
Clinical Decision-Making Case: Thyroid Storm
Abstract
Audience:
This clinical decision-making case is intended for all emergency physicians (EP) in training.
Introduction:
Thyroid storm (TS) is a rare but life-threatening endocrine emergency that represents the most severe form of thyrotoxicosis. If not promptly recognized and appropriately managed, TS carries a mortality rate of up to 25%.ref. 1 However, with timely and aggressive treatment, mortality can be significantly reduced to 1.2–3.6% in the United States.ref. 2 Due to its rarity and often nonspecific presentation, early diagnosis and intervention in the emergency department are essential to improving patient outcomes. Recognizing its critical nature, the American Board of Emergency Medicine (ABEM) identifies thyroid storm as a core emergency condition that emergency physicians (EPs) must be trained to manage.ref. 3 Additionally, recent updates to the ABEM certifying examination emphasize the importance of clinical decision-making and the ability to verbalize diagnostic reasoning and management plans. This case has been designed to help learners practice and demonstrate these skills in the context of a high-stakes, time-sensitive clinical scenario involving thyroid storm.
Educational Objectives:
By the end of the session, learners will be able to: 1) verbalize key pertinent historical and physical exam findings in a young female patient presenting with altered mental status; 2) formulate a prioritized differential diagnosis based on the history and physical exam; 3) order appropriate diagnostic studies and recognize abnormalities suggesting thyroid storm; 4) describe pathophysiology, management and rationale of sequential pharmacologic therapy in thyroid storm; 5) communicate patient’s medical care and course to family; and 6) review essential disposition actions including consultations and level of care for admission.
Educational Methods:
We implemented a certifying exam board format case aligned with the ABEM’s updated certifying exam board examination. The case was co-developed by experts in simulation-based education and emergency medicine and underwent external peer review, which focused on the accuracy of the clinical context, clarity of scenario instructions, and educational value.
Research Methods:
The case was iteratively developed and refined through multi-site piloting. Initial design was completed by three faculty with emergency medicine and simulation backgrounds, followed by external review using the Simulation Scenario Evaluation Tool (SSET). Feedback focused on case progression, realism, alignment with objectives, and consistency with assessment standards.
The case was then piloted at two academic training sites and at the Society for Academic Emergency Medicine (SAEM) Annual Meeting. Participants included faculty facilitators and EM residents. Residents and faculty completed a modified usability survey incorporating Likert-scale items (1 = strongly disagree to 5 = strongly agree) and open-ended comments. Data was collected in Qualtrics® and analyzed in Excel®. Revisions were made after each iteration to improve clarity, usability, and educational impact.
Results:
The simulation scenario evaluation tool (SSET) evaluations were strongly positive. Facilitators (n = 3) consistently rated the case objectives, critical actions, and supporting materials as clear. They agreed or strongly agreed that the case was appropriate for the learner level, that the clinical course adhered to the ABEM format, and that the critical actions supported the stated objectives. Mean ratings ranged from 4 to 5 for ease of use, and facilitators noted that their colleagues would also find the materials accessible. They described the case as well-integrated, expressed confidence in facilitation, and endorsed its utility for ABEM certifying exam preparation.
Resident feedback was similarly supportive. Three learners unanimously agreed that the case provided helpful practice for the ABEM exam and reported that both the written and verbal instructions were clear.
Discussion:
The thyroid storm clinical decision-making case proved to be an effective educational tool, meeting its intended objectives and offering meaningful preparation for emergency medicine residents facing the new ABEM certifying examination. Facilitators consistently reported that the case objectives, critical actions, and supporting materials were clear and aligned with the targeted level of learner training. Similarly, both facilitators and residents found the case to be a valuable exercise, providing relevant and realistic practice in the style of the certifying exam.
While early results are encouraging, future challenges and opportunities remain. In particular, the evolving structure and scoring approach of the new ABEM certifying examination introduces areas where additional refinement may be needed. As more information becomes available regarding the exam’s evaluation metrics, this case can be further tailored to enhance alignment and maximize its educational impact. Continued iterative development will ensure the case remains a practical and high-yield resource for residents as they prepare for certification.
Topics:
Hyperthyroidism, communication, clinical decision-making case, certifying exam, thyroid storm, endocrinology.
Affiliations: University of Central Florida, Department of Emergency Medicine, Orlando; Creighton School of Medicine Phoenix, Department of Emergency Medicine, Phoenix, AZ; Hennepin County Medical Center, Department of Emergency Medicine, Minneapolis, MN; Montefiore Medical Center, Department of Emergency Medicine, Bronx, NY; Zucker School of Medicine at Hofstra/Northwell, Department of Emergency Medicine, Hempstead, NY; NYC Health + Hospitals, Department of Emergency Medicine, Brooklyn, NY; Boston University/Boston Medical Center, Department of Emergency Medicine, Boston, MA; Stanford University, Department of Emergency Medicine, Palo Alto, CA
License: © 2025 Stapleton, et al. CC BY 4.0 This is an open access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) License. See: http://creativecommons.org/licenses/by/4.0/
Article links: DOI: 10.21980/J8.53003 | PubMed: 41522638 | PMC: PMC12782603
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (8.1 MB)
USER GUIDE
List of Resources: Abstract260 User Guide263 For Examiner Only267 Certifying Exam Assessment274 Stimulus276 Debriefing and Evaluation Pearls287
Learner Audience:
All emergency medicine physicians in training.
Time Required for Implementation:
Case: Clinical Decision-Making cases are 15 minutes as directed by American Board of Emergency Medicine (ABEM).
Debriefing: 5 minutes
Recommended number of learners per instructor:
This case can be used to provide a mock certifying exam experience for emergency medicine residents, either in isolation or alongside additional cases to make the experience more realistic in preparation for the exam. For realism and accurate practice, we suggest arranging the case with a 1:1 ratio of faculty and learner. This case could be run with multiple learners for group practice. An additional use of the case would be to have a resident take the role of facilitator to gain an examiner’s perspective. The entire case, including feedback, should take 20 minutes, with 15 minutes for the case and 5 minutes for feedback.
Topics:
Hyperthyroidism, communication, clinical decision-making case, certifying exam, thyroid storm, endocrinology.
Objectives:
By the end of the session, learners will be able to:
- Verbalize key pertinent historical and physical exam findings in a young female patient presenting with altered mental status.
- Formulate a prioritized differential diagnosis based on the history and physical exam.
- Order appropriate diagnostic studies and recognize abnormalities suggesting thyroid storm.
- Describe pathophysiology, management, and rationale of sequential pharmacologic therapy in thyroid storm.
- Communicate patient’s medical care and course to family.
- Review essential disposition actions including consultations and level of care for admission.
Linked objectives, methods and results
This clinical decision-making case centers on a 33-year-old female who presents to the emergency department with altered mental status. The facilitator begins by providing minimal initial information, prompting the learner to identify the focused historical elements they would obtain from the patient, EMS, family members, or bystanders, including information relevant to endocrine, infectious, or other causes of altered mental status (Objective 1). The learner is then asked to describe the components of a targeted multisystem physical exam and explain the relevance of specific findings, such as neurologic status, cardiovascular abnormalities, fever, skin changes, or signs suggestive of thyroid dysfunction or infection (Objective 1).
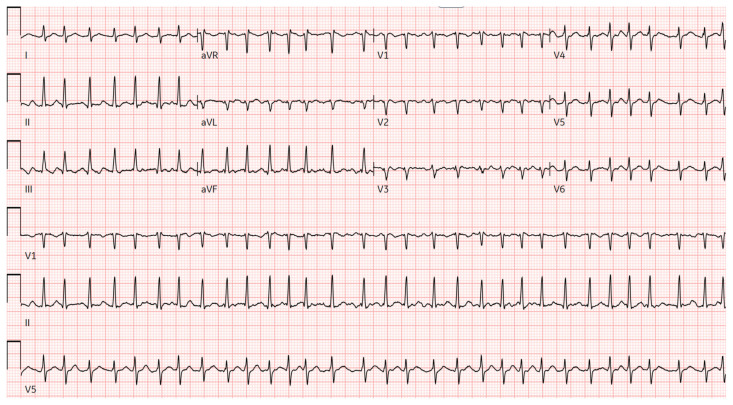
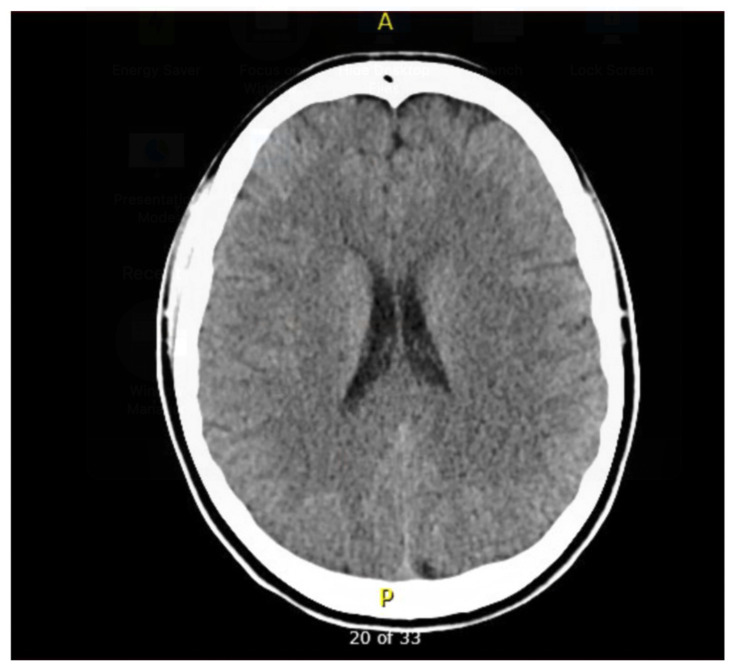
Next, the learner must formulate a prioritized differential diagnosis that includes both common and life-threatening etiologies of altered mental status in a young woman (Objective 2). Based on their assessment and differential, the learner will be required to select appropriate diagnostic studies and accurately interpret key clinical data, including laboratory values, urinalysis, ECG, imaging, and point-of-care tests (Objective 3). The diagnostic results in this case include leukocytosis, a nitrite-positive urinalysis, a normal glucose level, a normal head CT, and a suppressed thyroid-stimulating hormone (TSH) with elevated T3 and free T4. An ECG is provided that shows atrial fibrillation with rapid ventricular response, which the learner must recognize and incorporate into their diagnostic reasoning.
With these results, the learner is expected to initiate appropriate emergency department management for thyroid storm, including starting a beta-blocker, administering antithyroid medication, providing corticosteroids, offering supportive care, and considering empiric antibiotics when infection is suspected (Objective 4). The learner must then explain the rationale for the correct sequence of thyroid storm medications—beta-blocker followed by thionamide, then iodine, and corticosteroids—and identify relevant treatment endpoints such as heart rate, temperature, and mental status (Objective 4).
As the scenario progresses, the learner should reassess the patient and adapt the management plan based on evolving clinical information, changes in vital signs, and response to treatment (Objective 4). Throughout the case, the learner is expected to verbalize their medical decision- making, justify diagnostic and therapeutic actions, and communicate their interpretation of abnormal findings (Objective 4).
As the patient stabilizes, the facilitator introduces the patient’s husband, prompting the learner to provide anticipatory guidance, including a clear explanation of the diagnosis, treatment plan, expected hospital course, and next steps after admission (Objective 5). The learner must then identify appropriate consultants—including endocrinology and internal medicine—and determine that the patient requires ICU-level care based on her clinical status (Objective 6). Throughout the encounter and debrief, the learner is expected to demonstrate understanding of the pathophysiology of thyroid storm, including its systemic manifestations and common triggers, and connect this knowledge to the clinical presentation (Objective 4).
Recommended pre-reading for instructor
- Farooqi S, Raj S, Koyfman A, Long B. High risk and low prevalence diseases: Thyroid storm. Am J Emerg Med. 2023;69:127–135. doi:10.1016/j.ajem.2023.03.035
Results and tips for successful implementation
Tips for successful implementation
For additional realism, programs may incorporate a second faculty member to serve exclusively as the examiner, allowing the facilitator to focus on case delivery and prompts. The faculty facilitator followed a standardized script designed to replicate the new ABEM certifying exam format, ensuring consistency, realism, and educational relevance. During the case, residents were presented with a brief clinical stem and were required to verbalize both their patient assessment and their broader clinical reasoning. When available, a second faculty examiner used a structured checklist to capture communication behaviors and critical decision-making points.
Methods
The case was co-developed by three faculty members with expertise in emergency medicine and simulation-based education. It underwent external peer review to assess accuracy of the clinical content, clarity of instructions, and educational value. Reviewers used the Simulation Scenario Evaluation Tool (SSET) to provide structured feedback on case progression, realism, objectives, and alignment with assessment standards.
Following peer review, the case was piloted at two academic training sites and at the Society for Academic Emergency Medicine Annual Meeting. We employed an iterative trialing process with a convenience sample of EM residents. Residents and faculty participants completed usability surveys consisting of Likert-scale items (1 = strongly disagree to 5 = strongly agree) and open-ended feedback. Data were collected via QualtricsR (Provo, UT) and analyzed in ExcelR (Microsoft, Redmond, WA). The project was deemed exempt by the Boston University Institutional Review Board.
Examiner experience feedback survey:
- What regional area do you practice in? Northeast, South, Midwest, West
- What is your practice environment? Urban, Suburban, Rural
- What is your role? Residency leadership, core faculty, non-core faculty, resident
- Please rank your agreement with the following questions regarding the CURRICULUM guide:
- CURRICULUM General notes/comments
- Please rank your agreement with the following questions regarding the CASE guide:
- CASE General notes/comments
- Are there any clinical topics you would like to see in this case format?
Examinee experience feedback survey:
- Where are you testing this case? BMC, RWJ, SAEM, Northwell, Other___
- What regional area do you practice in? Northeast, South, Midwest, West
- What is your practice environment? Urban, Suburban, Rural
- What is your experience level? PGY1, PGY2, PGY3, PGY4, Fellow, Faculty
- Please rank your agreement with the following questions:
- What would you change?
- What was helpful?
- Are there any clinical topics you would like to see in this case format?
- Any other feedback/comments?
Iterative Piloting
- Round 1: Two EM residents at an academic site tested the case with faculty evaluation using the SSET and resident usability surveys.
- Round 2: At the SAEM Annual Meeting (May 2025, Philadelphia, PA), two facilitators and three residents participated, again using the SSET and usability surveys.
- Round 3: At a second academic site, seven PGY-3 residents completed the case and provided structured feedback.
Across all sites, revisions were made iteratively to the case content, facilitator script, and assessment tools, resulting in improved clarity, usability, and educational impact.
Results
The SSET evaluations were strongly positive (Table 1). Facilitators (n = 3) consistently rated the case objectives, critical actions, and supporting materials as clear. They agreed or strongly agreed that the case was appropriate for the learners’ knowledge and skill level, that the critical actions aligned with the stated objectives, and that the clinical course adhered to the ABEM format. Mean ratings ranged from 4 to 5 for ease of use, and facilitators indicated that their colleagues would also find the materials accessible. The debriefing plan component of the SSET received the lowest rating, with a mean Likert score of 1, reflecting that the initial manuscript did not present a sufficiently detailed debriefing strategy. Based on this feedback, the case was revised to include a more structured and robust debriefing plan, which improved the overall clarity and educational utility of the materials. Overall, they described the case as well-integrated, expressed confidence in facilitating it, and endorsed its value for ABEM certifying exam preparation.
Table 1: SSET Evaluation Raw Results (3 peer reviewer respondents)
| Learning Objectives | |||
| Objectives pertain to the skill level and knowledge base of the target audience | 5 | 5 | 5 |
| Objectives are specific | 5 | 5 | 5 |
| Objectives are measurable | 5 | 5 | 5 |
| Objectives are action-oriented | 5 | 5 | 5 |
| Objectives are relevant | 5 | 5 | 5 |
| Objectives are time-specific | 5 | 5 | 5 |
| Objectives specify the types of knowledge/skills expected to be gained by completing the simulation exercise | 5 | 5 | 5 |
| Clinical Context/Scenario Overview | |||
| Clinical context elements pertain to the skill level and knowledge base of the target audience | 5 | 5 | 5 |
| Clinical context elements support the learning objectives of the simulation-based experience | 5 | 5 | 5 |
| Critical Actions | |||
| Attainable in accordance with the skill level and knowledge base of the target audience | 5 | 5 | 5 |
| Support the learning objectives | 4 | 5 | 5 |
| Directly observable | 3 | 5 | 5 |
| Patient States | |||
| Clinically appropriate for case progression | 5 | 5 | 4 |
| Accounts for multiple management pathways a learner may take | 4 | 5 | 4 |
| Effective for meeting the learning objectives | 5 | 5 | 4 |
| Effective for eliciting the outline critical actions | 5 | 5 | 4 |
| Scenario Materials and Resources | |||
| Provides a list of necessary materials, equipment and human resources to support facilitation | 5 | 5 | 5 |
| Provides a list of necessary patient historical data, atrioventricular (AV) stimuli and clinical resources to support case facilitation | 5 | 5 | 5 |
| Debriefing Plan | |||
| Presents a clear debriefing plan | 1 | 1 | 1 |
| Provides supporting materials with References to aid debrief | 4 | 5 | 1 |
| Does the case follow the format provided by the ABEM case example? | 5 | 5 | 5 |
| Does the case follow the format provided by the JETem template? | 4 | 5 | 5 |
| Global Rating Scale What is the overall rating of the sim case quality? | 80 | 91 | 93 |
Given the very small number of respondents, these early findings should be interpreted cautiously. Only one resident completed the post-session survey during the pilot. This PGY-2 resident rated the written materials as very clear (5/5), the verbal instructions as clear (4/5), and the overall helpfulness of the case for ABEM exam preparation as 5/5. In open-ended feedback, the learner highlighted the value of “step-by-step instructor guidance,” and recommended minor clarification regarding expectations for the history and physical examination. The resident also identified “toxidromes” as a topic of interest for future cases developed in this format.
Faculty feedback, although also limited (n = 2), demonstrated similarly positive impressions. Both facilitators indicated they would use the case for ABEM preparation (ratings 4 and 5). Ratings reflected that the case was generally easy to use (3 and 5), well-integrated (4 and 5), and easy to learn (4 and 5). Confidence in facilitating the case ranged from 3 to 5. Across comments, facilitators endorsed the clarity of the materials, the organization of the case, and its utility as a certifying exam board practice tool.
Taken together, these preliminary results suggest high acceptability and perceived usefulness among early users, but further evaluation with a larger and more diverse group of residents and faculty will be necessary to draw more definitive conclusions.

| List of Resources: | |
|---|---|
| Abstract | 260 |
| User Guide | 263 |
| For Examiner Only | 267 |
| Certifying Exam Assessment | 274 |
| Stimulus | 276 |
| Debriefing and Evaluation Pearls | 287 |
| I. History | Yes | No | |
| 1a | Current symptoms that prompted Emergency Department visit | ||
| 1b | Symptom duration | ||
| 1c | Triggers for Thyroid Storm (infection, trauma, surgery, medications, recent medication changes, etc.) | ||
| 1d | Medications | ||
| 1e | Past Medical History | ||
| II. Physical Examination | |||
| 2a | HEENT Exam (pupillary exam, mucous membranes, proptosis, lid lag) | ||
| 2b | Neck Exam (goiter or meningismus) | ||
| 2c | Cardiac Exam (irregularly irregular rhythm, rate) | ||
| 2d | Neuro Exam (evaluation of altered mental status looking for patient orientation, focal neurologic deficits) | ||
| III. Differential Diagnosis | |||
| 3a | Thyroid Storm | ||
| 3b | 2nd appropriate diagnosis (see Prompt 3 scoring guidelines above) | ||
| 3c | 3rd appropriate diagnosis (see Prompt 3 scoring guidelines above) | ||
| IV. Diagnostic Studies | |||
| 4a | TSH/Free T4/T3 | ||
| 4b | CBC | ||
| 4c | Drug/Toxicology Screen | ||
| 4d | Pregnancy Test | ||
| 4e | ECG | ||
| 4f | Urinalysis and Urine culture | ||
| 4g | Consider Sepsis: Blood culture and lactic acid | ||
| V. Broad Concepts: Head CT | |||
| 5 | Able to provide three findings on a head CT that would cause altered mental status | ||
| VI. Broad Concepts: ECG | |||
| 6 | Correct interpretation of EKG (Atrial fibrillation with RVR) | ||
| 7 | Able to provide rationale for indications of rate control in a patient in Afib with RVR | ||
| VII. Treatment and Other Actions | |||
| 8a | Beta Blocker 1st | ||
| 8b | Propylthiouracil/methimazole 2nd | ||
| 8c | Steroid 3rd or 4th (can be given before or after iodine) | ||
| 8d | Iodine 3rd or 4th (should be given 1 hour after PTU or methimazole) | ||
| 8e | IV antibiotics for UTI (after urine culture is obtained) | ||
| VIII. Final Diagnosis | |||
| 9 | Urinary Tract Infection | ||
| 10 | Thyroid Storm | ||
| IX. Communication/Disposition/Transition of Care | |||
| 11a | Informed conversation with the husband about diagnosis, management, and next steps in layman’s terms | ||
| 11b | Consultation to Endocrine | ||
| 11c | Admission to ICU | ||
| Candidate Task Sheet | |
| #1 | Emergency Department Admitting Form |
| #2 | Historical Information |
| #3 | Physical Exam Findings |
| #4 | ECG |
| #5 | Laboratory and Point-of-Care Studies |
| #6 | Chest X-ray |
| #7 | Head CT |
Clinical Decision-Making Task Sheet
| CASE PARAMETERS |
| PATIENT INFORMATION |
| 33-year-old female presents to the ED via EMS for altered mental status. |
| VITAL SIGNS |
| TASK STATEMENT |
| Your tasks are as follows: |
STIMULUS 1: Emergency Department Admitting Form
| Patient Information | |
| Patient Name | Jessica Gonzalez |
| Age | 33 yo |
| Gender | F |
| Method of Arrival | EMS |
| General Appearance/History of Present Illness | She is diaphoretic, confused and can only provide her name. |
| Vital Signs on ED Arrival | BP: 158/99P: 142R: 24T: 40.1° CO2 sat:98% |
STIMULUS 2: Historical Information
| History of Present Illness/Description of Event | |
| History | |
| Past Medical History | Celiac Disease |
| Past Surgical History | None |
| Medications | Multivitamin, Oral Contraception |
| Allergies | No known drug allergies |
| Social | None |
STIMULUS 3: Physical Exam Findings
| Physical Examination | |
| General | Laying on the stretcher, diaphoretic. |
| HEENT | Atraumatic, normocephalic.Pupils are 3 mm bilaterally and reactive to light. Normal Conjunctiva.Proptosis bilaterally and lid lag with extraocular movements.Normal tympanic membranes bilaterally and external ears normal.Dry mucous membranes; no oropharyngeal edema, erythema, or exudates. |
| Neck | Supple, full range of motion. No meningismus. Palpable goiter. |
| Cardiovascular | Irregularly irregular rhythm, rapid rate, no murmurs. |
| Respiratory | Tachypneic. Breath sounds clear and equal bilaterally without any wheezing, crackles, or ronchi. |
| Abdomen | Soft, non-distended. Suprapubic tenderness to palpation. No rebound tenderness or involuntary guarding. |
| Genital | No vaginal discharge or bleeding. Normal, closed cervix. No cervical motion tenderness. No adnexal tenderness or masses. |
| Back | No midline tenderness to palpation. Right costovertebral angle tenderness. |
| Extremities | Normal range of motion of joints with no rigidity. |
| Neuro | Agitated. Oriented to self only. Opens eyes to voice. Follows commands in all four extremities. Cranial nerves II–XII intact. 5/5 strength and intact sensation to light touch in all four extremities. No clonus. Hyperreflexia. |
| Skin | Diaphoretic. No rashes. |
| Lymph | No lymphadenopathy. |
| Psych | Unable to completely assess since patient is only able to state her name. |
STIMULUS 4: Laboratory and Point-of-Care Studies
| Lab Panel | Type | Units | Normal Values |
| Point-of-Care | Glucose | 90 mg/dL | 70–105 mg/dL |
| HCG | Negative | Negative | |
| Complete Blood Count | WBC | 16.1 × 103/μL | 4–11 × 103/μL |
| HCT | 38.80% | 36–47% female | |
| 41–51% male | |||
| HGB | 12.9 g/dl | 12–14 g/dL female | |
| 14–17 g/dL male | |||
| PLT | 270 × 103/μL | 150–450 × 103/μL | |
| Neutrophils | 66% (10,626) | ||
| Lymphocytes | 26% (4186) | ||
| Monocytes | 5% (402) | ||
| Eosinophils | 2.5% (402) | ||
| Basophils | 0.5% (81) | ||
| Basic Metabolic Panel | Na | 142 mEq/L | 136–145 mEq/L |
| K | 4.4 mEq/L | 3.5–5 mEq/L | |
| Cl | 107 mEq/L | 98–106 mEq/L | |
| CO2 | 24 mEq/L | 23–28 mEq/L | |
| BUN | 13 mEq/dL | 8–20 mEq/dL | |
| Creatinine | 0.68 mg/dL | 0.7–1.3 mg/dL | |
| Glucose | 95 mg/dL | 70–105 mg/dL | |
| Calcium | 9.4 mg/dl | 9.0–10.5 mg/dL | |
| Liver Function Panel | AST | 15 U/L | 0–35 U/L |
| ALT | 11 U/L | 0–35 U/L | |
| Alk Phos | 49 U/L | 36–92 U/L | |
| T bili | 0.4 mg/dL | 0.3–1.2 mg/dL | |
| D bili | 0.2 mg/dL | 0.0–0.3 mg/dL | |
| Albumin | 4.1 g/dL | 3.5–5.0 mg/dL | |
| Total Protein | 7.3 g/dL | 6–8.3 mg/dL | |
| Urinalysis | Specific Gravity | 1.023 | 1.005–1.030 |
| pH | 5.5 | 4.5–8.0 | |
| Protein | 30 mg/dL | <150 md/dL | |
| Glucose | Negative | Negative | |
| Ketones | Negative | Negative | |
| Bili | Negative | Negative | |
| Blood | Small | None | |
| LE | Large | None | |
| Nitrite | Positive | Negative | |
| Color | Yellow | Yellow | |
| WBC | 1123/hpf | <2–5 WBC/hpf | |
| RBC | 35 hpf | <2 RBC/hpf | |
| Bacteria | 3+ | None | |
| Arterial Blood Gas | pH | 7.41 | 7.37–7.44 |
| PO2 | 94 mm Hg | 80–100 mm Hg | |
| PCO2 | 37 mm Hg | 35–45 mm Hg | |
| HCO3 | 26 mmol/L | 22–26 mmol/L | |
| Lactate | 2.4 mEq/L | 0.4–2.3 mEq/L | |
| Thyroid Function Studies | TSH | 0.04 mIU/L | 0.350 – 3.600 mIU/L |
| Free T4 | 17.4 ng/dl | 0.70 – 1.37 ng/dL | |
| T3 | 308 ng/dL | 80 to 200 ng/dL | |
| Troponin | Troponin | <0.01 ng/ml | <0.01 ng/ml |
| Serum Tox Screen | Acetaminophen | Negative | Negative |
| Ethanol | Negative | Negative | |
| Salicylate | Negative | Negative | |
| Urine Tox Screen | Acetaminophen | Negative | Negative |
| Amphetamine | Negative | Negative | |
| Barbiturate | Negative | Negative | |
| Benzodiazepine | Negative | Negative | |
| Buprenorphine | Negative | Negative | |
| Cannabinoid | Negative | Negative | |
| Cocaine | Negative | Negative | |
| Ethanol | Negative | Negative | |
| Methadone | Negative | Negative | |
| Opiate | Negative | Negative | |
| Oxycodone | Negative | Negative | |
| Salicylate | Negative | Negative | |
| Tricyclic | Negative | Negative |
References
- B Pokhrel, W Aiman, K Bhusal. Thyroid Storm. StatPearls [Internet], 2025
- S Farooqi, S Raj, A Koyfman, B Long. High risk and low prevalence diseases: Thyroid storm. Am J Emerg Med, 2023. [DOI | PubMed]
- MS Beeson, R Bhat, JS Broder. The 2022 Model of the Clinical Practice of Emergency Medicine. J Emerg Med, 2023. [DOI | PubMed]
- J Hernandez, A Frallicciardi, NA Nadir, MD Gothard, RA Ahmed. Development of a Simulation Scenario Evaluation Tool (SSET): modified Delphi study. BMJ Simul Technol Enhanc Learn, 2020. [DOI | PubMed]