Intrahepatic Rupture of Acute Cholecystitis Complicated by Septic Portal Thrombosis
Abstract
Gallbladder rupture, though rare, is a serious complication often arising from choledocholithiasis and subsequent interventions such as endoscopic retrograde cholangiopancreatography (ERCP). In this case, the patient presented with acute choledocholithiasis and underwent ERCP with sphincterotomy and stone extraction, followed by placement of a fully covered metal stent in the common bile duct (CBD). While the use of covered stents is appropriate, it is important to note that these stents can obstruct the cystic duct orifice in patients with a gallbladder. This occurs in more than 33% of patients with a low cystic duct junction, leading to obstructive acute cholecystitis, as seen in patients with pancreatic ductal adenocarcinoma (PDAC) or distal cholangiocarcinoma who receive metal biliary stents. In this case, the patient developed a liver abscess following a gallbladder rupture, likely due to the stent obstructing the cystic duct. The liver abscess was managed with percutaneous drainage, and cultures grew Streptococcus anginosus, a common pathogen in hepatobiliary infections. The patient was treated with IV piperacillin-tazobactam, followed by oral amoxicillin-clavulanate for a 4-6 week course. Additionally, portal vein thrombosis, a known complication of severe infection, was identified and treated with anticoagulation. This case highlights the need for careful stent selection and possible prophylactic cholecystectomy in patients with a functioning gallbladder to prevent post-ERCP complications like cholecystitis and abscess formation. Early diagnosis, timely drainage, and appropriate antibiotic therapy are critical to managing such complex hepatobiliary conditions.
Article type: Case Report
Keywords: biliary fistula, biliary stent, cholangitis, cholecystitis, ercp, gallbladder, gallbladder rupture, liver abscess
License: Copyright © 2024, Louis et al. CC BY 4.0 This is an open access article distributed under the terms of the Creative Commons Attribution License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Article links: DOI: 10.7759/cureus.73865 | PubMed: 39697909 | PMC: PMC11652117
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (5.7 MB)
Introduction
In managing choledocholithiasis, endoscopic retrograde cholangiopancreatography (ERCP) with stone extraction and stent placement is often the treatment of choice [ref. 1]. However, in patients with an intact gallbladder, the use of a fully covered metal stent presents a unique risk [ref. 2]. While effective at maintaining biliary drainage, these stents can inadvertently occlude the cystic duct orifice [ref. 3]. This leads to obstructive acute cholecystitis in a significant portion of patients, particularly those with a low cystic duct junction, making it a crucial consideration during stent selection and post-procedural care [ref. 4]. The incidence of acute cholecystitis following the placement of fully covered metal stents ranges from 3% to 12%, though progression to gallbladder rupture remains rare and is not well-documented.
Obstruction of the cystic duct orifice by a stent can trigger severe inflammation, bile stasis, and infection, as bile flow from the gallbladder is blocked [ref. 4]. Without appropriate intervention, this obstruction may progress to gallbladder rupture, biliary fistula formation, and the development of liver abscesses, as bile and bacteria infiltrate adjacent structures [ref. 5]. Early recognition of this complication, along with consideration for prophylactic cholecystectomy in certain high-risk patients, is essential to prevent serious outcomes and optimize recovery [ref. 6].
Case presentation
A 30-year-old male presented with subacute progressive right upper quadrant abdominal pain, nausea, and bilious emesis. The patient denied any history of inflammatory bowel disease, alcohol use, sick exposures, or abdominal trauma/surgery. He had previous cocaine and methamphetamine abuse.
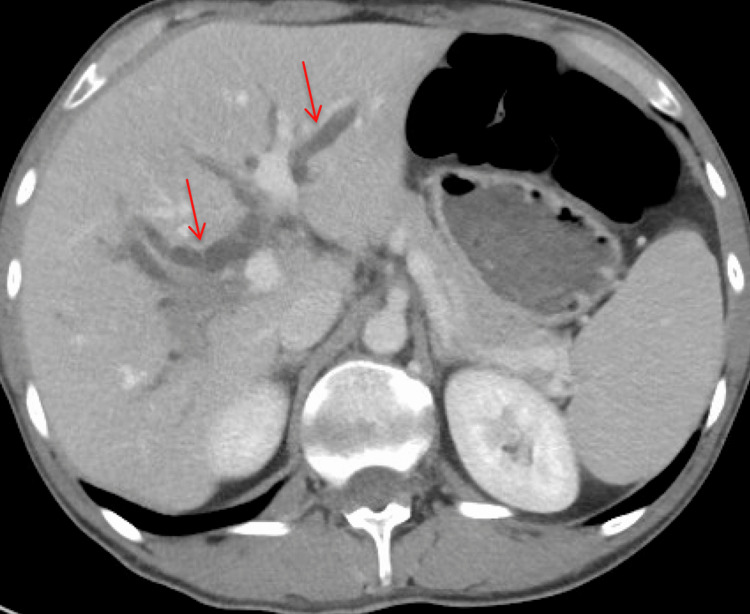
On physical examination, the patient was afebrile with stable vital signs. Laboratory investigations are shown in Table 1. A CT scan of the abdomen and pelvis identified diffuse intra and extrahepatic biliary ductal dilation without obstructing stone or mass (Figure 1).
Table 1: AST: aspartate aminotransferase; ALT: alanine aminotransferase; H&H: hemoglobin and hematocrit; ALP: alkaline phosphatase; WBS: white blood cells; UA: urinalysis
| Lab test | Result | Reference range |
| AST | 138 U/L | 10-40 U/L |
| ALT | 218 U/L | 7-56 U/L |
| Total bilirubin | 9.0 mg/dL | 0.1-1.2 mg/dL |
| Direct bilirubin | 6.2 mg/dL | 0-0.4 mg/dL |
| WBC | 10.6 x 109/L | 4.5-11 x 109/L |
| Lipase | 25 U/L | 0-160 U/L |
| UA (bilirubin) | Moderate | Negative |
| pH (UA) | 8.0 | 4.5-8.0 |
| Total protein (UA) | Trace | Negative |
| Total bilirubin (day 2) | 7.29 mg/dL | 0.1-1.2 mg/dL |
| AST (day 2) | 36 U/L | 10-40 U/L |
| ALT (day 2) | 107 U/L | 7-56 U/L |
| ALP (day 2) | 237 U/L | 44-147 U/L |
| WBC (day 2) | 12.1 x 109/L | 4.5-11 x 109/L |
| H&H | 13.5/40.5 | Hemoglobin: 13.5-17.5 g/dL, hematocrit: 41-50% |
| Platelets | 342 x 109/L | 150-400 x 109/L |
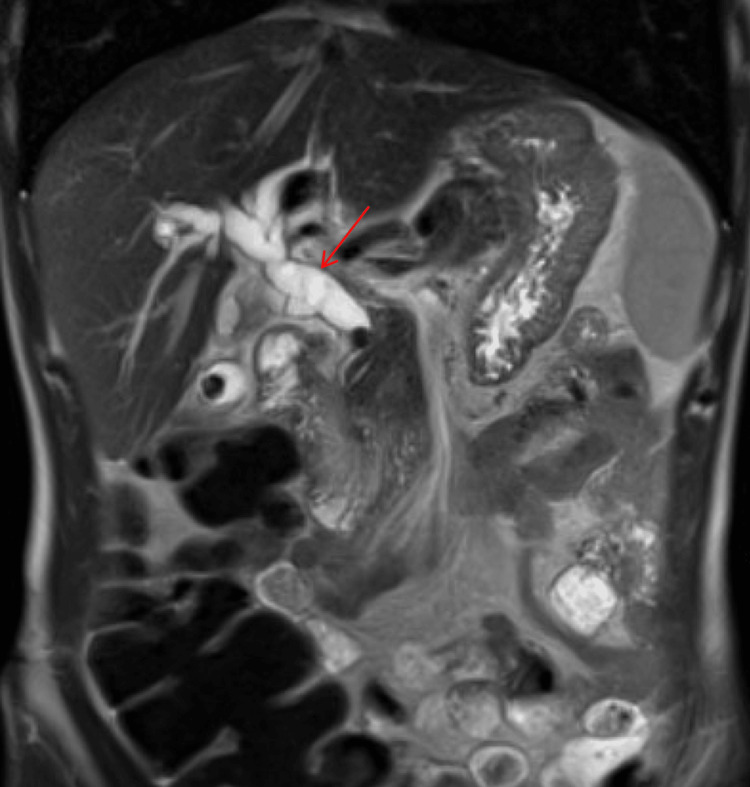
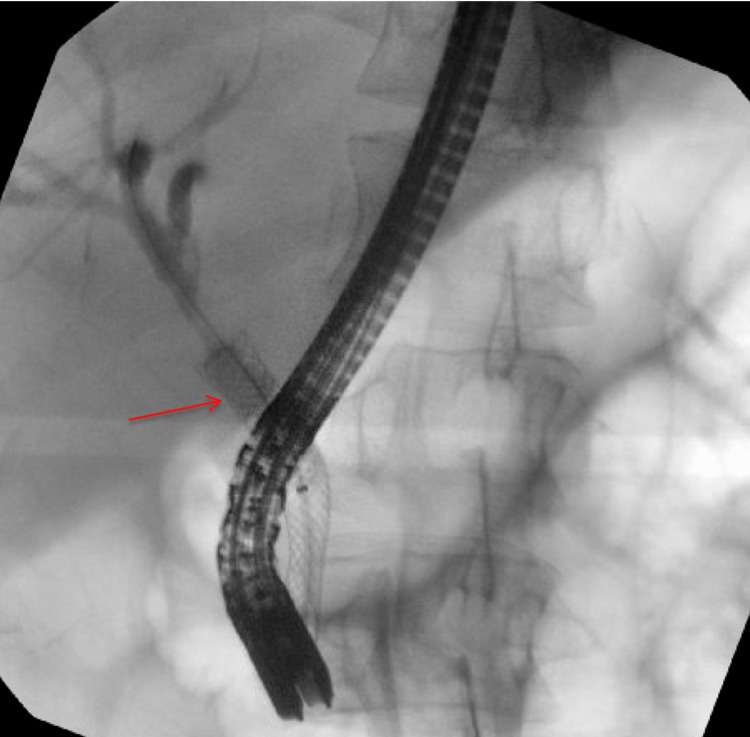
An MRCP demonstrated choledocholithiasis within the distal common bile duct (CBD) with significant intra and extrahepatic ductal dilation (Figure 2). He underwent an endoscopic retrograde cholangiopancreatography with sphincterotomy. Multiple stones were removed; however, due to concern for residual retained stones, a 10 French fully covered metal endobiliary stent was placed (Figure 3). A prophylactic plastic endopancreatic stent was also placed in the dorsal pancreatic duct due to incidental cannulation.
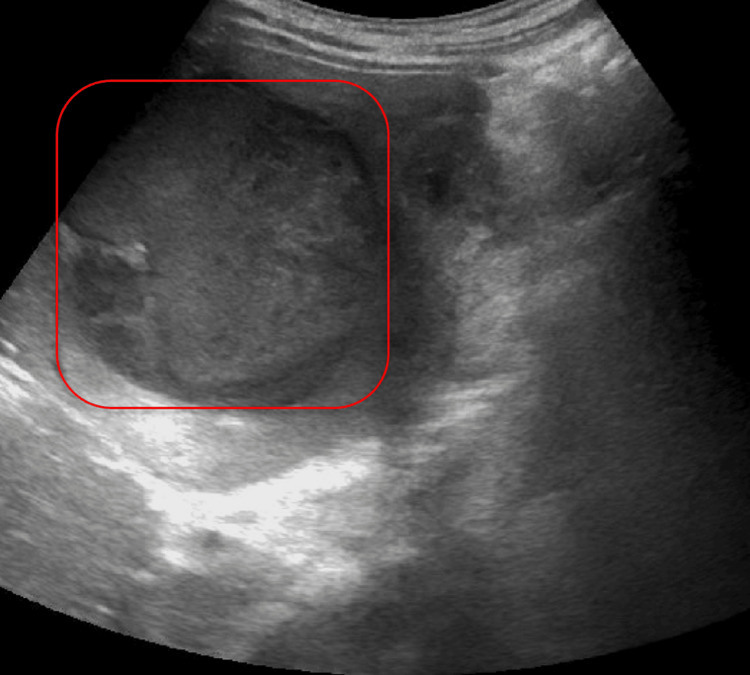
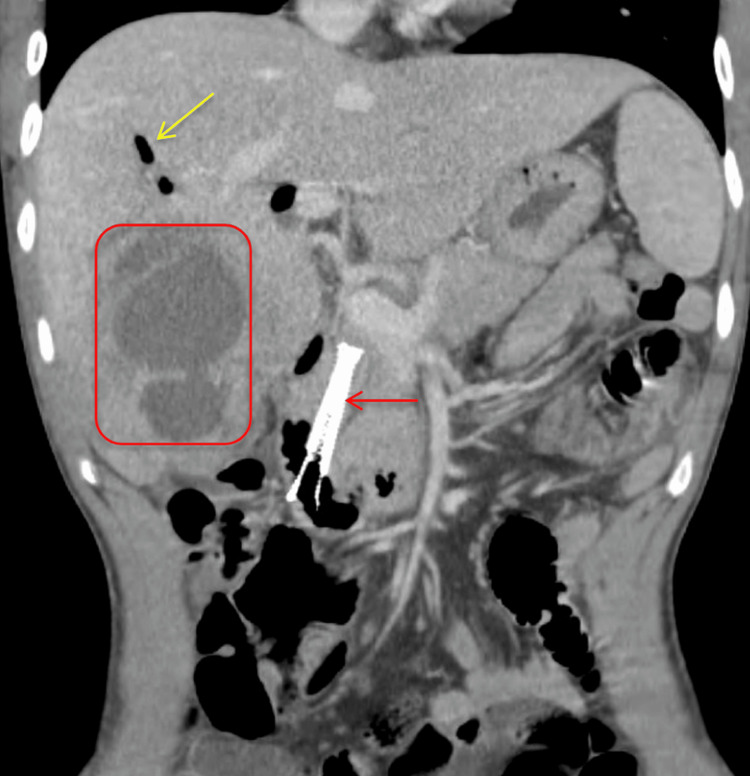
Post-procedure, the patient developed improved jaundice and abdominal pain and was able to tolerate a regular diet with discharge home on the fifth post-procedure day. He re-presented three weeks later due to progressive cramping abdominal right upper quadrant (RUQ) pain, nausea, and bilious emesis. An abdominal ultrasound and CT demonstrated a large 8.5 cm liver abscess in the right hepatic lobe, with a posterior defect in the hepatic margin of the gallbladder wall (Figures 4–6). There was noted septic thrombosis of the right portal venous system. He underwent emergent CT-guided percutaneous transhepatic drainage of the liver abscess, with cultures demonstrating Streptococcus anginosus. He was initiated on empiric IV piperacillin-tazobactam, followed by a transition to a four-week course of oral amoxicillin-clavulanate 875-125 mg twice daily after sensitivity results were completed. He was initiated on therapeutic enoxaparin followed by conversion to oral apixaban for a planned six-month course for portal thrombosis. Repeat CT imaging demonstrated stable portal thrombus without extension or enlarging hepatic abscess. He was discharged home with planned interval endobiliary stent removal and delayed interval cholecystectomy. No complications or recurrent symptoms were observed during the patient’s follow-up after discharge.

Discussion
The use of a fully covered metal stent during ERCP is a common and effective solution for biliary drainage in cases of choledocholithiasis [ref. 7]. However, in patients with an intact gallbladder, the placement of such stents can introduce complications [ref. 8]. Fully-covered stents have a significant risk of obstructing the cystic duct orifice, particularly in patients with a low cystic duct junction [ref. 9]. This anatomical feature occurs in over 33% of cases, making it a critical factor to consider during stent placement [ref. 10,ref. 11]. When the cystic duct becomes obstructed, bile cannot drain from the gallbladder, leading to bile stasis and acute cholecystitis [ref. 12]. Without timely intervention, this can escalate into more serious complications, such as gallbladder rupture, as seen in this case [ref. 13]. While the use of fully covered metal stents in managing choledocholithiasis is common, cases like this one, where the stent placement led to cystic duct obstruction and subsequent gallbladder rupture, remain rare. Comparatively, most documented cases involving ERCP and stenting complications tend to present with acute cholecystitis rather than progressing to rupture and abscess formation [ref. 2].
Once the gallbladder ruptures, the potential for serious complications increases dramatically [ref. 14]. In this case, bile and bacteria leaked from the gallbladder into surrounding structures, forming a fistula between the gallbladder and the liver [ref. 13]. This direct communication allowed the spread of infection into the liver parenchyma, resulting in a large hepatic abscess [ref. 15]. Gallbladder ruptures are rare, but when they occur, they often lead to the development of liver abscesses, which are polymicrobial in nature [ref. 16]. Streptococcus anginosus, a frequent pathogen in biliary infections, was cultured from this patient’s abscess, consistent with the fistulous connection between the inflamed gallbladder and the liver [ref. 17,ref. 18]. Imaging, including ultrasound and CT, played a crucial role in diagnosing both the gallbladder rupture and the liver abscess, guiding the therapeutic approach [ref. 19].
ERCP with sphincterotomy and stone extraction remains the cornerstone of treatment for choledocholithiasis [ref. 1]. However, the decision to place a fully-covered metal stent in patients with an intact gallbladder requires careful consideration due to the risk of cystic duct occlusion [ref. 6]. In some cases, a prophylactic cholecystectomy should be considered, especially when the anatomy suggests a high likelihood of the stent covering the cystic duct [ref. 20]. In patients with pancreatic ductal adenocarcinoma (PDAC) or distal cholangiocarcinoma, the same risk exists when metal biliary stents are used, often resulting in fevers, chills, and right upper quadrant pain due to the blocked cystic duct [ref. 9]. Therefore, in patients receiving fully-covered metal stents, vigilant monitoring and consideration of surgical intervention are critical to prevent severe outcomes like obstructive cholecystitis or, as in this case, gallbladder rupture [ref. 21].
After the liver abscess was identified, prompt percutaneous drainage under CT guidance was performed to reduce the risk of further infection and sepsis [ref. 19]. Drainage remains the gold standard for managing large abscesses, especially when surgical resection is not feasible [ref. 15]. Coupled with targeted antibiotic therapy, drainage is critical for preventing the spread of infection and ensuring resolution [ref. 17]. In this case, the patient was initially treated with broad-spectrum antibiotics, including piperacillin-tazobactam, followed by a course of oral amoxicillin-clavulanate to cover the common biliary pathogens identified in the abscess culture. The prolonged antibiotic therapy helped prevent recurrence and allowed for a full recovery from the infection.
Complicating the course of this patient’s condition was the development of portal vein thrombosis, a recognized but serious complication of hepatobiliary infections [ref. 22]. Severe inflammation and infection within the liver can create a hypercoagulable state, increasing the risk of thrombosis in nearby vascular structures [ref. 23]. Portal vein thrombosis can lead to complications such as bowel ischemia or portal hypertension if left untreated [ref. 24]. In this case, therapeutic anticoagulation was initiated early to prevent these complications and promote resolution of the thrombosis.
Here, we illustrate the potential dangers associated with stent placement in patients with an intact gallbladder. The stent induced obstruction of the cystic duct, leading to gallbladder rupture. While ERCP remains an essential tool in managing choledocholithiasis, we must remain vigilant for post-procedure complications, particularly in patients receiving fully-covered stents. Early identification of complications such as liver abscesses and portal vein thrombosis, along with appropriate interventions like drainage and anticoagulation, are essential to ensure favorable outcomes in these complex cases. Alternative approaches, such as using partially covered or plastic stents, may reduce the risk of cystic duct obstruction in patients with an intact gallbladder. In high-risk cases, a prophylactic cholecystectomy could also be considered to prevent complications associated with stent-induced cystic duct occlusion.
Conclusions
In patients with an intact gallbladder undergoing ERCP, fully covered metal stents should be used cautiously due to the risk of cystic duct obstruction, which can lead to complications like acute cholecystitis and, in rare cases, gallbladder rupture. Practitioners should consider alternative stenting options, such as partially covered or prophylactic cholecystectomy for high-risk patients. Prompt imaging, drainage, and targeted antibiotic therapy are essential for managing liver abscesses if they develop. Early recognition of complications and a multidisciplinary approach can significantly improve patient outcomes in such complex cases.
References
- A Copelan, BS Kapoor. Choledocholithiasis: diagnosis and management. Tech Vasc Interv Radiol, 2015. [PubMed]
- R Lam, T Muniraj. Fully covered metal biliary stents: a review of the literature. World J Gastroenterol, 2021. [PubMed]
- P Aepli, A St John, S Gupta, LF Hourigan, R Vaughan, M Efthymiou, A Kaffes. Success and complications of an intra-ductal fully covered self-expanding metal stent (ID-FCSEMS) to treat anastomotic biliary strictures (AS) after orthotopic liver transplantation (OLT). Surg Endosc, 2017. [PubMed]
- K Yamao, M Takenaka, T Ogura. Utility and safety of a novel fully covered metal stent in unresectable distal malignant biliary obstruction. Dig Dis Sci, 2020. [PubMed]
- KT Suk, HS Kim, JW Kim. Risk factors for cholecystitis after metal stent placement in malignant biliary obstruction. Gastrointest Endosc, 2006. [PubMed]
- JH Jung, SW Park, B Hyun, J Lee, DH Koh, D Chung. Identification of risk factors for obstructive cholecystitis following placement of biliary stent in unresectable malignant biliary obstruction: a 5-year retrospective analysis in single center. Surg Endosc, 2021. [PubMed]
- CH Wu, SF Wang, MH Lee. Efficacy of fully covered self-expandable metal stents for distal biliary obstruction caused by pancreatic ductal adenocarcinoma: primary metal stent vs. metal stent following plastic stent. Cancers, 2023
- H Isayama, T Kawabe, Y Nakai. Cholecystitis after metallic stent placement in patients with malignant distal biliary obstruction. Clin Gastroenterol Hepatol, 2006. [PubMed]
- M Watanabe, K Okuwaki, J Woo. Cholecystitis after placement of covered self-expandable metallic stents in patients with distal malignant biliary obstructions. Clin Endosc, 2021. [PubMed]
- I Tsitouridis, G Lazaraki, C Papastergiou, E Pagalos, G Germanidis. Low conjunction of the cystic duct with the common bile duct: does it correlate with the formation of common bile duct stones?. Surg Endosc, 2007. [PubMed]
- S Uetsuji, Y Okuda, H Komada, M Yamamura, Y Kamiyama. Clinical evaluation of a low junction of the cystic duct. Scand J Gastroenterol, 1993. [PubMed]
- A Taghavi, M Azizi, A Rasekhi, Z Gholami. Anatomic variations of the cystic duct in magnetic resonance cholangiopancreatography in Shiraz: a cross-sectional study. Iran J Med Sci, 2022. [PubMed]
- A Peer, E Witz, H Manor, S Strauss. Intrahepatic abscess due to gallbladder perforation. Abdom Imaging, 1995. [PubMed]
- RS Date, SG Thrumurthy, S Whiteside, MA Umer, KG Pursnani, JB Ward, MM Mughal. Gallbladder perforation: case series and systematic review. Int J Surg, 2012. [PubMed]
- EA Bakalakos, WS Melvin, R Kirkpatrick. Liver abscess secondary to intrahepatic perforation of the gallbladder, presenting as a liver mass. Am J Gastroenterol, 1996. [PubMed]
- K Singh, A Singh, SH Vidyarthi, S Jindal, CK Thounaojam. Spontaneous intrahepatic type II gallbladder perforation: a rare cause of liver abscess – case report. J Clin Diagn Res, 2013. [PubMed]
- F Bonenfant, E Rousseau, P Farand. Streptococcus anginosus pyogenic liver abscess following a screening colonoscopy. Can J Infect Dis Med Microbiol, 2013
- BR Karki, L Costanzo, SK Jha, S Nainan, SI McFarlane. Multiple hepatic abscesses secondary to Streptococcus anginosus infection: a case report and review of the literature. Cureus, 2022
- S Lardière-Deguelte, E Ragot, K Amroun. Hepatic abscess: diagnosis and management. J Visc Surg, 2015. [PubMed]
- G Mc Geehan, C Melly, N O’ Connor. Prophylactic cholecystectomy offers best outcomes following ERCP clearance of common bile duct stones: a meta-analysis. Eur J Trauma Emerg Surg, 2023. [PubMed]
- H Kawabata, Y Kawakatsu, K Yamaguchi. Prophylactic biliary stenting before cholecystectomy in patients with gallstones and common bile duct stones. Gastroenterology Res, 2019. [PubMed]
- M García-Gutiérrez, R Luque-Márquez, S Rodríguez-Suárez. Portal vein thrombosis associated with biliary tract infection. [Article in Spanish]. Gastroenterol Hepatol, 2012. [PubMed]
- FR Ponziani, MA Zocco, C Campanale. Portal vein thrombosis: insight into physiopathology, diagnosis, and treatment. World J Gastroenterol, 2010. [PubMed]
- Y Zhang, BY Xu, XB Wang. Prevalence and clinical significance of portal vein thrombosis in patients with cirrhosis and acute decompensation. Clin Gastroenterol Hepatol, 2020. [PubMed]