
Alcohol Withdrawal
Abstract
Audience:
Emergency medicine residents and medical students on emergency medicine rotations
Introduction:
Alcohol use disorder (AUD) is common in the United States, with an estimated lifetime prevalence of 30%.ref. 1 The rate of use is higher among white males, Native Americans, and individuals of low socioeconomic status.ref. 1 Alcohol withdrawal symptoms manifest in 50% of individuals who misuse alcohol.ref. 1 While life-threatening sequelae of alcohol withdrawal are rare, the syndrome is a common reason for emergency department (ED) presentations. Alcohol withdrawal symptoms range from benign, cravings, nausea, anxiety and tremulousness, to life-threatening autonomic dysfunction, seizures, coma, and death.ref. 2 The pathophysiology of this clinical syndrome involves dysregulation of central nervous system (CNS) receptor function. Alcohol acts as a CNS depressant through activation of the CNS Gamma-aminobutyric acid (GABA) receptors. Chronic or heavy alcohol use results in downregulation of CNS inhibitory GABA receptors and upregulation of CNS excitatory N-methyl-D-aspartate (NMDA) receptors.ref. 2 Upon discontinuation of alcohol use, this imbalance results in CNS hyperexcitability, creating the clinical symptoms of alcohol withdrawal.ref. 2 Symptoms typically manifest within eight hours after alcohol cessation, reach their peak in one to three days, and can extend for up to two weeks.ref. 3 Mild symptoms include anxiety, tremors, diaphoresis, nausea and/or vomiting. Severe symptoms include hallucinations (typically 12–24 hours after last alcohol intake) in 2–8% of patients, seizures (12–48 hours after last intake) in up to 15% of patients, and delirium tremens.ref. 3 Delirium tremens is a potentially fatal encephalopathy in patients experiencing alcohol withdrawal and occurs in 3–5% of patients approximately 72 hours after last alcohol intake.ref. 3 Without recognition or prompt treatment, mortality from delirium tremens can be as high as 50%.ref. 4 Management of alcohol withdrawal requires prompt recognition and control of symptoms. Most often this is accomplished by administering benzodiazepines, though alternative medications such as barbiturates, ketamine, or propofol are also used. Severe withdrawal may progress to intubation and mechanical ventilation.ref. 5 Given the high prevalence of AUD in the United States and the potential for life-threatening withdrawal symptoms, ED practitioners must recognize the spectrum of this disease and be comfortable with managing an array of presentations.
Educational Objectives:
At the end of this oral boards session, learners will: 1) demonstrate the ability to perform a detailed history and physical examination in a patient presenting with signs and symptoms of alcohol withdrawal, 2) investigate the broad differential diagnoses, including electrolyte abnormalities, trauma in the intoxicated patient, mild alcohol withdrawal, and delirium tremens, 3) list appropriate laboratory and imaging studies to include complete blood count (CBC), complete metabolic panel (CMP), magnesium level, computed tomography (CT) scan of the brain; 4) understand the management of hypoglycemia with concurrent administration of thiamine to prevent Wernicke’s encephalopathy and subsequent Korsakoff syndrome, 5) appropriately treat acute alcohol withdrawal with intravenous (IV) hydration and benzodiazepines, phenobarbital, or alternative medications, and 6) understanding the need for the complex management of these patients, appropriately disposition the patient to the intensive care unit after consulting with critical care specialists.
Educational Methods:
The case was written as an oral boards case to test learners in a simulated oral board format. In this manner, learners could be evaluated on their critical thinking skills one-on-one with an instructor, outside of the distractions of the emergency department. Oral board simulation can test multiple modalities, including data collection, data synthesization and pharmacologic treatment in order to assess residents’ overall clinical care and competence. Learners were assessed both by the instructor with immediate feedback, as well as by using Google forms to tie critical actions to Emergency Medicine Milestones. Results were compiled and used during clinical competency evaluations.
Research Methods:
Learners (n=40) and examiners were given the option to provide written feedback after the case was completed to assess for strengths and weaknesses of the oral boards case, and subsequent changes were made to improve the administration of the case.
Results:
Residents and medical students rated this highly and found this to be an enjoyable, yet still challenging, way to stay current on their management skills of alcohol withdrawal. Learners rated the session 4.6 out of 5 using a five-point Likert scale (5 being excellent) after the session was completed (n=25).
Discussion:
We found this oral board case to be an effective educational tool for reviewing alcohol use disorder among students and residents. Using an oral board case allows junior and senior residents to be tested quickly in a low-stakes environment. Learners and instructors both felt the content was appropriate, and using the completed forms in competency meetings improved the committee’s ability to assess residents on specific milestones. Though we initially wrote this case requiring the examinee to have advance knowledge of the Clinical Institute Withdrawal Assessment Alcohol Scale Revised (CIWA-Ar), this was not deemed essential to emergency medicine residents or faculty, and it was removed. The current case formatting represents a more realistic case presentation and critical actions.
Topics:
Alcohol withdrawal, electrolyte abnormalities, seizures, altered mental status.
Affiliations: *Emory University School of Medicine, Department of Emergency Medicine, Atlanta, GA; ^Utah Emergency Physicians, P.C. Murray, Utah
License: © 2025 Meloy, et al. CC BY 4.0 This is an open access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) License. See: http://creativecommons.org/licenses/by/4.0/
Article links: DOI: 10.21980/J87S8Q | PubMed: 39926251 | PMC: PMC11801492
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (5.9 MB)
USER GUIDE
| List of Resources: | |
|---|---|
| Abstract | 1 |
| User Guide | 3 |
| For Examiner Only | 6 |
| Oral Boards Assessment | 12 |
| Stimulus | 15 |
| Debriefing and Evaluation Pearls | 29 |
List of Resources: Abstract1 User Guide3 For Examiner Only6 Oral Boards Assessment12 Stimulus15 Debriefing and Evaluation Pearls29
Learner Audience:
Medical Students, Interns, Junior Residents, Senior Residents
Time Required for Implementation:
Case: 15 minutes
Debriefing: 10 minutes
Learners per instructor: 1, 1–2 others may observe
Topics:
Alcohol withdrawal, electrolyte abnormalities, seizures, altered mental status.
Objectives:
At the end of this oral boards session, learners will:
- Demonstrate the ability to perform a detailed history and physical examination in a patient presenting with signs and symptoms of alcohol withdrawal.
- Investigate the broad differential diagnoses, including electrolyte abnormalities, trauma in the intoxicated patient, mild alcohol withdrawal, and delirium tremens.
- List appropriate laboratory and imaging studies to include complete blood count (CBC), complete metabolic panel (CMP), magnesium level, and computed tomography (CT) scan of the brain.
- Understand the management of hypoglycemia with concurrent administration of thiamine to prevent Wernicke’s encephalopathy and subsequent Korsakoff syndrome.
- Appropriately treat acute alcohol withdrawal with intravenous (IV) hydration and benzodiazepines, phenobarbital, or alternative medications.
- Appropriately disposition the patient to the intensive care unit after consulting with critical care specialists, understanding the need for the complex management of these patients.
Linked objectives, methods and results
Acute alcohol withdrawal is common in emergency medicine. Prompt diagnosis and early aggressive treatment reduces the risk of symptom progression to delirium tremens. The learner in this case should be able to synthesize the available historical and physical examination data in order to develop a broad differential diagnosis and identify signs and symptoms of acute alcohol withdrawal.
On initial evaluation, the learner will obtain a detailed history and complete physical examination which will suggest acute alcohol withdrawal (Objective 1). The learner should maintain a broad differential and obtain a thorough workup, including laboratory tests and imaging (Objectives 2 and 3). Recognize the need for point-of-care glucose testing in an altered patient and treat accordingly with glucose administration and concurrent administration of thiamine in the setting of alcohol abuse (Objective 4). Once the learners identify the patient is in acute alcohol withdrawal, they initiate treatment, to be guided by the clinical response to treatment (Objectives 3 and 5). The learner should provide appropriate disposition of the patient to an intensive care unit (Objective 6). Debriefing will ensure the learner can assimilate all of the clinical and lab findings in order to find the correct diagnosis.
Recommended pre-reading for instructor
- Yancey J, Micciche D. Alcohol withdrawal syndrome: identification and management. emDocs Published May 2022. Accessed December 27, 2023. https://www.emdocs.net/alcohol-withdrawal-syndrome-identification-and-management/
- Newman RK, Stobart Gallagher MA, Gomez AE. Alcohol withdrawal. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 21, 2023.
Results and tips for successful implementation
This model is best executed as an oral board single case examination. Learners should be directly observed by the instructor. Additional evaluators or instructors may also observe the case progression. This examination was tested during a mock oral board simulation, as well as during oral board practice sessions. Learners were evaluated using assessment forms that were created using Google forms. (https://docs.google.com/forms). The forms measured critical actions, which were also tied to Emergency Medicine Milestones (https://www.abem.org/public/docs/default-source/default-document-library/em-milestones.pdf?sfvrsn=e627c8f4_0). Using this format, oral board testing can be used to assess examinees’ clinical acumen and measure their progression along the emergency medicine milestones pathway.
This case was administered to 40 residents and used as one of three cases during an oral board simulation examination. Both interns and senior residents participated. Learner feedback for this case was positive, and learners were generally pleased with the case, rating it 4.6 out of 5 (n=25) on a 1–5 point Likert scale on overall enjoyment of the case (1 = poor, 5 = excellent). Learners overwhelmingly preferred the activity to a lecture format, rating 4.8 out of 5 (n=25) on a 1–5 Likert scale (1 = prefer lecture, 5 = prefer oral board testing). We also asked learners to provide open-ended comments, and these were generally positive, including, “I like being one-on-one with the attending to get a little more personal attention,” “This was my first time really managing alcohol withdrawal without a senior there, so it was helpful to go through the process,” and “I’d rather do this here than at ABEM general.”
The first iteration of this case was tested on five learners and required learners to calculate a CIWA-Ar score on their own. This requirement was removed after one session due to lack of utility; instructors and learners alike felt that this was both unnecessary from a learning standpoint and was unlikely to be tested in an oral board exam, and it was subsequently removed.
We feel this oral board case is highly testable and relevant in emergency medicine, and reinforces clinical and pharmacologic knowledge in a low-stakes setting.
Pearls
- Alcohol withdrawal is a clinical diagnosis and should be taken into consideration within a broad infectious/toxic/metabolic differential so as not to prematurely close on an incorrect course of management.ref. 3
- Suspect alcohol withdrawal in a patient with a history of alcohol use disorder who reduces or ceases intake and presents with two or more of the following:
- Severity of alcohol withdrawal symptoms can be determined by the Clinical Institute Withdrawal Assessment of Alcohol Scale, revised (CIWA-Ar), with scores ranging from 0–67.ref. 9, ref. 10
- Alcohol withdrawal symptoms typically begin a few hours after reduction or cessation in intake, peak at one to three days, and can last up to 14 days.ref. 3
- Life-threatening complications of alcohol withdrawal include seizures (6–15% of patients) and Delirium Tremens (3–5% of hospitalized patients).ref. 2
- Patients may exhibit malnourishment and have severe electrolyte imbalances. Life-threatening hypoglycemia, hypomagnesemia, hypokalemia and hyponatremia may need urgent correction. Consider co-administration of thiamine while administering glucose.ref. 8
- Symptom-triggered management, as directed by a patient’s CIWA-Ar score, is preferred over a fixed-dose strategy, and the intent is to achieve a lightly dozing but arousable state.ref. 11
- First-line treatment for alcohol withdrawal is the administration of benzodiazepines.
- Alternative treatment agents:
| Vitals: | HR 107 | BP 181/98 | RR 14 | Temp 36.4°C (97.5°F) | O2Sat 98% (room air) |
| Milestone | Did not achieve level 1 | Level 1 | Level 2 | Level 3 | |
|---|---|---|---|---|---|
| 1 | Emergency Stabilization (PC1) | □Did not achieve Level 1 | □Recognizes abnormal vital signs | □Recognizes an unstable patient, requiring interventionPerforms primary assessmentDiscerns data to formulate a diagnostic impression/plan | □Manages and prioritizes critical actions in a critically ill patientReassesses after implementing a stabilizing intervention |
| 2 | Performance of focused history and physical (PC2) | □Did not achieve Level 1 | □Performs a reliable, comprehensive history and physical exam | □Performs and communicates a focused history and physical exam based on chief complaint and urgent issues | □Prioritizes essential components of history and physical exam given dynamic circumstances |
| 3 | Diagnostic studies (PC3) | □Did not achieve Level 1 | □Determines the necessity of diagnostic studies | □Orders appropriate diagnostic studiesPerforms appropriate bedside diagnostic studies/procedures | □Prioritizes essential testingInterprets results of diagnostic studiesConsiders risks, benefits, contraindications, and alternatives to a diagnostic study or procedure |
| 4 | Diagnosis (PC4) | □Did not achieve Level 1 | □Considers a list of potential diagnoses | □Considers an appropriate list of potential diagnosisMay or may not make correct diagnosis | □Makes the appropriate diagnosisConsiders other potential diagnoses, avoiding premature closure |
| 5 | Pharmacotherapy (PC5) | □Did not achieve Level 1 | □Asks patient for drug allergies | □Selects an appropriate medication for therapeutic intervention, considering potential adverse effects | □Selects the most appropriate medication(s) and understands mechanism of action, effect, and potential side effectsConsiders and recognizes drug-drug interactions |
| 6 | Observation and reassessment (PC6) | □Did not achieve Level 1 | □Reevaluates patient at least one time during the case | □Reevaluates patient after most therapeutic interventions | □Consistently evaluates the effectiveness of therapies at appropriate intervals |
| 7 | Disposition (PC7) | □Did not achieve Level 1 | □Appropriately selects whether to admit or discharge the patient | □Appropriately selects whether to admit or dischargeInvolves the expertise of some of the appropriate specialists | □Educates the patient appropriately about their dispositionAssigns patient to an appropriate level of care (ICU/Tele/Floor)Involves expertise of all appropriate specialists |
| 22 | Patient centered communication (ICS1) | □Did not achieve level 1 | □Establishes rapport and demonstrates empathy to patient (and family)Listens effectively | □Elicits patient’s reason for seeking health care | □Manages patient expectations in a manner that minimizes potential for stress, conflict, and misunderstanding. |
| 23 | Team management (ICS2) | □Did not achieve level 1 | □Recognizes other members of the patient care team during case (nurse, techs) | □Communicates pertinent information to other healthcare colleagues | □Communicates a clear, succinct, and appropriate handoff with specialists and other colleaguesCommunicates effectively with ancillary staff |
| #1 | Patient Information Form |
| #2 | Venous blood gas |
| #3 | CBC |
| #4 | BMP |
| #5 | Urinalysis |
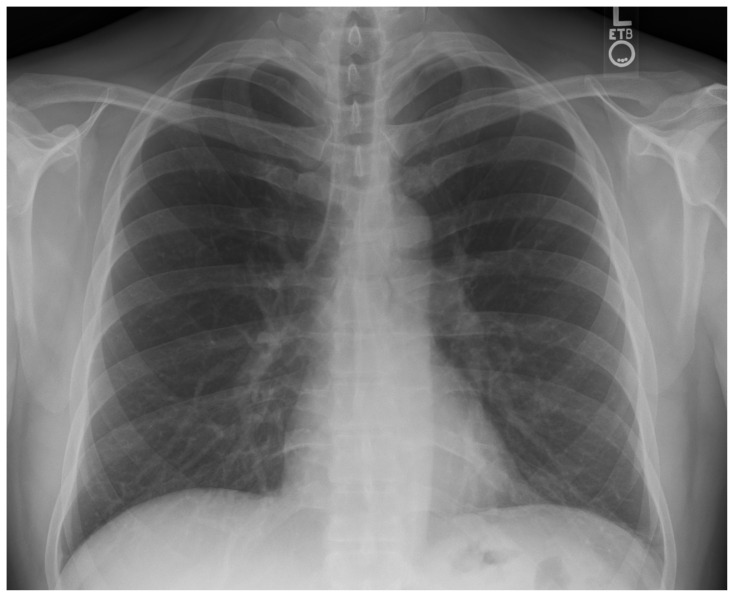
| #6 | CXR |
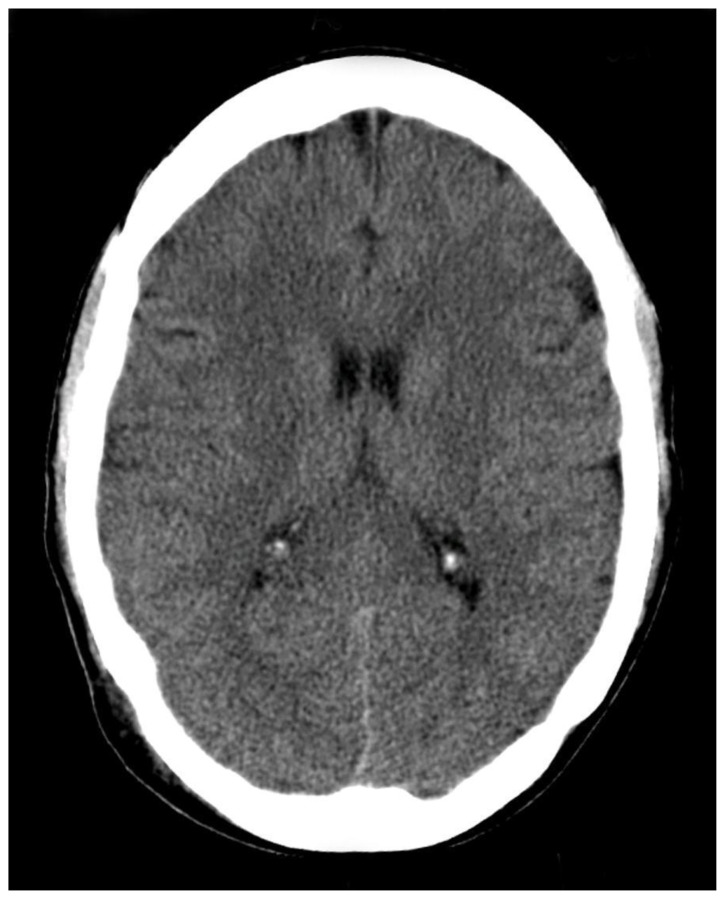
| #7 | Head-CT |
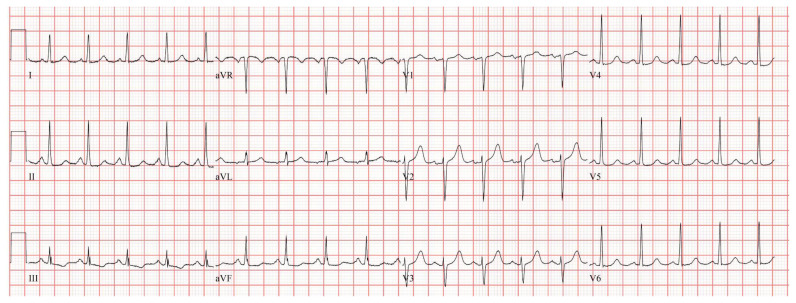
| #8 | EKG |
| #9 | Toxicology (serum and urine) |
| #10 | Hepatic function panel |
| #11 | Magnesium level |
| #12 | Cardiac markers |
| #13 | Coagulation panel |
| Patient’s Name: | Mark Jones |
| Age: | 47 |
| Gender: | M |
| Chief Complaint: | Intoxication |
| Person Providing History: | EMS, patient |
| Vital Signs: | |
| Temp: | 36.4°C (97.5°F) |
| BP: | 181/98 |
| P: | 107 |
| RR: | 14 |
| Pulse Ox: | 98% (room-air) |
| Weight: | 93 kg (205 lb) |
| pH | 7.18 |
| pCO2 | 38 mmHg |
| pO2 | 78 mmHg |
| HCO3 | 21 mmol/L |
| O2 | sat 96% |
| WBC | 14.4 × 103/μL |
| Hgb | 11.7 g/dL |
| Hct | 34.2% |
| Platelets | 290 × 103/μL |
| Differential | |
| Neutrophils | 58% |
| Lymphocytes | 32% |
| Monocytes | 4% |
| Eosinophils | 3% |
| Bands | 3% |
| Na | 144 mEq/L |
| K | 2.3 mEq/L |
| Cl | 102 mEq/L |
| CO2 | 20 mEq/L |
| BUN | 28 mg/dL |
| Cr | 1.9 mg/dL |
| Glucose | 133 mg/dL |
| Appearance | Clear |
| Color | Yellow |
| Glucose | Trace |
| Ketones | 2+ |
| Sp Gravity | 1.020 |
| Blood | Negative |
| pH | 6.5 |
| Protein | Negative |
| Nitrite | Negative |
| Leukocyte | Negative |
| WBC | 0–2/hpf |
| RBC | 0–2/hpf |
| Squamous Cells | 15/hpf |
| Bacteria | 0–2/hpf |
| Amphetamines: | Negative |
| Barbiturates: | Negative |
| Benzodiazepines: | Negative |
| Cocaine: | Negative |
| Opiates: | Negative |
| Cannabinoids: | Positive |
| Acetaminophen: | <10 mCg/mL |
| Salicylates: | <15 mg/dL |
| Ethanol: | 115 mg/dL |
| ALT | 80 IU/L |
| AST | 129 IU/L |
| AlkPhos | 88 IU/L |
| T-bili | 1.0 mg/dL |
| Direct Bilirubin | 0.5 mg/dL |
| Magnesium | 1.4 mEq/L |
| Troponin – I | 24 ng/L |
| Reference: < 20 ng/L – normal; | |
| 20 ng/L – 80 ng/L – indeterminant; | |
| > 80 ng/L – elevated | |
| BNP | 71 pg/ml |
| Reference: < 90 pg/ml – normal |
| PTT: | 29.1 seconds |
| PT: | 15.1 seconds |
| INR: | 1.1 |
References
- BF Grant, RB Goldstein, TD Saha. Epidemiology of DSM-5 Alcohol Use Disorder: Results from the national epidemiologic survey on alcohol and related conditions III. JAMA Psychiatry, 2015. [DOI | PubMed]
- D Long, B Long, A Koyfman. The emergency medicine management of severe alcohol withdrawal. Am J Emerg Med, 2017. [DOI | PubMed]
- MA Schuckit. Recognition and management of withdrawal delirium (delirium tremens). N Engl J Med, 2014. [DOI | PubMed]
- A Rahman, M Paul. Delirium Tremens. StatPearls, 2023
- KJ Schmidt, MR Doshi, JM Holzhausen, A Natavio, M Cadiz, JE Winegardner. Treatment of severe alcohol withdrawal. Ann Pharmacother, 2016. [DOI | PubMed]
- A Wong, NJ Benedict, MJ Armahizer, SL Kane-Gill. Evaluation of adjunctive ketamine to benzodiazepines for management of alcohol withdrawal syndrome. Ann Pharmacother, 2015. [DOI | PubMed]
- J Rosenson, C Clements, B Simon. Phenobarbital for acute alcohol withdrawal: A prospective randomized double-blind placebo controlled study. JEM, 2013. [DOI]
- G Airagnes, G Ducoutumany, B Laffy-Beaufils, AL Le Faou, F Limosin. Alcohol withdrawal syndrome management: Is there anything new?. Rev Med Interne, 2019. [DOI | PubMed]
- K Ng, K Dahri, I Chow, M Legal. Evaluation of an alcohol withdrawal protocol and a preprinted order set at a tertiary care hospital. Can J Hosp Pharm, 2011. [DOI | PubMed]
- MA Nuss, DM Elnicki, TS Dunsworth, EH Makela. Utilizing CIWA-Ar to assess use of benzodiazepines in patients vulnerable to alcohol withdrawal syndrome. W V Med J, 2004. [PubMed]
- J Daeppen, P Gache, U Landry. Symptom-triggered vs fixed-schedule doses of benzodiazepine for alcohol withdrawal: A randomized treatment trial. Arch Intern Med, 2002. [DOI | PubMed]