GAD-7) for anxiety symptoms, the Patient Health Questionnaire 9 (PHQ-9) for depressive symptoms, and the Brief Resilience Scale (BRS) for resilience assessment.
2.2. Inclusion and Exclusion Criteria
All students enrolled in the M.D. program at RSU who demonstrated sufficient proficiency in either Latvian or English were eligible to participate. The M.D. program is a 6-year course comprising 360 European Credit Transfer and Accumulation System (ECTS) credits, corresponding to level 7 of the European Qualifications Framework [ref. 28]. In instances where participants fulfilled the formal eligibility criteria but self-identified as non-eligible, their self-classification was respected, and these responses were excluded from the analytic sample.
2.3. Ethics and Ethical Considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki for research involving human participants. Ethical approval was obtained from the RSU Research Ethics Committee in February 2024 (Document Nr. 2-PEK-4/163/2024). Participation was entirely voluntary and anonymous. Electronic informed consent was obtained prior to the initiation of the online questionnaire, and participants were informed that they could withdraw from the study at any time without penalty.
2.4. Measurement Tools and Procedures
The WHO ASSIST V3.1, developed by the World Health Organization, is a standardized primary care screening instrument comprising eight items that assess both lifetime and recent (past three months) use of ten substance classes: tobacco products, alcohol, cannabis, cocaine, amphetamine-type stimulants (ATS), inhalants, sedatives and sleeping pills (e.g., benzodiazepines), hallucinogens, opioids, and other drugs [ref. 34,ref. 35]. For each substance, a substance-specific involvement (sum of items 2–7) classifies individuals into low, moderate, or high-risk categories, indicating the level of intervention required. An aggregate Total Involvement Score (TIS) can also be derived by summing across all substances. Although the TIS is not applied clinically, it has been used in research contexts [ref. 36]; in this study, it served as the dependent outcome in the regression analysis.
To capture additional psychoactive substances not included in the WHO ASSIST, a appendix (Table A1) was developed to assess lifetime (ever used) and past three-month use. The appendix was administered separately, following completion of the WHO ASSIST, to preserve the integrity of the validated instrument. The appendix included pharmacological classes with specified brand names to facilitate accurate reporting, particularly in relation to variations in legal status and accessibility across countries [ref. 37,ref. 38]. This appendix represented an exploratory adaptation specific to the current study and was not part of the validated WHO ASSIST instrument.
Table A1: Lifetime substance use prevalence, and past-three-month substance use prevalence for supplementary psychoactive substance use.
| Question 1: In Your Life, Which of the Following Substances Have You Ever Used? | |||||
| Examples (pharmacological/brand names as in the original) | No | Yes | |||
| Caffeine | Coffee, tea, energy drinks, etc. | ☐ | ☐ | ||
| Question 1.1: Please answer the following substances, if you have used them as medicine prescribed by a doctor/doctor’s prescription. | |||||
| Antidepressants | Fluoxetine/Prozac, Paroxetine/Paxil, Sertraline/Zoloft, Escitalopram/Cipralex/Lexapro, Trazadone/Desyrel/Oleptro, Bupropion/Wellbutrin/Zyban, etc. | ☐ | ☐ | ||
| Anxiolytics | Alprazolam/Xanax/Niravam, Gabazolamine, Diazepam/Valium, Lorazepam/Ativan, etc. | ☐ | ☐ | ||
| Medicinal stimulants | Amphetamine/Dextroamphetamine/Adderall, Methylphenidate/Concerta,/Ritalin, etc. | ☐ | ☐ | ||
| Other (specify): | ☐ | ☐ | |||
| Question 2: In the past three months, how often have you used the substances you mentioned (first drug, second drug, etc.)? | |||||
| Category | Never | Once or twice | Monthly | Weekly | Daily or almost daily |
| Caffeine (coffee, tea, energy drinks, etc.) | 0 | 2 | 3 | 4 | 6 |
| Antidepressants (Fluoxetine/Prozac, Paroxetine/Paxil, Sertraline/Zoloft, Escitalopram/Cipralex/Lexapro, Trazadone/Desyrel/Oleptro, Bupropion/Wellbutrin/Zyban, etc.) | 0 | 2 | 3 | 4 | 6 |
| Anxiolytics (Alprazolam/Xanax/Niravam, Gabazolamine, Diazepam/Valium, Lorazepam/Ativan, etc.) | 0 | 2 | 3 | 4 | 6 |
| Medicinal stimulants (Amphetamine/Dextroamphetamine/Adderall, Methylphenidate/Concerta/Ritalin, etc.) | 0 | 2 | 3 | 4 | 6 |
| Other (specify): | 0 | 2 | 3 | 4 | 6 |
The appendix substances included caffeine, antidepressants, anxiolytics, and medical stimulants. Excluding caffeine, these represent prescription medications used in the treatment of psychiatric conditions. In this exploratory framework, anxiolytics and antidepressants were assessed, including selective serotonin reuptake inhibitors (SSRIs), serotonin antagonists and reuptake inhibitors (SARIs), and norepinephrine–dopamine reuptake inhibitors (NDRIs). SSRIs are established as first-line pharmacological treatments for anxiety disorders, whereas SARIs and NDRIs are primarily antidepressants with limited evidence for anxiolytic benefit, occasionally prescribed in patients with comorbid depression and anxiety [ref. 39]. Antidepressant use was assessed through self-reported use of SSRIs, SARIs, serotonin–norepinephrine reuptake inhibitors (SNRIs), and NDRIs, reflecting both therapeutic and potential off-label use [ref. 40,ref. 41], while anxiolytic use also included benzodiazepines and γ-aminobutyric acid (GABA) analogs [ref. 39]. Medical stimulant use refers to amphetamine and methylphenidate derivatives, which are increasingly reported among student populations [ref. 42,ref. 43,ref. 44]. Caffeine, the most widely consumed psychoactive substance globally [ref. 45,ref. 46], was included due to its emerging associations with psychiatric symptoms and comorbidities [ref. 47,ref. 48].
The BRS was used to assess participants’ ability to recover from stress, i.e., resilience [ref. 16]. The six-item BRS employs a five-point Likert scale with both positively and negatively worded items, reverse scored as appropriate. Higher mean scores (ranging from 1–5) indicate greater resilience. The six-item BRS has demonstrated good internal consistency and construct validity [ref. 16,ref. 49].
Depressive symptoms were assessed using the PHQ-9, a nine-item validated self-report screening instrument measuring depression symptom severity over the previous two weeks [ref. 50]. The PHQ-9 demonstrated good internal consistency and criterion validity [ref. 50]. The PHQ-9 assesses depression symptomatology on a scale of 0 to 27, where scores of 0 to 4 indicate minimal or no depression, 5 to 9: mild depression, 10 to 14: moderate depression, 15 to 19: moderately severe depression, and ≥20: severe depressive symptoms [ref. 50]. The presence of clinically relevant depressive symptoms was defined using a cut-off score of ≥10 [ref. 50].
Anxiety symptoms were assessed using the GAD-7, a seven-item validated self-report screening instrument evaluating generalized anxiety symptoms over the previous two weeks [ref. 51]. The GAD-7 assesses general anxiety symptomatology on a scale of 0 to 21, where scores of 0 to 4 indicate none to minimal anxiety, 5 to 9: mild anxiety, 10 to 14: moderate anxiety, and ≥15: severe anxiety symptoms [ref. 51]. The GAD-7 demonstrates high internal consistency, and the presence of clinically relevant anxiety symptoms was defined using a cut-off score of ≥10 [ref. 51].
To minimize language bias, participants completed questionnaires in their primary language of medical instruction (Latvian or English).
Validated bilingual versions of the PHQ-9 [ref. 52] and GAD-7 [ref. 53], as well as the registered Latvian adaptation of the BRS [ref. 54], were used. The WHO ASSIST was translated into Latvian by an external bilingual contributor and back-translated into English in collaboration with the authors. This preliminary adaptation was developed for use in the present exploratory study. Sociodemographic data were collected to explore trends related to substance use, and participants were categorized as preclinical (Years 1–3) and clinical (Years 4–6). To standardize reporting of recent psychiatric treatment, a 90-day recall window (≈three months) was applied, reflecting a practical short-term observation period shown to reduce recall bias in healthcare surveys [ref. 55].
2.5. Data Collection Procedure
The required minimum sample size was calculated using Cochran’s formula for sample size estimation based on a 95% confidence level (α = 0.05), resulting in a target sample size of n = 323. Survey invitations and the access link were distributed through the official RSU email system to all students enrolled in the M.D. program.
Additional recruitment was conducted electronically via social media channels, including RSU student associations, WhatsApp groups, Instagram, and semester-specific chat groups using a single survey link. To minimize ineligible or duplicate entries [ref. 32], safeguards included restricting submissions to one per IP address and requiring participants to manually enter their age as an open-ended response for verification.
2.6. Statistical Analysis
Data were screened for entry errors and typographical inconsistencies, and variables were recorded into categorical bins where appropriate. To ensure validity, only fully completed instruments and WHO ASSIST scores were retained for analysis. Missing data were handled using a combined approach. Listwise deletion was applied for all multivariable analyses, consistent with default procedures in IBM SPSS Statistics (version 29.0.2.0). Pairwise deletion was used for descriptive statistics and other bivariate analyses to maximize available data. Descriptive statistics and normality testing were conducted, followed by the application of parametric or nonparametric tests. All tests were two-tailed, with statistical significance set at α = 0.05.
Continuous measures were summarized as mean ± standard deviation (M ± SD) when normally distributed, and as median with interquartile ranges [IQR] when non-normally distributed. Associations between categorical variables were examined using Pearson’s chi-squared test (χ2). Only variables meeting chi-square assumptions (minimum expected cell count ≥ 5) were retained, and results are reported as χ2 and corresponding p-values. Between-group differences in continuous nonparametric variables were assessed using the Mann–Whitney U test (two groups) or the Kruskal–Wallis test (more than two groups). For Mann–Whitney comparisons, Hodges–Lehmann estimators (HL) with 95% confidence intervals (CI) were provided as measures of effect size. When the Kruskal–Wallis test indicated significant omnibus differences, pairwise Mann–Whitney U tests with Bonferroni correction were applied. Parametric comparisons between two independent groups were performed using Welch’s t test, with results reported as t(df), p-values, and 95% confidence intervals for the mean difference (MD).
Predictor variables identified in preliminary analyses and from existing literature were entered into a Generalized Linear Model (GLM). Given the over-dispersed, count-like distribution of the dependent variable (TIS), a negative binomial regression with a log link was applied. Multicollinearity among predictors was examined using Variance Inflation Factors (VIF) and tolerance statistics. Backward elimination, guided by statistical significance (p < 0.05), theoretical considerations, and relative model fit (Akaike’s Information Criterion, AIC), was used to derive a parsimonious final model.
3. Results
3.1. Socio-Demographic Characteristics of the Study Sample
Of the 1,756 medical students actively enrolled during the study period, approximately 31.8% completed the questionnaire (Figure 1). In total, 742 responses were collected. After excluding 183 ineligible or incomplete responses, the final analytic sample comprised 559 medical students. Participants were recruited primarily via RSU email (n = 354, 63.3%), and additionally through a social media link (n = 205, 36.7%).
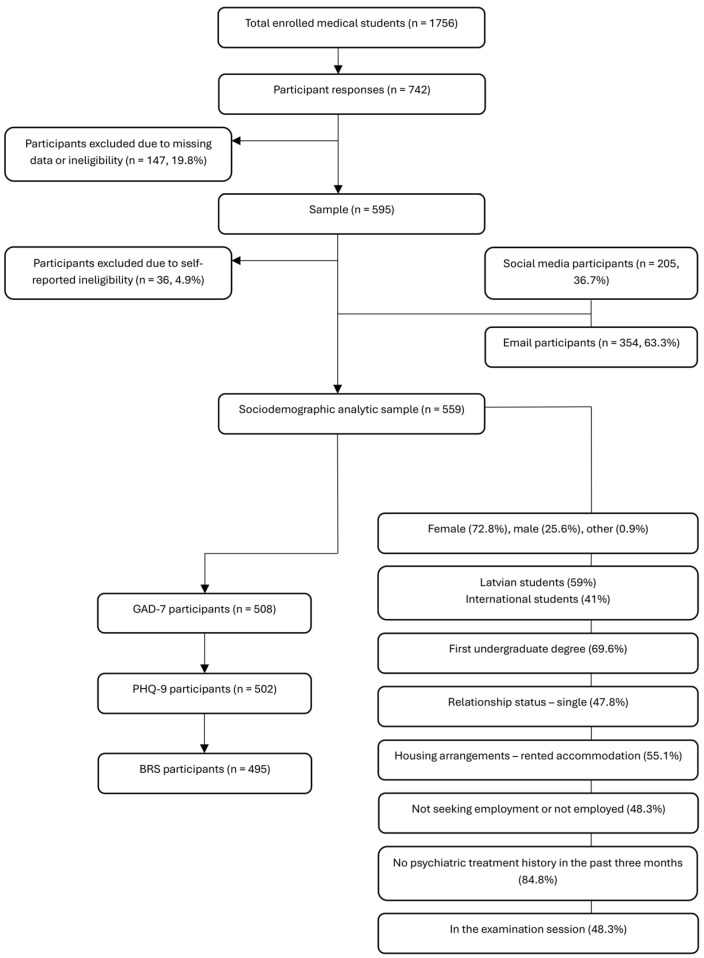
Latvian students represented 59% of participants, while international students accounted for 41%. The sample was predominantly female (72.8%), followed by male (25.6%), and other gender identities (0.9%). The mean age was 22.3 years (SD = 4.1). Nearly half of the participants were first-year students (43.5%), and most were pursuing medicine as their first undergraduate degree (69.6%). Most participants reported having no children (92.7%), 47.8% were single, and 55.1% rented accommodation.
Approximately 48.3% of participants were not employed or seeking work. The most commonly reported combined monthly household income, representing the total income of all household members, excluding grants and loans, was between EUR 2001–EUR 5000 (24.2%). The majority (84.8%) had not accessed mental health care in the past three months. Among those with a treatment history, 10.4% had received psychotherapy alone, while 11.3% reported both psychotherapy and pharmacotherapy.
Data collection was nearly evenly distributed between examination and non-examination periods (48.3% vs. 49.7%). Detailed socio-demographic characteristics of the study sample are presented in Table 1.
Table 1: Sociodemographic profile of medical student participants (n = 559).
| Variables | Categories | M ± SD |
|---|---|---|
| Mean age | 22.3 ± 4.1 | |
| n (%) | ||
| Gender | Male | 143 (25.6) |
| Female | 407 (72.8) | |
| Other | 5 (0.9) | |
| No response | 4 (0.7) | |
| Student origin | International students | 229 (41.0) |
| Latvian students | 330 (59.0) | |
| International student nationality * | German | 64 (27.9) |
| Swedish | 36 (15.7) | |
| Finnish | 23 (10.0) | |
| Italian | 22 (9.6) | |
| Russian | 22 (9.6) | |
| All other nationalities | 62 (27.0) | |
| Academic year | 1 | 243 (43.5) |
| 2 | 60 (10.7) | |
| 3 | 72 (12.9) | |
| 4 | 47 (8.4) | |
| 5 | 81 (14.5) | |
| 6 | 49 (8.8) | |
| No response | 7 (1.3) | |
| Prior education | Attending university but no degree | 389 (69.6) |
| Associate’s degree | 19 (3.4) | |
| Bachelor’s degree | 47 (8.4) | |
| Graduate degree | 69 (12.3) | |
| No response | 35 (6.3) | |
| Marital status | Single | 267 (47.8) |
| In a committed relationship | 250 (44.7) | |
| Married | 26 (4.7) | |
| Separated or widowed | 12 (2.1) | |
| No response | 4 (0.7) | |
| Housing arrangements | Owned | 58 (10.4) |
| Rented | 308 (55.1) | |
| Live with family or partner | 186 (33.3) | |
| No response | 7 (1.3) | |
| Employment status | Employed > 160 h—full-time | 29 (5.2) |
| Employed < 160 h—part-time | 185 (33.1) | |
| Not employed, looking for work | 65 (11.6) | |
| Not employed, not looking for work | 270 (48.3) | |
| No response | 10 (1.8) | |
| Any applicable psychiatric treatment | Pharmacotherapy | 35 (6.3) |
| Psychotherapy | 58 (10.4) | |
| Psychotherapy and pharmacotherapy | 63 (11.3) | |
| Brain stimulation therapy | 1 (0.2) | |
| All other combinations | 3 (0.5) | |
| None | 384 (68.7) | |
| No response | 15 (2.7) | |
| Psychiatric treatment in the last 90 days | Yes | 76 (13.6) |
| No | 474 (84.8) | |
| No response | 9 (1.6) | |
| Children | None | 518 (92.7) |
| One or More | 33 (5.9) | |
| No response | 8 (1.4) | |
| Examination status | In the exam session | 270 (48.3) |
| Not in the exam session | 278 (49.7) | |
| No response | 11 (2.0) | |
| Total monthly income earned by all members of the household, excluding grants and loans | EUR 0–1000 | 105 (18.8) |
| EUR 1001–2000 | 88 (15.7) | |
| EUR 2001–5000 | 135 (24.2) | |
| EUR 5001–10,000 | 45 (8.1) | |
| EUR 10,001–20,000 | 25 (4.5) | |
| EUR 20,001 or more | 27 (4.8) | |
| I do not wish to answer | 127 (22.7) | |
| No response | 7 (1.3) |
Note: Continuous variables are presented as the mean ± standard deviation (M ± SD). Categorical variables are presented as n (%). Percentages may not total 100% due to rounding. * Subcategory calculated from n = 229.
3.1.1. Measurement Instruments (PHQ-9, GAD-7, BRS) and Their Trends
The median scores for the total sample were 10.0 [5.0–15.0] for the GAD-7, and 9.0 [4.8–15.0] for the PHQ-9, while the mean BRS score was 3.25 ± 0.88. Overall, the prevalence of clinically relevant anxiety and depression symptoms (≥10) was 51.0% and 47.5%, respectively (Table 2). Female students reported higher anxiety and depression symptom scores than males. Median GAD-7 scores were 11.0 [7.0–15.0] in females versus 5.0 [3.0–11.0] in males (U = 14,495.50, HL = 4.0, 95% CI [3.0–6.0], p < 0.001). Similarly, median PHQ-9 scores were 10.0 [5.0–15.5] versus 6.0 [3.0–13.0], respectively (U = 17,429.50, HL = 3.0, 95% CI [2.0–4.0], p < 0.001). Gender differences were also evident in categorical symptom distributions for both anxiety (χ2(3) = 53.82, p < 0.001) and depression (χ2(4) = 31.23, p < 0.001). Females were more frequently represented above the clinically relevant symptom threshold for both anxiety and depression compared with males (58.8% vs. 27.7% and 53.2% vs. 32.3%, respectively).
Table 2: Gender differences in anxiety and depression symptoms and resilience scores among participants.
| Instrument | Total Sample | Female | Male | Test Statistic | p |
|---|---|---|---|---|---|
| Continuous scores | |||||
| BRS | 3.25 ± 0.88 (n = 495) | 3.10 ± 0.82 (n = 361) | 3.69 ± 0.92 (n = 127) | t(201.9) = −6.34; MD = −0.59, 95% CI [−0.77–−0.40] | p < 0.001 |
| GAD-7 | 10.0 [5.0–15.0] (n = 508) | 11.0 [7.0–15.0] (n = 371) | 5.0 [3.0–11.0] (n = 130) | U = 14,495.50; HL = 4.0, 95% CI [3.0–6.0] | p < 0.001 |
| PHQ-9 | 9.0 [4.8–15.0] (n = 502) | 10.0 [5.0–15.5] (n = 365) | 6.0 [3.0–13.0] (n = 130) | U = 17,429.50; HL = 3.0, 95% CI [2.0–4.0] | p < 0.001 |
| Categorical classifications | |||||
| BRS categories | (n = 495) | (n = 361) | (n = 127) | ||
| Low resilience (1.00–2.99) | 185 (37.4%) | 151 (41.8%) | 29 (22.8%) | χ2(2) = 48.87 | p < 0.001 |
| Normal resilience (3.00–4.30) | 238 (48.1%) | 180 (49.9%) | 56 (44.1%) | ||
| High resilience (4.31–5.00) | 72 (14.5%) | 30 (8.3%) | 42 (33.1%) | ||
| GAD-7 Scores | (n = 508) | (n = 371) | (n = 130) | ||
| None to minimal (0–4) | 113 (22.2%) | 56 (15.1%) | 57 (43.8%) | χ2(3) = 53.82 | p < 0.001 |
| Mild (5–9) | 136 (26.8%) | 97 (26.1%) | 37 (28.5%) | ||
| Moderate (10–14) | 124 (24.4%) | 106 (28.6%) | 17 (13.1%) | ||
| Severe (15–21) | 135 (26.6%) | 112 (30.2%) | 19 (14.6%) | ||
| PHQ-9 Scores | (n = 502) | (n = 365) | (n = 130) | ||
| None or minimal (0–4) | 125 (24.9%) | 69 (18.9%) | 55 (42.3%) | χ2(4) = 31.23 | p < 0.001 |
| Mild (5–9) | 138 (27.5%) | 102 (27.9%) | 33 (25.4%) | ||
| Moderate (10–14) | 110 (21.9%) | 93 (25.5%) | 17 (13.1%) | ||
| Moderately severe (15–19) | 63 (12.5%) | 51 (14.0%) | 10 (7.7%) | ||
| Severe (20–27) | 66 (13.1%) | 50 (13.7%) | 15 (11.5%) | ||
Note: Data are presented as the mean ± SD, median [IQR], or n (%). Denominators vary due to item-level missing responses (pairwise deletion), and the total sample includes participants with nonbinary or unspecified gender; therefore, subgroup counts may not sum to the total sample. Percentages may not total 100% due to rounding. GAD-7 = Generalized Anxiety Disorder-7; PHQ-9 = Patient Health Questionnaire-9; BRS = Brief Resilience Scale. All p < 0.05.
Resilience scores were significantly lower among females (3.10 ± 0.82) than males (3.69 ± 0.92), t(201.9) = −6.34, p < 0.001, MD = −0.59 (95% CI [−0.77–−0.40]). Categorical analyses supported this difference (χ2(2) = 48.87, p < 0.001), with females more frequently classified as low-resilience (41.8% vs. 22.8%), while males predominated in the high-resilience group (33.1% vs. 8.3%).
Latvian-origin students reported higher anxiety and depression symptom scores compared with international students studying in Latvia. Median GAD-7 scores were 11.0 [7.0–15.0] among Latvian students and 7.0 [4.0–12.5] among international students (U = 39,130.00, HL = −3.0, 95% CI [−4.0–−2.0], p < 0.001; Table 3). Median PHQ-9 scores were also higher among Latvian students (11.0 [6.0–16.0]) compared with international students (7.0 [3.0–12.0]; U = 39,321.50, HL = −3.0, 95% CI [−5.0–−2.0], p < 0.001). Student origin differences were also evident in categorical symptom distributions for both anxiety (χ2(3) = 28.64, p < 0.001) and depression (χ2(4) = 38.41, p < 0.001). Latvian-origin students were more frequently represented above the clinically relevant symptom threshold for both anxiety and depression, compared with international students (57.9% vs. 41.2% and 56.7% vs. 34.9%, respectively). Resilience scores were significantly lower among Latvian origin students (3.03 ± 0.83) than international medical students (3.54 ± 0.87), t(432.2) = −6.45, p < 0.001, MD = −0.50 (95% CI [−0.66–−0.35]). Categorical analyses supported this difference (χ2(2) = 32.63, p < 0.001), with Latvian students more frequently classified as low resilience (45.6% vs. 26.0%), while international students were more often classified as high-resilience (23.6% vs. 8.1%).
Table 3: Differences in anxiety, depression symptoms, and resilience scores between international and Latvian-origin medical students.
| Instrument | Total Sample | International Students | Latvian Students | Test Statistic | p |
|---|---|---|---|---|---|
| Continuous scores | |||||
| BRS | 3.25 ± 0.88 (n = 495) | 3.54 ± 0.87 (n = 208) | 3.03 ± 0.83 (n = 285) | t(432.2) = −6.45; MD = −0.50, 95% CI [−0.66–−0.35] | p < 0.001 |
| GAD-7 | 10.0 [5.0–15.0] (n = 508) | 7.0 [4.0–12.5] (n = 211) | 11.0 [7.0–15.0] (n = 295) | U = 39,130.00; HL = −3.0, 95% CI [−4.0–−2.0] | p < 0.001 |
| PHQ-9 | 9.0 [4.8–15.0] (n = 502) | 7.0 [3.0–12.0] (n = 209) | 11.0 [6.0–16.0] (n = 291) | U = 39,321.50; HL = −3.0, 95% CI [−5.0–−2.0] | p < 0.001 |
| Categorical classifications | |||||
| BRS categories | (n = 495) | (n = 208) | (n = 285) | ||
| Low resilience (1.00–2.99) | 185 (37.4%) | 54 (26.0%) | 130 (45.6%) | χ2(2) = 32.63 | p < 0.001 |
| Normal resilience (3.00–4.30) | 238 (48.1%) | 105 (50.5%) | 132 (46.3%) | ||
| High resilience (4.31–5.00) | 72 (14.5%) | 49 (23.6%) | 23 (8.1%) | ||
| GAD-7 Scores | (n = 508) | (n = 211) | (n = 295) | ||
| None to minimal (0–4) | 113 (22.2%) | 71 (33.6%) | 42 (14.2%) | χ2(3) = 28.64 | p < 0.001 |
| Mild (5–9) | 136 (26.8%) | 53 (25.1%) | 82 (27.8%) | ||
| Moderate (10–14) | 124 (24.4%) | 45 (21.3%) | 78 (26.4%) | ||
| Severe (15–21) | 135 (26.6%) | 42 (19.9%) | 93 (31.5%) | ||
| PHQ-9 Scores | (n = 502) | (n = 209) | (n = 291) | ||
| None or minimal (0–4) | 125 (24.9%) | 80 (38.3%) | 45 (15.5%) | χ2(4) = 38.41 | p < 0.001 |
| Mild (5–9) | 138 (27.5%) | 56 (26.8%) | 81 (27.8%) | ||
| Moderate (10–14) | 110 (21.9%) | 37 (17.7%) | 72 (24.7%) | ||
| Moderately severe (15–19) | 63 (12.5%) | 17 (8.1%) | 46 (15.8%) | ||
| Severe (20–27) | 66 (13.1%) | 19 (9.1%) | 47 (16.2%) | ||
Note: Data are presented as mean ± SD, median [IQR], or n (%). Denominators vary due to item-level missing responses (pairwise deletion), and the total sample includes participants who did not specify student origin; therefore, subgroup counts may not sum to the total sample. Percentages may not total 100% due to rounding. GAD-7 = Generalized Anxiety Disorder-7; PHQ-9 = Patient Health Questionnaire-9; BRS = Brief Resilience Scale. All p < 0.05.
3.1.2. Sociodemographic Factors and PHQ-9 Scores
Pre-clinical students reported higher PHQ-9 scores compared to clinical students (HL = 2.0, 95% CI [1.0–3.0]; U = 22,695.00, p = 0.002; Table 4).
Table 4: Group differences in PHQ-9 scores by year of study (n = 498; pre-clinical n = 333, clinical n = 165).
| Dependent Variable | Independent Variable | Median [IQR] | Test Statistic | p |
|---|---|---|---|---|
| PHQ-9 total score | Clinical year | Pre-clinical: 10.0 [5.0–15.0] Clinical: 7.0 [3.0–14.0] | U = 22,695.00, HL = 2.0, 95% CI [1.0–3.0] | 0.002 |
Note: U = Mann–Whitney U test with Hodges–Lehmann estimator and 95% CI. HL = Hodges–Lehmann estimator; CI = confidence interval. Group values are presented as median [IQR]. PHQ-9 = Patient Health Questionnaire-9. All p < 0.05.
3.2. WHO ASSIST Substance Use Trends
Substance Use and WHO ASSIST Risk Grouping
The most commonly reported psychoactive substances were alcohol, tobacco, and cannabis. Lifetime substance use prevalence was highest for alcohol (93.9%), followed by tobacco (68.4%) and cannabis (50.9%). The corresponding past-three-month prevalence rates were 84.6%, 49.5%, and 19.8%, respectively (Table 5). Among supplementary substances, caffeine was most frequently reported (98.7% lifetime; 97.0% past three months), followed by antidepressants (16.8% lifetime; 8.9% past three months) and anxiolytics (14.7% lifetime; 7.9% past three months).
Table 5: Lifetime substance use prevalence, past-three-month substance use prevalence, and gender differences for psychoactive substance use.
| WHO ASSIST Psychoactive Substance | Lifetime Substance Use Prevalence, n (%) | Past-Three-Month Substance Use Prevalence, n (%) | Male Lifetime Substance Use Prevalence, n (%) | Female Lifetime Substance Use Prevalence,n (%) |
|---|---|---|---|---|
| Alcohol | 505 (93.9%) | 455 (84.6%) | 131 (95.6%) | 367 (93.1%) |
| Tobacco | 379 (68.4%) | 274 (49.5%) | 111 (78.2%) | 264 (65.3%) |
| Cannabis | 270 (50.9%) | 105 (19.8%) | 83 (62.4%) | 185 (47.4%) |
| Cocaine | 56 (10.6%) | 19 (3.6%) | 23 (17.6%) | 32 (8.2%) |
| Amphetamine-type stimulants | 73 (13.9%) | 25 (4.8%) | 34 (26.2%) | 39 (10.1%) |
| Inhalants | 24 (4.6%) | 4 (0.8%) | 14 (10.8%) | 9 (2.3%) |
| Sedatives | 73 (13.9%) | 49 (9.3%) | 19 (14.6%) | 54 (13.9%) |
| Hallucinogens | 55 (10.5%) | 23 (4.4%) | 26 (20.0%) | 29 (7.5%) |
| Opioids | 13 (2.5%) | 9 (1.7%) | 6 (4.6%) | 7 (1.8%) |
| Other | 18 (3.4%) | 12 (2.3%) | 9 (6.9%) | 9 (2.3%) |
| Any non-medical drug by injection | 3 (0.6%) | |||
| Supplementary psychoactive substances | ||||
| Caffeine | 518 (98.7%) | 509 (97.0%) | 128 (98.5%) | 383 (98.7%) |
| Antidepressants | 87 (16.8%) | 46 (8.9%) | 14 (10.8%) | 71 (18.6%) |
| Anxiolytics | 76 (14.7%) | 41 (7.9%) | 18 (13.8%) | 58 (15.3%) |
| Medical stimulants | 49 (9.5%) | 34 (6.6%) | 22 (16.9%) | 27 (7.1%) |
| Other | 21 (4.1%) | 14 (2.7%) | 5 (3.8%) | 16 (4.2%) |
Note: Denominators vary across substances due to item-level missing responses. Percentages reflect item-level response counts. WHO ASSIST = World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test V3.1.
Gender comparisons revealed higher lifetime prevalence of tobacco (78.2% vs. 65.3%) and cannabis (62.4% vs. 47.4%) among males, while alcohol and caffeine use were comparable between genders. Therapeutic agent use was more frequent among females, including antidepressants (18.6% vs. 10.8%) and anxiolytics (15.3% vs. 13.8%). Less prevalent psychoactive substances included sedatives and amphetamine-type stimulants (13.9% each), cocaine (10.6%), hallucinogens (10.5%), inhalants (4.6%), opioids (2.5%), other drugs (3.4%), and any non-medical drugs by injection (0.6%) (Table 5).
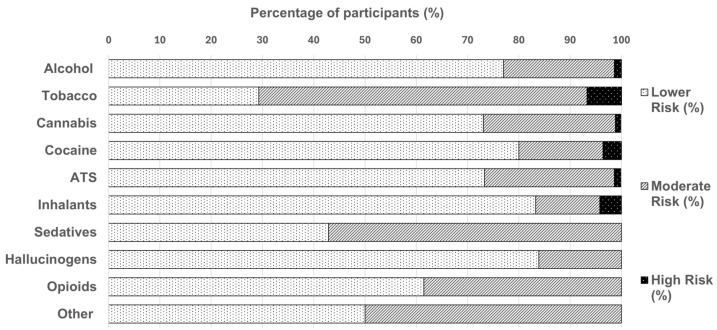
The WHO ASSIST substances associated with high-risk use were tobacco (6.8%), inhalants (4.2%), cocaine (3.6%), alcohol (1.4%), amphetamine-type stimulants (1.3%), and cannabis (1.1%) (Figure 2). Additionally, among those who reported use of other drugs (n = 19), 50% were classified as medium risk.
The negative binomial regression model was statistically significant compared with the intercept-only model (χ2(2) = 28.16, p < 0.001; Table 6). PHQ-9 scores were positively associated with the TIS, with each one-point increase on the PHQ-9 predicting a 3.4% increase in expected TIS (B = 0.033, SE = 0.007, 95% CI [0.019–0.046], Exp(B) = 1.034, p < 0.001). Gender also significantly predicted the TIS, with females having 26% lower expected scores than males (B = −0.299, SE = 0.108, 95% CI [−0.510–−0.088], Exp(B) = 0.741, p = 0.006). Model diagnostics indicated an adequate fit (Deviance/df = 1.04; AIC = 3731.33). In addition, when entered separately into adjusted negative binomial models, controlling for gender and PHQ-9 scores, student origin (Latvian vs. international; p = 0.054) and living arrangement (p = 0.063) demonstrated marginal significance. The omnibus test statistics for the preliminary negative binomial regression model are provided in Table A2, and the full predictor-level parameter estimates from that model are presented in Table A3.
Table 6: Negative binomial regression predicting the Total Involvement Score (TIS) from gender and PHQ-9 depression scores (n = 470).
| Predictor | B | SE | 95% CI for B | Wald χ2 | p | Exp(B) |
|---|---|---|---|---|---|---|
| Intercept | 2.821 | 0.112 | [2.602–3.041] | 636.704 | <0.001 | 16.8 |
| Gender (female vs. male) | −0.299 | 0.108 | [−0.510–0.088] | 7.692 | 0.006 | 0.741 |
| PHQ-9 total score | 0.033 | 0.007 | [0.019–0.046] | 21.713 | <0.001 | 1.034 |
Note: Values are regression coefficients (B), standard errors (SE), 95% confidence intervals (CI), with Wald χ2 statistics, p-values, and exponentiated coefficients Exp(B). PHQ-9 = Patient Health Questionnaire-9. All p < 0.05.
Table A2: Omnibus Wald χ2 tests from a preliminary generalized linear model (negative binomial regression) predicting the TIS (n = 466).
| Predictor | Wald χ2 | df | p |
|---|---|---|---|
| Intercept | 572.458 | 1 | <0.001 |
| Gender | 10.468 | 1 | 0.001 |
| Living quarters | 5.099 | 2 | 0.078 |
| Student origin | 3.085 | 1 | 0.079 |
| PHQ-9 total score | 3.458 | 1 | 0.063 |
| GAD-7 total score | 2.149 | 1 | 0.143 |
| Clinical year | 0.316 | 1 | 0.574 |
Note: Wald χ2 statistics, degrees of freedom (df), and corresponding p-values are presented. GAD-7 = Generalized Anxiety Disorder-7; PHQ-9 = Patient Health Questionnaire-9. All p < 0.05.
Table A3: Parameter estimates from a preliminary generalized linear model (negative binomial regression) predicting the TIS (n = 466).
| Predictor | B | SE | 95% CI for B | Wald χ2 | p | Exp(B) |
|---|---|---|---|---|---|---|
| Intercept | 2.692 | 0.165 | [2.369–3.015] | 266.545 | <0.001 | 14.77 |
| Gender (female vs. male) | −0.394 | 0.122 | [−0.633–−0.155] | 10.468 | 0.001 | 0.674 |
| Living quarters (owned vs. family) | 0.140 | 0.170 | [−0.194–0.473] | 0.676 | 0.411 | 1.150 |
| Living quarters (rented vs. family) | 0.310 | 0.137 | [0.041–0.579] | 5.099 | 0.024 | 1.364 |
| Student origin (international vs. Latvian) | −0.241 | 0.137 | [−0.510–0.028] | 3.085 | 0.079 | 0.786 |
| PHQ-9 total score | 0.020 | 0.016 | [−0.001–0.041] | 3.458 | 0.063 | 1.020 |
| GAD-7 total score | 0.019 | 0.013 | [−0.006–0.044] | 2.149 | 0.143 | 1.019 |
| Clinical year (pre-clinical vs. clinical) | 0.061 | 0.108 | [−0.152–0.274] | 0.316 | 0.574 | 1.063 |
Note: Values are regression coefficients (B), standard errors (SE), 95% confidence intervals (CI), Wald χ2 statistics, exponentiated coefficients Exp(B) and corresponding p-values are presented. GAD-7 = Generalized Anxiety Disorder-7; PHQ-9 = Patient Health Questionnaire-9. All p < 0.05.
3.3. Additional Findings and Miscellaneous Results
Within the group of psychoactive substances classified as other in the appendix (n = 39), the most frequently reported classes were hallucinogens (35%), stimulants (25%), sedatives and anxiolytics (20%), nicotine products (10%), and antidepressants (10%). Open-ended responses recorded in the other category of the WHO ASSIST (n = 19) identified 32 distinct substances, reflecting multiple mentions per participant. The most reported were 2C-B (15.8%), 3,4-methylenedioxymethamphetamine (MDMA)/ecstasy (15.8%), and poppers/alkyl nitrites (10.5%).
4. Discussion
Women represented 70.8% of the faculty’s total student body. Consistent with this distribution, women were also strongly represented in our sample, comprising 72.8% of participants. This pattern reflects the documented increase in female participation in medical education across Europe [ref. 56]. Among international students, a majority originated from Western Europe (63.2%), reflecting cross-border enrollment trends within EU medical education. Regarding socioeconomic indicators, household income responses indicated a heterogeneous distribution; however, interpretation is limited by a 24.0% nonresponse rate. The rate of income nondisclosure in our sample aligns with European survey patterns, where approximately 20–40% of respondents in some countries decline to disclose household income [ref. 57]. Given the absence of more detailed socioeconomic measures (such as parental education and occupation), the reported income distribution appeared less skewed relative to comparable datasets. For example, data from Germany [ref. 58] and the United Kingdom [ref. 59,ref. 60] demonstrate that medical students are often overrepresented among higher-income families.
Most students reported no prior history of psychiatric treatment; however, a notable minority (13.6%) reported having accessed treatment within the past three months. This finding is consistent with meta-analytic evidence indicating elevated levels of depression and anxiety symptoms among medical students [ref. 12,ref. 13,ref. 14]. Overall, our sample mirrors European trends of gendered mental health, which may have implications for female medical students in their specialty choice and training pathways at both the European [ref. 56,ref. 61] and local institutional level [ref. 28].
4.1. Substance Use Trends
The lifetime prevalence of psychoactive substance use in our sample—particularly for alcohol (93.9%), tobacco (68.4%), and cannabis (50.9%)—was higher than the rates reported in a WHO ASSIST–based study of Swiss medical students (n = 886). That study reported lower lifetime rates of alcohol (86.6%), tobacco (31.4%), and cannabis use (23.5%) [ref. 4]. Specific data on regular use and dependence among medical schools in France and Italy indicate further heterogeneity across European medical schools. Pre-COVID-19 data from France (n = 171) reported higher regular alcohol (97%) and cannabis use (77%), but lower regular tobacco use (21%) [ref. 5]. In contrast, Italian data collected during the COVID-19 pandemic (n = 222) reported lower regular rates overall for alcohol (66%), cannabis use (6%), and tobacco use (25%) [ref. 62]. These differences may partly reflect national variations in psychoactive substance use, reporting methodology (lifetime vs. regular), or sampling methods.
Caffeine use was nearly universal among participants, exceeding reported rates of coffee consumption in comparable medical student samples. The lifetime prevalence of caffeine-containing substance use in our sample was 98.7%, surpassing reported rates of lifetime coffee consumption alone (n = 301, 82.9%) [ref. 63] and habitual coffee consumption (n = 583, 91.4%) [ref. 64] observed in two independent Italian samples of medical students. This difference likely reflects the broader definition of caffeine use in our study, which encompassed all caffeinated substances.
With respect to other substances, Swiss medical students reported lower lifetime prevalence for cocaine (1.4% vs. 10.6%), hallucinogens (1% vs. 10.5%), opioids (1.2% vs. 2.5%), and sedatives (6.8% vs. 13.9%) [ref. 4]. Recent use was also lower in the Swiss study, with only 3% reporting monthly sedative use and ≤0.3% reporting opioid and stimulant use. Overall, these findings support evidence that alcohol, tobacco, and cannabis remain the most commonly used substances among medical students across European contexts [ref. 21,ref. 22], while also highlighting considerable local variation.
Our study identified higher rates of lifetime and past-three-month prevalence of antidepressants and anxiolytics compared to other datasets (Table 5). In total, 10.4% of students reported receiving psychotherapy, 6.3% pharmacotherapy only, and 11.3% in combination with psychotherapy, while 28.7% reported any form of psychiatric treatment (Table 1). By contrast, a large French cross-sectional cohort of medical students (n = 10,985) reported lower rates of daily use, with 5.7% for anxiolytics and 2.8% for antidepressants, indicating that ongoing pharmacotherapy was less frequent in that context [ref. 65].
The observed gradient (regular use < recent use < lifetime use) may reflect both measurement differences and real-world factors such as intermittent adherence, misdiagnosis, other comorbidities, and substance use [ref. 39,ref. 40]. In support of this, substance use trends among medical students are possibly under-reported due to access, stigma, or variable approaches in treatment [ref. 66]. These factors may obscure actual patterns of pharmacotherapy uptake, even in the presence of clinical need [ref. 14].
Cognitive enhancement substance use also emerged as a relevant factor in understanding patterns of stimulant use among medical students. A Lithuanian study (n = 579) reported the use of nootropics, ATS, and related agents among 8.1% of medical students [ref. 67], while a large Belgian survey of university students (n = 12,144) reported lifetime medical stimulant use of 6.9% [ref. 43]. The corresponding lifetime prevalence in our sample was 9.5%, slightly higher than both the Lithuanian and Belgian figures, yet still within the ranges identified in international reviews [ref. 21,ref. 23,ref. 24]. This study also distinguished prescription stimulant use from non-prescription stimulant use, revealing a prevalence difference of approximately 4% (Table 5). However, stimulant use in medical students is primarily guided by psychiatric comorbidity [ref. 23,ref. 68], cognitive enhancement motives [ref. 21,ref. 23,ref. 24,ref. 67,ref. 68], and polysubstance use [ref. 38,ref. 68]. Therefore, potential confounding effects must be examined prior to more definitive conclusions. Furthermore, psychotropic medication use may also contribute to confounding within psychiatric screening outcomes and reported psychoactive substance use prevalence.
In summary, these findings suggest that psychotropic medication exposure is relatively common in this sample, with observed differences likely reflecting variability in treatment access, and treatment engagement shaped by both individual and systemic factors beyond the immediate medical school context [ref. 66,ref. 69]. Furthermore, our lifetime prevalence for psychoactive substances was broadly comparable with European studies, although differences in methodology and the limited availability of recent post-COVID-19 data among medical students constrain more definitive comparisons.
Distinct gendered patterns were observed: males reported higher use across all WHO ASSIST substances, whereas females reported greater use of antidepressants and anxiolytics (Table 5). These findings align with previous European research. At the Medical University of Vienna, a WHO ASSIST–based study of medical students (n = 589) found that males generally reported a higher past three-month prevalence of psychoactive substance use [ref. 70]. The only exception was sedatives, where females reported slightly higher rates in the 2nd (5.1% vs. 4.8%) and 6th years (2.8% vs. 0.0%) [ref. 70].
Although initial Mann–Whitney U and Kruskal–Wallis tests suggested differences in WHO ASSIST substance use risk scores by student origin and year of study (Figure 2), these effects were not confirmed when examining Hodges–Lehmann confidence intervals. This indicates that the apparent group differences may reflect statistical noise rather than meaningful variation.
Of particular relevance, our data also highlighted the use of 2C-B (a psychedelic phenethylamine with hallucinogenic and entactogenic properties) [ref. 71] and poppers (alkyl nitrites), substances often associated with chemsex and linked to adverse mental health outcomes [ref. 72]. A Belgian population study (n = 836) reported chemsex engagement among 30.9% of participants, most commonly with poppers (73%) and, to a lesser extent, 2C-B (3%) [ref. 73]. Similarly, a Parisian study of university students (n = 153) reported past-year hallucinogen (9.8%) and poppers use (5.2%), with chemsex behavior significantly associated with medical training (p = 0.021) [ref. 74]. Although limited in scope, these findings underscore shifting motivations for recreational polysubstance use, where psychoactive and physiological effects within distinct sociodemographic niches warrant further investigation.
4.2. Associations Between Demographics and Depression, Anxiety, and Resilience Scores
The proportion of students screening positive (≥10) for depression (PHQ-9) and anxiety (GAD-7) in our sample (Table 2 and Table 3) exceeded pooled global prevalence estimates reported in prior meta-analyses [ref. 12,ref. 13,ref. 14]. This difference may partly reflect significant variability by gender and student origin. Female students reported higher median scores on both the GAD-7 and the PHQ-9 compared with males (Table 2), a pattern consistent with global findings. For example, a multicenter study of 40 United States (U.S.) medical schools (n = 1428) conducted during the COVID-19 pandemic reported higher median scores among females than males (GAD-7: 7.0 vs. 5.0, p < 0.00001; PHQ-9: 6.0 vs. 4.0, p < 0.00001) [ref. 8]. Gender disparities in symptom burden have been associated with coping strategies such as self-distraction, behavioral disengagement, and denial [ref. 75]. These findings align with global data indicating a higher prevalence of depressive symptoms (31.5% vs. 24.2%) and an approximately two-fold greater likelihood of experiencing anxiety among female medical students [ref. 76]. However, gender-based differences are evident at a broader population level before [ref. 77,ref. 78] and during the COVID-19 pandemic [ref. 79]. In addition, the six-month timeframe of this study limits temporal comparability and precludes conclusions regarding persistent gender-specific trends. Thus, the gender disparities likely reflect broader gender linked mental health patterns rather than phenomena unique to medical education.
Latvian medical students reported comparable rates of depression, but markedly higher rates of anxiety compared with a Lithuanian sample of multidisciplinary students (n = 1368; depression: 56.7% vs. 45.0%; anxiety: 57.9% vs. 38.0%) [ref. 80]. Prevalence estimates for Latvian medical students also exceeded those reported for European medical students during the COVID-19 pandemic, where pooled estimates of moderate-to-severe symptoms were 23.9% for depression (95% CI [18.1–29.8]) and 29.7% for anxiety (95% CI [13.2–46.2]) across five studies [ref. 9].
In contrast, international medical students in Latvia reported lower symptom levels (depression: 34.9%; anxiety: 41.2%), although these values still surpassed comparable European values. However, across broader European subgroups, overall symptom prevalence was higher (depression: 39.9%; anxiety: 45.0%), reflecting the inclusion of milder symptomatology [ref. 9], whereas the present study defined prevalence at moderate or greater symptom severity. Historical data from Estonian medical students (n = 413) assessed using the Emotional State Questionnaire identified anxiety symptoms in 21.9% and depressive symptoms in 30.6% of participants [ref. 81]. Although based on a pre-COVID-19 sample and a different instrument, these findings, together with data on Latvian origin students [ref. 31], suggest that elevated symptom prevalence within Baltic student populations (Latvian, Lithuanian, and Estonian) is not exclusive to the COVID-19 pandemic. Furthermore, potential variations in optimal cutoff thresholds and instrument sensitivities across psychiatric screening instruments may also contribute to higher apparent prevalence rates in the Baltic region [ref. 52,ref. 80].
Resilience differed significantly by gender and student origin (Table 2 and Table 3), although mean scores for all groups remained within the normal range. Comparable mean scores and gender-based patterns have been reported in other European studies conducted during the COVID-19 pandemic. A Serbian study reported a mean BRS score of 3.17 ± 0.80 among medical students, while 33.3% of all study participants were classified as low, 56.7% as medium, and 10% as high resilience [ref. 82]. Similarly, a Swedish study of medical students (n = 457; semesters 2–10) found lower resilience scores among females (p < 0.001), with most participants classified as normal resilience (53.1%), followed by low (27.9%) and high (19.0%) [ref. 83]. However, post hoc analysis did not confirm specific differences between groups, and the exclusion of early and final year students may limit direct comparability with our findings. Nevertheless, resilience levels observed in this study appear consistent with broader European patterns, despite gender and sample composition differences.
Normality diagnostics indicated borderline to significant deviations across all psychiatric screening tools. Skewness Z-scores were 0.52 for the BRS, 1.43 for the GAD-7, and 4.98 for the PHQ-9, while kurtosis Z-scores ranged from 2.78 to 4.17. These values exceed accepted thresholds of normality (Z > 1.96), reflecting distributional properties typical of psychiatric screening instruments [ref. 84].
4.3. Year-of-Study Differences in Depression, Anxiety, and Resilience
The PHQ-9 results from this study align with large multicenter investigations that have demonstrated significant stage of study differences in depressive symptoms among medical students [ref. 1,ref. 8], as well as with meta-analytic evidence showing greater symptom burden among pre-clinical students [ref. 14]. However, other reviews, such as that by Rotenstein et al. [ref. 12], reported no significant stage-related differences, emphasizing sample heterogeneity and methodological limitations. In contrast, meta-analytic data have generally shown no significant stage differences for anxiety [ref. 13], which is consistent with the absence of stage effects in our GAD-7 data. Similarly, resilience may stabilize as students develop coping strategies or self-select out of medical training, resulting in comparable scores across study stages [ref. 83].
4.4. Associations Between Mental Health, Socio-Demographics, and Substance Use Risk
Our negative binomial regression model identified depressive symptoms and gender as significant predictors of substance involvement, as measured by the WHO TIS. Each additional PHQ-9 point corresponded to a 3.4% higher expected TIS, while female students had a 26% lower expected TIS compared with males (Table 6). These findings align with prior research among Polish [ref. 3] and Italian medical students [ref. 62], where male gender was linked to hazardous alcohol use. Similarly, data from Ethiopia indicate that gender and the interaction of gender with residence are significant predictors of risky substance use in a WHO ASSIST-based study on engineering students (n = 243) [ref. 85]. A comparable association was observed among U.S. registered nurses (n = 1478), where WHO ASSIST data linked depressive symptoms to increased substance use risk [ref. 86].
Furthermore, a Spanish study of medical students (n = 1265) reported higher depression symptom levels among females and gender differences in substance use patterns [ref. 1]. Several variables previously identified as predictors were not significant in our model. For example, age, study year, anxiety, and impulsiveness have been identified as predictors of substance use in a large multidisciplinary logistic regression study from a German University sample (n = 3991) [ref. 87]. Similarly, anxiety was a significant predictor across multivariate regression models examining substance use among registered nurses [ref. 86]. However, none of these variables predicted substance use involvement in our data, and housing arrangements only approached significance.
These discrepancies likely reflect both contextual differences and the application of a parsimonious negative binomial model, which optimized explanatory power while addressing over-dispersion in count data (skewness = 2.16; kurtosis = 8.68). Nonetheless, variables excluded from our model may remain important in studies employing alternative analytic frameworks, such as logistic or linear regression.
4.5. Implications and Recommendations
The findings of this research highlight the importance of education, monitoring, and referral programs, which can be shaped by local context and supported according to institutional capacity.
The Association of American Medical Colleges Guidelines for the Development of Chemical Impairment Policies for Medical Schools emphasize that chemical dependency is a treatable condition [ref. 88,ref. 89]. Institutional policies should therefore ensure confidentiality, encourage early self-referral, and support recovery while maintaining patient safety [ref. 88,ref. 89]. At RSU, existing policies prohibit the use of illegal psychoactive substances on University or affiliated clinical premises. In addition, smoking and vaping bans were introduced across RSU premises in October 2022.
Future institutional policies should further emphasize stigma reduction surrounding psychoactive substance use, recognizing education as central to effective prevention [ref. 88,ref. 89,ref. 90]. Furthermore, brief mandatory modules focused on addiction medicine and harm-reduction principles may contribute to improved understanding, reduced stigma, greater empathetic awareness, and strengthened professional responsibility [ref. 89,ref. 90,ref. 91]. Incorporating these modules early and within the educational curriculum promotes and empowers a culture of both individual, collective, and institutional action [ref. 89,ref. 90,ref. 91]. This educational approach reframes substance use from a stigmatized disciplinary issue to a personal and public-health issue that requires evidence-based screening, early intervention, and empathetic, pragmatic support.
Effective policy depends on accurate, recent, and actionable data. A structured, longitudinal monitoring program is warranted to facilitate early detection and intervention. Institutional monitoring of both incoming and current medical students may help identify knowledge gaps, attitudes, and potentially problematic psychoactive substance use [ref. 4,ref. 91]. Furthermore, large cross-sectional datasets, including this study, consistently demonstrate an association between psychoactive substance use and psychological distress among medical students [ref. 1,ref. 4,ref. 92] and in the general population [ref. 93]. Therefore, integrated, time-sensitive monitoring of both psychoactive substance use and mental health is essential in medical education.
Evidence-based screening tools such as the Brief Alcohol Screening and Intervention for College Students have proven effective in reducing alcohol related harms in university populations [ref. 94]. A pragmatic institutional solution would include an annual, anonymous questionnaire distributed to all RSU medical students to assess and identify at-risk students, monitor mental health, and identify students requiring a follow-up within a longer-term project such as the ETMED-L project [ref. 4]. The instruments used in this study demonstrate the value of anonymous bilingually validated tools for screening purposes: the WHO ASSIST V3.1, PHQ-9, GAD-7, and BRS. However, broader implementation of the WHO ASSIST remains contingent upon its successful validation in the Latvian language, with V3.0 recommended for online research applications [ref. 35].
Where risk or impairment is evident, referral to cognitive-behavioral therapy or motivational interviewing is recommended, ensuring confidentiality and clear criteria for return to training [ref. 4,ref. 88,ref. 89]. RSU offers an established support system for students. The RSU Health Centre provides medical and psychiatric care, while the Career Guidance and Well-Being Centre offers confidential counselling, crisis support, and self-referral pathways [ref. 95]. Additional mental health services are available through the Clinic of Psychosomatic Medicine and Psychotherapy. Recommended interventions can be flexibly integrated within this support framework to ensure timely and student-centered care.
Integrating detection, harm reduction, and treatment pathways into a unified student-centered strategy fulfills ethical mandates while mitigating long-term professional risk. Moreover, this model ensures that RSU remains aligned with its mandate to safeguard medical student health, patient safety, and institutional integrity through confidentiality, support, and rehabilitation.
5. Limitations
Several limitations should be considered when interpreting these findings.
First, among all respondents (n = 742), 4.9% (n = 36) self-reported their ineligibility during survey completion. This self-reporting highlights concerns regarding perceived anonymity and privacy, particularly related to the disclosure of sensitive mental health and substance use information. As the study design prioritized anonymity and data quality, no participant contact details or identifying information were stored. Thus, participants did not receive individualized referral links or feedback related to their reported mental health or psychoactive substance use. However, future studies should more explicitly emphasize data protection and confidentiality while integrating self-referral information to university support services. Adopting a hybrid anonymous-confidential design could enhance participant well-being and trust in data protection procedures.
Second, the cross-sectional study design precludes causal inference. Although significant associations were observed, these reflect correlations at a single time point within a six-month data collection window; therefore, definitive conclusions on directionality are limited. More broadly, online survey-based research is vulnerable to convenience sampling, self-selection, and nonresponse biases. These factors may partly explain the significant deviations from normality observed in the continuous scores of the GAD-7, the PHQ-9, and the BRS. Such deviations may have reduced measurement sensitivity.
Third, approximately 70–80% of participants who reported substances under the other or appendix categories did so despite the WHO ASSIST providing comprehensive, predefined substance classifications. This pattern suggests ambiguity regarding substance categorization or a possible misinterpretation of survey items, potentially reflecting the preliminary nature of the Latvian adaptation of the WHO ASSIST. Future applications of the WHO ASSIST in Latvia should be contingent on completing the designated WHO validation process to ensure linguistic and conceptual equivalence.
Fourth, the psychiatric screening tools (GAD-7, PHQ-9, BRS) assess symptoms over the preceding two weeks, whereas the WHO ASSIST evaluated substance use over the past three months. Although this temporal mismatch may introduce some asynchrony, it should be noted that the negative binomial regression model did not directly compare these measures but modeled their associations within the same analytic framework. Finally, the sample included medical students from only one of the two Latvian universities offering medical education, which may limit the generalizability. Although the sample was large and diverse, inclusion of medical students from the University of Latvia in future research would enhance representativeness.
Consequently, future investigations should refine methodological items and variables approaching significance in this study, while expanding the range of contextual, cultural, social, and religious factors assessed. Doing so may improve model validity and provide a more nuanced understanding of substance use behaviors among medical students in Latvia.
6. Conclusions
This study contributes novel data on substance use patterns, gender-specific differences, and mental health correlates among medical students in Latvia following the COVID-19 pandemic. The findings highlight the importance of targeted prevention strategies, enhanced education on substance use, and efforts to reduce stigma surrounding mental health support within medical training. Elevated prescription substance use and relatively high levels of recent (past-three-month) psychoactive substance consumption in male students, combined with a substantial proportion of female students exceeding standard clinical cutoffs (≥10) on the GAD-7 and the PHQ-9, warrant further investigation. Future longitudinal research should clarify causal relationships and incorporate sociodemographic and cultural factors that may shape both substance use and mental health trajectories in this population.
References
- B. Atienza-Carbonell, V. Guillén, M. Irigoyen-Otiñano, V. Balanzá-Martínez. Screening of substance use and mental health problems among Spanish medical students: A multicenter study. J. Affect. Disord., 2022. [DOI | PubMed]
- E. Balogh, N. Faubl, H. Riemenschneider, P. Balázs, A. Bergmann, K. Cseh, F. Horváth, J. Schelling, A. Terebessy, Z. Wagner. Cigarette, waterpipe and e-cigarette use among an international sample of medical students. Cross-sectional multicenter study in Germany and Hungary. BMC Public Health, 2018. [DOI | PubMed]
- M. Gajda, K. Sedlaczek, S. Szemik, M. Kowalska. Determinants of Alcohol Consumption among Medical Students: Results from POLLEK Cohort Study. Int. J. Environ. Res. Public Health, 2021. [DOI | PubMed]
- J. Gaume, V. Carrard, S. Berney, C. Bourquin, A. Berney. Substance use and its association with mental health among Swiss medical students: A cross-sectional study. Int. J. Soc. Psychiatry, 2024. [DOI | PubMed]
- M. Gignon, E. Havet, C. Ammirati, S. Traullé, C. Manaouil, T. Balcaen, G. Loas, G. Dubois, O. Ganry. Alcohol, Cigarette, and Illegal Substance Consumption Among Medical Students. Workplace Health Saf., 2015. [DOI | PubMed]
- C. Song-Smith, E. Jacobs, J. Rucker, M. Saint, J. Cooke, M. Schlosser. UK medical students’ self-reported knowledge and harm assessment of psychedelics and their application in clinical research: A cross-sectional study. BMJ Open, 2024. [DOI]
- B. Jullian, M. Deltour, N. Franchitto. The consumption of psychoactive substances among French physicians: How do they perceive the creation of a dedicated healthcare system?. Front. Psychiatry, 2023. [DOI | PubMed]
- S.J. Halperin, M.N. Henderson, S. Prenner, J.N. Grauer. Prevalence of Anxiety and Depression Among Medical Students During the Covid-19 Pandemic: A Cross-Sectional Study. J. Med. Educ. Curric. Dev., 2021. [DOI | PubMed]
- Y.-K. Lin, I.D. Saragih, C.-J. Lin, H.-L. Liu, C.-W. Chen, Y.-S. Yeh. Global prevalence of anxiety and depression among medical students during the COVID-19 pandemic: A systematic review and meta-analysis. BMC Psychol., 2024. [DOI | PubMed]
- B. Christophers, E. Nieblas-Bedolla, J.S. Gordon-Elliott, Y. Kang, K. Holcomb, M.K. Frey. Mental Health of US Medical Students During the COVID-19 Pandemic. J. Gen. Intern. Med., 2021. [DOI | PubMed]
- P. Tempski, F.M. Arantes-Costa, R. Kobayasi, M.A.M. Siqueira, M.B. Torsani, B.Q.R.C. Amaro, M.E.F.M. Nascimento, S.L. Siqueira, I.S. Santos, M.A. Martins. Medical students’ perceptions and motivations during the COVID-19 pandemic. PLoS ONE, 2021. [DOI | PubMed]
- L.S. Rotenstein, M.A. Ramos, M. Torre, J.B. Segal, M.J. Peluso, C. Guille, S. Sen, D.A. Mata. Prevalence of Depression, Depressive Symptoms, and Suicidal Ideation Among Medical Students. JAMA, 2016. [DOI | PubMed]
- T.T.-C. Quek, W.W.-S. Tam, B.X. Tran, M. Zhang, Z. Zhang, C.S.-H. Ho, R.C.-M. Ho. The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis. Int. J. Environ. Res. Public Health, 2019. [DOI | PubMed]
- R. Puthran, M.W.B. Zhang, W.W. Tam, R.C. Ho. Prevalence of depression amongst medical students: A meta-analysis. Med. Educ., 2016. [DOI | PubMed]
- S.R. Azim, M.S.B. Yusoff, N.S. Roslan. Mapping the multidimensional factors of medical student resilience development: A scoping review. BMC Med. Educ., 2025. [DOI | PubMed]
- B.W. Smith, J. Dalen, K. Wiggins, E. Tooley, P. Christopher, J. Bernard. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med., 2008. [DOI | PubMed]
- D. Karlin, S.J. Suponcic, N. Chen, C. Steinhart, P. Duong. Prevalence of Generalized Anxiety Disorder Among Five European Countries Before and During COVID. Eur. Psychiatry, 2024. [DOI]
- J.A.-D. La Torre, G. Vilagut, A. Ronaldson, I. Bakolis, A. Dregan, V. Martín, G. Martinez-Alés, A.J. Molina, A. Serrano-Blanco, J.M. Valderas. Prevalence and variability of depressive symptoms in Europe: Update using representative data from the second and third waves of the European Health Interview Survey (EHIS-2 and EHIS-3). Lancet Public Health, 2023. [DOI | PubMed]
- T. Salisbury, C. Chamanadjian, H. Nguyen. Substance Misuse Among Medical Students, Resident Physicians, and Fellow Physicians: A Review with Focus on the United States’ Population. Cureus, 2024. [DOI | PubMed]
- E.E. Ayala, D. Roseman, J.S. Winseman, H.R.C. Mason. Prevalence, perceptions, and consequences of substance use in medical students. Med. Educ. Online, 2017. [DOI | PubMed]
- C. Roncero, A. Egido, L. Rodríguez-Cintas, J. Pérez-Pazos, F. Collazos, M. Casas. Substance Use among Medical Students: A Literature Review 1988–2013. Actas Esp. Psiquiatr., 2015. [PubMed]
- G. Papazisis, S. Siafis, I. Tsakiridis, I. Koulas, T. Dagklis, D. Kouvelas. Prevalence of Cannabis Use Among Medical Students: A Systematic Review and Meta-analysis. Subst Abuse, 2018. [DOI | PubMed]
- A.N. Edinoff, C.A. Nix, S.E. McNeil, S.E. Wagner, C.A. Johnson, B.C. Williams, E.M. Cornett, K.S. Murnane, A.M. Kaye, A.D. Kaye. Prescription Stimulants in College and Medical Students: A Narrative Review of Misuse, Cognitive Impact, and Adverse Effects. Psychiatry Int., 2022. [DOI]
- N. Plumber, M. Majeed, S. Ziff, S.E. Thomas, S.R. Bolla, V.R. Gorantla. Stimulant Usage by Medical Students for Cognitive Enhancement: A Systematic Review. Cureus, 2021. [DOI | PubMed]
- D.C. Gottfredson, D.B. Wilson. Characteristics of Effective School-Based Substance Abuse Prevention. Prev. Sci., 2003. [DOI | PubMed]
- A.L. Stone, L.G. Becker, A.M. Huber, R.F. Catalano. Review of risk and protective factors of substance use and problem use in emerging adulthood. Addict. Behav., 2012. [DOI | PubMed]
- J.T. Goldbach, E.E. Tanner-Smith, M. Bagwell, S. Dunlap. Minority Stress and Substance Use in Sexual Minority Adolescents: A Meta-analysis. Prev. Sci., 2014. [DOI | PubMed]
- N. Jain, K. Jersovs, T. Safina, M. Pilmane, N. Jansone-Ratinika, I. Grike, A. Petersons. Medical education in Latvia: An overview of current practices and systems. Front. Med., 2023. [DOI]
- Which Countries Have the Most Doctor and Dentist Graduates? Website: News Article
- R.S. University. Medicine 3.0 Study Programme—A New Era in Latvian Medical Education. Riga Stradins University
- K.-K. Rueckert, G. Ancane. Cross-sectional study among medical students in Latvia: Differences of mental symptoms and somatic symptoms among Latvian and international students. Pap. Anthropol., 2018. [DOI]
- M. Griffin, R.J. Martino, C. LoSchiavo, C. Comer-Carruthers, K.D. Krause, C.B. Stults, P.N. Halkitis. Ensuring survey research data integrity in the era of internet bots. Qual. Quant., 2022. [DOI | PubMed]
- F.J. Gill, G.D. Leslie, C. Grech, J.M. Latour. Using a web-based survey tool to undertake a Delphi study: Application for nurse education research. Nurse Educ. Today, 2013. [DOI | PubMed]
- R. Humeniuk, R. Ali, T.F. Babor, M. Farrell, M.L. Formigoni, J. Jittiwutikarn, R.B. De Lacerda, W. Ling, J. Marsden, M. Monteiro. Validation of the alcohol, smoking and substance involvement screening test (ASSIST). Addiction, 2008. [DOI | PubMed]
- R. Humeniuk, R. Ali, V. Poznyak, M. Monteiro. The Alcohol Smoking and Substance Involvement Screening Test (ASSIST): Manual for Use in Primary Care, 2010
- J. McNeely, S.M. Strauss, J. Rotrosen, A. Ramautar, M.N. Gourevitch. Validation of an audio computer-assisted self-interview (ACASI) version of the alcohol, smoking and substance involvement screening test (ASSIST) in primary care patients. Addiction, 2016. [DOI | PubMed]
- S. Monteith, T. Glenn. Searching online to buy commonly prescribed psychiatric drugs. Psychiatry Res., 2018. [DOI | PubMed]
- G. Papazisis, I. Tsakiridis, S. Siafis. Nonmedical Use of Prescription Drugs among Medical Students and the Relationship With Illicit Drug, Tobacco, and Alcohol Use. Subst. Abus., 2018. [DOI | PubMed]
- A. Garakani, J.W. Murrough, R.C. Freire, R.P. Thom, K. Larkin, F.D. Buono, D.V. Iosifescu. Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment Options. Front. Psychiatry, 2020. [DOI | PubMed]
- S. Chiappini, R. Vickers-Smith, A. Guirguis, J.M. Corkery, G. Martinotti, F. Schifano. A Focus on Abuse/Misuse and Withdrawal Issues with Selective Serotonin Reuptake Inhibitors (SSRIs): Analysis of Both the European EMA and the US FAERS Pharmacovigilance Databases. Pharmaceuticals, 2022. [DOI | PubMed]
- A. Fagiolini, L.D. Grošelj, M. Šagud, A. Silić, M. Latas, Č.D. Miljević, A. Cuomo. Targeting heterogeneous depression with trazodone prolonged release: From neuropharmacology to clinical application. Ann. Gen. Psychiatry, 2025. [DOI | PubMed]
- T. Callovini, D. Janiri, D. Segatori, G. Mastroeni, G.D. Kotzalidis, M. Di Nicola, G. Sani. Examining the Myth of Prescribed Stimulant Misuse among Individuals with Attention-Deficit/Hyperactivity Disorder: A Systematic Review. Pharmaceuticals, 2024. [DOI | PubMed]
- M. Sabbe, J. Sawchik, M. Gräfe, F. Wuillaume, S. De Bruyn, P. Van Antwerpen, G. Van Hal, M. Desseilles, J. Hamdani, H. Malonne. Use and misuse of prescription stimulants by university students: A cross-sectional survey in the French-speaking community of Belgium, 2018. Arch. Public Health, 2022. [DOI | PubMed]
- M. Scalese, M. Baroni, S. Biagioni, L. Bastiani, F. Denoth, S. Molinaro. Exploring changes in non-medical prescription use of pharmaceutical stimulants among Italian adolescents from 2008 to 2023. J. Public Health, 2025. [DOI]
- D. Wikoff, B.T. Welsh, R. Henderson, G.P. Brorby, J. Britt, E. Myers, J. Goldberger, H.R. Lieberman, C. O‘BRien, J. Peck. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol., 2017. [DOI | PubMed]
- J.L. Temple, C. Bernard, S.E. Lipshultz, J.D. Czachor, J.A. Westphal, M.A. Mestre. The Safety of Ingested Caffeine: A Comprehensive Review. Front. Psychiatry, 2017. [DOI | PubMed]
- M. Davoudi, F. Abdoli, F. Momeni, M.H. Asgarabad. Network analysis of caffeine use disorder, withdrawal symptoms, and psychiatric symptoms. BMC Psychiatry, 2025. [DOI | PubMed]
- M.M. Sweeney, D.C. Weaver, K.B. Vincent, A.M. Arria, R.R. Griffiths. Prevalence and Correlates of Caffeine Use Disorder Symptoms Among a United States Sample. J. Caffeine Adenosine Res., 2020. [DOI | PubMed]
- J. Sánchez, N. Estrada-Hernández, J. Booth, D. Pan. Factor structure, internal reliability, and construct validity of the Brief Resilience Scale (BRS): A study on persons with serious mental illness living in the community. Psychol. Psychother. Theory Res. Pract., 2021. [DOI]
- K. Kroenke, R.L. Spitzer, J.B.W. Williams. The PHQ-9. J. Gen. Intern. Med., 2001. [DOI | PubMed]
- R.L. Spitzer, K. Kroenke, J.B.W. Williams, B. Löwe. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med., 2006. [DOI | PubMed]
- E. Rancans, M. Trapencieris, R. Ivanovs, J. Vrublevska. Validity of the PHQ-9 and PHQ-2 to screen for depression in nationwide primary care population in Latvia. Ann. Gen. Psychiatry, 2018. [DOI | PubMed]
- J. Vrublevska, L. Renemane, A. Kivite-Urtane, E. Rancans. Validation of the generalized anxiety disorder scales (GAD-7 and GAD-2) in primary care settings in Latvia. Front. Psychiatry, 2022. [DOI | PubMed]
- B.W. Smith. The Brief Resilience Scale (BRS)—Originally by B. W. Smith (2008), Adapted by G. Freimane as Īsā Dzīvesspēka Skala (2010), Obtained from RSU Psychology Laboratory’s Registry of Tests and Surveys. 2008
- G. Kjellsson, P. Clarke, U.-G. Gerdtham. Forgetting to remember or remembering to forget: A study of the recall period length in health care survey questions. J. Health Econ., 2014. [DOI | PubMed]
- V. Steiner-Hofbauer, H.W. Katz, J.S. Grundnig, A. Holzinger. Female participation or ‘feminization’ of medicine. Wien. Med. Wochenschr., 2023. [DOI | PubMed]
- P. Jabkowski, A. Piekut. Between task complexity and question sensitivity: Nonresponse to the income question in the 2008–2018 European Social Survey. Surv. Res. Methods, 2024. [DOI]
- O.R. Groene, T. Huelmann, W. Hampe, P. Emami. German Physicians and Medical Students Do Not Represent the Population They Serve. Healthcare, 2023. [DOI | PubMed]
- S. Fielding, P.A. Tiffin, R. Greatrix, A.J. Lee, F. Patterson, S. Nicholson, J. Cleland. Do changing medical admissions practices in the UK impact on who is admitted? An interrupted time series analysis. BMJ Open, 2018. [DOI]
- K. Steven, J. Dowell, C. Jackson, B. Guthrie. Fair access to medicine? Retrospective analysis of UK medical schools application data 2009-2012 using three measures of socioeconomic status. BMC Med. Educ., 2016. [DOI | PubMed]
- L. Mulder, A. Wouters, E.U. Akwiwu, A.S. Koster, J.H. Ravesloot, S.M. Peerdeman, M. Salih, G. Croiset, R.A. Kusurkar. Diversity in the pathway from medical student to specialist in the Netherlands: A retrospective cohort study. Lancet Reg. Health-Eur., 2023. [DOI | PubMed]
- M. Muselli, L. Tobia, E. Cimino, C. Confalone, M. Mancinelli, L. Fabiani, S. Necozione, V. Cofini. COVID-19 Impact on Substance Use (Tobacco, Alcohol, Cannabis) and Stress in Medical Students. OBM Neurobiol., 2024. [DOI]
- M. Pighi, G. Pontoni, A. Sinisi, S. Ferrari, G. Mattei, L. Pingani, E. Simoni, G.M. Galeazzi. Use and Propensity to Use Substances as Cognitive Enhancers in Italian Medical Students. Brain Sci., 2018. [DOI | PubMed]
- M. Lamberti, F. Napolitano, P. Napolitano, A. Arnese, V. Crispino, G. Panariello, G. Di Giuseppe. Prevalence of alcohol use disorders among under- and post-graduate healthcare students in Italy. PLoS ONE, 2017. [DOI | PubMed]
- A. Bourbon, L. Boyer, P. Auquier, M. Boucekine, V. Barrow, C. Lançon, G. Fond. Anxiolytic consumption is associated with tobacco smoking and severe nicotine dependence. Results from the national French medical students (BOURBON) study. Prog. Neuropsychopharmacol. Biol. Psychiatry, 2019. [DOI | PubMed]
- G. Fond, A. Bourbon, C. Lançon, M. Boucekine, J.-A. Micoulaud-Franchi, P. Auquier, L. Boyer. Psychiatric and psychological follow-up of undergraduate and postgraduate medical students: Prevalence and associated factors. Results from the national BOURBON study. Psychiatry Res., 2019. [DOI | PubMed]
- A. Lengvenytė, R. Strumila. Do medical students use cognitive enhancers to study? Prevalence and correlates from lithuanian medical students sample. Eur. Psychiatry, 2016. [DOI]
- T. Jebrini, K. Manz, G. Koller, D. Krause, M. Soyka, A.G. Franke. Psychiatric Comorbidity and Stress in Medical Students Using Neuroenhancers. Front. Psychiatry, 2021. [DOI | PubMed]
- G. Fond, A. Bourbon, M. Boucekine, M. Messiaen, V. Barrow, P. Auquier, C. Lançon, L. Boyer. First-year French medical students consume antidepressants and anxiolytics while second-years consume non-medical drugs. J. Affect. Disord., 2020. [DOI | PubMed]
- V. Steiner-Hofbauer, A. Holzinger. How to Cope with the Challenges of Medical Education? Stress, Depression, and Coping in Undergraduate Medical Students. Acad. Psychiatry, 2020. [DOI | PubMed]
- A.L. Halberstadt. Recent advances in the neuropsychopharmacology of serotonergic hallucinogens. Behav. Brain Res., 2015. [DOI | PubMed]
- A. Bohn, D. Sander, T. Köhler, N. Hees, F. Oswald, N. Scherbaum, D. Deimel, H. Schecke. Chemsex and Mental Health of Men Who Have Sex with Men in Germany. Front. Psychiatry, 2020. [DOI | PubMed]
- T. Platteau, C. Herrijgers, V. Barvaux, W.V. Berghe, L. Apers, T. Vanbaelen. Chemsex and its impact on gay and bisexual men who have sex with men: Findings from an online survey in Belgium. HIV Med., 2025. [DOI | PubMed]
- L. Malandain, S. Mosser, S. Mouchabac, J.-V. Blanc, C. Alexandre, F. Thibaut. Chemical sex (chemsex) in a population of French university students. Dialogues Clin. Neurosci., 2021. [DOI | PubMed]
- A. Neufeld, G. Malin. How medical students cope with stress: A cross-sectional look at strategies and their sociodemographic antecedents. BMC Med. Educ., 2021. [DOI | PubMed]
- A.A. Mirza, M. Baig, G.M. Beyari, M.A. Halawani, A.A. Mirza. Depression and Anxiety Among Medical Students: A Brief Overview. Adv. Med. Educ. Pract. Vol., 2021. [DOI | PubMed]
- C. McLean, A. Asnaani, B.T. Litz, S.G. Hofmann. Gender differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. J. Psychiatr. Res., 2011. [DOI | PubMed]
- O. Remes, C. Brayne, R. van der Linde, L. Lafortune. A systematic review of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav., 2016. [DOI | PubMed]
- T.D. Santo, Y. Sun, Y. Wu, C. He, Y. Wang, X. Jiang, K. Li, O. Bonardi, A. Krishnan, J.T. Boruff. Systematic review of mental health symptom changes by sex or gender in early-COVID-19 compared to pre-pandemic. Sci. Rep., 2022. [DOI | PubMed]
- A. Pranckeviciene, A. Saudargiene, J. Gecaite-Stonciene, V. Liaugaudaite, I. Griskova-Bulanova, D. Simkute, R. Naginiene, L.L. Dainauskas, G. Ceidaite, J. Burkauskas. Validation of the patient health questionnaire-9 and the generalized anxiety disorder-7 in Lithuanian student sample. PLoS ONE, 2022. [DOI | PubMed]
- T. Eller, A. Aluoja, V. Vasar, M. Veldi. Symptoms of anxiety and depression in Estonian medical students with sleep problems. Depress. Anxiety, 2006. [DOI | PubMed]
- D.I. Ristić, D. Hinić, D. Banković, A. Kočović, I. Ristić, G. Rosić, B. Ristić, D. Milovanović, V. Janjić, M. Jovanović. Levels of stress and resilience related to the COVID-19 pandemic among academic medical staff in Serbia. Psychiatry Clin. Neurosci., 2020. [DOI | PubMed]
- E. Kristoffersson, J. Boman, A. Bitar. Impostor phenomenon and its association with resilience in medical education—A questionnaire study among Swedish medical students. BMC Med. Educ., 2024. [DOI | PubMed]
- M.K. Cain, Z. Zhang, K.-H. Yuan. Univariate and multivariate skewness and kurtosis for measuring nonnormality: Prevalence, influence and estimation. Behav. Res. Methods, 2017. [DOI | PubMed]
- K.M. Mengistie, K.Z. Berhanu. Depression and substance abuse among university students. Medicine, 2025. [DOI | PubMed]
- K.J. Foli, L. Zhang, B. Reddick. Predictors of Substance Use in Registered Nurses: The Role of Psychological Trauma. West. J. Nurs. Res., 2021. [DOI | PubMed]
- T.A. Hoff, S. Heller, J.L. Reichel, A.M. Werner, M. Schäfer, A.N. Tibubos, P. Simon, M.E. Beutel, S. Letzel, T. Rigotti. Cigarette Smoking, Risky Alcohol Consumption, and Marijuana Smoking among University Students in Germany: Identification of Potential Sociodemographic and Study-Related Risk Groups and Predictors of Consumption. Healthcare, 2023. [DOI | PubMed]
- Guidelines for the Development of Chemical Impairment Policies for Medical Schools. AAMC: Leading. Serving. Advocating
- Z. Mannes, T.L. Wang, W. Ma, J. Selzer, C. Blanco. Student Substance Use Policies in US Allopathic Medical Schools. JAMA Psychiatry, 2021. [DOI | PubMed]
- K.R. Smith, N.K. Shah, A.L. Adamczyk, L.C. Weinstein, E.L. Kelly. Harm reduction in undergraduate and graduate medical education: A systematic scoping review. BMC Med. Educ., 2023. [DOI | PubMed]
- T.E. Moses, M. Chammaa, R. Ramos, E. Waineo, M.K. Greenwald. Incoming Medical Students’ Knowledge of and Attitudes Toward People with Substance use Disorders: Implications for Curricular Training. Subst. Abus., 2021. [DOI | PubMed]
- A. Bahji, M. Danilewitz, E. Guerin, B. Maser, E. Frank. Prevalence of and Factors Associated With Substance Use Among Canadian Medical Students. JAMA Netw. Open, 2021. [DOI | PubMed]
- R. Alsuhaibani, D.C. Smith, R. Lowrie, S. Aljhani, V. Paudyal. Scope, quality and inclusivity of international clinical guidelines on mental health and substance abuse in relation to dual diagnosis, social and community outcomes: A systematic review. BMC Psychiatry, 2021. [DOI | PubMed]
- A. Fachini, P.P. Aliane, E.Z. Martinez, E.F. Furtado. Efficacy of brief alcohol screening intervention for college students (BASICS): A meta-analysis of randomized controlled trials. Subst. Abus. Treat. Prev. Policy, 2012. [DOI]
- Career Guidance and Wellbeing Centre. RSU: Career Guidance and Wellbeing Centre