Laparoscopic cholecystectomy with common bile duct exploration for choledocholithiasis in a patient with situs inversus totalis – Case report and review of literature
Abstract
Introduction and importance:
Laparoscopic common bile duct (CBD) exploration with cholecystectomy in patients with situs inversus totalis (SIT) is technically demanding and warrants comprehensive knowledge of the mirror image anatomy along with laparoscopic orientation of the left upper quadrant.
Case presentation:
In this case report, we present a female patient who presented with pain in the left hypochondrium, yellowish discoloration of the eyes since 2 months. She was evaluated, diagnosed to be a case of SIT with cholelithiasis and choledocholithiasis in cholangitis and endoscopic attempts for stone clearance failed. She subsequently underwent laparoscopic common bile duct exploration (LCBDE) with cholecystectomy. Per-operative, cystic duct was short and a choledochoscope was utilized for bile duct clearance.
Clinical discussion:
Laparoscopic surgery in patients with SIT is complex, technically challenging and requires a in depth knowledge of remodeled anatomy. We noted a change in the relation of portal vein with CBD as in the portal vein was postero-lateral to bile duct rather than being completely posterior. The key here is to stay close to the common bile duct which can avoid confusion and inadvertent injury to vital structures in the hepato-duodenal ligament.
Conclusion:
Laparoscopic cholecystectomy and CBD exploration in situs inversus is extremely challenging and the surgeon should be aware of the ergonomics and practice to operate laparoscopically with the opposite hand I.e the non-dominant hand in right-handed surgeon. Thus, laparoscopic cholecystectomy with LCBDE in situs inversus totalis is safe and feasible but demands technical difficulties.
Article type: Case Report
Keywords: Laparoscopic common bile duct exploration, Situs inversus totalis, Choledocholithiasis, Mirror image transposition, Case report
License: © 2025 The Authors. Published by Elsevier Ltd on behalf of IJS Publishing Group Limited. CC BY 4.0 This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.1016/j.ijscr.2025.111238 | PubMed: 40203625 | PMC: PMC12005859
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (3.2 MB)
Introduction
Laparoscopic common bile duct exploration (LCBDE) with cholecystectomy is a widely accepted technique for managing choledocholithiasis, especially in patients with failed Endoscopic Retrograde cholangiography (ERC) and stone extraction [ref. 1]. The difficulty in ERC and stone retrieval may result from large, multiple or impacted stones or altered anatomy of the duodenum and the ampulla [ref. 2]. One such rare condition of altered anatomy is situs inversus totalis (SIT), where there is mirror image transposition of abdominal and thoracic organs. SIT, an autosomal recessive congenital disorder, was first reported by Kruchenmeister in 1824 [ref. 3]. While the occurrence of biliary tract disorders in SIT is comparable to that of the general population, it poses a significant diagnostic and management challenge due to altered anatomy [ref. 4]. In this report, we describe a SIT patient with cholelithiasis and choledocholithiasis with a history of failed ERC managed with laparoscopic cholecystectomy and CBD exploration and a brief review of the literature. This work has been reported in line with the SCARE criteria [ref. 5].
Case report
A 56 year old female who was a known diabetic and hypertensive on regular medication, presented with dull aching type of pain in the left hypochondrium radiating to back and associated with occasional non bilious vomiting for the past 2 months which was managed by over the counter analgesics. She had history of yellowish discoloration of eyes with passage of dark yellow urine and fever of multiple spikes for 5 days. On examination she was icteric, well hydrated and abdominal examination revealed mild tenderness in the left hypochondrium. She was initially admitted and evaluated by the team of Medical Gastroenterology. Her blood investigations are depicted in the Table 1.
Table 1: Preoperative & postoperative blood investigations of the study patient.
| Haemoglobin – 13.3 g/dl (13.1–17.2 g/dL) | Blood urea – 48 mg/dl (17–43 mg/dl) | Direct bilirubin – 4.59 mg/dl (0.03–0.18 mg/dL) | Gamma glutamyl transferase – 499 U/L (5–40 U/L) | INR – 1.11 (0.8–1.1) |
|---|---|---|---|---|
| Preoperative blood investigations of the study patient – | ||||
| TLC – 17,050 cells/cumm(4000–11,000 cells/cumm) | Serum creatinine – 1.16 mg/dl (0.6–1.2 mg/dl) | AST – 380 (0–35 IU/L)ALT – 819 (0–35 IU/L) | Serum amylase – 19 U/L (22–80 IU/L) | |
| Platelet – 3,60,000 cells/cumm(150000–400,000 cells/cumm) | Total bilirubin −7.35 mg/dl (0.3–1.2 mg/dl) | Alkaline phosphatase – 436 IU/L (30–120 IU/L) | Prothrombin time – 12.1 s (10–13 s) | |
| Postoperative blood investigations of the study patient – | ||||
| Haemoglobin – 11.1 g/dl (13.1–17.2 g/dL) | Blood urea – 22 mg/dl (17–43 mg/dl) | Direct bilirubin – 0.35 mg/dl (0.03–0.18 mg/dL) | Gamma glutamyl transferase – 49 U/L (5–40 U/L) | INR – 0.93 (0.8–1.1) |
| TLC – 10,800 cells/cumm (4000–11,000 cells/cumm) | Serum creatinine – 0.61 mg/dl (0.6–1.2 mg/dl) | AST – 18 (0–35 IU/L)ALT – 21 (0–35 IU/L) | Serum amylase – 39 U/L (22–80 IU/L) | |
| Platelet – 2,23,000 cells/cumm(150000–400,000 cells/cumm) | Total bilirubin −1.09 mg/dl(0.3–1.2 mg/dl) | Alkaline phosphatase – 158 IU/L (30–120 IU/L) | Prothrombin time – 10.1 s (10–13 s) | |
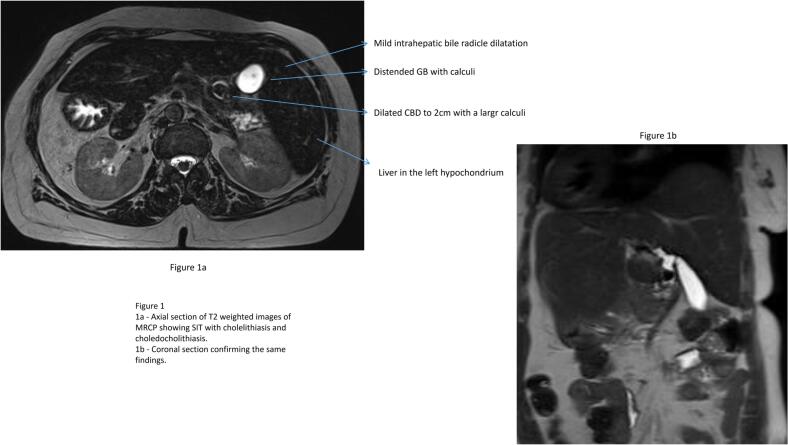
An ultrasonogram abdomen revealed liver in the left hypochondriac and epigastric region with normal echoes and no focal lesions, Gall bladder calculi of 1 cm with normal wall thickness and sonographic positive Murphy’s sign. The common bile duct could not be visualised due to excessive bowel gas. An MRCP revealed features of situs inversus with distended gall bladder with large calculus of 1.5 cm and dilated CBD of 2 cm with mid CBD calculus of 1.8 cm with dilated intra hepatic biliary radicles (Fig. 1). She was eventually diagnosed with situs inversus totalis, cholecystolithiasis, and choledocholithiasis with obstructive jaundice in cholangitis. In view of the cholangitis, she received parenteral antibiotics and was planned for ERC, stone retrieval and biliary stenting. However, ERC was attempted and failed twice due to altered duodenal anatomy and difficult manipulation. Subsequently, she was referred to our team of Surgical Gastroenterology and a decision for surgical intervention was made.
Surgical technique
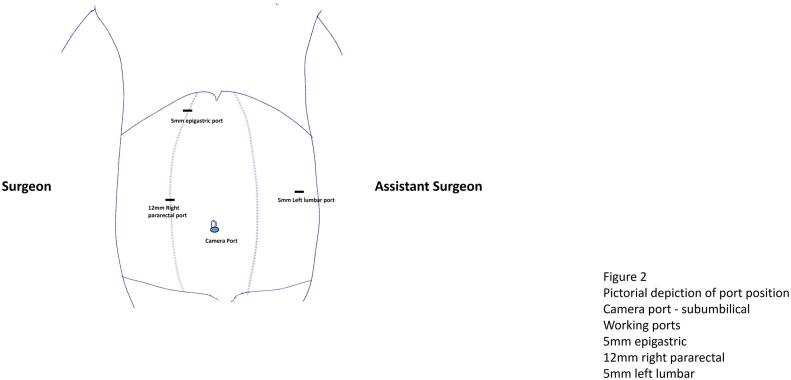
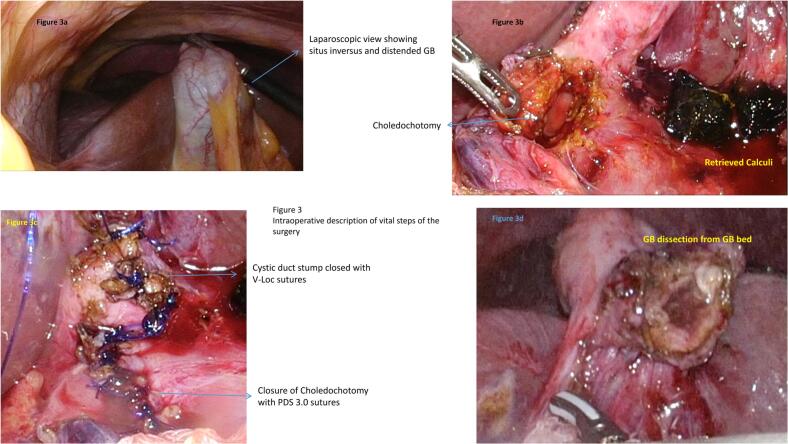
Under General anaesthesia, the ports were placed as depicted in the Fig. 2. A sub-umbilical 12 mm port was inserted by open technique and pneumoperitoneum was created with CO2 and 3D laparoscope was introduced. Left lumbar 5 mm port, right para-rectal port 12 mm port and 5 mm epigastric ports were placed under direct vision. The gallbladder was retracted upwards and laterally. Adhesion was released. Posterior and anterior peritoneal layers were dissected out and cystic artery was identified and ligated. CBD was opened 1 cm below the cystic duct insertion. Two large stones of size 1 cm were removed and thorough saline irrigation was given. A choledochoscope was passed in to CBD and stone clearance was confirmed. Cystic duct was short and dilated. Cystic duct was divided at infundibulum and suture closed with barbed absorbable suture material (3–0). CBD was repaired with PDS 3–0 sutures in intermittent fashion. Gallbladder was dissected from the liver bed and delivered out through the umbilical port in retrieval bag with the CBD stone. One 16 French suction drain was placed in the subhepatic space (Fig. 3). She was started on oral sips on Post-operative Day (POD) 1 and further escalated to soft diet on the same day. Her drain output remained around 20-30 ml/ day (serous), hence a decision was done to retain the drain. Her blood investigations at the time of discharge were as depicted in the Table 1. Her port sites remained healthy and she was discharged in a stable condition with drain in situ. On further follow up after 1 week, the drain output was reduced to 10 ml/day and eventually drain was removed. The histopathological examination of the gall bladder revealed features of chronic cholecystitis with cholelithiasis.
Discussion
Laparoscopic cholecystectomy has increasingly become the standard treatment for both uncomplicated and complicated biliary stone disease, with a growing number of articles discussing its widespread adoption [ref. 6]. However, in cases of SIT, where the visceral organs are mirrored from their usual positions, laparoscopic cholecystectomy with or without CBD exploration exploration present unique technical challenges due to the reversed anatomical orientation. Surgeons must exercise particular caution to avoid accidental injury in this unfamiliar surgical landscape [ref. 7,ref. 8]. Our literature review identified a total of 9 reported cases of laparoscopic CBD exploration in patients with SIT for choledocholithiasis [ref. [9], ref. [10], ref. [11]]. Of these, preoperative ERCP was attempted but failed in five cases, predominantly due to the altered anatomy of the duodenum and ampulla, making cannulation difficult [ref. 12,ref. 13]. Intraoperative cholangiography (IOC) and the use of a choledochoscope were employed in two and three cases, respectively, leading to successful clearance of CBD stones. Most reports indicated that the surgeon operated from the right side, with one exception where the surgeon positioned themselves between the patient’s legs [ref. 14]. The standard four-port technique was used in all cases except for one, which utilized a multichannel port to perform a single-incision laparoscopic CBD exploration [ref. 15]. Other intraoperative parameters and postoperative outcomes are depicted in Table 2.
Table 2: Preoperative and intraoperative parameters of the case reports describing laparoscopic CBD exploration for choledocholithiasis in patients with situs inversus totalis.
| Author/year | Preoperative co-morbidities | Preoperative ERCP intervention | Intraoperative application of IOC or Choledochoscope | Number of ports | Technique applied for CBD exploration | Length of hospital stay (days) |
|---|---|---|---|---|---|---|
| Chiu BY, 2022 | Hypertension, diabetes and chronic kidney disease | No | IOC | Multichannel port | Transcystic approach with wire basket retrieval | 3 |
| Simkhada, 2021 | Hypertension and chronic kidney disease | Yes | Choledochoscope | 4 | Choledochotomy with primar closure | Not specified |
| Takalkar, 2018 | No comorbidities | Yes | None | 4 | Choledochotomy with choledochoduodenostomy | Not specified |
| Senthilnathan, 2017 | No comorbidities | Yes | IOC | 4 | Choledochotomy with choledochoduodenostomy | 7 |
| Liu, 2017 | No comorbidities | No | Not specified | 4 | Not specified | 3 |
| Han, 2012 | No comorbidities | Yes | Choledochoscope | 4 | Choledochotomy with primary closure | Not specified |
| Tai, 2004 | Coronary heart disease | Yes | Choledochoscope | 4 | Choledochotomy with primary closure | Not specified |
| Kang, 2004 | Cardiac arrhythmias | No | Choledochoscope | 4 | Choledochotomy with T tube insertion | Not specified |
| Our case report, 2023 | Hypertensive and diabetic | Yes | Choledochoscope | 4 (Modified) | Choledochotomy with primary closure | 3 |
Our patient presented with cholangitis and was initially treated with intravenous antibiotics, with a plan for ERC and stone removal. However, due to a failed ERC, we opted for an operative management. During the procedure, we made a slight modification to the standard port placement by introducing a right pararectal port specifically for CBD exploration. Our modified technique involved using both the right pararectal port and a left lumbar port for the exploration of the CBD. A choledochoscope was employed for CBD clearance, followed by primary closure of the choledochotomy. A key principle we adhered to, and which should be considered a critical step in such cases, is to avoid excessive dissection near the CBD, as the altered anatomy in SIT can significantly alter the anatomical relationships of the portal vein, hepatic artery, and CBD within the hepatoduodenal ligament. In our case, for example, the portal vein was observed to be more anteriorly positioned and was crossing the distal portion of the CBD (Fig. 3). By following this principle, the risk of inadvertent injuries can be minimized in patients with altered anatomy.
Conclusion
Laparoscopic cholecystectomy and CBD exploration in patients with situs inversus poses significant challenges due to the mirrored anatomical orientation. Surgeons must be mindful of the altered ergonomics and practice operating with their non-dominant hand, particularly for right-handed surgeons, since the usual orientation is reversed. Despite these difficulties, the fundamental principles of surgery remain unchanged. Therefore, while laparoscopic cholecystectomy with laparoscopic CBD exploration in situs inversus totalis is safe and feasible, it requires overcoming notable technical challenges.
Author contribution
Study concept/design: R Kalayarasan/Biju Pottakkat.
Data collection: Sai Krishna.
Data analysis: Sai Krishna.
Writing the paper: R Kalayarasan.
Final check and corrections: R Kalayarasan/Biju Pottakkat.
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval for this case report was provided by ethical committee of JIPMER, Puducherry on 10 November 19, 2024.
Guarantor
Sai Krishna.
Funding
No funding was provided.
Declaration of competing interest
No conflict of interest.
References
- 1Park CH. [The Management of Common Bile Duct Stones]. Korean J Gastroenterol. 2018 May 25;71(5):260–263. Korean. doi:10.4166/kjg.2018.71.5.260. PMID: 29791984.
- J. Emmanuel, N. Sriram, R. Muthukaruppan. Endoscopic retrograde cholangiopancreatography in a patient with complete situs inversus viscerum: a case report and literature review. DEN Open, 2021 May 27. [DOI]
- K. Eitler, A. Bibok, G. Telkes. Situs inversus totalis: a clinical review. Int. J. Gen. Med., 2022 Mar. [DOI]
- I.A. Salama, M.H. Abdullah, M. Houseni. Laparoscopic cholecystectomy in situs inversus totalis: feasibility and review of literature. Int. J. Surg. Case Rep., 2013. [PubMed]
- C. Sohrabi, G. Mathew, N. Maria, A. Kerwan, T. Franchi, R.A. Agha. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. Lond. Engl., 2023
- H. Tafazal, P. Spreadborough, D. Zakai, N. Shastri-Hurst, S. Ayaani, M. Hanif. Laparoscopic cholecystectomy: a prospective cohort study assessing the impact of grade of operating surgeon on operative time and 30-day morbidity. Ann. R. Coll. Surg. Engl., 2018 Mar. [DOI | PubMed]
- 7Tai CK, Tang CN, Ha JP, Chau CH, Siu WT, Li MK. Laparoscopic exploration of common bile duct in difficult choledocholithiasis. Surg. Endosc. 2004; 18: 910–914 [PMID: 15095079 DOI:10.1007/s00464-003-8216-8].
- 8Mendoza Rojas HJ, Martínez Cevallos C, Hinojo Chanco JR. Colecistectomía con exploración de vías biliares laparoscópica en paciente con situs inversus totalis [Laparoscopic cholecystectomy with common bile duct exploration in situs inversus totalis patient]. Rev Gastroenterol Peru. 2023 Oct-Dec;43(4):378–382. Spanish. PMID: 38228306.
- 9Liu Y, Wu L, Chen Y, Li D, Jiang J, Zhong W, Cao Y. Delayed diagnosis of abdominal pain in patient with situs inversus totalis in emergency department: a case report. Medicine (Baltimore) 2017; 96: e9028 [PMID: 29245291 DOI:10.1097/MD.0000000000009028].
- A. Weber-Sánchez, C. Bravo-Torreblanca, D. Garteiz-Martínez, R. Carbó-Romano, F. Vega-Rivera, R. Hernández. Case report: laparoscopic cholecystectomy and common bile duct exploration in a 60 year-old patient with situs inversus. Rev. Gastroenterol. Mex., 2011. [PubMed]
- S.J. Han, K.S. Chun, I.S. Song. Laparoscopic cbd exploration in patient with situs inversus totalis. HPB, 2012. [DOI]
- S. Simkhada, B. Malla, R. Shrestha. Laparoscopic cholecystectomy and common bile duct exploration in situs inversus patients. Kathmandu Univ. Med. J. (KUMJ), 2021. [PubMed]
- 13Takalkar YP, Koranne MS, Vashist KS, Khedekar PG, Garale MN, Rege SA, Dalvi AN. Laparoscopic cholecystectomy with choledochoduodenostomy in a patient with situs inversus totalis. J. Minim. Access Surg. 2018; 14: 241–243 [PMID: 29882522 DOI:10.4103/jmas.JMAS_122_17].
- P. Senthilnathan, R. Parthasarathi, S. Rajapandian, P. Praveen Raj, A. Vijai, V.P. Nalankilli, G. Srivatsan, S. Sabnis, C. Palanivelu. Laparoscopic CBD exploration with choledochoduodenostomy for bileduct stones in a patient with situs inversus totalis. Surg. Endosc. Other Interv. Tech., 2017. [DOI]
- B.Y. Chiu, S.H. Chuang, S.C. Chuang, K.K. Kuo. Laparoscopic common bile duct exploration to treat choledocholithiasis in situs inversus patients: a technical review. World J. Clin. Cases, 2023 Mar 26. [DOI | PubMed]