
How do substance and polysubstance use trajectories differ by sexual attraction from ages 17 to 24? A community-based longitudinal cohort study in Switzerland
Abstract
Introduction:
Longitudinal, population-based studies of how youth substance use (SU) varies by sexual attraction, sex and their interaction remain scarce, especially in Europe. This study examines poly-SU (PSU) trajectories at 17, 20 and 24; disparities between sexual minority (SM) youth and heterosexual (HET) youth regarding these trajectories; and their correlates.
Methods:
We obtained data from the Zurich Project on Social Development from Childhood to Adulthood. SU was self-reported by n=1384 participants at 17, 20 and 24, and hair-tested at 20 and 24. Regression models included SM status, sex, their interaction, sociodemographic variables and psychosocial variables. This population-based longitudinal cohort analysis used linear mixed-effect models to examine developmental trajectories.
Results:
The proportion of SM youth increased from 11.3% at 17 to 23.4% at 24. At 20 and 24, SM were more likely than HET youth to have used cannabis, stimulants, ecstasy and hallucinogens in the past year. At 17, SM females reported high SU, which increased until 20, then plateaued or declined by 24, approaching those of HET males. SM males exhibited lower use at 17, but this sharply increased, reaching the highest levels by 24. HET females reported the lowest use. SM females had higher tobacco use, whereas SM males showed steep increases in alcohol, cannabis and stimulant use, surpassing all other groups regarding PSU by 24. Peer SU, low self-control, sensation-seeking and internalising symptoms predicted SU-related outcomes.
Conclusions:
Our findings on distinct developmental timing of the increases and escalation in SU highlight important opportunities for public health intervention, indicating that prevention efforts should be strategically timed and tailored to the unique escalation patterns observed among SM youth.
Article type: Research Article
Keywords: Mental Health, Community Health, statistics and numerical data, Sexual Health, Drug Monitoring
Affiliations: Department of Adult Psychiatry and Psychotherapy, University Hospital of Psychiatry Zurich, University of Zurich, Zürich, Switzerland; Jacobs Center for Productive Youth Development, University of Zurich, Zürich, Switzerland; Department of Global Public Health, Karolinska Institute, Stockholm, Sweden; Swiss Aids Federation, Zürich, Switzerland; Department Public and Global Health, University of Zurich Institute of Epidemiology Biostatistics and Prevention, Zürich, Switzerland; Department of Psychology, University of Zurich, Zürich, Switzerland; Population Research Center, University of Zurich, Zürich, Switzerland; Department of Psychiatry, University Medical Centre Groningen, Groningen, Netherlands; Zurich Institute of Forensic Medicine, University of Zurich, Zürich, Switzerland; Institute of Criminology, University of Cambridge, Cambridge, UK
License: Copyright © Author(s) (or their employer(s)) 2026. Re-use permitted under CC BY. Published by BMJ Group. CC BY 4.0 This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Article links: DOI: 10.1136/bmjph-2025-003583 | PubMed: 41626608 | PMC: PMC12853546
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (4.0 MB)
Introduction
Most research on substance use (SU) among youth and young adults does not differentiate by sexual orientation. In this paper, we focus on sexual minority (SM) and heterosexual (HET) individuals across ages 17–24, capturing the transition from late adolescence (17 years) through emerging adulthood (20 years) into young adulthood (24 years). Ages 17–24 represent a key developmental window in which autonomy increases, peer contexts change and SU typically escalates and consolidates.ref. R1 Prior work in this cohort showed early emergence of SM-HET disparities but was limited to ages 17–20. We expand this evidence by adding age 24 data and modelling trajectories across the transition into young adulthood.ref. R2
Evidence indicates that SM individuals experience higher rates of SU and SU disorders than their HET counterparts (with studies typically including participants aged 18–30 years and rarely including participants younger than 18). This disparity represents a persistent public health concern. Research shows that SM adults are more than twice as likely to use illegal substancesref. R3 and develop SU disorders as compared with HET people.ref. R4 Such elevated rates have been documented across a range of substances, including tobacco,ref. R5 alcohol,ref. R7 cannabis,ref. R9 ecstasy/3,4-methylendioxymethylamphetamine (MDMAref. R10), stimulantsref. R11 and opioids.ref. R12 However, some studies suggest that the difference in alcohol use can be less pronounced.ref. R13 Furthermore, although most research on the LGBTIQ+ population has focused on men who have sex with men,ref. R14 research indicates that SM women might be at a higher risk of elevated SU.ref. R16
The disparities in SU among SM and HET seem to emerge during adolescence and young adulthood.ref. R17 Two recent Swiss population-based studies found pronounced SU differences among female SM compared with female HET, especially for cannabis, whereas no such differences were observed among males.ref. R2 At age 17, female SM reported significantly higher rates of use for cannabis, ecstasy and some hallucinogens than female HET, and by age 20, female SM reported the elevated use of tobacco, stimulants and additional hallucinogens. In contrast, male SM youth reported lower rates of use for cannabis and tobacco as compared with male HET at age 17, but significantly higher rates of use for ecstasy and hallucinogens by age 20.ref. R2 The present study builds on these prior analyses by adding an assessment at age 24, allowing us to examine whether group differences persist over time or change as the participants transition into young adulthood.
In addition to higher rates of use for individual substances, poly-SU (PSU), use of multiple substances within the past 12 months, is more common among SM than HET. SM are more likely to combine tobacco, alcohol and cannabis, whereas HET typically use tobacco and alcohol only.ref. R19 This differs from simultaneous use, which emphasises concurrent consumption in a short window. Most existing studies are cross-sectional, limiting insight into SU trajectories across adolescence and young adulthood. Moreover, changes in reported sexual attraction over time (ie, sexual fluidity) are rarely considered in longitudinal SU research.ref. R20
Sex differences within SM and HET
Rates of SU differ substantially by sex, and this further differs by SM status. Sex-based analyses indicate that female HET report lower SU rates than male HET.ref. R21 Studies in late adolescence and adult populations have found that female SM have comparable or even higher rates than male SM.ref. R4 Male SM are more likely to use cannabis, inhalants and stimulants compared with male HET, whereas female SM report the elevated use of cannabis and stimulants as compared with female HET.ref. R3 Sexualised SU, especially in chemsex (using substances to extend arousal),ref. R23 may influence use patterns in SM, though it has mainly been studied in adult male SM, with limited evidence available for adolescents or young SM individuals.ref. R24
Explaining SU disparities: psychosocial theories
Three complementary frameworks help explain the disparities in SU between SM and HET. The Minority Stress Modelref. R25 posits that SM face chronic, identity-related stress due to stigma, discrimination and marginalisation. These stressors contribute to psychological distress and increase SM’s vulnerability to using substances as a coping strategy.ref. R27 This framework is often associated with the use of substances such as alcohol, tobacco or cannabis, which are commonly used for stress relief, emotional regulation or numbing. The Syndemic Theoryref. R28 builds on this model, suggesting that co-occurring problems, such as depression and SU, mutually reinforce one another, particularly in the context of overlapping structural vulnerabilities. Together, these frameworks emphasise that both external and internalised stress, coupled with social disadvantage, may increase the risk of SU and PSU among SM. Sociocultural and peer contexts can shape SU norms among youth,ref. R29 and some LGBTQ+ (lesbian, gay, bisexual, transgender, queer and more) environments may be more substance-tolerant, particularly for men.ref. R31 These influences, together with minority stress processes, may help explain elevated SU risk among SM youth. In addition, established psychosocial factors—including peer SU, sensation seeking, self-control, emotional distress and bullying—are consistently associated with adolescent SUref. R2 and were therefore included as predictors.
The present study
Existing studies, predominantly from the USA, show higher SU among SM youth, but offer limited guidance for European contexts. Longitudinal, population-based studies on SM-HET SU disparities in Europe are scarce, and most prior work is cross-sectional. Few studies combine repeated self-reports with biological markers such as hair toxicology to address reporting biases.ref. R33 This study is among the first in Switzerland to examine SU and PSU trajectories among SM youth using longitudinal data and comprehensive psychosocial predictors.
To address these gaps, we use longitudinal data obtained from a Swiss community-based cohortref. R34 to investigate SU among HET and SM at ages 17, 20 and 24, the transition from late adolescence into young adulthood, allowing for examining SU disparities across this critical developmental period. In this study, we use the term ‘SM’ to refer to people reporting any level of same-sex attraction. Please note, however, that sexual attraction, behaviour and sexual orientation are correlated but distinct constructs.ref. R35 SU was assessed through self-reports at all three time points, with additional hair test data available at ages 20 and 24 to complement the survey responses.
The study had four main objectives. First, we examined the development of sexual attraction from ages 17 to 24. Rather than assuming changes in reported attraction reflect actual sexual fluidity, we conceptualise such shifts as indicative of developmental processes of identity disclosure (‘coming out’), consistent with prior literature showing that awareness of sexual orientation precedes self-identification,ref. 37ref. 39 making it likely that classification changes from HET to SM. Additionally, sexuality can be fluid over time, and sexual diversity develops through dynamic processes rather than being rigid or categorical.ref. R40 We therefore expect that some participants may report changes in their attraction across assessment waves and account for these reported changes at each time point (To evaluate whether time-varying sexual orientation may bias results, we further conducted additional sensitivity analyses using baseline-only (age 17) and time-invariant (‘ever SM’) operationalisations of sexual orientation. These analyses supported the robustness of the main findings.). Second, we compared SM and HET youth regarding psychosocial stressors, expecting that SM would report higher levels, due to experiences of discrimination and marginalisation.ref. R26 Third, we investigated substance-specific SU and PSU trajectories across SM status, sex and their interaction, anticipating consistently higher levels among SM and potential interaction effects.ref. R2 Fourth, we examined whether psychosocial stressors predict SU trajectories and help explain observed group disparities, expecting that stressors particularly relevant to SM would significantly predict elevated SU.ref. R2 Finally, as an exploratory step, we compared self-reported SU data with objective hair data (ages 20 and 24) to assess concordance and support the validity of participants’ reported SU trajectories, though hair data were not used in inferential models due to sample size limitations.ref. R31
Materials and methods
Recruitment and participants
Participants were drawn from the Zurich Project on Social Development from Childhood to Adulthood (z-prosoref. R34), an ongoing longitudinal cohort study initiated in 2004. The original target sample comprised 1675 participants from 56 primary schools in the city of Zurich, selected through stratified random sampling to ensure representation across various socioeconomic backgrounds. Across all assessment waves, data were obtained from 1583 participants (94.5% of the initial sample), each contributing information at least once at nine main data waves, either directly or through another informant. The current analysis focuses on SU data collected at waves 7–9, corresponding to ages 17, 20 and 24, with a few additional constructs measured at earlier waves. We refer to the three assessment ages as late adolescence (17 years), emerging adulthood (20 years) and young adulthood (24 years). Participants were included if they provided at least one valid data point on sexual attraction and SU across these waves (n=1384). Sample retention was high (95.6% at 17, 88.1% at 20, 84.2% at 24, see online supplemental table S1). All data used in this study were pseudonymised before analysis and stored separately from identifying information, which is not accessible to users of the data. Data, including information on sexual attraction, were collected through secure electronic questionnaires, and confidentiality was ensured according to Swiss data protection standards. As the study uses fully pseudonymised cohort data and contains no identifiable individuals or case details, patient consent for publication was not required.
Measures
Please refer to online supplement for detailed or additional information on all measures.
Past-year SU frequency for tobacco, alcohol, cannabis, ecstasy/MDMA, stimulants such as cocaine and (meth-)amphetamine, hallucinogens, benzodiazepines and opioids was assessed at ages 17, 20 and 24 using standard 6-point frequency scales (details in online supplement).ref. R43 For the hair data, participants provided samples at ages 20 and 24, as objective indicators of SU. Analytical procedures and detection thresholds are reported in online supplement.ref. R44 PSU variables were operationalised using three indices (Poly1–3) reflecting different substance groupings across waves (details in online supplement).ref. R32 Sexual attraction was self-reported at each wave, using a 5-point scale. Individuals indicating any same-sex attraction were classified as SM, others were classified as HET (details in online supplement). Sociodemographic variables included sex assigned at birth, parental migration background, family socioeconomic status (SES) (international socio-economic index (ISEI)ref. R46) and educational level.ref. R32 Coding details and distributions are provided in online supplement. Psychosocial and behavioural variables were selected based on their established associations with adolescent and young adult SU and related problem behaviours,ref. R17 and to align with previous analyses conducted with the same cohort.ref. R2 Peer SU,ref. R47 sensation-seeking,ref. R48 low self-control,ref. R50 internalising symptoms,ref. R51 bullying victimisationref. R52 and leisure activitiesref. R47 were assessed using validated scales. Information on items, reliability coefficients, coding and wave-specific availability is detailed in online supplement.
Statistical analysis
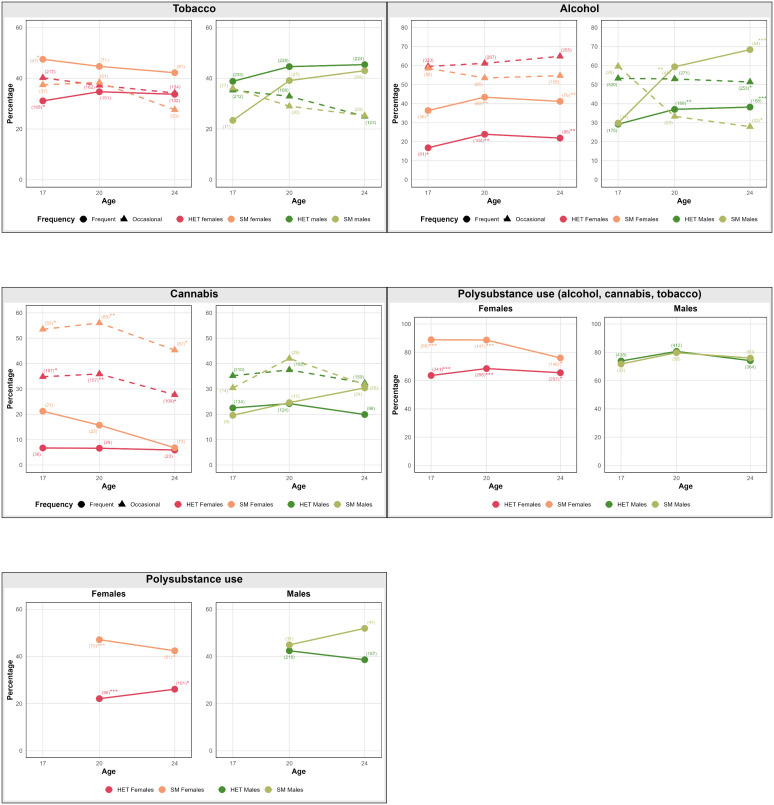
We conducted descriptive and longitudinal analyses of SU trajectories at ages 17, 20 and 24. Trajectory graphs illustrated changes in prevalence over time, and z-tests for proportions tested group differences at each time point (*p<0.05, **p<0.01, ***p<0.001). High-prevalence substances (tobacco, alcohol and cannabis) were categorised into frequent (ie, weekly or (almost) daily use) and occasional use (ie, less than weekly use) to provide a nuanced depiction of use patterns. Any other substance (ie, ecstasy, (meth-)amphetamines, cocaine, stimulants, hallucinogens, opioids and benzodiazepines) was coded as a binary (use vs no use) due to lower prevalence (figure 1; online supplemental figures 1 and 2a–c). To model developmental trajectories, we used linear mixed-effects models with repeated measures nested within individuals. Missing data were not imputed. However, linear mixed-effects models were estimated using restricted maximum likelihood, allowing the inclusion of all available observations per participant. Age was entered as a continuous variable (linearly and quadratically) to capture curvilinear patterns.ref. R53 Substances assessed at only two waves (benzodiazepines, opioids, poly 3) were analysed linearly. No formal corrections for multiple testing were applied, as analyses were exploratory. Effect sizes and estimates (β, SE and 95% CI where applicable) were reported consistently. Interaction effects (sex×sexual attraction) were tested for each substance and PSU category. Models were built stepwise: (1) baseline (age, sexual attraction, sex), (2) sociodemographic (adding migration background, ISEI, education) and (3) full model (adding psychosocial/behavioural predictors described above). Interaction effects (sex×sexual attraction) were interpreted using model coefficients and visualised via predicted trajectories. No formal contrast testing was conducted, as analyses were exploratory and primarily descriptive. Hair toxicology data were not included in statistical models, due to limited availability and convergence issues; however, they were analysed descriptively to validate self-reported SU patterns across groups (see figures2 3). Analyses were conducted in R V.4.2.2ref. R54 using psych,ref. R55 tidyverse,ref. R56 rstatix,ref. R57 ggplot2,ref. R58 lme4ref. R59 and lmerTest.ref. R60
Patient and public involvement
This research was conducted without patient or public involvement and was not pre-registered. We followed the Strengthening the Reporting of Observational Studies in Epidemiology statement for the reporting of observational studies.ref. R61
Results
Sample characteristics and sexual attraction changes
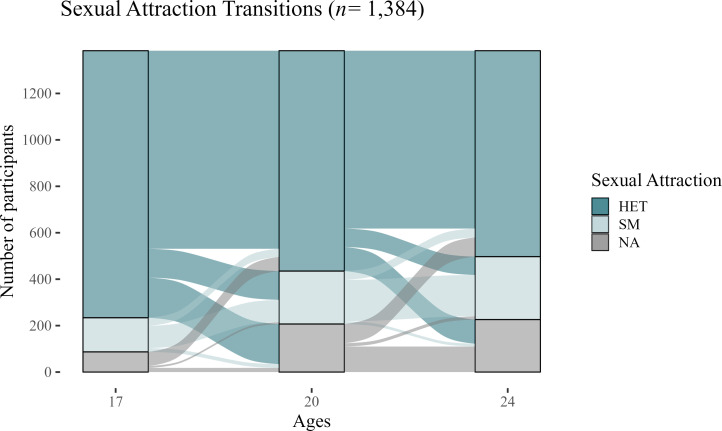
Between ages 17 and 24, the prevalence of SM increased from 11.3% at age 17 (n=147/1297; females 15.5%, males 7.2%) to 23.4% at age 24 (n=271/1158), indicating sexual attraction fluidity (figure 4, online supplemental table S1). Women consistently reported higher rates of same-sex attraction compared with men across all waves (age 24: females 32.8%, males 13.8%).
Group differences in sociodemographic and psychosocial characteristics are summarised in online supplemental table S1. Although raw group comparisons showed only small variations in SES, education and migration background, regression models revealed more consistent patterns, particularly for migration background. Psychosocially, SM youth reported higher internalising symptoms, more bullying victimisation (especially among males at age 17), and greater exposure to substance-using peers compared with HET youth, particularly at age 20. Other variables, such as sensation-seeking, self-control and engagement in leisure activities, showed minor or inconsistent differences across groups.
Longitudinal trajectories of SU
Trajectories of self-reported SU differed notably between SM and HET (figure 1, online supplemental S1) and between females and males (online supplemental figure S2a–c). SM youth, particularly SM females during late adolescence and SM males in early adulthood, consistently reported higher levels of use compared with their HET peers. While SM females reported elevated SU as early as age 17, with patterns stabilising or slightly declining by age 24, SM males exhibited comparatively lower use at 17 but showed a marked increase between ages 20 and 24, ultimately surpassing all other groups by young adulthood. In contrast, HET females consistently reported the lowest levels across substances and time. Frequent use increased more sharply over time than occasional use, particularly among males. SM females maintained the highest levels of tobacco use from adolescence onward, whereas SM males showed a strong increase in alcohol, cannabis and stimulant use across time. For cannabis, female SM youth initially reported the highest occasional use, but their levels declined by age 24, whereas SM males became increasingly frequent users over time. Similar trajectories were observed for ecstasy/MDMA and other stimulant substances, with SM males showing the steepest increase by age 24. For benzodiazepine and opioid use, sex differences were more pronounced than SM status differences, with females reporting higher levels than males overall. Regarding PSU, SM females showed the highest levels of combined tobacco, alcohol and cannabis use (Poly1), whereas SM males had the steepest increase in broader PSU categories (Poly2 and Poly3), reaching the highest levels by age 24.
Predictors of SU and PSU
Baseline regression analyses confirmed significant differences between SM and HET youth across multiple substances, including alcohol, cannabis, ecstasy/MDMA, stimulants, cocaine, (meth-)amphetamines, hallucinogens and PSU categories (online supplemental table S2a). Interaction terms between sex and sexual attraction at baseline indicated significantly higher vulnerability among SM females compared with males. Specifically, significant sex×sexual attraction interactions were observed for tobacco, alcohol, cannabis, ecstasy/MDMA and all PSU categories. These interactions consistently highlighted elevated SU, specifically among SM females relative to males (figure 5, online supplemental table S2b).
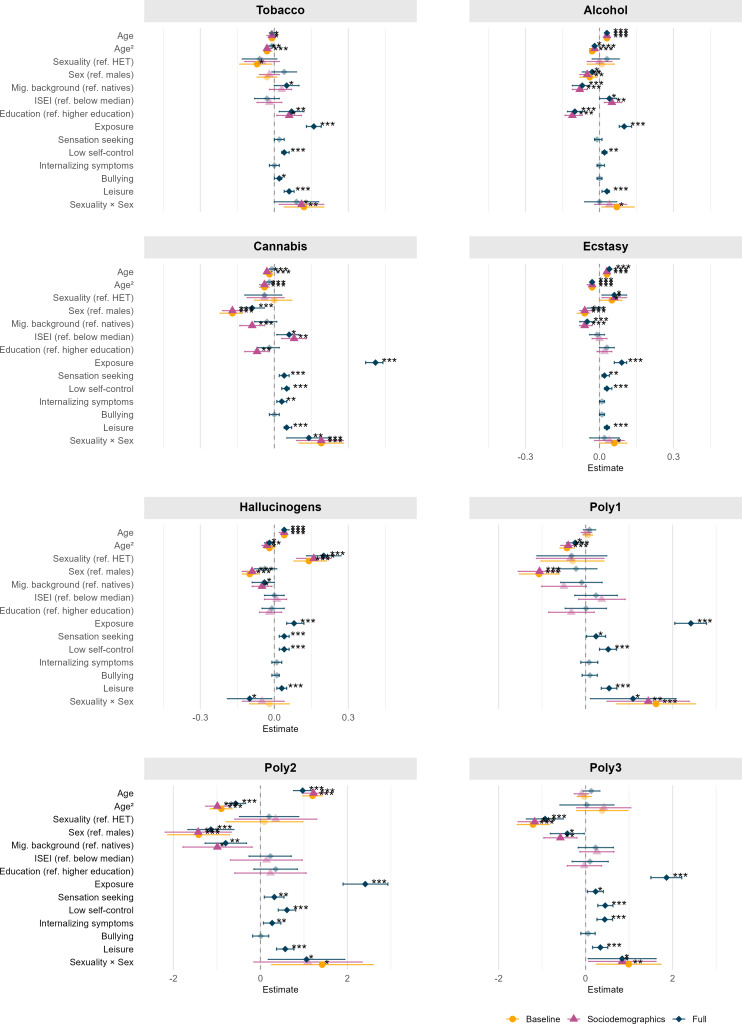
After adjusting for sociodemographic covariates (including parental migration background, SES and educational background), SM status remained a robust predictor of elevated SU for most substances. Socioeconomic indicators demonstrated variable significance: parental migration background generally predicted lower SU, whereas higher educational attainment was associated with differentially elevated SU depending on the specific substance (online supplemental table S3a). In the sociodemographic-adjusted models, significant interaction terms between sex and sexual attraction persisted for several substances, confirming that SM females remain particularly vulnerable even after accounting for socioeconomic background. Notably, significant sex×sexual attraction interactions were identified for tobacco and cannabis, and the polysubstance categories, Poly 1 and Poly 3 (figure 5, online supplemental table S3b).
When including all sociodemographic and psychosocial covariates, SM status continued to be a significant predictor of increased SU across most substances and polysubstance categories. Psychosocial factors also showed strong, consistent associations. Higher sensation-seeking scores significantly predicted increased SU across most substances and polysubstance categories. Elevated internalising symptoms consistently emerged as significant associations, emphasising the role of emotional distress in SU among adolescents and young adults. Additionally, the influence of peers on SU-related behaviours was a robust and significant predictor across nearly all substances, further underscoring the influence of peers on substance-related behaviours (online supplemental table S4a). In the fully adjusted models, significant interactions between sex and sexual attraction persisted, most notably for cannabis, hallucinogens and all PSU categories (figure 5, online supplemental table S4b). An overview of significant associations for the final interaction model is provided in online supplemental table S4c.
Prevalence of self-reported and hair-assessed SU at ages 20 and 24
In addition to the longitudinal trajectories, we examined self-reported and hair-assessed SU at ages 20 and 24. These analyses provided a more detailed picture of SU patterns, including substances not assessed at age 17, and allowed for cross-validation of self-reported data through hair testing. However, further statistical analyses of predictors were not stable due to the limited availability of hair data at only two time points.
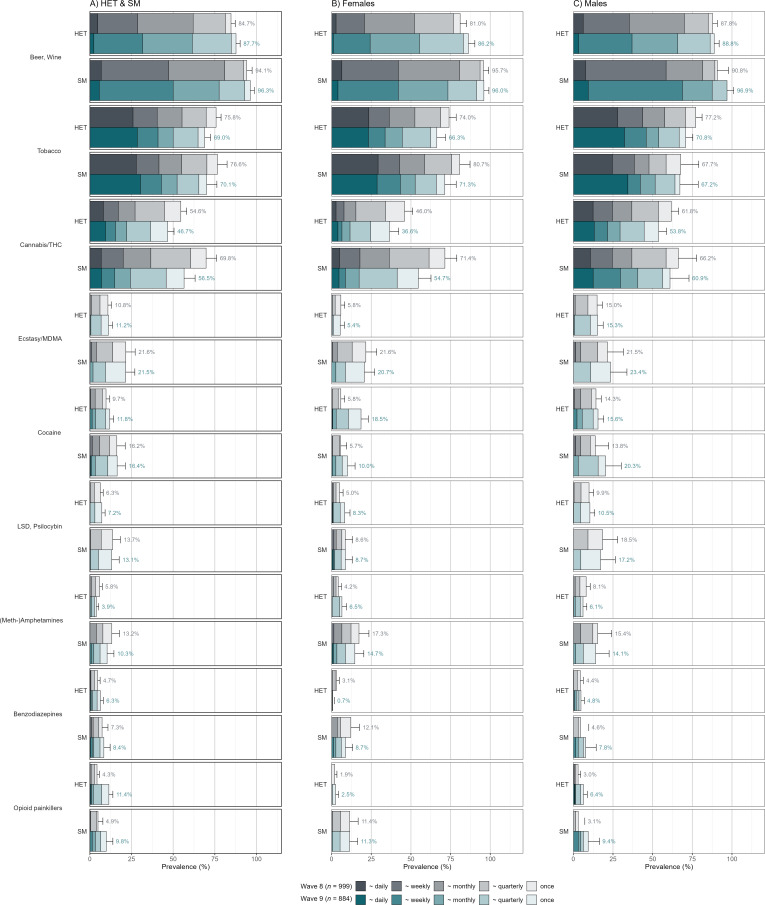
The 12-month self-reported prevalence rates revealed significant disparities between SM and HET youth at ages 20 and 24. SM consistently reported higher prevalence rates across most substances, notably THC (Δ9-tetrahydrocannabinol, the primary psychoactive component of cannabis measured in hair), ecstasy/MDMA, stimulants (including cocaine and (meth-)amphetamines) and hallucinogens (figure 2).
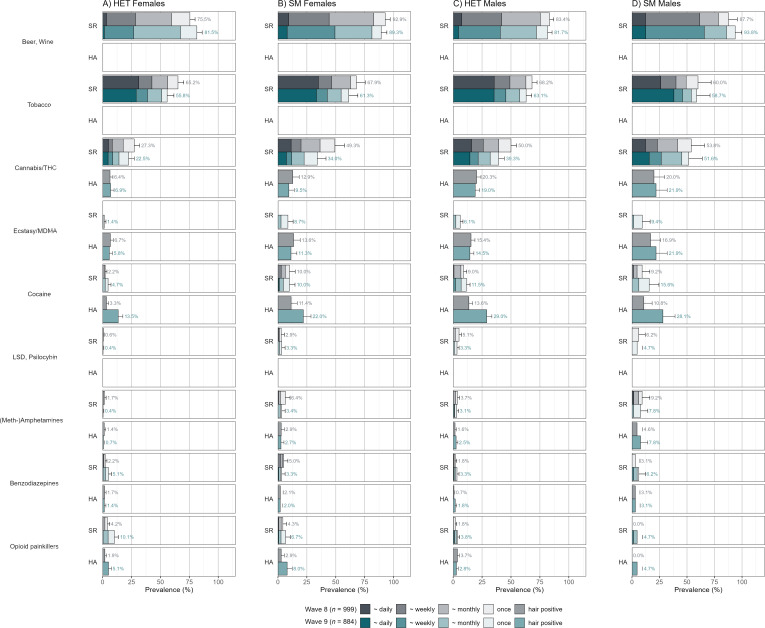
Notably, THC can only be reliably detected in hair from individuals with frequent or heavy cannabis use, limiting its sensitivity for occasional users.ref. R62 Disparities between SM and HET were pronounced for stimulants and MDMA, substances typically associated with recreational nightlife contexts. In hair analysis, disparities in the 3-month prevalence of substances were further accentuated, especially for substances associated with greater social stigma. SM and HET youth displayed higher hair-analysed prevalence rates for stimulants (eg, cocaine, amphetamines) and prescription opioids compared with self-reported data, suggesting systematic underreporting biases among SM in self-reported measures (figure 3), as seen in previous studies of youth.ref. R42
Discussion
This study tracked SU and PSU trajectories from ages 17 to 24 among SM and HET youth in a large urban Swiss cohort. SM youth, particularly females in adolescence and males in early adulthood, consistently reported higher SU than HET peers, with disparities widening over time. Frequent use of tobacco, alcohol, cannabis and party drugs (eg, ecstasy/MDMA, stimulants) increased notably among SM youth, and PSU was most prevalent among SM females, especially for combined alcohol, cannabis and tobacco use. These findings highlight the developmental nature of SU disparities and underscore critical timing windows for targeted prevention, earlier for SM females and later for SM males.
Developmental timing and trajectory differences
The distinct developmental trajectories suggest that SU disparities among SM evolve dynamically across adolescence and early adulthood. In female SM, elevated SU risk was already evident by age 17 and remained high, whereas male SM showed a delayed but sharp increase in SU, particularly between ages 20 and 24. These diverging patterns may reflect differences in identity development timelines and community integration. For instance, gendered social norms may shape how and when youth disclose or act on same-sex attraction. Among male SM, stronger stigma and social pressure may contribute to underreporting or later outward expression, potentially delaying engagement with LGBTQ+ communities. In contrast, SM females may differentiate earlier from HET peers, leading to earlier SU increases, similar to HET males. By ages 20 and 24, participation in LGBTQ+ nightlife and peer networks may further amplify SU, particularly among male SM in urban settings like Zurich. Although some studies suggest similar or even earlier identity development among SM males (eg,ref. R64 the timing and social context of disclosure and community engagement likely vary by gender, setting, culture and geographic location).
Psychosocial mechanisms
Findings indicating elevated SU among SM youth align with the Minority Stress theory,ref. R25 which posits that chronic stigma increases psychological distress and vulnerability to SU. Indeed, SM in this study reported higher levels of internalising symptoms and bullying victimisation compared with HET youth, which may link minority status to SU. The results also resonate with the Syndemic Theory,ref. R28 particularly the co-occurrence of psychosocial vulnerabilities and elevated PSU among SM. This suggests a cumulative risk process in which co-occurring adversities interact to amplify health risks.
Sociocultural environment
At the same time, our findings extend beyond stress-based models. Elevated stimulant, ecstasy/MDMA and PSU among SM, particularly females, support emerging sociocultural perspectives that conceptualise SU as embedded in community norms, nightlife practices and identity expression.ref. R65 In urban contexts, such as Zurich, SU is often embedded in recreational and social settings. Queer-coded spaces, particularly those tied to electronic music and techno culture, with their longstanding association with SM communities, may represent settings where substances are more tolerated or accessible for some individuals, although practices vary widely across LGBTQ+ spaces. This aligns with research indicating that social and cultural environments, including peer norms, nightlife participation and community-based identity expression, can influence SU among SM populations. Large-scale events such as the Street Parade and Zurich Pride reflect the visibility and diversity of these intersecting scenes. For some, SU may serve as a coping mechanism as well as a means of social integration or enhancing intimacy, consistent with observations of sexualised SU and chemsex practices, particularly among men having sex with men.ref. R66
Furthermore, the political context needs to be taken into account. In Switzerland, SMs still face significant prejudice and discrimination.ref. R38 However, SM is generally widely accepted and protected by Swiss law. In contrast, more than 60 countries criminalise SM,ref. R67 which may increase risky SU among SM populations. Additionally, legal access to certain substances during adolescence and early adulthood may also influence developmental trends in SU. Alcoholic beverages with <16% alcohol (eg, beer and wine) and tobacco products are legally purchasable from age 16, whereas spirits are available from age 18 onwards. Previous research has shown that a substantial proportion of adolescents tries substances a year before they can legally buy them.ref. R43 Cannabis remains illegal for recreational use (<1% THC), although public debate and tolerance practices are ongoing.ref. R68 These regulatory conditions shape availability and social acceptance, particularly from age 16 onward, and should be considered when interpreting age-related increases in SU.
This framework also contextualises our PSU findings. High PSU among SM females highlights a high-risk profile not fully captured by single-substance models.ref. R32 These patterns reinforce the need for public health approaches that recognise both the individual vulnerabilities and respect the sociocultural contexts that shape SU behaviour among SM. Furthermore, the high SU observed among female SM indicates that services targeting queer females (and non-binary youth) are necessary, and that studies on LGBTIQ+ populations should become more inclusive of understudied populations within the community.ref. R14
Finally, hair toxicology data at ages 20 and 24 among a subsample of participants provided a valuable lens for validating self-reported SU patterns. The objective SU data largely confirmed trends observed in self-reports, but also revealed higher prevalence rates for substances typically underreported due to stigma, such as opioids and stimulants.ref. R42 Although the sample size for hair data was smaller, it offered crucial methodological triangulation and supports future integration of objective measures in SU research.
Strengths and limitations
Several key strengths can be addressed. First, this study draws on longitudinal data spanning from late adolescence to early adulthood, a period during which SU patterns unfold. The use of these three assessment waves for most self-reported measures allowed for detailed trajectory modelling and subgroup comparisons based on sexual attraction and sex. Second, the study included a large urban community sample assessing SU among both HET and SM, enabling robust analyses of the effect of SM status, sex and their intersection, which are rarely feasible in general population cohorts. Third, self-reported SU was complemented with objective hair toxicology among a subset of participants, enhancing the validity of findings and addressing concerns about potential reporting biases. Finally, including multiple psychosocial predictors allowed for nuanced exploration of underlying risk mechanisms.
However, the study also has several limitations. First, SM status was assessed via sexual attraction only, without additional indicators such as sexual identity or behaviour. Because attraction, behaviour and identity are distinct constructs, this underrepresents the complexity of SM status. Moreover, the study did not directly ask participants about their sexual orientation, which may have excluded or misclassified individuals with identities (eg, asexual, or those primarily attracted to non-binary or transgender people). We further did not distinguish between mono- and plurisexual SM. Yet, Swiss data reveal that plurisexual individuals face more discrimination and receive less support, both from inside and outside the LGBTIQ+ community.ref. R69 Furthermore, changes in reported attractions across waves may reflect identity disclosure, since the coming out process often occurs during this age range,ref. R38 potentially leading to some misclassification. Second, the male SM subgroup was relatively small, particularly in early waves, which may limit statistical power. Underreporting of SM identification due to social stigma is quite common.ref. R70 Given that societal norms towards male same-sex attraction are more negative than compared with female same-sex attraction,ref. R71 underreporting might have been more pronounced among male participants. Third, the present study assessed sex in a binary fashion, without distinguishing between sex and gender. We further did not assess transgender and intersex status. As a result, gender-diverse and intersex individuals may be underrepresented or misclassified. Future studies should go beyond the sex and gender binary and also assess people’s transgender status, aiming to be more inclusive of people who fall outside of the sex and/or gender spectrum.ref. R14 Fourth, the legal and social acceptance of SM varies dramatically across countries, with more than 60 nations still criminalising SM people.ref. R67 However, the vast majority of research is conducted in relatively tolerant Western countries.ref. R14 To better understand how context influences the experiences of SM people, future research should intensify efforts to collect data from Africa, Asia and Central America, while prioritising the safety of the involved scholars and participants. Fifth, hair toxicology data were only available at ages 20 and 24, and not all participants provided samples, limiting representativeness. Women and those with a migration background were less likely to participate (see ref. R74 for details). Additionally, due to the limited number of valid hair samples, particularly among SM males, models using hair data as outcomes did not converge for less common substances, and hair concentrations were therefore used only to support the validity of self-reported SU. Sixth, SU is always highly context-specific. This study focuses on youth in an urban Swiss context with specific cultural and structural characteristics, limiting its generalisability particularly to rural settings, non-European contexts, or populations with differing legal, cultural or structural conditions related to SU and sexuality. Finally, although psychosocial factors were included, minority stress-specific variables were not explicitly measured, which limits the ability to formally test theoretical frameworks.
Implications for prevention, intervention and future research
Elevated SU emerges by age 17 among female SMs and rises sharply among male SM in early adulthood, highlighting the need for targeted, developmentally sensitive prevention and intervention strategies. Efforts should focus on school-based programmes during critical transition periods and span multiple settings: schools, youth services, primary care, and, where appropriate, LGBTQ+ community spaces or nightlife-based harm-reduction initiatives address not only SU but also underlying psychosocial factors, including emotional distress and peer influence. Inclusive, identity-sensitive approaches are essential. Because SM youth often anticipate rejection,ref. R75 educators, parents and peers should actively communicate acceptance and support, fostering safer, more affirming environments that reduce vulnerability and promote healthy development.
Future research should aim to more directly assess the structural and cultural mechanisms hypothesised to underlie SU disparities, ideally in large, representative cohort studies and possibly include earlier timepoints.ref. R13 Cross-cultural comparisons could help understand whether similar patterns arise in different policy or social environments and assess mechanisms more directly, such as minority stress pathways or access to community resources. In addition, studies should move beyond damage-centred frameworks by also highlighting protective and community-based factors, such as resilience, social support and inclusive environments.ref. R76 Stronger intersectional designs are needed to better capture diversity within sexual and gender minority groups, as studies have shown differences, for example, between lesbian and bisexual women regarding their SUref. R77 as well as among transgender and gender-diverse individuals, who may have a range of sexual orientations.ref. R78
Conclusion
This study provides a longitudinal investigation of SU disparities between SM and HET youth in a European context, tracking developmental trajectories from adolescence into early adulthood. The findings reveal persistent and, in some cases, widening disparities in SU and PSU between SM and HET, particularly among females. These disparities were not fully explained by established psychosocial risk factors, underscoring the importance of considering minority-specific stressors and sociocultural influences. This study highlights the need for timely, tailored, culturally and contextually sensitive prevention efforts by integrating objective biomarkers and examining subgroup-specific patterns over time. These findings provide actionable evidence for tailoring early intervention and harm-reduction strategies to SM youth, with attention to sex-specific developmental timing and integration across school, healthcare and community settings.
Supplementary Materials
References
- JJ Arnett. Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 2000. [DOI | PubMed]
- F Vock, L Johnson-Ferguson, L Bechtiger. Substance use in sexual minority youth: prevalence in an urban cohort. Child Adolesc Psychiatry Ment Health, 2023. [DOI | PubMed]
- G Medley, RN Lipari, J Bose. Sexual orientation and estimates of adult substance use and mental health: Results from the 2015 National Survey on Drug Use and Health. NSDUH Data Rev, 2016
- BT Kerridge, RP Pickering, TD Saha. Prevalence, sociodemographic correlates and DSM-5 substance use disorders and other psychiatric disorders among sexual minorities in the United States. Drug Alcohol Depend, 2017. [DOI | PubMed]
- JR Blosnich, GW Farmer, JGL Lee. Health Inequalities Among Sexual Minority Adults. Am J Prev Med, 2014. [DOI | PubMed]
- MS Schuler, CE Rice, RJ Evans-Polce. Disparities in substance use behaviors and disorders among adult sexual minorities by age, gender, and sexual identity. Drug Alcohol Depend, 2018. [DOI | PubMed]
- JL Allen, O Mowbray. Sexual orientation, treatment utilization, and barriers for alcohol related problems: Findings from a nationally representative sample. Drug Alcohol Depend, 2016. [DOI | PubMed]
- JN Fish, TL Hughes, ST Russell. Sexual identity differences in high-intensity binge drinking: findings from a US national sample. Addiction, 2018. [DOI | PubMed]
- JE Parnes, WJ Kiekens, EH Mereish. LGBT-THC: A Systematic Review of Psychosocial Mechanisms Linking Minority Stressors and Cannabis Use among Sexual and Gender Minoritized Individuals. Curr Addict Rep, 2024. [DOI | PubMed]
- M Griffin, D Callander, DT Duncan. Differential Risk for Drug Use by Sexual Minority Status among Electronic Dance Music Party Attendees in New York City. Substance Use & Misuse, 2020. [DOI | PubMed]
- B Rosner, J Neicun, JC Yang. Substance use among sexual minorities in the US – Linked to inequalities and unmet need for mental health treatment? Results from the National Survey on Drug Use and Health (NSDUH. J Psychiatr Res, 2021. [DOI | PubMed]
- DT Duncan, S Zweig, HR Hambrick. Sexual Orientation Disparities in Prescription Opioid Misuse Among U.S. Adults. Am J Prev Med, 2019. [DOI | PubMed]
- JN Fish, MD Bishop, ST Russell. Developmental Differences in Sexual Orientation and Gender Identity–Related Substance Use Disparities: Findings From Population-Based Data. J Adolesc Health, 2021. [DOI | PubMed]
- T Hässler, NT Fogwell, A Gonzalez. Reimagining LGBTIQ+ research – Acknowledging differences across subpopulations, methods, and countries. J Soc Issues, 2024. [DOI]
- A Klysin. Conducting research within the acronym: Problematizing LGBTIQ+ research in psychology. J Soc Issues, 2024. [DOI]
- JD Kidd, KB Jackman, M Wolff. Risk and Protective Factors for Substance Use Among Sexual and Gender Minority Youth: a Scoping Review. Curr Addict Rep, 2018. [DOI | PubMed]
- MP Marshal, MS Friedman, R Stall. Sexual orientation and adolescent substance use: a meta‐analysis and methodological review*. Addiction, 2008. [DOI | PubMed]
- S Lucia, S Stadelmann, M Amiguet. Enquêtes populationnelles sur la victimisation et la délinquance chez les jeunes dans les canton de vaud et zurich: les jeunes non-exclusivement hétérosexuel∙le∙s: populations davantage exposées?. 2017
- J Lee, RJ Evans-Polce, J Ahlquist. Polysubstance use by sexual identity among US adults, 2021. Prev Med, 2023. [DOI | PubMed]
- SL Katz-Wise, KP Todd. The current state of sexual fluidity research. Curr Opin Psychol, 2022. [DOI | PubMed]
- JN Fish, K Pasley. Sexual (Minority) Trajectories, Mental Health, and Alcohol Use: A Longitudinal Study of Youth as They Transition to Adulthood. J Youth Adolesc, 2015. [DOI | PubMed]
- D Demant, L Hides, DJ Kavanagh. Differences in substance use between sexual orientations in a multi-country sample: findings from the Global Drug Survey 2015. J Public Health, 2016. [DOI]
- D Stuart. Chemsex: origins of the word, a history of the phenomenon and a respect to the culture. DAT, 2019. [DOI]
- J Hakim. The rise of chemsex: queering collective intimacy in neoliberal London. Cultural Studies, 2019. [DOI]
- VR Brooks. Minority Stress and Lesbian Women, 1981
- IH Meyer. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull, 2003. [DOI | PubMed]
- C Zhang, S Qiao, W Chang. Applying an Intersectional Approach to Examine the Associations between Sexual Minority Stressors, Resilience, and Substance Misuse Disparities among a National Sample of Sexual Minority Populations, 2025
- M Singer. Introduction to Syndemics: A Critical Systems Approach to Public and Community Health, 2009
- M Frese. Cultural Practices, Norms, and Values. J Cross Cult Psychol, 2015. [DOI]
- R Room. Stigma, social inequality and alcohol and drug use. Drug Alcohol Rev, 2005. [DOI | PubMed]
- JJ Palamar, A Salomone, E Gerace. Hair testing to assess both known and unknown use of drugs amongst ecstasy users in the electronic dance music scene. Int J Drug Policy, 2017. [DOI | PubMed]
- A Steinhoff, L Bechtiger, D Ribeaud. Polysubstance Use in Early Adulthood: Patterns and Developmental Precursors in an Urban Cohort. Front Behav Neurosci, 2021. [DOI | PubMed]
- JJ Palamar, A Salomone, KM Keyes. Underreporting of drug use among electronic dance music party attendees. Clin Toxicol (Phila), 2021. [DOI | PubMed]
- D Ribeaud, A Murray, L Shanahan. Cohort Profile: The Zurich Project on the Social Development from Childhood to Adulthood (z-proso). J Dev Life Course Criminol, 2022. [DOI | PubMed]
- T Fu, D Herbenick, B Dodge. Relationships Among Sexual Identity, Sexual Attraction, and Sexual Behavior: Results from a Nationally Representative Probability Sample of Adults in the United States. Arch Sex Behav, 2019. [DOI | PubMed]
- E Mishel. Intersections between Sexual Identity, Sexual Attraction, and Sexual Behavior among a Nationally Representative Sample of American Men and Women. J Off Stat, 2019. [DOI]
- B Mustanski, L Kuper, GJ Greene. APA Handbook of Sexuality and Psychology, 2014
- L Eisner, T Hässler. Swiss lgbtiq+ survey 2019: summary report. PsyArXiv, 2019. [DOI]
- EK Layland, R Bränström, GR Murchison. Kept in the Closet: Structural Stigma and the Timing of Sexual Minority Developmental Milestones Across 28 European Countries. J Youth Adolesc, 2023. [DOI | PubMed]
- LM Diamond. Sexual Fluidity in Male and Females. Curr Sex Health Rep, 2016. [DOI]
- DM Frost, IH Meyer. Minority stress theory: Application, critique, and continued relevance. Curr Opin Psychol, 2023. [DOI | PubMed]
- C Janousch, L Eggenberger, A Steinhoff. Words versus Strands: Reliability and Stability of Concordance Rates of Self-Reported and Hair-Analyzed Substance Use of Young Adults over Time. Eur Addict Res, 2024. [DOI | PubMed]
- BB Quednow, A Steinhoff, L Bechtiger. High Prevalence and Early Onsets: Legal and Illegal Substance Use in an Urban Cohort of Young Adults in Switzerland. Eur Addict Res, 2022. [DOI | PubMed]
- C Scholz, J Cabalzar, T Kraemer. A Comprehensive Multi-Analyte Method for Hair Analysis: Substance-Specific Quantification Ranges and Tool for Task-Oriented Data Evaluation. J Anal Toxicol, 2021. [DOI | PubMed]
- C Scholz, MM Madry, T Kraemer. LC-MS-MS Analysis of Δ9-THC, CBN and CBD in Hair: Investigation of Artifacts. J Anal Toxicol, 2022. [DOI | PubMed]
- HBG Ganzeboom, PM De Graaf, DJ Treiman. A standard international socio-economic index of occupational status. Soc Sci Res, 1992. [DOI]
- z-proso Handbook: Instruments and Procedures in the Adolescent and Young Adult Surveys (Age 11 to 24; Waves K4-K9). 2024. [DOI]
- FD Alsaker, E Gutzwiller-Helfenfinger. Handbook of School Bullying. An International Perspective, 2010
- AL Murray, M Eisner, I Obsuth. Identifying Early Markers of “Late Onset” Attention Deficit and Hyperactivity/Impulsivity Symptoms. J Atten Disord, 2020. [DOI | PubMed]
- HG Grasmick, CR Tittle, RJ Bursik. Testing the Core Empirical Implications of Gottfredson and Hirschi’s General Theory of Crime. Journal of Research in Crime and Delinquency, 1993. [DOI]
- AL Murray, I Obsuth, M Eisner. Evaluating Longitudinal Invariance in Dimensions of Mental Health Across Adolescence: An Analysis of the Social Behavior Questionnaire. Assessment, 2019. [DOI | PubMed]
- AL Murray, M Eisner, D Ribeaud. Validation of a Brief Self-Report Measure of Adolescent Bullying Perpetration and Victimization. Assessment, 2021. [DOI | PubMed]
- M Wicki, S Marmet, J Studer. Curvilinear associations between sexual orientation and problematic substance use, behavioural addictions and mental health among young Swiss men. Addict Behav, 2021. [DOI | PubMed]
- R: a language and environment for statistical computing. 2023
- W Revelle. Psych: procedures for personality and psychological research. r package version 2.4.6. 2024
- H Wickha. Welcome to the Tidyverse. J Open Source Softw, 2019. [DOI]
- A Kassambara. Statix: pipe-friendly framework for basic statistical tests
- H Wickham. Use R!, 2016
- D Bates, M Mächler, B Bolker. Fitting Linear Mixed-Effects Models Using lme4. J Stat Softw, 2015. [DOI]
- A Kuznetsova, PB Brockhoff, RHB Christensen. lmerTest Package: Tests in Linear Mixed Effects Models. J Stat Soft, 2017. [DOI]
- JP Vandenbroucke, E von Elm, DG Altman. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). Epidemiology (Sunnyvale), 2007. [DOI]
- A Steinhoff, L Shanahan, L Bechtiger. When Substance Use Is Underreported: Comparing Self-Reports and Hair Toxicology in an Urban Cohort of Young Adults. Journal of the American Academy of Child & Adolescent Psychiatry, 2023. [DOI | PubMed]
- M Taylor, R Lees, G Henderson. Comparison of cannabinoids in hair with self‐reported cannabis consumption in heavy, light and non‐cannabis users. Drug Alcohol Rev, 2017. [DOI | PubMed]
- RC Savin-Williams, LM Diamond. Sexual identity trajectories among sexual-minority youths: gender comparisons. Arch Sex Behav, 2000. [DOI | PubMed]
- K Pienaar, DA Murphy, K Race. Drugs as technologies of the self: Enhancement and transformation in LGBTQ cultures. International Journal of Drug Policy, 2020. [DOI | PubMed]
- J Sun, B She, PM Latt. Comparing the impact of sexualised drug use with and without chemsex on sexual behaviours among men who have sex with men in China: a national multi-site cross-sectional study. Sex Health, 2024. [DOI]
- I World. ILGA World Maps,” ILGA World Maps
- F Zobel, LJ Maier. Collapse of the global order on drugs: from UNGASS 2016 to Review 2019, 2018
- C Thöni, L Eisner, T Hässler. Not straight enough, nor queer enough: Identity denial, stigmatization, and negative affect among bisexual and pansexual people. Psychol Sex Orientat Gend Divers, 2024. [DOI]
- RC Savin-Williams, K Joyner, G Rieger. Prevalence and stability of self-reported sexual orientation identity during young adulthood. Arch Sex Behav, 2012. [DOI | PubMed]
- L Eisner, F Turner-Zwinkels, D Spini. The Impact of Laws on Norms Perceptions. Pers Soc Psychol Bull, 2021. [DOI | PubMed]
- T Morgenroth, MK Ryan. The Effects of Gender Trouble: An Integrative Theoretical Framework of the Perpetuation and Disruption of the Gender/Sex Binary. Perspect Psychol Sci, 2021. [DOI | PubMed]
- C Rioux, A Paré, K London-Nadeau. Sex and gender terminology: a glossary for gender-inclusive epidemiology. J Epidemiol Community Health, 2022. [DOI]
- L Eggenbe. Something is not nothing: Hair-tested substance use and cognitive functions in a large community sample of young adults. 2025
- T Hässler, L Eisner. Swiss lgbtiq+ panel – 2020 summary report. PsyArXiv, 2020. [DOI]
- R Cipollina, MA Ruben, MR Maroney. The damaging legacy of damage-centered LGBTIQ+ research: Implications for healthcare and LGBTIQ+ health. J Soc Issues, 2024. [DOI | PubMed]
- SJ Ehlke, AL Stamates, ML Kelley. Bisexual Women’s Reports of Descriptive Drinking Norms for Heterosexual, Bisexual, and Lesbian Women. Psychol Sex Orientat Gend Divers, 2019. [DOI | PubMed]
- A Roxburgh, T Lea, J de Wit. Sexual identity and prevalence of alcohol and other drug use among Australians in the general population. Int J Drug Policy, 2016. [DOI | PubMed]