An economic evaluation of implementing a decentralized dengue screening intervention under the National Vector Borne Disease Control Programme in Tamil Nadu, South India
Abstract
Background:
Lack of effective early screening is a major obstacle for reducing the fatality rate and disease burden of dengue. In light of this, the government of Tamil Nadu has adopted a decentralized dengue screening strategy at the primary healthcare (PHC) facilities using blood platelet count. Our objective was to determine the cost-effectiveness of a decentralized screening strategy for dengue at PHC facilities compared with the current strategy at the tertiary health facility (THC) level.
Methods:
Decision tree analysis followed a hypothetical cohort of 1000 suspected dengue cases entering the model. The cost-effectiveness analysis was performed at a 3% discount rate for the proposed and current strategy. The outcomes are expressed in incremental cost-effectiveness ratios (ICERs) per quality-adjusted life years gained. One-way sensitivity analysis and probabilistic sensitivity analysis were done to check the uncertainty in the outcome.
Results:
The proposed strategy was found to be cost-saving and ICER was estimated to be −41 197. PSA showed that the proposed strategy had a 0.84 probability of being an economically dominant strategy.
Conclusions:
The proposed strategy is cost-saving, however, it is recommended to consider optimal population coverage, costs to economic human resources and collateral benefits of equipment.
Article type: Research Article
Keywords: cost-effectiveness, dengue, economic evaluation, QALY, screening
Affiliations: Scientist-D & Head, Department of Health Economics, ICMR-National Institute for Research in Tuberculosis, No. 1, Sathyamoorthy Road, Chetpet, Chennai 60003, India; Department of Health Research, Ministry of Health and Family Welfare, 2nd Floor, IRCS Building, 1, Red Cross Road, New Delhi 110001, India; Department of Public Health and Preventive Medicine, Government of Tamil Nadu, 359, Anna Salai, Chokkalingam Nagar, Teynampet, Chennai 600006, India
License: © The Author(s) 2021. Published by Oxford University Press on behalf of Royal Society of Tropical Medicine and Hygiene. CC BY 4.0 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted reuse, distribution, and reproduction in any medium, provided the original work is properly cited.
Article links: DOI: 10.1093/inthealth/ihab045 | PubMed: 34453836 | PMC: PMC9070504
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (669 KB)
Introduction
Dengue is the most common vector-borne infection globally, with an estimated 100–400 million infections occurring every year.1 There is no effective vaccine or medicine available to prevent or cure dengue and it leads to around 20 000 deaths per year.2 Symptomatic dengue infections have a broad range of severity and the clinical characteristics of dengue may mimic other disease characteristics, which increases the probability of misdiagnosis.3
India contributes around 34% of the global burden of dengue.4 A meta-analysis of Indian studies estimated the dengue fatality rate to be 2.6%.5 Although dengue is a notifiable disease in India, studies and modelling estimates suggest that the disease is grossly underreported due to the existing gaps in the public health surveillance system. Dengue surveillance in India is conducted through a network of >600 sentinel hospitals under the National Vector-Borne Disease Control Programme (NVBDCP), Integrated Disease Surveillance Program (IDSP) and a network of 52 Virus Research and Diagnostic Laboratories (VRDLs).6 Tamil Nadu (TN) is one of the largest states in India and reported a high burden of dengue infection.7 High dengue disease burden and frequent outbreaks result in an adverse impact on the country’s economy and strain the health system.
One of the major hindrances in the control and management of dengue infection is the lack of timely and point-of-care diagnosis in TN. The complex clinical presentation of dengue symptoms and a lack of effective screening and diagnosis results in delayed diagnosis and leads to rapid disease progression and mortality. Dengue diagnosis and management in India is undertaken as per NVBDCP8 guidelines that recommend screening of platelet counts and enzyme-linked immunosorbent assay (ELISA) testing for confirmation. Currently both screening and confirmatory testing for a dengue diagnosis are being done only at the tertiary healthcare (THC) facilities in TN, which requires multiple visits. This results in an increased patient load at the THC facilities and remains a barrier for access by all sections of the population. It also leads to increased out-of-pocket expenditures for patients, delay in diagnosis, delay in treatment and loss to follow-up for treatment.
To address this gap in the dengue diagnostic cascade, the government of TN has adopted a decentralized dengue screening strategy at the primary healthcare (PHC) facilities. In this strategy, haematology analyser equipment is installed at the PHC facilities for screening suspected dengue cases with low platelet count (thrombocytopenia) who will be further referred to a THC facility for confirmation and disease management. The strategy of using platelet counts (thrombocytopenia) for predicting dengue has been increasingly recognised in the research literature as a valid screening tool. Studies have shown the importance of haematology analysers in hospital-based settings with a minimal patient load.9,10 This strategy prioritizes the present delay in diagnosing dengue at an earlier stage, which could help reduce dengue morbidity and mortality. However, the implementation of such a screening strategy has not been studied for its suitability in large community settings with a high dengue burden. In the absence of any large-scale primary evaluation studies, we utilised economic modelling to provide evidence for policymakers to implement evidence-based interventions. Thus the objective of this study was to determine the cost-effectiveness of a decentralized screening strategy for dengue at PHC facilities compared with the current strategy at THC facilities.
Methods
This economic evaluation was conducted by following the Consolidated Health Economic Evaluation Reporting Standards guidelines (eTable 1). This is a model-based study from a societal perspective for the year 2019.
Study setting and population
The study was conducted in TN, where the decentralized screening strategy has been implemented at the district level. Further, this strategy is being considered for scale-up at the subdistrict level in a phased manner. Our study population represents a hypothetical cohort of 1000 individuals who access care at PHC facilities in these settings with fever and symptoms suggestive of dengue.
Comparator and time horizon
The present model compares the proposed decentralized dengue screening strategy at the PHC facilities with the current screening strategy used for dengue diagnosis at the THC facilities. Under the decentralized strategy, point-of-care screening is provided for those who access PHC facilities with fever and symptoms suggestive of dengue. Both the strategies involve a confirmatory ELISA test for dengue at the THC facilities. A single episode of dengue infection with a lifetime horizon and a global discount rate of 3% is considered for the estimation of effectiveness and cost.
Model assumption
This economic model was conceptualized based on the natural history of dengue infection followed by ambulatory or hospitalization-based treatment and care. This model characterises all the health states of dengue from infection to cure or death. The specific assumptions used for the model were two repeat dengue screening tests at 2-d intervals followed by an ELISA test for those with a platelet count (PLC) >100 000/mm3 in the proposed strategy, one repeat dengue screening test at a 2-d interval with an ELISA test for those with a PLC >100 000/mm3 in the current strategy, a 50% reduction in severe dengue cases due to early diagnosis in the proposed strategy (based on expert opinion) and no loss to follow-up in the screening, diagnosis and treatment cascade (considered in both strategies, as there are no available data on loss-to-follow-up details).
Model structure
The present study utilised an economic model to calculate the incremental cost-effectiveness ratios (ICERs) for the current and proposed dengue screening strategies. The ICER is calculated from the cost and quality-adjusted life years (QALYs) of the two different strategies for dengue screening. The strategies considered for dengue diagnosis are summarized in Table 1.
Table 1.: Different screening strategies for dengue
| Strategies | Level of implementation | Diagnostic tool | Population | Frequency of screening | Referral |
|---|---|---|---|---|---|
| Proposed strategy | PHC | CBC for platelet level | Persons with febrile illness and warning signs | Repeat CBC at days 2 and 4 if PLC >100 000/mm3 | Tertiary for ELISA. If ELISA is positive, repeat CBC twice a day and hospitalize |
| Comparator | THC | CBC and ELISA | Persons with febrile illness and warning signs | Repeat CBC once for self-reporting patients at 2-d intervals if PLC >100 000/mm3 | If ELISA is positive, repeat CBC twice a day and hospitalize |
Current strategy
Patients with 2–5 d of febrile illness having two or more symptoms of headache, retro-orbital pain, myalgia, arthralgia, rash and haemorrhagic manifestations are considered as suspected dengue cases. The suspected dengue cases approaching the PHC facility were referred to the THC facility for diagnosis. At the THC facility, the symptoms are managed along with a dengue diagnosis. A dengue diagnosis in the THC facility is done by testing the PLC (<100 000/mm3) for screening and an ELISA test for confirmation. During treatment the patient is subjected to continuous monitoring at the THC facility for a reduction in the blood PLC.
Proposed strategy
For early diagnosis of dengue, it is proposed to screen the suspected dengue cases at the PHC facility using a haematology analyser. The PLC is assessed and those with <100 000/mm3 will be referred to the THC facility for further management and those with >100 000/mm3 will be reassessed at 2-d intervals. A maximum of two repeat PLCs will be undertaken to rule out dengue.
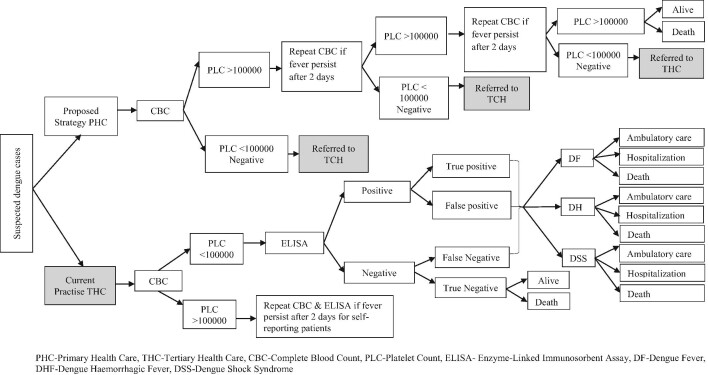
Decision tree model
The decision model planned for this study was constructed based on the natural progression of dengue and its diagnostic cascade (Figure 1).7,11–13 Both the proposed and current strategies were modelled as two parallel trees using probabilities associated with the dengue diagnosis, treatment and outcome. A patient diagnosed with dengue in each strategy was further classified based on the disease severity into three disease states: dengue fever (DF), dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS). In each disease state, the outcomes considered were survival after hospitalization, survival after ambulatory treatment and death. An Excel spreadsheet (Microsoft, Redmond, WA, USA) and TreeAge software (version 1.0; TreeAge Software, Williamstown, MA, USA) were used for analysis.
Model input parameters
The key input parameters for the model include demography;7 prevalence of dengue;5 prevalence of suspected dengue cases;14 sensitivity and specificity of the ELISA;4 health state probability of DF,15 DHF,14 DSS14 and death due to dengue;5 all-cause mortality;16 probability of cure;17 quality-of-life score for different health states18 and health system and patient costs incurred for dengue diagnosis and treatment.16,19 All this information was extracted from the published literature and NVBDCP reports. Table 2 presents the input parameter values used in the analysis with 20% upper and lower limits along with their distribution.
Table 2.: Input parameters used for model-based cost-effectiveness analysis of dengue screening at the PHC facility
| Parameters | To model | Lower limit | Upper limit | Distribution | Source | |
|---|---|---|---|---|---|---|
| Demographic values | Average age of suspected dengue cases (years) | 22 | NA | NA | NA | 5 |
| Life expectancy for an average age of suspected dengue cases (years) | 53 | 42.4 | 63.6 | Normal | 15 | |
| Cohort population | 1000 | NA | NA | NA | Assumption | |
| Prevalence | Seroprevalence of dengue | 0.383 | NA | NA | NA | 5 |
| Mortality | Probability of all-cause mortality for the average age of suspected dengue cases | 0.006 | 0.005 | 0.007 | β | 15 |
| Probability of death due to dengue in the current strategy | 0.026 | NA | NA | NA | 5 | |
| Probability of death due to dengue in early screening | 0.010 | NA | NA | NA | 1 | |
| Probability of death due to DF | 0 | 0 | 0 | NA | Assumption | |
| Probability of death due to DHF in the current strategy | 0.010 | 0.008 | 0.012 | β | Estimated | |
| Probability of death due to DSS in the proposed strategy | 0.015 | 0.012 | 0.018 | β | Estimated | |
| Relative risk of mortality due to DHF in the proposed strategy | 0.380 | 0.300 | 0.460 | β | Estimated | |
| Relative risk of mortality due to DSS in the proposed strategy | 0.380 | 0.300 | 0.0460 | β | Estimated | |
| CBC | Probability of PLC <100 000/mm3 in the presence of warning signs | 0.710 | 0.568 | 0.852 | β | 13 |
| Probability of CBC test positive | 0.399 | 0.319 | 0.478 | β | Estimated | |
| ELISA | Sensitivity | 0.77 | NA | NA | NA | 4 |
| Specificity | 0.94 | NA | NA | NA | 4 | |
| True positive | 0.888 | 0.704 | 1 | β | Estimated | |
| True negative | 0.868 | 0.694 | 1 | β | Estimated | |
| Disease state probability | Lab confirmed DF in the current strategy | 0.77 | 0.616 | 0.924 | β | 5 |
| Lab confirmed DHF in the strategy | 0.18 | 0.144 | 0.216 | β | 5 | |
| Lab confirmed DHF in the proposed strategy | 0.09 | 0.072 | 0.108 | β | Assumption | |
| Lab confirmed DSS in the current strategy | 0.05 | 0.04 | 0.06 | β | 5 | |
| Lab confirmed DSS in the proposed strategy | 0.025 | 0.02 | 0.03 | β | Assumption | |
| Outpatients among patients with DF | 0.68 | 0.544 | 0.816 | β | 32 | |
| Outpatients among patients with DHF | 0.26 | 0.208 | 0.312 | β | 32 | |
| Outpatients among patients with DSS | 0 | 0 | 0 | NA | 32 | |
| Utility value | Utility for death | 0 | 0 | 0 | NA | By Definition |
| Utility for undifferentiated fever | 0.91 | 0.728 | 1 | β | Assumption | |
| Utility for DF | 0.91 | 0.728 | 1 | β | Assumption | |
| Utility for DHF | 0.66 | 0.528 | 0.792 | β | 17 | |
| Utility for DSS | 0.41 | 0.328 | 0.492 | β | Assumption | |
| Diagnostic cost | Cost of CBC per test (in INR) | 153.65 | 122.92 | 184.38 | γ | 18 |
| Cost of ELISA per test (in INR) | 314.85 | 251.88 | 377.82 | γ | 18 | |
| Treatment | Cost of ambulatory not-fatal disease per case (in INR) | 2896.78 | 2317.42 | 3476.13 | γ | 16 |
| Cost of hospitalized not-fatal disease per episode (in INR) | 21 816.20 | 17 452.96 | 26 179.44 | γ | 16 | |
| Non-medical cost per non-fatal case in the current strategy (in INR) | 1260.20 | 1008.16 | 1512.24 | γ | 16 | |
| Non-medical cost per non-fatal case in the proposed strategy | 630.10 | 504.08 | 756.12 | γ | Assumption | |
| Direct fatal cost per case | 5186.11 | 4148.88 | 6223.33 | γ | 16 | |
| Indirect fatal cost per case | 2 730 021.97 | 2 184 017.56 | 3 276 026.35 | γ | 16 | |
| Willingness-to-pay threshold | Willingness-to-pay threshold (GDP per capita, in INR) | 135 966 | – | – | NA | 19 |
NA: not applicable.
Cost data
Cost data were used from a meta-analysis report of Indian studies.16 The average cost of dengue non-fatal and fatal cases was estimated, which included health system costs, patient out-of-pocket expenditures and productivity loss. Information on health system costs such as complete blood count (CBC) and ELISA costs were obtained from the Central Government Health Scheme (CGHS) rates for 2014 published by the government of India. All the costs were adjusted for 2019. The total cost incurred by a dengue patient for a single disease episode was calculated separately in each strategy.
Effectiveness data
Health outcomes are determined in terms of the number of suspected dengue cases diagnosed with dengue infection and their related quality-of-life scores. Since the utility score for each state of dengue infection was not available for India, we used contextually relevant data from Indonesia, a comparable Asian country.17 Treatment outcomes in terms of cure and mortality were taken from an Indian meta-analysis report.5
Other data
Life expectancy was taken from India’s life table, published based on Sample Registration System (SRS) data.15 The start age of the cohort in the model was 22 y, which was based on the mean age of dengue patients during the time of diagnosis. The mean age of dengue infection and prevalence of dengue were used from the recently published meta-analysis on dengue infection in India.5
Base case analysis
Estimation of incremental costs and QALYs gained by the introduction of a new dengue screening strategy for the cohort population entering the decision-analytic model was done. Results were expressed in terms of QALYs and life years gained, deaths averted and cost per cure.
Calibration and sensitivity analysis
The robustness of model results was tested through sensitivity analysis by varying input parameters between 20% above and below the estimated values. The parameter uncertainties that could influence the ICER were evaluated by one-way sensitivity analysis (OWSA) and presented in a tornado diagram. The robustness of the model was further evaluated by probabilistic sensitivity analysis (PSA), which gives 1000 different costs and effectiveness for each strategy. The resulting ICER values were plotted in a scatter plot. The cost-effectiveness acceptability curve (CEAC) was drawn to indicate the model’s probabilistic response to different cost-effectiveness thresholds.
Budget impact analysis
The costs of the haematology analyser, reagents, training and maintenance were considered for implementation costs. The unit cost for implementing the screening strategy at the PHC facility and the estimated population coverage were used to calculate the additional budget requirement of the government of TN for implementing haematology analysers for screening suspected dengue cases at the PHC facility. Assuming increased coverage of suspected dengue cases in the PHC over years, the cost, QALY and ICER values were estimated. The projection was made for 5 y with 10–70% coverage compared with the base year.
Model outcomes
The outcomes of the model were expressed in terms of QALYs and life years gained, including the overall cost incurred per patient in intervention and comparator strategies. The model also compared the incremental cost with incremental QALYs to obtain the ICER. Further, the ICER was compared with a threshold of one-time gross domestic product (GDP) per capita in India to determine its cost-effectiveness.20 We also calculated net monetary benefit (NMB) and the additional budget required for implementing haematology analysers for screening suspected dengue cases at the PHC facilities.
Results
Model descriptive analysis
The average age of the suspected dengue cases entering the cohort was 22 y (Table 3). The proposed decentralised screening strategy detected 24 additional dengue cases when compared with the current strategy. Severe dengue cases and deaths (three vs four) were reduced in the proposed strategy as compared with the current strategy. The hospitalization for dengue was more in the proposed strategy as compared with the current strategy (12.05% vs 11.1%).
Table 3.: Results of model descriptive analysis for dengue screening at PHC facility
| Parameters, n (%) | Proposed strategy | Current strategy |
|---|---|---|
| Test positive | 130 (26) | 106 (21) |
| DF | 146 (29) | 103 (21) |
| DHF | 15 (3) | 24 (5) |
| DSS | 4 (0.82) | 7 (1.34) |
| Hospitalized care | 60 (12.05) | 56 (11.12) |
| Outpatient care | 103 (20.60) | 77 (15.38) |
| Death | 3 (0.65) | 4 (0.79) |
Base case analysis
Cost estimation
The total health system cost for the cohort estimated in the proposed and current strategies were INR1 910 131 and INR1 696 177, respectively (Table 4). It contributed 17.45% and 14.67% to the total cost estimated in the proposed and current strategies, respectively. Patient out-of-pocket expenditures and productivity loss were reduced in the proposed strategy when compared with the current strategy (INR9 030 056 vs INR9 859 103). The productivity loss due to premature death contributed more to the total cost in the proposed and current strategies (81.57% and 83.87%, respectively).
Table 4.: Summary of costs estimated for dengue screening at PHC facility
| Total cost (in INR) | ||
|---|---|---|
| Cost type | Proposed strategy | Current strategy |
| Health system cost | ||
| Ambulatory care cost (medical) for non-fatal cases | 297 807 | 221 723 |
| Hospitalization care cost (medical) for non-fatal cases | 1 319 351 | 1 230 295 |
| Investigation cost | 273 997 | 223 556 |
| Medical cost for death patients | 18 977 | 20 602 |
| Total health system costs | 1 910 131 | 1 696 177 |
| Patient costs | ||
| Non-medical cost for non-fatal cases | 102 884 | 167 525 |
| Indirect cost for death | 8 927 172 | 9 691 578 |
| Total patient costs | 9 030 056 | 9 859 103 |
The total cost incurred for the diagnosis and treatment of dengue in the current strategy was more when compared with the proposed screening strategy (Table 5). The undiscounted cost per person for the current and proposed strategies was INR23 564 and INR22 372, respectively. Discounting for 53 y of average remaining life expectancy, the estimated discounted cost per person was INR4919 and INR4670, respectively.
Table 5.: Base case results for dengue screening at PHC facility
| Parameters | Proposed strategy | Current strategy |
|---|---|---|
| Total costs (in INR) | ||
| Undiscounted | 11 186 000 | 11 782 000 |
| Discounted | 2 335 000 | 2 458 000 |
| Total life years | ||
| Undiscounted | 26 327 | 26 312 |
| Discounted | 5496 | 5493 |
| Total QALYs | ||
| Undiscounted | 23 665 | 23 455 |
| Discounted | 4940 | 4896 |
Effectiveness estimation
The total undiscounted life-years and QALYs estimated in the proposed strategy was more when compared with the current strategy (Table 5). The undiscounted QALYs per person for the current and proposed strategies was 46.91 and 47.33, respectively.
Incremental costs and effectiveness
The proposed strategy was cost-saving and the incremental cost saved over the current strategy was estimated to be INR1192 per person (Table 6). The total incremental life years gained with and without discount was 3.02 and 14.4, respectively, and the total incremental QALYs gained with and without discount was 43.83 and 210, respectively.
Table 6.: Model outcome summary table for dengue screening at PHC facility
| Outcome | Value |
|---|---|
| Incremental cost (in INR) | |
| Undiscounted | −596 000 |
| Discounted | −124 415 |
| LYs gained | |
| Undiscounted | 14.4 |
| Discounted | 3.02 |
| QALYs gained | |
| Undiscounted | 210 |
| Discounted | 43.83 |
| ICER (using LYs) | |
| Undiscounted | −41 388.88 |
| Discounted | −41 197.01 |
| ICER (using QALYs) | |
| Undiscounted | −2838.90 |
| Discounted | −2838.58 |
| Total death averted | 0.27 |
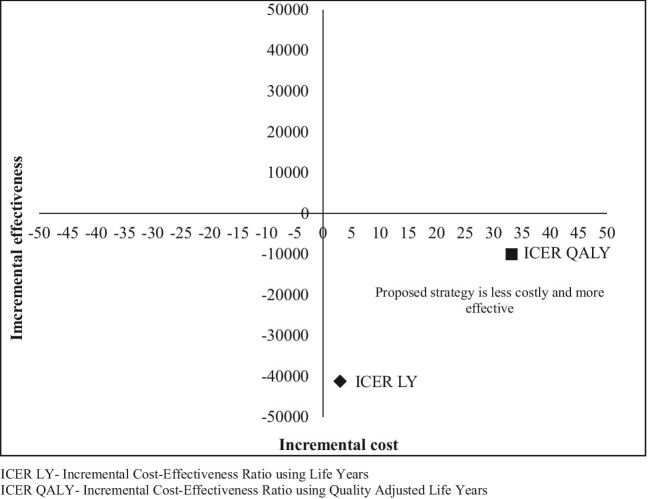
ICER
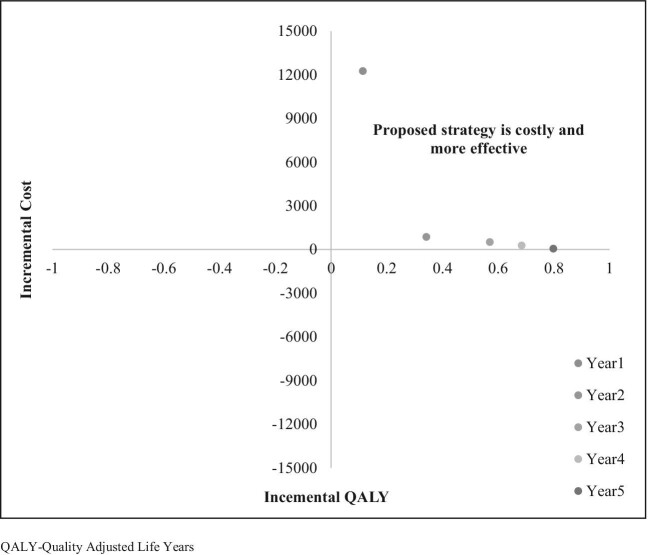
The ICER calculated using discounted life years and QALYs gained was −41 197.10 and −2383.58, respectively (Table 6). The incremental cost-effectiveness plane indicated that the proposed dengue screening strategy was more effective and less expensive compared with the current strategy (Figure 2).
Out-of-pocket expenditures
In terms of out-of-pocket expenditures, the current screening strategy incurs INR64 641 additional costs than the proposed strategy. The proposed intervention increased case detection compared with the current strategy, however, due to reduced travel distance and visits to tertiary care facilities, patients saved INR129 per person.
NMB
The NMB estimated using the willingness to pay was INR66.9 million for the proposed strategy and INR66.3 million for the current strategy. This resulted in an incremental NMB of INR0.61 for the proposed strategy, suggesting that the proposed strategy was highly acceptable for achieving a net benefit.
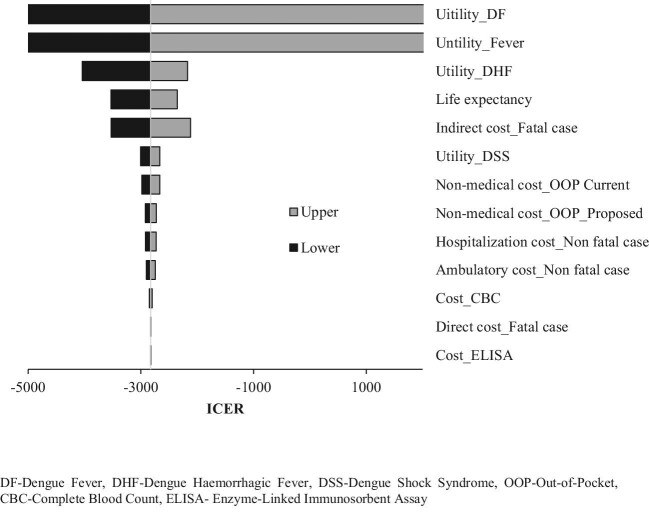
OWSA
In the OWSA, the utility parameters of the DHF and DSS dengue health states had a greater influence on the ICER value (Figure 3).
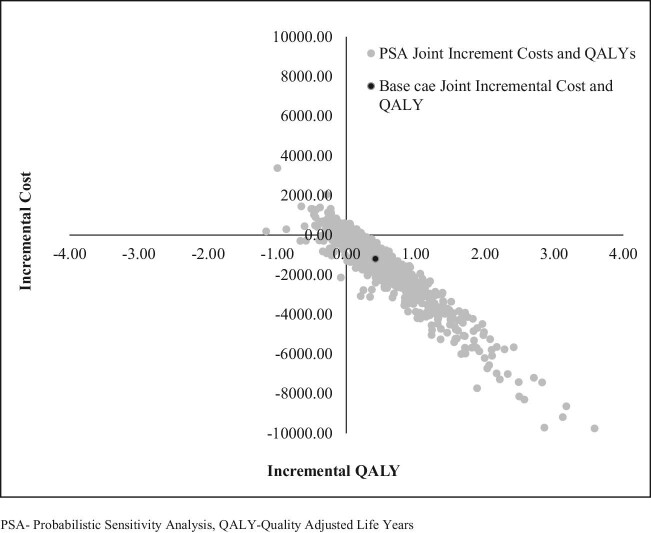
PSA
The PSA showed that the joint incremental cost and effectiveness using QALYs was less costly and more effective for approximately 84% of the iteration values (Figure 4).
CEAC
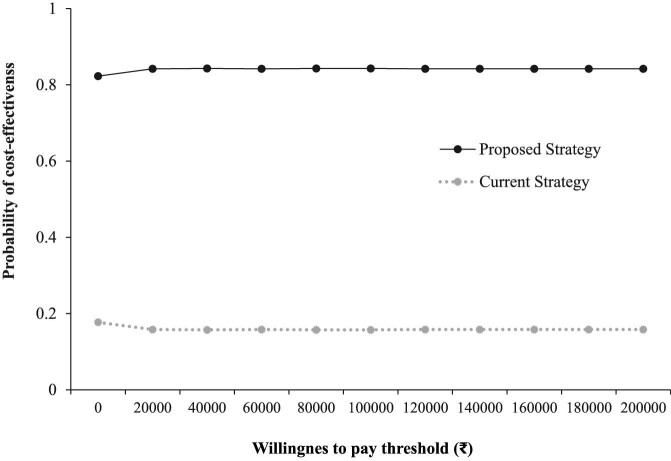
The CEAC highlights that the proposed strategy had a 0.8 probability of being an economically dominant strategy as compared with the current strategy at different cost-effectiveness threshold values (Figure 5).
Budget impact analysis
Based on 2011 census data, the projected population of TN for 2019 was 82 439 997. Considering a 14.8% prevalence of dengue acute febrile illness in TN and 0.38% seropositive prevalence, 46 365 dengue cases were estimated for the base year. An additional budget of INR57.4 million would be required for the government to implement the proposed screening strategy in the base year. With the increase in the proposed strategy’s population coverage, deaths and severe dengue cases (DHF and DSS) averted increased (Figure 6).
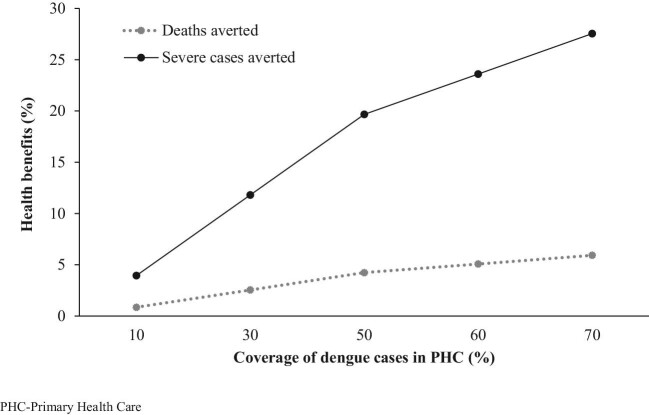
ICER vs variations in PHC access for dengue screening
Assuming a 10–70% increase in PHC access over 5 y, it was found that health benefits gained in terms of QALYs increased (Figure 7). Without implementation costs, the proposed strategy was found to be less costly and more effective even at 10% coverage in the PHC facilities. However, the cost was high in the implementation phase, which gradually decreased over years. Thus the ICER values considering implementation costs suggest that the proposed strategy was more costly and more effective.
Discussion
We assessed the economic impact of using haematology analyser equipment at the PHC facilities for dengue screening. A decision tree model was used for this evaluation that compared the intervention with the current strategy. Dengue preventive measures such as vector control and vaccination are highly challenging. Model-based studies have been undertaken in high-burden settings to assess the cost-effectiveness of various control measures, including pre-screening for vaccination.21,22 These studies highlight that extensive resources are required for the large-scale implementation of such strategies, which makes it difficult to adopt in a resource-constrained setting. In the absence of dengue vaccination in the current study setting, early diagnosis of dengue and prompt care are the only effective ways to address the mortality and morbidity due to dengue. Still, the present decentralised approach for dengue screening proposed in TN could well be integrated with future vaccination efforts in high dengue burden settings. Such an integrated approach has proven to be useful to cater to the diagnostic and vaccine prevention needs of the population at risk of vector-borne diseases.23,24
Evidence suggests that dengue patients experience significant disability during the acute and hospitalization phase of the infection.25 There is also a significant decrease in quality of life in these patients during the hospitalization and recovery periods.26 The key findings from our evaluation highlight that the implementation of dengue screening at PHC facilities could lead to an incremental gain in QALYs and life years in dengue patients. Our study projected the health outcomes of dengue patients for their lifetime, which highlights that the interventions aimed at the early stage of diagnosis and acute phase of dengue could lead to long-term health gains.
Systematic reviews conducted on the economic benefits of the rapid diagnostic test (RDT) for dengue found that the RDT for dengue was cost effective in endemic settings.27,28 It was also found that the RDT was less advantageous to symptomatic treatment and management. The review emphasised the background burden of the setting to be determinant of cost-effectiveness and highlighted the limitations of generalising cost-effectiveness evidence. The present study was conducted within a high dengue burden state in India and the results can be generalized only to a similar setting.
A study in south India on the comparative evaluation of validity and cost–benefit analysis of the RDT reported that the RDT was useful in dengue-endemic and resource-limited settings for screening.29 Our economic evaluation within the same setting identified that the implementation of a dengue screening test at PHC facilities is cost effective, with additional gains in QALYs and a reduction in mortality. This was especially strongly associated with the level of access to diagnostic services at the PHC facilities.
The cost-effectiveness finding of the proposed screening strategy in the present evaluation needs to be interpreted in the context of decentralisation of diagnostic service at the PHC facilities. The importance of strengthening the PHC facilities for effective healthcare delivery in India was highlighted earlier. India has a three-tier health system and the urban–rural distribution of THC facilities is quite unequal. This results in almost two-thirds of patients in urban hospitals being from rural areas.30 Studies conducted on decentralised screening of infectious disease have highlighted the economic benefits associated with such strategies.31–33 Our study results are in line with these findings, suggesting that the decentralized dengue screening strategy was cost-saving.
The decentralised nature of our proposed diagnostic strategy was identified as a cost-saving intervention for both the health system and patients. The out-of-pocket expenditures experienced by patients was found to be decreased due to the proposed intervention. The cost-saving strategy could be due to early diagnosis followed by early treatment, resulting in the prevention of acute and prolonged illness due to delayed diagnosis. Our sensitivity analysis highlights that the three factors—QALYs of patients with DF and DHF health states and the cost of death due to dengue—had a greater influence on the ICER value. This underscores the possible impact of dengue infections on the long-term quality of life of individuals. The decentralised diagnostic strategy could improve early diagnosis and might result in an incremental gain in quality-of-life scores.34
Delayed diagnosis of dengue could potentially lead to hospitalisation and increased bed days and thus increase the expenditures for both the health system and the patient.35 Our study identifies a reduction in the severity of dengue cases, including DHF and DSS. This again could be attributed to the decentralized nature of the proposed dengue screening strategy. Considering the implementation costs, the proposed screening strategy was still cost effective. However, we did not account for the other collateral benefits of the equipment used for dengue screening at the PHC facility (Table 7). The current implementation plan of the state government does not prioritize the use of equipment for disease diagnosis other than dengue, consideration of which could reduce the cost further.
Table 7.: Other benefits of haematology analyser at PHC facility
| Disease | Haematology analysis |
|---|---|
| Typhoid and other non-specific fevers36 | Lymphocyte count (<40%)PLC (150 001–450 000/mm3) |
| Malaria37 | Haemoglobin (9.8 g/dl) |
| PLC (50 000–100 000/mm3) | |
| Lymphocyte count (<40%) | |
| Japanese encephalitis38 | PLC (<50 000/mm3) |
| Antenatal care | Haemoglobin (monitoring normal range) |
| Neonatal sepsis39 | Haematological scoring system (score >5) |
Limitations of the study
This economic evaluation model was conducted using published and secondary data. Also, the economic costs for human resources (HR) was not considered in this study. Further evaluation of this model is planned using primary data from the field, including the economic costs for HR. The utility score for dengue health states included in the model was utilized from a different setting and may have resulted in over- or underestimation of the benefits and ICERs. However, this limitation was addressed through the sensitivity analysis technique.
Conclusions
The model results conclude that dengue screening at the PHC facility in TN is cost-saving and cost effective at 70% and 10% population coverage, respectively, when compared with the current strategy. Although high costs are incurred for the implementation of the intervention, our budget impact analysis highlights that the proposed strategy turns cost-saving from the fifth year of implementation.
Supplementary Materials
References
- 1 World Health Organisation . Dengue and severe dengue. Available from: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue [accessed 21 September 2020].
- The global burden of dengue: an analysis from the Global Burden of Disease Study 2013.. Lancet Infect Dis., 2016. [PubMed]
- The global distribution and burden of dengue.. Nature., 2013. [PubMed]
- Burden of dengue infection in India, 2017: a cross-sectional population based serosurvey.. Lancet Glob Health., 2019. [PubMed]
- Dengue infection in India: a systematic review and meta-analysis.. PLoS Negl Trop Dis., 2018. [PubMed]
- 6 Department of Health Research, Government of India . Establishment of a network of laboratories for managing epidemics and natural calamities (VRDL). Available from: http://dhr.gov.in/schemes/establishment-networklaboratories-managing-epidemics-and-natural-calamities [accessed 23 September 2020].
- 7 National Vector Borne Disease Control Programme annual report 2014–2015. Delhi: Government of India, National Vector Borne Disease Control Programme, Directorate General of Health Services, Ministry of Health and Family Welfare; 2015. Available from: https://nvbdcp.gov.in/Doc/Annual-report-NVBDCP-2014-15.pdf [accessed 23 September 2020].
- 8 National Vector Borne Disease Control Programme . Guidelines for clinical management of dengue fever, dengue haemorrhagic fever and dengue shock syndrome. Delhi: Government of India, National Vector Borne Disease Control Programme, Directorate General of Health Services, Ministry of Health and Family Welfare; 2008. Available from: http://www.nvbdcp.gov.in/Doc/Clinical%20Guidelines.pdf [accessed 23 September 2020].
- Useful clinical features and hematological parameters for the diagnosis of dengue infection in patients with acute febrile illness: a retrospective study.. BMC Hematol., 2018. [PubMed]
- Value of peripheral blood count for dengue severity prediction.. BMC Res Notes., 2018. [PubMed]
- 11 National Health Portal . Dengue fever. Available from: https://www.nhp.gov.in/disease/musculo-skeletal-bone-joints-/dengue-fever [accessed 23 September 2020].
- 12Rege S, Swaminathan S. Management of dengue. In: Association of Physicians of India, editors. Progress in medicine. Available from: http://apiindia.org/wp-content/uploads/pdf/progress_in_medicine_2017/mu_03.pdf [accessed 24 September 2020].
- Clinical and laboratory diagnosis of dengue virus infection.. J Infect Dis., 2017. [PubMed]
- Evaluation of thrombocytopenia in dengue infection along with seasonal variation in rural Melmaruvathur.. J Clin Diagn Res., 2014. [PubMed]
- Cost-effectiveness of dengue vaccination in Indonesia: considering integrated programs with Wolbachia-infected mosquitos and health education.. Int J Environ Res Public Health., 2020
- 16 Office of the Registrar General and Census Commissioner . Abridged life tables 2012–16. Available from: https://censusindia.gov.in/Vital_Statistics/SRS_Life_Table/SRS-12-16/3.Lftb%202012-16_85.pdf [accessed 24 September 2020].
- Economic burden of dengue illness in India from 2013 to 2016: a systematic analysis.. Int J Infect Dis., 2019
- Cost-of-illness and the health-related quality of life of patients in the dengue fever outbreak in Hanoi in 2017.. Int J Environ Res Public Health., 2018
- 19 Central Government Health Scheme . CGHS Chennai rate list 2014. Available from: https://cghs.gov.in/showfile.php?lid=4355 [accessed 24 September 2020].
- 20 Ministry of Statistics and Programme Implementation . GDP per capita of India. Available from: http://statisticstimes.com/economy/gdp-capita-of-india.php [accessed 25 September 2020].
- Cost effectiveness of dengue vaccination following pre-vaccination serological screening in Sri Lanka.. Int J Technol Assess Health Care., 2019. [PubMed]
- The cost-effectiveness of controlling dengue in Indonesia using wMel Wolbachia released at scale: a modelling study.. BMC Med., 2020. [PubMed]
- A novel multiplex RT-PCR assay for simultaneous detection of dengue and chikungunya viruses.. Int J Mol Sci., 2020
- Diagnostic accuracy of a rapid E1-antigen test for chikungunya virus infection in a reference setting.. Clin Microbiol Infect., 2018. [PubMed]
- Impact of a nonfatal dengue episode on disability-adjusted life years: a systematic analysis.. Am J Trop Med Hyg., 2018. [PubMed]
- Quality of life of dengue patients.. Am J Trop Med Hyg., 2008. [PubMed]
- A systematic review of the economic impact of rapid diagnostic tests for dengue.. BMC Health Serv Res., 2017. [PubMed]
- Rapid diagnostic tests for determining dengue serostatus: a systematic review and key informant interviews.. Clin Microbiol Infect., 2019. [PubMed]
- Comparative evaluation of validity and cost-benefit analysis of rapid diagnostic test (RDT) kits in diagnosis of dengue infection using composite reference criteria: a cross-sectional study from south India.. J Vector Borne Dis., 2016. [PubMed]
- Strengthening of primary health care: key to deliver inclusive health care.. Indian J Public Health., 2013. [PubMed]
- Decentralized care for multidrug-resistant tuberculosis: a systematic review and meta-analysis.. Bull World Health Org., 2017. [PubMed]
- Decentralisation of child tuberculosis services increases case finding and uptake of preventive therapy in Uganda.. Int J Tuberc Lung Dis., 2018. [PubMed]
- Decentralized, community-based treatment for drug-resistant tuberculosis: Bangladesh program experience.. Glob Health Sci Pract., 2018
- Health-related quality of life after dengue fever, Morelos, Mexico, 2016–2017.. Emerg Infect Dis., 2020. [PubMed]
- Challenges in the early diagnosis of dengue: a practical approach.. J Sci Soc., 2014
- Comparison of hematological parameters in various acute febrile illnesses.. Natl Lab Med., 2016
- An analysis of hematological parameters as a diagnostic test for malaria in patients with acute febrile illness: an institutional experience.. Oman Med J., 2014. [PubMed]
- Japanese encephalitis virus transmitted via blood transfusion, Hong Kong, China.. Emerg Infect Dis., 2018
- Significance of hematological scoring system (HSS) in early diagnosis of neonatal sepsis.. Indian J Hematol Blood Transfus., 2011. [PubMed]