
Non-Cisplatin Concurrent Systemic Therapy with Radiotherapy for Locally Advanced Head and Neck Squamous Cell Carcinoma: A Network Meta-Analysis of Randomized Clinical Trials
Abstract
Head and neck squamous cell carcinoma is one of the most common cancer types worldwide. The standard therapy for patients with locally advanced disease that has not spread to distant organs typically includes radiotherapy combined with cisplatin chemotherapy. However, a considerable number of patients are not fit for this regimen, due to poor general health or because of an increased risk for severe side effects like kidney and hearing damage. For this group, alternative treatment options are needed. Our work aims to compare different cisplatin-free regimens, including data from 28 studies with 7000 patients. Compared to cisplatin, none of the alternatives showed superior length of survival or tumor control. However, durvalumab and cetuximab induce less dysphagia, cetuximab induces less renal impairment, and panitumumab and cetuximab induce less weight loss than cisplatin. Our findings may help to guide treatment decisions for patients who cannot receive cisplatin.
Article type: Review Article
Keywords: chemoradiotherapy, immunoradiotherapy, HNSCC, cisplatin-ineligible, second-line, cetuximab, carboplatin
Affiliations: Department of Radiotherapy and Radiation Oncology, Jena University Hospital, 07747 Jena, Germany; anne-josephin.schoele@uni-jena.de (A.-J.S.); klaus.pietschmann@med.uni-jena.de (K.P.);; Comprehensive Cancer Center Central Germany, Partner Site Jena, 07747 Jena, Germany
License: © 2026 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Article links: DOI: 10.3390/cancers18101599 | PMC: PMC13204043
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (1.9 MB)
1. Introduction
With 750,000 new cases worldwide annually, HNSCC is among the most common cancer entities [ref. 1]. Men are affected about twice as often as women, and numerous risk factors, such as smoking, alcohol consumption, and HPV infection, favor their development [ref. 2]. Accordingly, a therapy that not only achieves a high overall survival rate but also preserves the patients’ quality of life during and after treatment is important. In a curatively intended setting, surgical resection and chemoradiotherapy (CRT) represent the mainstay treatment options. However, feasible therapies vary depending on the stage of the disease. For locally advanced HNSCC, the preferred treatment is surgical resection followed by adjuvant CRT [ref. 3]. If the tumor is functionally unresectable or contraindications for surgery exist, definitive CRT is the treatment of choice as a curative-intended approach. Owing to its ability to improve regional control rates and overall survival, cisplatin is the concurrent agent of choice [ref. 3]. In addition to known hypersensitivity to the drug, various contraindications exist for its use, including impaired renal function, pre-existing hearing impairment, as well as myelosuppression and peripheral neuropathy [ref. 4]. However, no universally standardized definition for cisplatin-ineligibility exists, limiting research in this specific subgroup, and therefore recommendations vary. According to current guidelines [ref. 5], carboplatin, cetuximab, and taxane-based treatments are commonly used options for concurrent therapy in this scenario. However, selecting the regimen of choice is challenging, as they differ substantially in terms of reported side-effect profiles and oncologic efficacy [ref. 3]. Carboplatin was the first platinum preparation to be developed for better tolerability and features a modified side effect profile with lower nephrotoxicity and emetogenicity compared to cisplatin [ref. 6]. Taxanes use a different mechanism of action by inducing the polymerization of microtubules and thus inhibiting cell division [ref. 7]. The EGFR antibody cetuximab is a more recent addition to combination regimens. Due to its higher affinity to the epidermal growth factor receptor, it can displace the body’s own ligands and thus negatively regulate cell growth by internalizing the receptor, resulting in inhibition of tumor growth [ref. 8]. The heterogeneity of treatment options, particularly combinations of two or more of these drugs, represents an enormous challenge in the clinical setting. This network meta-analysis (NMA) compares cisplatin-free treatment schedules in order to simplify the choice of treatment for cisplatin-ineligible patients.
2. Method
2.1. Protocol and Study Selection
This systematic review and NMA were conducted in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The review was prospectively registered on PROSPERO (CRD42024578276). The final protocol is provided in the Supplementary Materials (Supplementary Material S1).
A systematic search was initially conducted in four databases (Medline (PubMed), Web of Science Core Collection (WoS), Cochrane Library, and Scopus) from November 2023 to January 2026. For each database, a complex search strategy was developed consisting of a combination of MeSH terms, keywords, and synonyms, including different spelling variants connected to HNSCC and chemoradiotherapy or immunoradiotherapy. The complete search string is available in the Supplementary Materials (Supplementary Material S2).
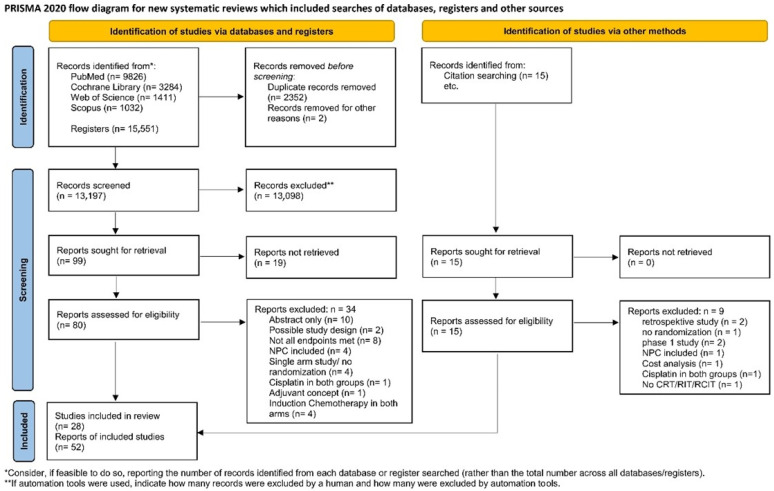
After importing the search results into EndNote 20.6 (Bld 17174), all duplicates were removed, and a title–abstract screening was carried out by two independent reviewers (KS, AS). In case of disagreement, consensus was reached by discussion or, if consensus could not be reached, by consulting a third reviewer (MR). Afterwards, all full texts were retrieved and screened again independently by both reviewers. When the title and abstract did not have sufficient information for screening purposes, a full-text copy was retrieved as well. Additionally, the bibliography of all retrieved articles was manually screened for relevant studies. Such studies were included if they provided a comprehensive description of the study. The study flow during this process is presented in Figure 1.
2.2. Criteria for Including and Excluding Studies in This Network Meta-Analysis
As cisplatin-ineligibility is a rather common difficulty when treating patients with HNSCC, many trials evaluating alternatives exist. To ensure maximum methodological homogeneity, statistical rigor, and a lower risk of bias, only randomized controlled trials were included in this NMA.
Trials including nasopharyngeal carcinoma (NPC) were excluded, because NPC differs distinctly from HNSCC regarding pathogenesis, treatment and outcome [ref. 2,ref. 10,ref. 11]. A publication cutoff excluding trials from before 2005 was chosen a priori to focus on contemporary treatment options and to reduce heterogeneity related to outdated RT techniques, imaging, staging, and supportive care.
The inclusion criteria were as follows:
- Patients with HNSCC undergoing definitive CRT/radioimmunotherapy (RIT)/radiochemoimmunotherapy (RCIT).
- At least one treatment arm of concomitant CRT/RIT/RCIT with active agents other than cisplatin.
- Randomization of patients between treatment arms.
Detailed inclusion and exclusion criteria are provided in Table 1.
Table 1: Inclusion and exclusion criteria based on PICO.
| PICO | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Patient | Patients with HNSCC undergoing definitive radiochemotherapy or radioimmunotherapy or radiochemoimmunotherapy | Patients with precancerous conditions or Carcinoma in situPreclinical studiesNasopharyngeal carcinoma |
| Intervention | Concomitant radiochemotherapy or radioimmunotherapy or radiochemoimmunotherapy with active agents other than cisplatin | radiochemotherapy with cisplatin as an active agent in all treatment armschemotherapy or immunotherapy or chemoimmunotherapy as only adjuvant/neoadjuvant/induction therapypalliative approach |
| Comparison | All possible control groups (active control, placebo, standard/guideline/usual care)Randomized study | Single-arm studyNo randomization |
| Outcome | Overall survivalProgression/disease-free survivalToxicity and adverse events | |
| Others | Language: German and EnglishFull publicationPublished 2005—today | Grey literature (conference articles, abstracts, letters, ongoing studies, unpublished literature…)Full text not available in German or EnglishPublished before 2005 |
2.3. Data Extraction
Data extraction was performed by two independent reviewers (KS, MR) using a standardized extraction template in Microsoft Word (Supplementary Material S4 [ref. 12,ref. 13,ref. 14,ref. 15,ref. 16,ref. 17,ref. 18,ref. 19,ref. 20,ref. 21,ref. 22,ref. 23,ref. 24,ref. 25,ref. 26,ref. 27,ref. 28,ref. 29,ref. 30,ref. 31,ref. 32,ref. 33,ref. 34,ref. 35,ref. 36,ref. 37,ref. 38,ref. 39,ref. 40,ref. 41]).
The template included:
- General study information: author, journal, year of publication, number of patients in general and for each treatment arm, observation period.
- Patient characteristics: age, sex, cancer sites, cancer stage.
- Intervention: type of irradiation procedure, total dose and dose per fraction, type and dose of systemic treatment.
- Main reported outcomes: OS, PFS, LC, dermatitis, mucositis, weight loss, acneiform rash, dysphagia, and renal impairment.
2.4. Assessment of Risk of Bias and Methodological Quality
All characteristics were assessed by two independent reviewers (KS, AS). Discrepancies were resolved by discussion. If consensus could not be reached, a third reviewer was consulted (MR).
The risk of bias of the included RCTs was analyzed with the Scottish Intercollegiate Guidelines Network (SIGN) Methodology Checklist 2: Controlled Trials [ref. 42]. Further, these studies were rated according to the Oxford criteria [ref. 43].
Additional criteria concerning methodology were the size of the population, application of power analysis, adequacy of statistical tests (e.g., control of premises or multiple testing), and selective outcome reporting (report of all assessed outcomes with specification of statistical data as the p-value), as well as possible conflicts of interest.
To assess publication bias, a funnel plot for every network with ≥10 studies was created, as recommended by Sterne et al. [ref. 44].
2.5. Data Synthesis
Overall survival (OS), progression-free survival (PFS), and locoregional control (LC) were the primary outcomes. These outcomes were analyzed using hazard ratios (HR). When an HR was not reported, it was estimated from its Kaplan–Meier curve using digitizeIt (version 2.5.9) and the Excel spreadsheet (version 3.0) developed by Matthew Sydes and Jayne Tierney [ref. 45,ref. 46,ref. 47]. Different treatment classes were included in the same network if they addressed the same clinical decision context: RT-based treatment of locally advanced HNSCC when cisplatin is unsuitable or serves as the comparator. Clinically distinct strategies, including altered-fractionation RT and regimens containing induction or adjuvant systemic therapy, were retained as separate nodes to avoid inappropriate pooling. Transitivity was assessed qualitatively by comparing key potential effect modifiers across trials, including age, sex, tumor site, tumor stage, performance status where available, HPV status where reported, RT technique, RT dose/fractionation, and systemic treatment regimen. Because reporting of cisplatin-ineligibility, baseline comorbidities, HPV status, performance status, and RT quality was incomplete and heterogeneous, transitivity could not be formally confirmed, and residual intransitivity was considered an important limitation.
Dermatitis, mucositis, weight loss, acneiform rash, dysphagia, and renal impairment were analyzed as secondary outcomes using odds ratios (ORs) for each. ORs were calculated from the reported percentages. As not all studies reported adverse events according to CTCAE grading, and because concomitant CRT carries a high risk of mild adverse events (grade 1–2), while toxicity-related deaths (grade 5) were inconsistently reported across studies, only grade 3–4 adverse events were extracted whenever possible. If toxicity data were not reported in sufficient detail to identify the relevant endpoint, grade, numerator, and denominator, the study was not included in the corresponding endpoint-specific adverse-event analysis. When only percentages were reported, odds ratios were calculated from these percentages and the available arm-level denominators, acknowledging the possibility of rounding errors. Missing toxicity data were not imputed.
The statistical analysis was performed using R Studio version 4.4.1 (14 June 2024) “Cranberry Hibiscus” [ref. 48].
We performed a frequentist network meta-analysis to compare the treatment options directly and indirectly. A frequentist random effects framework was chosen because it provides a transparent and reproducible approach without requiring prior assumptions, which were difficult to justify given the heterogeneity of interventions and the limited amount of direct evidence for several comparisons [ref. 49]. For the primary outcomes, the log hazard ratios and their standard errors were used. For the secondary outcomes, the log odds ratios and their standard errors were used. Additionally, to account for the slightly different populations of the studies, a random effects model was used. The tolerance of consistency had to be set to 0.5 because three three-arm studies were included.
For every outcome, a netgraph, forest plot, and treatment ranking were created. Treatment rankings were generated as exploratory descriptive summaries of the network results. If subnetworks occurred, those were analyzed individually. For the endpoint of dysphagia, the second subnetwork consisted of only one study (Rodríguez et al. [ref. 12]) and could not be compared further. The second subnetwork of weight loss consisted also of only one study (Fallai et al. [ref. 13]) and could not be compared further. For better readability, the treatment regimens of induction therapy with Docetaxel + Cisplatin + 5-FU, and concurrent Cetuximab were abbreviated as “Induction TPF + Cetuximab” and concurrent Cetuximab with adjuvant Cetuximab as “Cetuximab + adj. CTX” in plots and figures.
3. Results
The systematic search revealed 15,551 results. An additional 15 studies were added by hand search. At first, duplicates were removed, leaving 13,197 studies. After screening the title and abstract, 99 studies remained, which were retrieved to complete full-text screening. Finally, 52 publications of 28 studies were included in this NMA, but only 26 could be analyzed, because two studies (Nagpal et al. [ref. 14] and Argiris et al. [ref. 15]) missed a connection to the network.
Detailed characterization of the included studies may be seen in Table 2.
Table 2: Characteristics of included studies.
| The Basic Information of All Included Studies in the Network Meta-Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|
| Author | Year | Pat. (n) | Age (y) | Fem (%) | CT Regimen | Dose of CT | RTTechnique | RT Regimen (in Gy) |
| Al-Saleh et al. [ref. 16] | 2019 | 40 | 27–72 | 12.5 | pbCT vs. CTX | Cisplatin: 100 mg/m2; 3-weekly or 40 mg/m2 weeklyCetuximab: loading dose 400 mg/m2; 250 mg/m2 during radiation | IMRT | 69.6 Gy/1.2 Gy twice daily |
| Argiris et al. [ref. 15] | 2016 | 80 | 35–76 | 19.2 | CTX, PMX vs. CTX, PMX, Beva + maintenance | Cetuximab: loading dose 400 mg/m2; 250 mg/m2 during radiationPemetrexed: 500 mg/m2 on days 1, 22, 43Bevacizumab: 15 mg/kg on days 1, 22, 43 + 6 months maintenance | RT | 70–74 Gy/2 Gy |
| Bonner et al. [ref. 17] | 2006 | 424 | 34–83 | 19.8 | CTX vs. RT | Cetuximab: loading dose 400 mg/m2; 250 mg/m2 during radiation | RT | Once daily: 70 Gy/2 GyTwice daily: 72.0–76.8 Gy/1.2 Gy |
| Bourhis et al. [ref. 18] | 2012 | 840 | 34–75 | 13 | CBDP, 5-FU vs. HART vs. Acc HART | RT:Carboplatin: 70 mg/m2 on days 1–4, 22–25, 43–465-FU: 600 mg/m2 on days 1–4, 22–25, 43–46HART:Carboplatin: 70 mg/m2 on days 1–5, 29–335-FU: 600 mg/m2 on days 1–5, 29–33 | RT | RT: 70 Gy/2 GyHART: 70 Gy/2 Gy/fraction until 40 Gy, then 1.5 Gy/fraction twice dailyRT 5 days per weekacc HART: 64.8 Gy/1.8 Gy twice daily |
| Budach et al. [ref. 19,ref. 20] | 2005 | 384 | 33–71 | 16.1 | MitC, 5-FU vs. HART | 5-FU: 600 mg/m2 days 1 to 5Mitomycin-C: 10 mg/m2 on days 5 and 36 | RT | RT: 30 Gy/2 Gy followed by 1.4 Gy twice daily to 70.6 GyHART: 16 Gy/2 Gy followed by 1.4 Gy twice daily to 77.6 Gy |
| Chitapanarux et al. [ref. 21] | 2013 | 85 | 20–77 | 24.7 | RT vs. CBDP, 5-FU | Carboplatin: 70 mg/m2 on days 1, 22, 435-FU: 600 mg/m2 on days 1, 22, 43 | RT | RT: 70 Gy2 Gy/fraction until 40 Gy, then 1.8 Gy first RT/day and 1.2 Gy second RT/dayRT 5 days per weekCRT: 66 Gy/2 Gy5 fractions per week |
| Essa et al. [ref. 22] | 2010 | 41 | Mean: 55.1/55.7 | 19.5 | Pacli vs. CDDP | Paclitaxel: 30 mg/m2 weeklyCisplatin: 30 mg/m2 weekly | RT | 66–70 Gy/2 Gy |
| Ezzat et al. [ref. 23] | 2005 | 60 | Mean: 53/54/49 | 75 | RT vs. HART vs. MitC, HART | Mitomycin C: 15 mg/m2 at the end of 1st week | RT | 68 Gy/2 GyRT: 5 fractions per weekHART: 6 fractions per week |
| Fallai et al. [ref. 13,ref. 24] | 2006 | 192 | Median: 56.1 | 11.5 | RT vs. HART vs. CBDP,5-FU | Carboplatin: 75 mg/m2, days 1–45-FU: 1000 mg/m2, days 1–4 | RT | RT: 66–70 Gy/2 GyHART: 64–67.2 Gy 2 fractions daily with 1.6 Gy |
| Gebre-Medhin et al. [ref. 25] | 2021 | 298 | 33–77 | 20 | CDDP vs. CTX | Cisplatin: 40 mg/m2Cetuximab: loading dose of 400 mg/m2, seven weekly doses of 250 mg/m2 | RT | 68 Gy/2 Gy |
| Geoffrois et al. [ref. 26] | 2018 | 370 | Median: 56/56.5 | 15/13 | Induction TPF, CTX vs. CBDP, 5-FU | TPF: docetaxel 75 mg/m2 day 1 + cisplatin 75 mg/m2 day 1 + FU 750 mg/m2 days 1 to 5Cetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiationCarboplatin: 70 mg/m2 daily5-FU: 600 mg/m2 days 1 to 4 | RT | 70 Gy/2 Gy |
| Gillison et al. [ref. 27] | 2019 | 849 | 33–83 | 10 | CDDP vs. CTX | Cisplatin: 100 mg/m2 days 1 and 22Cetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiation | IMRT | 70 Gy/2 Gy |
| Giralt et al. [ref. 28] | 2015 | 151 | NG | 19 | Pani vs. CDDP | Cisplatin: 100 mg/m2 days 1 and 22Panitumumab: 9.0 mg/kg days 1, 22, 43 | IMRT/3D conformal RT | 70–72 Gy/2–2.4 Gy |
| Halim et al. [ref. 29] | 2012 | 216 | 20–70 | 39/43 | Gem vs. Pacli | Gemcitabine: 100 mg/m2 weeklyPaclitaxel: 20 mg/m2 weekly | RT | 65 Gy/2 Gy |
| Magrini et al. [ref. 30] | 2016 | 70 | 36–80 | 28.6 | CDDP vs. CTX | Cisplatin: 40 mg/m2Cetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiation | 3D conformal RT, IMRT, IMRT with simultaneous boost, helical IMRT | 70 Gy/2 Gy |
| Mehanna et al. [ref. 31] | 2019 | 334 | 52–63 | 20 | CDDP vs. CTX | Cisplatin: 100 mg/m2, days 1, 22, 43Cetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiation | RT | 70 Gy/2 Gy |
| Mell et al. [ref. 32] | 2024 | 190 | 48–90 | 16 | Durvalumab vs. CTX | Durvalumab: 1500 mg2 weeks before RT, every 4 weeks starting week 2Cetuximab 400 mg/m2 1 week before RT, 250 mg/m2 weekly | RT | 70 Gy/2 Gy |
| Mercke et al. [ref. 33] | 2023 | 152 | Median: 59.8 | 24.6 | Induction TPF, CTX vs. CTX | Induction CT2 cycles Docetaxel: 75 mg/m22 cycles Cisplatin: 75 mg/m22 cycles 5-FU: 1000 mg/m2cycles 21 days apartduring RTCetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiation | RT | 68 Gy/2 Gy |
| Mesia et al. [ref. 34] | 2012 | 91 | 42–80 | 14.3 | CTX vs. CTX, adj. CTX | Cetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiationadj. CTX: 250 mg/m2 weekly over 12 weeks | RT | Concurrent: 70 Gy/2 Gyadjuvant: 69.9 Gy/1.8 Gy |
| Nagpal et al. [ref. 14] | 2021 | 49 | 42–76 | 10.2 | CBDP, Gef vs. CBDP, Erl | Carboplatin: AUC 2Gefitinib: 250 mg ODErlotinib: 250 mg OD | RT | 66 Gy/2 Gy |
| Rischin et al. [ref. 35] | 2021 | 189 | Median: 57.4 | 10 | CDDP vs. CTX | Cisplatin: 40 mg/m2 weeklyCetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiation | IMRT | 70 Gy/2 Gy |
| Rodríguez et al. [ref. 12] | 2010 | 105 | Median: 59/65 | 22.6 | Nimo vs. Placebo | Nimotuzumab: 200 mg administered 6× during treatmentPlacebo: 6× during treatment | RT | 60–66 Gy/2 Gy |
| Ruo Redda et al. [ref. 36] | 2010 | 157 | Median: 60 | 10 | RT vs. CBDP | Carboplatin 45 mg/m2 on days 1–5, at weeks 1, 3, 5, 7 | RT | 70 Gy/2 Gy |
| Semrau et al. [ref. 37] | 2006 | 263 | 28–73 | 15 | RT vs. CBDP, 5-FU | Carboplatin: 70 mg/m25-FU: 600 mg/m2 days 1–5 and 29–33 | RT | 69.9 Gy/1.8 Gy |
| Siu et al. [ref. 38] | 2017 | 315 | Median: 56 | 16 | CDDP vs. Pani | Cisplatin: 100 mg/m2 on days 1, 22, 43Panatimumab: 9 mg/kg every 3 weeks, starting one week before RT (days 7, 15, 36) | RT | 70 Gy/2 Gy |
| Tao et al. [ref. 39] | 2018 | 406 | 36–70 | 16 | CTX vs. CTX, CBDP | Cetuximab: loading dose of 400 mg/m2, 250 mg/m2 during radiationCarboplatin: 70 mg/m2; 3 cycles on days 1–45-FU: 600 mg/m2; 3 cycles on days 1–4 | IMRT | 70 Gy/2 Gy |
| Tao et al. [ref. 40] | 2023 | 131 | 47–81 | 14.5 | Pembro vs. CTX | Pembrolizumab: 200 mg on days 1, 22, 43 during RTCetuximab: loading dose of 400 mg/m2 on day 8, 250 mg/m2 weekly during radiation | IMRT | 69.96 Gy/2.12 Gy |
| Thompson et al. [ref. 41] | 2023 | 338 | 45–84 | 22.5 | Placebo vs. Nimorazole | Nimorazole: 1.2 g/m2Placebo: 1.2 g/m2 | IMRT | 65 Gy/2.17 Gy |
Acc HART, accelerated HART; adj CTX, adjuvant cetuximab; Beva, bevacizumab; CBDP, carboplatin; CDDP, cisplatin; CTX, cetuximab; Erl, erlotinib; Fem, female; Gef, gefitinib; Gem, gemcitabine; Induction TPF, induction docetaxel, 5-fluorouracil, cisplatin; MitC, mitomycin-C; Nimo, nimotuzumab; Pacli, paclitaxel; Pani, panitumumab; Pat., Patients; pbCT, platinum-based chemotherapy; Pembro, pembrolizumab; PMX, pemetrexed; n, number; y, years; CT, chemotherapy; RT, radiotherapy; Gy, grays; IMRT, intensity-modulated radiation therapy.
3.1. Characteristics of Included Studies
Concerning all relevant studies, 6870 patients were included, and 6687 of them were analyzed, due to 183 dropouts. The age of patients ranged from 20 to 90 years. A total of 1.147 (17.2%) participants were female, and 5.540 (82.8%) were male.
3.2. Excluded Studies
A list of the studies excluded after full-text screening and the reasons for exclusion are presented in the Supplementary Materials (Supplementary Material S5 [ref. 50,ref. 51,ref. 52,ref. 53,ref. 54,ref. 55,ref. 56,ref. 57,ref. 58,ref. 59,ref. 60,ref. 61,ref. 62,ref. 63,ref. 64,ref. 65,ref. 66,ref. 67,ref. 68,ref. 69,ref. 70,ref. 71,ref. 72,ref. 73,ref. 74,ref. 75,ref. 76,ref. 77,ref. 78,ref. 79,ref. 80,ref. 81,ref. 82,ref. 83,ref. 84,ref. 85,ref. 86,ref. 87,ref. 88,ref. 89,ref. 90,ref. 91,ref. 92,ref. 93,ref. 94,ref. 95,ref. 96,ref. 97,ref. 98,ref. 99,ref. 100]).
3.3. Risk of Bias of Included Studies
The methodical quality was rated according to the SIGN Methodology Checklist 2: Controlled Trials [ref. 42]. These studies were further rated based on the Oxford criteria [ref. 43]. These results and additional comments on methodology are provided in Supplementary Material S6. Overall, all studies were of sufficient quality and therefore included in further analysis.
3.4. Efficacy of Cisplatin-Free Chemoradiotherapy
3.4.1. Overall Survival
The analysis of OS included 25 studies with 6535 patients. The corresponding netgraph is shown in Figure 2A. Compared to the standard regimen of cisplatin plus RT, no alternative treatment demonstrated a significant OS advantage. For details, see Figure 2B. A numerical improvement of OS was seen with paclitaxel (HR = 0.74; 95%-CI: 0.35–1.57) and gemcitabine (HR = 0.84; 95%-CI: 0.37–1.94). Concomitant cetuximab plus adjuvant cetuximab (HR = 1.01; 95%-CI: 0.54–1.88) and platinum-based therapy (HR = 1.04; 95%-CI: 0.29–3.69) showed comparable results to the standard regimen, while panitumumab (HR = 1.31; 95%-CI: 0.88–1.97), cetuximab, carboplatin (HR = 1.38; 95%-CI: 0.88–2.16) and induction TPF + cetuximab (HR = 1.55; 95%-CI: 0.84–2.86) showed numerically worse OS.
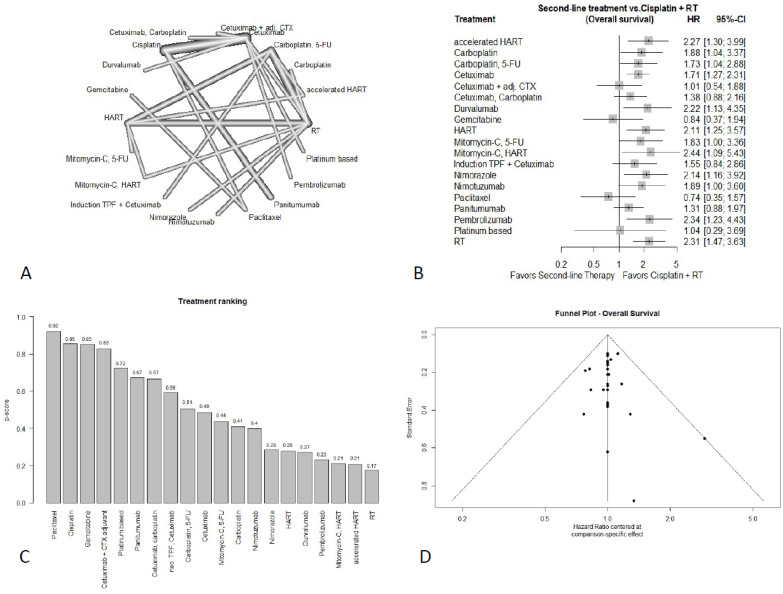
Carboplatin + 5-FU (HR = 1.73; 95%-CI: 1.04–2.88), cetuximab (HR = 1.71; 95%-CI: 1.27–2.31), mitomycin-C + 5-FU (HR = 1.83; 95%-CI: 1.00–3.36), carboplatin (HR = 1.88; 95%-CI: 1.04–3.37), nimotuzumab (HR = 1.89; 95%-CI: 1.00–3.60), nimorazole (HR = 2.14; 95%-CI: 1.16–3.92), HART (HR = 2.11; 95%-CI: 1.25–3.57), durvalumab (HR = 2.22; 95%-CI: 1.13–4.35), pembrolizumab (HR = 2.34; 95%-CI: 1.23–4.43), mitomycin C + HART (HR = 2.44; 95%-CI: 1.09–5.43), and accelerated HART (HR = 2.27; 95%-CI: 1.30–3.99) each showed significantly worse OS with conventional RT without concomitant systemic treatment (cRT) (HR = 2.31; 95%-CI: 1.47–3.63) being the least favorable option. The full treatment ranking can be seen in Figure 2C.
3.4.2. Progression-Free Survival
Thirteen studies with 4233 patients reported on PFS. The corresponding netgraph is shown in Figure 3A.
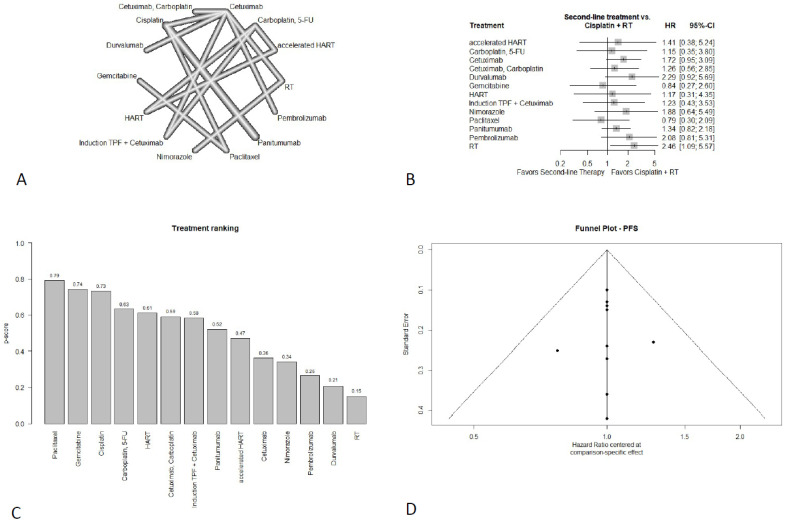
In terms of PFS, all alternative regimens failed to show a significantly superior result compared to the standard regimen of cisplatin plus RT (Figure 3B). Paclitaxel (HR = 0.79; 95%-CI: 0.30–2.09) and gemcitabine (HR = 0.84; 95%-CI: 0.27–2.60) showed a non-significant PFS improvement. Although the wide confidence interval (CI) of gemcitabine indicates substantial uncertainty regarding the true effect. Carboplatin + 5-FU (HR = 1.15; 95%-CI: 0.35–3.80), HART (HR = 1.17; 95%-CI: 0.31–4.35), cetuximab + carboplatin (HR = 1.26; 95%-CI: 0.56–2.85), induction therapy (docetaxel + cisplatin + 5-FU) plus cetuximab (HR = 1.23; 95%-CI: 0.43–3.53), panitumumab (HR = 1.34; 95%-CI: 0.82–2.18), accelerated HART (HR = 1.41; 95%-CI: 0.38–5.24), cetuximab (HR = 1.72; 95%-CI: 0.95–3.09), nimorazole (HR = 1.88; 95%-CI: 0.64–5.48), pembrolizumab (HR = 2.08; 95%-CI: 0.81–5.31), and durvalumab (HR = 2.29; 95%-CI: 0.92–5.69) each were associated with numerically worse PFS without statistical significance. cRT provided significantly worse PFS (HR = 2.46; 95%-CI: 1.09–5.57), thus being the least favorable option. The full treatment ranking can be seen in Figure 3C.
3.4.3. Locoregional Control
For the endpoint of LC, two separate subnetworks were analyzed due to a missing connection. The first subnetwork consisted of four studies with 721 patients, and the second included four studies with 610 patients.
Subnetwork 1
The netgraph of subnetwork 1 is shown in Figure 4(A1).
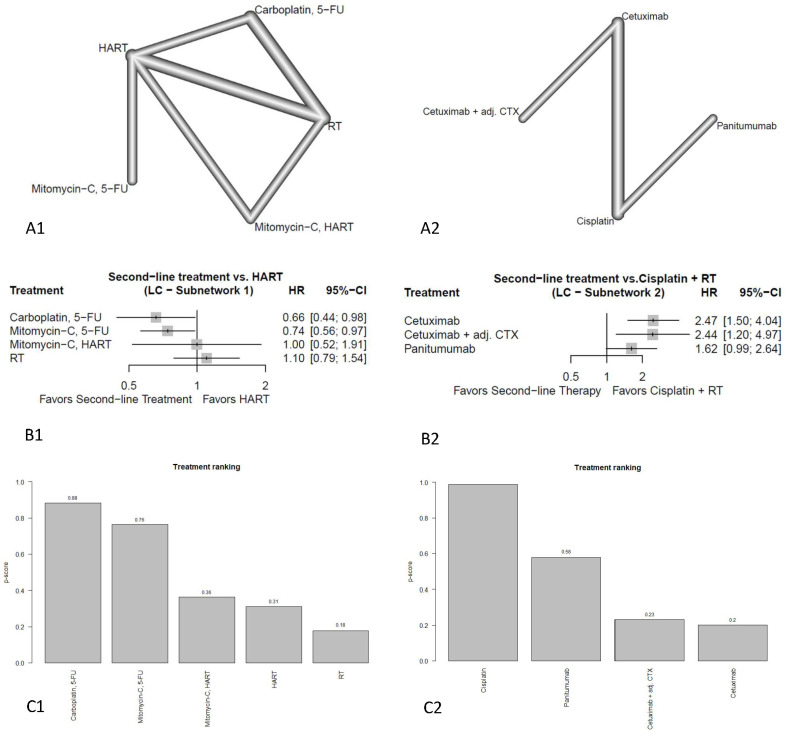
Compared to HART treatment with carboplatin + 5-FU (HR = 0.66; 95%-CI: 0.44–0.98) and mitomycin C + 5-FU (HR = 0.74; 95%-CI: 0.56–0.97) showed a significant improvement of LC (Figure 4(B1)). Mitomycin C plus HART showed comparable results (HR = 1.00; 95%-CI: 0.52–1.91) to HART alone, although the wide CI indicates substantial uncertainty regarding the true effect. cRT (HR = 1.10; 95%-CI: 0.79–1.54) showed numerically worse LC than HART. The full treatment ranking can be seen in Figure 4(C1).
Subnetwork 2
The netgraph of subnetwork 2 is shown in Figure 4(A2).
In terms of LC, all regimens failed to show improvement compared to the standard regimen of cisplatin plus RT (Figure 4(B2)). While panitumumab was numerically worse (HR = 1.62; 95%-CI: 0.99–2.64), both alternative regimens, concomitant cetuximab plus adjuvant cetuximab (HR = 2.44; 95%-CI: 1.20–4.97) and concomitant cetuximab only (HR = 2.47; 95%-CI: 1.50–4.04) showed significantly worse results. The full treatment ranking can be seen in Figure 4(C2).
3.5. Adverse Events
3.5.1. Dysphagia
Six studies reported on dysphagia, but because of a missing connection to the network, the study of Rodríguez et al. [ref. 12] could not be compared further, so only five studies, including 805 patients, remained for analysis. The netgraph is shown in Supplementary Material S7A. Durvalumab (OR = 0.37; 95%-CI: 0.15–0.89) and cetuximab showed significantly less dysphagia (OR = 0.55; 95%-CI: 0.33–0.93) compared to the standard regimen of cisplatin plus RT, while both panitumumab (OR = 1.32; 95%-CI: 0.77–2.25) and paclitaxel (OR = 1.60; 95%-CI: 0.38–6.81) showed numerically worse results (Supplementary Material S7B). The full treatment ranking can be seen in Supplementary Material S7C.
3.5.2. Acneiform Rash
Seven studies, including 2358 patients, reported on acneiform rash. The netgraph is shown in Supplementary Material S8A. Compared to the standard regimen of Cisplatin plus RT, all studies failed to show significantly superior results (Supplementary Material S8B). Pembrolizumab (OR = 2.18; 95%-CI: 0.09–52.90) and cRT (OR = 2.41; 95%-CI: 0.32–18.01) showed numerically worse results; however, their wide CI indicated substantial uncertainty regarding their true effect.
Cetuximab (OR = 52.29; 95%-CI: 12.81–213.50) and induction therapy (docetaxel + cisplatin + 5-FU) plus cetuximab (OR = 59.26; 95%-CI: 11.86–296.22) showed significantly worse results. Panitumumab (OR = 864.77; 95%-CI: 191.84–3898.23) was the least favorable treatment regimen and was associated with a highly significant increase in the risk of acneiform rash. The full treatment ranking can be seen in Supplementary Material S8C.
3.5.3. Renal Impairment
Seven studies, including 1978 patients, reported on renal impairment occurring during treatment. The netgraph for the endpoint of renal impairment is shown in Supplementary Material S9A. Compared to the standard regimen of cisplatin plus RT, only treatment with cetuximab showed significantly less renal impairment (OR = 0.07; 95%-CI: 0.02–0.25), while panitumumab (OR = 0.32; 95%-CI: 0.06–1.60) and durvalumab (OR = 0.14; 95%-CI: 0.00–4.11) only showed a numerical reduction, with durvalumab also showing a notably wide confidence interval. Platinum-based combination therapy (OR = 0.91; 95%-CI: 0.04–23.20) demonstrated no statistically significant difference, with a notably wide confidence interval. Cetuximab + carboplatin (OR = 1.71; 95%-CI: 0.08–38.65) showed numerically worse results, see Supplementary Material S9B. The full treatment ranking can be seen in Supplementary Material S9C.
3.5.4. Dermatitis
For dermatitis, two separate subnetworks were analyzed due to a missing connection. The first subnetwork consisted of 12 studies with 1948 patients, and the second included 5 studies with 1015 patients.
Subnetwork 1
The netgraph of subnetwork 1 is shown in Supplementary Material S9(A1). Compared to the standard regimen of Cisplatin plus RT, all alternative regimens failed to show a significant reduction in dermatitis incidence. Both panitumumab (OR = 0.43; 95%-CI: 0.11–1.67) and pembrolizumab (OR = 0.81; 95%-CI: 0.17–3.73) showed a numerically reduced incidence of dermatitis, while durvalumab (OR = 1.63; 95%-CI: 0.29–9.12), paclitaxel (OR = 2.12; 95%-CI: 0.26–17.51), concomitant cetuximab with adjuvant cetuximab (OR = 2.21; 95%-CI: 0.06–86.43), platinum-based therapy (OR = 5.65; 95%-CI: 0.09–370.52) and gemcitabine (OR = 3.92; 95%-CI: 0.34–44.99) showed a numerically higher incidence of dermatitis. Cetuximab (OR = 4.63; 95%-CI: 2.14–10.02) and cetuximab + carboplatin (OR = 6.30; 95%-CI: 1.15–34.54) showed a significantly higher incidence of treatment-related dermatitis Supplementary Material S10(B1). The full treatment ranking can be seen in Supplementary Material S10(C1).
Subnetwork 2
The netgraph of subnetwork 2 is shown in Supplementary Material S10(A2). Compared to HART, all studies failed to show a significant reduction in dermatitis incidence Supplementary Material S10(B2). Nimotuzumab (OR = 2.32; 95%-CI: 0.25–21.44), cRT (OR = 2.48; 95%-CI: 0.44–14.07), and carboplatin, 5-FU (OR = 4.44; 95%-CI: 0.84–23.47) showed numerically worse results, while induction therapy with TPF plus concurrent cetuximab (OR = 12.48; 95%-CI: 1.96–79.68) showed a significantly higher incidence of dermatitis. The full treatment ranking can be seen in Supplementary Material S10(C2).
3.5.5. Weight Loss
Six studies reported on weight loss, but because of a missing connection to the network, the study of Fallai et al. [ref. 13] could not be compared further, so that five studies, including 1274 patients, remained for analysis. The netgraph is shown in Supplementary Material S11A. While panitumumab (OR = 0.15; 95%-CI: 0.03–0.66) and cetuximab (OR = 0.66; 95%-CI: 0.47–0.92) showed significantly less incidence of weight loss compared to the standard regimen of cisplatin plus radiotherapy, durvalumab (OR = 0.68; 95%-CI: 0.26–1.78) and platinum-based combination therapy showed an only numerically lower incidence of weight loss (OR = 0.8; 95%-CI: 0.01–43.17) Supplementary Material S11B. Platinum-based combination therapy also showed a notably wide confidence interval. The full treatment ranking can be seen in Supplementary Material S11C.
3.5.6. Mucositis
Eighteen studies, including 3.836 patients, reported on the incidence of mucositis. The corresponding netgraph can be seen in Supplementary Material S12A. All alternative regimens failed to show a significant decrease in mucositis incidence compared to cisplatin plus RT Supplementary Material S12B. Pembrolizumab (OR = 0.57; 95%-CI: 0.07–4.55) showed a numerical decrease, while durvalumab (OR = 0.96; 95%-CI: 0.11–8.12), as well as panitumumab (OR = 1.00; 95%-CI: 0.36–2.81), provided comparable results to Cisplatin plus RT. RT (OR = 1.61; 95%-CI: 0.11–23.67), cetuximab (OR = 1.72; 95%-CI: 0.41–7.12), nimotuzumab (OR = 1.92; 95%-CI: 0.08–45.17), Induction TPF plus cetuximab (OR = 2.01; 95%-CI: 0.26–15.73), carboplatin + 5-FU (OR = 2.19; 95%-CI: 0.18–26.33), platinum-based therapy (OR = 2.10; 95%-CI: 0.03–174.93), carboplatin (OR = 2.30; 95%-CI: 0.10–54.80), paclitaxel (OR = 2.73; 95%-CI: 0.42–17.92), HART (OR = 3.22; 95%-CI: 0.22–46.12), gemcitabine (OR = 4.74; 95%-CI: 0.44–51.41), cetuximab plus adjuvant CTX (OR = 5.27; 95%-CI: 0.26–107.77), cetuximab + carboplatin (OR = 5.31; 95%-CI: 0.42–66.74), accelerated HART (OR = 5.21; 95%-CI: 0.31–86.43) and mitomycin C + HART (OR = 12.12; 95%-CI: 0.45–322.98) all showed a numerical increase in mucositis incidence. The full treatment ranking can be seen in Supplementary Material S12C.
Only the PFS and OS network, the first dermatitis subnetwork, and the mucositis network included at least 10 studies. Therefore, funnel plots were generated only for these networks. The funnel plot was evenly distributed for PFS and the first subnetwork of dermatitis. The funnel plot for mucositis also showed a symmetrical distribution, but also two scattered points outside the 95%-CI funnel. Those scattered points may be due to a small-study effect. The funnel diagram for OS showed a biased distribution with a scattered point in the middle of the funnel, indicating a possible publication bias, which may have also impacted the results. All funnel plots can be seen in Figure 2D and Figure 3D and Supplementary Material S13.
4. Discussion
Surgical resection followed by adjuvant CRT is the standard of care treatment for locally advanced HNSCC with a curative-intended approach. If functional unresectability or contraindications for surgery exist, definitive CRT is the treatment of choice. High-dose cisplatin and concurrent RT is the standard of care treatment in such cases [ref. 3]. However, toxicity and comorbidities restrict the applicability of cisplatin [ref. 4], the optimal treatment strategy for patients with locally advanced, non-metastatic HNSCC who are ineligible for cisplatin remains uncertain.
For the endpoint of OS, no regimen was superior to standard of care treatment with cisplatin. In case of cisplatin-ineligibility, both paclitaxel and gemcitabine showed numerically favorable but statistically non-significant OS estimates compared to cisplatin and therefore may represent potentially suitable non-cisplatin options in selected patients. The precision of these estimates is limited by wide confidence intervals, largely attributable to small sample sizes and a high proportion of indirect comparisons. Additionally, potential publication bias has to be considered, as evident in the funnel plot, so that these findings should be interpreted with caution.
None of the included agents showed a significant improvement in PFS compared to cisplatin, but paclitaxel and gemcitabine ranked ahead of cisplatin for PFS. However, for both substances, the wide CI leaves space for substantial uncertainty regarding their true effect, which should be considered when applying these results. It must also be mentioned that the network had a high proportion of indirect comparisons and studies with small sample sizes, leading to wide confidence intervals and limited precision and certainty of these findings. Therefore, these findings should not be interpreted as evidence of superiority. Rather, they may inform consideration of these regimens as potential non-cisplatin options in selected patients.
For the endpoint of LC carboplatin + 5-FU and mitomycin + 5-FU both showed significant improvement compared to HART in the first subnetwork, while no alternative treatment could improve LC in the second subnetwork compared to cisplatin. However, both subnetworks only included data from four studies, so the evidence base is limited.
In this NMA, none of the alternative concomitant systemic regimens significantly improved OS, PFS, or LC compared with cisplatin for patients with locally advanced HNSCC. Consequently, alternative chemoradiotherapy (CRT) regimens should be reserved for patients with clear contraindications to cisplatin. In this context, paclitaxel and gemcitabine may represent potentially suitable non-cisplatin options in selected patients, as both agents showed numerically favorable or comparable outcomes regarding OS and PFS without statistically significant differences relative to cisplatin. However, these findings remain limited by wide confidence intervals, small sample sizes, and a high proportion of indirect comparisons. Unfortunately, no comparative studies with paclitaxel versus gemcitabine CRT regimen exist, so a comparison between the two drugs is only indirectly possible.
Our findings are partially in line with current NCCN guidelines, where CRT with cisplatin is recommended as the standard of care, preferably delivered as high-dose treatment, alongside carboplatin + 5-FU [ref. 101]. However, neither paclitaxel nor gemcitabine is currently recommended as a systemic agent during CRT. A recently conducted NMA by Petrelli et al. [ref. 102] recommended cisplatin CRT as the standard of care, with concomitant carboplatin or docetaxel as alternatives for cisplatin-unfit patients. However, it should be mentioned that the differences between their results and ours might be due to the different statistical approaches used, as Petrelli et al. used a Bayesian framework with a fixed effects model, while our NMA was performed using a frequentist framework with a random effects model, thus leading to slightly different results due to the prior assumptions of the methods used [ref. 49,ref. 103]. Furthermore, Petrelli et al. employed different inclusion criteria, as adjuvant and neoadjuvant regimens, studies with only HPV-positive patients, experimental agents, and studies with anti-EGFR treatment were excluded. Additionally, our NMA ruled out studies that were published before 2005, which were included by Petrelli et al.
Given the prevalence of cisplatin ineligibility due to baseline comorbidities, the selection of alternative regimens requires a rigorous evaluation of their comparative adverse event (AE) profiles to ensure treatment tolerability. Compared to cisplatin, both cetuximab and durvalumab emerged as less-toxic alternatives with a significantly lower incidence of dysphagia. Cetuximab further demonstrated a significant reduction in treatment-related renal impairment and weight loss; panitumumab showed similar benefits regarding weight loss, though its impact on renal function was only numerically superior. In contrast, no regimen significantly reduced the incidence of acneiform rash or mucositis. The high incidence of acneiform rash is consistent with the pharmacological profiles of immune checkpoint inhibitors [ref. 104,ref. 105]. For dermatitis and mucositis, several agents (pembrolizumab, durvalumab, and panitumumab) showed numerical improvements, but results were statistically non-significant. The interpretation of these findings is constrained by small sample sizes (typically five studies per endpoint) and a high proportion of indirect comparisons, resulting in notably wide confidence intervals (CIs). Specifically, the mucositis analysis exhibited potential small-study effects or statistical outliers, as indicated by funnel plot asymmetry. Consequently, these results should be interpreted with caution. Overall, cetuximab and panitumumab demonstrated superior toxicity profiles compared to cisplatin, with cetuximab identified as the preferred alternative due to significant reductions in overall toxicity. These findings align with ESTRO guidelines [ref. 3], which maintain cisplatin-based CRT as the gold standard for locally advanced HNSCC while recommending cetuximab for cisplatin-ineligible patients. Although panitumumab showed comparable benefits in this network meta-analysis, it is not yet explicitly endorsed by ESTRO. However, panitumumab was not explicitly recommended by ESTRO guidelines, although both studies by Giralt et al. [ref. 28] and Siu et al. [ref. 38] were published at the time. Our results corroborate the results of previous meta-analyses [ref. 106] confirming cetuximab as a less-toxic alternative for the cisplatin-unfit population.
Some limitations of this NMA must be mentioned. For once, only studies published in English or German were included in this review. In consequence, most of the included studies were performed in North America and Europe, leading to an overrepresentation of these populations in our data. Therefore, our findings might not be generalizable to all populations [ref. 1,ref. 2]. In the absence of a standardized definition of cisplatin ineligibility, eligibility criteria vary substantially across studies, and well-conducted studies directly addressing this research question are scarce. Consequently, our study selection criteria had to navigate the tension between heterogeneity and a limited data basis, which presents an inherent limitation of data accuracy. Because several trials enrolled broader LA-HNSCC populations rather than exclusively cisplatin-ineligible patients, our findings should be interpreted as evidence on cisplatin-free RT-based regimens relevant to the cisplatin-ineligible setting, rather than as evidence generated solely in cisplatin-unfit populations. Resulting differences in frailty, comorbidities, and performance status between study populations may have introduced indirectness and residual intransitivity, potentially affecting both efficacy and toxicity comparisons. Additionally, since HPV status and HPV-stratified outcomes were inconsistently reported, imbalances in HPV prevalence across trials could not be adjusted for and may have affected indirect comparisons, particularly for survival endpoints. Also, only studies published in 2005 or later were included. This was done to minimize the heterogeneity of irradiation techniques and account for technical developments, such as the use of IMRT or 3D conformal RT, as well as improvements in supportive care, HPV testing and stratification, imaging, target delineation, and staging systems, which all have the potential to significantly affect oncologic outcomes and adverse events [ref. 107]. However, as demonstrated by a study from Peters et al. [ref. 108], publication after 2005 does not guarantee homogeneous RT quality. Differences in RT quality assurance and treatment planning could not be adjusted for, although such factors may affect oncologic outcomes in head and neck cancer. RT technique, dose, and fractionation were extracted, and altered fractionation schedules were modeled as separate treatment nodes where possible. However, because radiation delivery parameters were heterogeneously reported and unevenly distributed across comparisons, we could not perform a robust subgroup analysis or meta-regression, leaving residual RT-related heterogeneity as a limitation. The same limitation applies to possible subgroup analyses by HPV status and to subgroup-like treatment strategies, such as cetuximab plus adjuvant cetuximab and induction TPF plus cetuximab. As the nodes of these non-concurrent regimens were supported by few studies and were retained separately only because they represented clinically distinct interventions, their results should be interpreted with special caution. Late toxicity, quality of life, feeding tube dependence, and other functional outcomes could not be robustly analyzed because too few studies reported these endpoints using consistent definitions and time points. Additionally, excluding studies from before 2005 may have excluded earlier landmark CRT trials, potentially reducing network completeness and introducing selection bias.
Regimens containing induction or adjuvant systemic therapy were analyzed as separate nodes and not pooled with purely concurrent CRT regimens. Because these strategies represent distinct treatment paradigms and were supported by few studies, their estimates and rankings should be interpreted as exploratory. Furthermore, some HR were estimated from their Kaplan–Meier curves and OR from reported percentages, both methods allowing for rounding errors. Due to the selection of included studies, the network structure resulted in a high proportion of indirect comparisons and subnetworks with few patients, which are prone to confounding and also increase statistical inaccuracy through small-study effects [ref. 109]. Also, a high proportion of results showed a wide 95%-CI, so a substantial uncertainty regarding their true effect remains. Furthermore, several comparisons resulted in statistically non-significant results, which might be due to the selection of cisplatin as the reference, but more importantly, due to the high proportion of indirect comparisons. Due to these limitations, treatment rankings should be interpreted with caution. Therefore, rankings should not be considered a substitute for relative effect estimates or clinical judgment. Also, some studies had rather small sample sizes (e.g., Al-Saleh et al. [ref. 16], Essa et al. [ref. 22], Ezzat et al. [ref. 23]), which further adds to statistical dispersion and thus distortion of results. Also, the funnel plots of mucositis and OS hinted at a possible publication bias in the included studies, as well as possible bias through small-study effects. Although a frequentist random effects framework was used to account for between-study heterogeneity, the sparse network structure and high proportion of indirect comparisons limited the precision of several estimates. A Bayesian approach might have been an alternative, but results in such sparse networks may be sensitive to the choice of prior distributions.
5. Conclusions
Carboplatin + 5-FU and Mitomycin C + 5-FU improve LC compared to HART.
Compared to cisplatin, durvalumab and cetuximab are both associated with less dysphagia, while cetuximab is associated with less renal impairment compared to cisplatin. Panitumumab and cetuximab are associated with a decreased incidence of weight loss.
Overall, the findings of this analysis can show a trend in possible treatment options, but the evidence base is too limited for a definitive statement, and further research is necessary.
6. Highlights
- Network meta-analysis of non-cisplatin RT-based regimens relevant to cisplatin-ineligible LA HNSCC with RT.
- 28 RCTs (≈7000 patients) compared non-cisplatin concurrent systemic options.
- No regimen improved OS, PFS or LC versus cisplatin-based chemoradiotherapy.
- Carboplatin + 5-FU and mitomycin C + 5-FU improved LC versus HART.
- Durvalumab/cetuximab were associated with less dysphagia, and cetuximab with less renal toxicity and weight loss.
References
- H. Sung, J. Ferlay, R.L. Siegel, M. Laversanne, I. Soerjomataram, A. Jemal, F. Bray. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin., 2021. [DOI | PubMed]
- A. Wienecke, K. Kraywinkel. Epidemiologie von Kopf-Hals-Tumoren in Deutschland. Onkologie, 2019. [DOI]
- J.-P. Machiels, C.R. Leemans, W. Golusinski, C. Grau, L. Licitra, V. Gregoire. Reprint of “Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up”. Oral Oncol., 2021. [DOI | PubMed]
- CISplatin Injection
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Head and Neck Cancers. Version 1. 2026
- G.A. Curt, J.J. Grygiel, B.J. Corden, R.F. Ozols, R.B. Weiss, D.T. Tell, C.E. Myers, J.M. Collins. A phase I and pharmacokinetic study of diamminecyclobutane-dicarboxylatoplatinum (NSC 241240). Cancer Res., 1983. [PubMed]
- E.K. Rowinsky, L.A. Cazenave, R.C. Donehower. Taxol: A novel investigational antimicrotubule agent. J. Natl. Cancer Inst., 1990. [DOI | PubMed]
- S.M. Huang, P.M. Harari. Modulation of radiation response after epidermal growth factor receptor blockade in squamous cell carcinomas: Inhibition of damage repair, cell cycle kinetics, and tumor angiogenesis. Clin. Cancer Res., 2000. [PubMed]
- M.J. Page, J.E. McKenzie, P.M. Bossuyt, I. Boutron, T.C. Hoffmann, C.D. Mulrow, L. Shamseer, J.M. Tetzlaff, E.A. Akl, S.E. Brennan. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 2021. [DOI | PubMed]
- M.L. Chua, X. Zhang, K.C. Wong, G. Marret, A. Spreafico, B. Ma. Updates on Treatments and Management of Nasopharyngeal Carcinoma. Am. Soc. Clin. Oncol. Educ. Book, 2025. [DOI | PubMed]
- Y. Liu, N. Zhang, Y. Wen, J. Wen. Head and neck cancer: Pathogenesis and targeted therapy. MedComm, 2024. [DOI | PubMed]
- M.O. Rodríguez, T.C. Rivero, R.D.C. Bahi, C.R. Muchuli, M.A. Bilbao, E.N. Vinageras, J. Alert, J.J. Galainena, E. Rodríguez, E. Gracia. Nimotuzumab plus radiotherapy for unresectable squamous-cell carcinoma of the head and neck. Cancer Biol. Ther., 2010. [DOI | PubMed]
- C. Fallai, A. Bolner, M. Signor, A. Gava, G. Franchin, P. Ponticelli, R. Taino, F. Rossi, A. Ardizzoia, M. Oggionni. Long-term results of conventional radiotherapy versus accelerated hyperfractionated radiotherapy versus concomitant radiotherapy and chemotherapy in locoregionally advanced carcinoma of the oropharynx. Tumori J., 2006. [DOI]
- P. Nagpal, U. Suryanarayana, D.S. Pruthi, R.K. Vyas, M. Gohil. Comparison of concurrent chemoradiation with daily gefitinib versus daily erlotinib in locally advanced oropharyngeal cancers. Clin. Cancer Investig. J., 2021. [DOI]
- A. Argiris, J.E. Bauman, J. Ohr, W.E. Gooding, D.E. Heron, U. Duvvuri, G.J. Kubicek, D.M. Posluszny, M. Vassilakopoulou, S. Kim. Phase II randomized trial of radiation therapy, cetuximab, and pemetrexed with or without bevacizumab in patients with locally advanced head and neck cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol., 2016. [DOI]
- K. Al-Saleh, M. El-Sherify, R. Safwat, A. Elbasmy, J. Shete, A. Hussein, M. Nazeeh, A. Bedair. Phase II/III Randomized Controlled Trial of Concomitant Hyperfractionated Radiotherapy plus Cetuximab (Anti-EGFR Antibody) or Chemotherapy in Locally Advanced Head and Neck Cancer. Gulf J. Oncol., 2019
- J.A. Bonner, P.M. Harari, J. Giralt, N. Azarnia, D.M. Shin, R.B. Cohen, C.U. Jones, R. Sur, D. Raben, J. Jassem. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med., 2006. [DOI | PubMed]
- J. Bourhis, C. Sire, P. Graff, V. Grégoire, P. Maingon, G. Calais, B. Gery, L. Martin, M. Alfonsi, P. Desprez. Concomitant chemoradiotherapy versus acceleration of radiotherapy with or without concomitant chemotherapy in locally advanced head and neck carcinoma (GORTEC 99-02): An open-label phase 3 randomised trial. Lancet Oncol., 2012. [DOI | PubMed]
- V. Budach, M. Stuschke, W. Budach, M. Baumann, D. Geismar, G. Grabenbauer, I. Lammert, K. Jahnke, G. Stueben, T. Herrmann. Hyperfractionated accelerated chemoradiation with concurrent fluorouracil-mitomycin is more effective than dose-escalated hyperfractionated accelerated radiation therapy alone in locally advanced head and neck cancer: Final results of the radiotherapy cooperative clinical trials group of the German Cancer Society 95-06 Prospective Randomized Trial. J. Clin. Oncol., 2005. [PubMed]
- V. Budach, C. Stromberger, C. Poettgen, M. Baumann, W. Budach, G. Grabenbauer, S. Marnitz, H. Olze, K.-D. Wernecke, P. Ghadjar. Hyperfractionated accelerated radiation therapy (HART) of 70.6 Gy with concurrent 5-FU/Mitomycin C is superior to HART of 77.6 Gy alone in locally advanced head and neck cancer: Long-term results of the ARO 95-06 randomized phase III trial. Int. J. Radiat. Oncol. Biol. Phys., 2015. [DOI | PubMed]
- I. Chitapanarux, E. Tharavichitkul, P. Kamnerdsupaphon, N. Pukanhapan, R. Vongtama. Randomized phase III trial of concurrent chemoradiotherapy vs. accelerated hyperfractionation radiotherapy in locally advanced head and neck cancer. J. Radiat. Res., 2013. [DOI | PubMed]
- H.H. Essa, M. Azzam. Concurrent chemoradiation in locally advanced head and neck cancers: A comparative study of weekly Paclitaxel versus Cisplatin-based regimen. J. Egypt. Natl. Cancer Inst., 2010
- M. Ezzat, T. Shouman, K. Zaza, A. Safwat, A. El-Khoudary, M. El-Senosi, I. Ezzat. A randomized study of accelerated fractionation radiotherapy with and without mitomycin C in the treatment of locally advanced head and neck cancer. J. Egypt. Natl. Cancer Inst., 2005
- P. Olmi, S. Crispino, C. Fallai, V. Torri, F. Rossi, A. Bolner, M. Amichetti, M. Signor, R. Taino, M. Squadrelli. Locoregionally advanced carcinoma of the oropharynx: Conventional radiotherapy vs. accelerated hyperfractionated radiotherapy vs. concomitant radiotherapy and chemotherapy—A multicenter randomized trial. Int. J. Radiat. Oncol. Biol. Phys., 2003. [DOI | PubMed]
- M. Gebre-Medhin, E. Brun, P. Engström, H.H. Cange, L. Hammarstedt-Nordenvall, J. Reizenstein, J. Nyman, E. Abel, S. Friesland, H. Sjödin. ARTSCAN III: A Randomized Phase III Study Comparing Chemoradiotherapy with Cisplatin Versus Cetuximab in Patients with Locoregionally Advanced Head and Neck Squamous Cell Cancer. J. Clin. Oncol., 2021. [DOI | PubMed]
- L. Geoffrois, L. Martin, D. De Raucourt, X.S. Sun, Y. Tao, P. Maingon, J. Buffet, Y. Pointreau, C. Sire, C. Tuchais. Induction chemotherapy followed by cetuximab radiotherapy is not superior to concurrent chemoradiotherapy for head and neck carcinomas: Results of the GORTEC 2007-02 Phase III Randomized Trial. J. Clin. Oncol., 2018. [DOI | PubMed]
- M.L. Gillison, A.M. Trotti, J. Harris, A. Eisbruch, P.M. Harari, D.J. Adelstein, R.C.K. Jordan, W. Zhao, E.M. Sturgis, B. Burtness. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet, 2019. [DOI | PubMed]
- J. Giralt, J. Trigo, S. Nuyts, M. Ozsahin, K. Skladowski, G. Hatoum, J.-F. Daisne, A.C.Y. Ancona, A. Cmelak, R. Mesía. Panitumumab plus radiotherapy versus chemoradiotherapy in patients with unresected, locally advanced squamous-cell carcinoma of the head and neck (CONCERT-2): A randomised, controlled, open-label phase 2 trial. Lancet Oncol., 2015. [DOI | PubMed]
- A.A.-F. Halim, H.A. Wahba, H.A. El-Hadaad, A. Abo-Elyazeed. Concomitant chemoradiotherapy using low-dose weekly gemcitabine versus low-dose weekly paclitaxel in locally advanced head and neck squamous cell carcinoma: A phase III study. Med. Oncol., 2012. [PubMed]
- S.M. Magrini, M. Buglione, R. Corvò, L. Pirtoli, F. Paiar, P. Ponticelli, A. Petrucci, A. Bacigalupo, M. Crociani, L. Lastrucci. Cetuximab and Radiotherapy Versus Cisplatin and Radiotherapy for Locally Advanced Head and Neck Cancer: A Randomized Phase II Trial. J. Clin. Oncol., 2016. [DOI | PubMed]
- H. Mehanna, M. Robinson, A. Hartley, A. Kong, B. Foran, T. Fulton-Lieuw, M. Dalby, P. Mistry, M. Sen, L. O’Toole. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet, 2019. [PubMed]
- L.K. Mell, P. A Torres-Saavedra, S.J. Wong, J. A Kish, S.S. Chang, R.C. Jordan, T. Liu, M.T. Truong, E.W. Winquist, V. Takiar. Radiotherapy with cetuximab or durvalumab for locoregionally advanced head and neck cancer in patients with a contraindication to cisplatin (NRG-HN004): An open-label, multicentre, parallel-group, randomised, phase 2/3 trial. Lancet Oncol., 2024. [DOI | PubMed]
- C. Mercke, G. Wickart-Johansson, H. Sjödin, P.F.N. da Silva, G.A. von Döbeln, G. Margolin, S.J. Jaraj, H. Carstens, A. Berglund, I. Lax. Radiotherapy—Dose Escalated for Large Volume Primary Tumors—And Cetuximab with or without Induction Chemotherapy for HPV Associated Squamous Cell Carcinoma of the Head and Neck—A Randomized Phase II Trial. Cancers, 2023. [DOI | PubMed]
- R. Mesía, A. Rueda, R. Vera, A. Lozano, J.A. Medina, D. Aguiar, F. Árias, G. Triana, J. Carles, R. López-López. Adjuvant therapy with cetuximab for locally advanced squamous cell carcinoma of the oropharynx: Results from a randomized, phase II prospective trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol., 2013. [DOI]
- D. Rischin, M. King, L. Kenny, S. Porceddu, C. Wratten, A. Macann, J.E. Jackson, M. Bressel, A. Herschtal, R. Fisher. Randomized trial of radiation therapy with weekly cisplatin or cetuximab in low-risk hpv-associated oropharyngeal cancer (TROG 12.01)—A trans-Tasman radiation oncology group study. Int. J. Radiat. Oncol. Biol. Phys., 2021. [DOI | PubMed]
- M.G.R. Redda, R. Ragona, U. Ricardi, G. Beltramo, M. Rampino, P. Gabriele, S. Allis, M.R. La Porta, G. Moro, A. Melano. Radiotherapy alone or with concomitant daily low-dose carboplatin in locally advanced, unresectable head and neck cancer: Definitive results of a phase III study with a follow-up period of up to ten years. Tumori J., 2010. [DOI]
- R. Semrau, R.-P. Mueller, H. Stuetzer, S. Staar, U. Schroeder, O. Guntinas-Lichius, M. Kocher, H.T. Eich, A. Dietz, M. Flentje. Efficacy of intensified hyperfractionated and accelerated radiotherapy and concurrent chemotherapy with carboplatin and 5-fluorouracil: Updated results of a randomized multicentric trial in advanced head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys., 2006. [DOI | PubMed]
- L.L. Siu, J.N. Waldron, B.E. Chen, E. Winquist, J.R. Wright, A. Nabid, J.H. Hay, J. Ringash, G. Liu, A. Johnson. Effect of Standard Radiotherapy with Cisplatin vs. Accelerated Radiotherapy with Panitumumab in Locoregionally Advanced Squamous Cell Head and Neck Carcinoma: A Randomized Clinical Trial. JAMA Oncol., 2017. [PubMed]
- Y. Tao, A. Auperin, C. Sire, L. Martin, C. Khoury, P. Maingon, E. Bardet, M.-C. Kaminsky, M. Lapeyre, T. Chatellier. Improved outcome by adding concurrent chemotherapy to cetuximab and radiotherapy for locally advanced head and neck carcinomas: Results of the GORTEC 2007-01 Phase III Randomized Trial. J. Clin. Oncol., 2018. [DOI | PubMed]
- Y. Tao, J. Biau, X. Sun, C. Sire, L. Martin, M. Alfonsi, J. Prevost, A. Modesto, C. Lafond, J. Tourani. Pembrolizumab versus cetuximab concurrent with radiotherapy in patients with locally advanced squamous cell carcinoma of head and neck unfit for cisplatin (GORTEC 2015-01 PembroRad): A multicenter, randomized, phase II trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol., 2023. [DOI]
- D.J. Thompson, N.J. Slevin, H. Baines, G. Betts, S. Bolton, M. Evans, K. Garcez, J.H. Irlam, L. Lee, N. Melillo. A Randomised Placebo-controlled Trial of Synchronous NIMorazole Versus RADiotherapy Alone in Patients with Locally Advanced Head and Neck Squamous Cell Carcinoma Not Suitable for Synchronous Chemotherapy or Cetuximab. 2013
- Methodology Checklist 2: Randomised Controlled Trials. 2024
- B. Phillips, C. Ball, D. Sackett, D. Badenoch, S. Straus, B. Haynes, M. Dawes, J. Howick. Oxford Centre for Evidence-Based Medicine: Levels of Evidence (March 2009)
- J.A.C. Sterne, A.J. Sutton, J.P.A. Ioannidis, N. Terrin, D.R. Jones, J. Lau, J. Carpenter, G. Rücker, R.M. Harbord, C.H. Schmid. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ, 2011. [DOI | PubMed]
- M. Sydes, J. Tierney. Spreadsheet for Extracting Summary Statistics to Perform Meta-Analyses of Published Time-To-Event Data (Version 3.0), 2004
- M.K. Parmar, V. Torri, L. Stewart. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med., 1998. [DOI | PubMed]
- P.R. Williamson, C. Tudur Smith, J.L. Hutton, A.G. Marson. Aggregate data meta-analysis with time-to-event outcomes. Stat. Med., 2002. [DOI | PubMed]
- 48. R Core Team R: A Language and Environment for Statistical ComputingR Foundation for Statistical ComputingVienna, Austria2024
- B.P. Carlin, H. Hong, T.A. Shamliyan, F. Sainfort, R.L. Kane. Case Study Comparing Bayesian and Frequentist Approaches for Multiple Treatment Comparisons; AHRQ Methods for Effective Health Care, 2013
- J. Heukelom, O. Hamming, H. Bartelink, F. Hoebers, J. Giralt, T. Herlestam, M. Verheij, M.v.D. Brekel, W. Vogel, N. Slevin. Adaptive and innovative Radiation Treatment FOR improving Cancer treatment outcomE (ARTFORCE); a randomized controlled phase II trial for individualized treatment of head and neck cancer. BMC Cancer, 2013. [DOI | PubMed]
- Y. Tao, A. Aupérin, X. Sun, C. Sire, L. Martin, A. Coutte, C. Lafond, J. Miroir, X. Liem, F. Rolland. Avelumab–cetuximab–radiotherapy versus standards of care in locally advanced squamous-cell carcinoma of the head and neck: The safety phase of a randomised phase III trial GORTEC 2017-01 (REACH). Eur. J. Cancer, 2020. [DOI | PubMed]
- Y. Tao, A. Auperin, X. Sun, C. Sire, L. Martin, A. Coutte, C. Lafond, J. Miroir, X. Liem, F. Rolland. Avelumab-cetuximab-radiotherapy versus standards of care (SoC) in patients (pts) with locally advanced squamous cell carcinoma of head and neck (LA-SCCHN): Safety phase of randomized trial GORTEC 2017-01 (REACH). Ann. Oncol., 2019. [DOI]
- Y. Tao, A. Auperin, X.S. Sun, C. Sire, L. Martin, G. Bera, A. Coutte, J. Miroir, C. Lafond, N. Colin-Batailhou. Avelumab-cetuximab-radiotherapy (RT) versus standards of care (SoC) in locally advanced squamous cell carcinoma of the head and neck (SCCHN): Safety phase of the randomized trial GORTEC 2017-01 (REACH). J. Clin. Oncol., 2018. [DOI]
- Y. Tao, A. Aupérin, P. Graff, M. Lapeyre, V. Grégoire, P. Maingon, L. Geoffrois, P. Verrelle, G. Calais, B. Gery. Very accelerated radiotherapy or concurrent chemoradiotherapy for N3 head and neck squamous cell carcinoma: Pooled analysis of two GORTEC randomized trials. Oral Oncol., 2017. [DOI | PubMed]
- J. Bourhis, Y. Tao, X. Sun, C. Sire, L. Martin, X. Liem, A. Coutte, Y. Pointreau, J. Thariat, J. Miroir. LBA35 Avelumab-cetuximab-radiotherapy versus standards of care in patients with locally advanced squamous cell carcinoma of head and neck (LA-SCCHN): Randomized phase III GORTEC-REACH trial. Ann. Oncol., 2021. [DOI]
- A.D. Jensen, J. Krauss, K. Potthoff, C. Simon, A.V. Nikoghosyan, K. Lossner, J. Debus, M.W. Münter. Radiochemoimmunotherapy with intensity-modulated concomitant boost: Interim analysis of the REACH trial. Radiat. Oncol., 2012. [DOI | PubMed]
- Q.E. Zhang, Q. Wu, P.M. Harari, D.I. Rosenthal. Randomized phase II/III confirmatory treatment selection design with a change of survival end points: Statistical design of Radiation Therapy Oncology Group 1216. Head Neck, 2019. [DOI | PubMed]
- X. He, H. Yin, W. Guo, X. Sun, X. Hu, P. Yan, F. Li, S. Huang, H. Zhou, F. Zhang. Raltitrexed versus 5-fluorouracil with cisplatin and concurrent radiotherapy (CCRT) for locally advanced head and neck squamous cell carcinoma (LA-HNSCC): A randomized controlled multi-centered trial. Ann. Oncol., 2017. [DOI]
- S.M. McBride, E.J. Sherman, C.J. Tsai, S.S. Baxi, J. Aghalar, J. Eng, W.I. Zhi, D.C. McFarland, L.S. Michel, D. Spielsinger. A phase II randomized trial of nivolumab with stereotactic body radiotherapy (SBRT) versus nivolumab alone in metastatic (M1) head and neck squamous cell carcinoma (HNSCC). J. Clin. Oncol., 2018. [DOI]
- Q. Lei, Y. Wang, J. Sui, Q. Luo, F. Jin, B. Long, X. Shu, S. Li, L. Huang, M. Zhong. CAMRESBRT: Randomized Phase II Trial of Camrelizumab with Stereotactic Body Radiotherapy vs. Camrelizumab Alone in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys., 2022. [DOI]
- S. Venkateshulu, B.R.K. Kumar. A Study Comparing Acute Toxicities of Cetuximab and Cisplatin in Patients Undergoing Definitive Chemoradiation with Intensity-Modulated Radiotherapy for Locally Advanced Carcinoma Head and Neck. Cureus J. Med. Sci., 2021. [DOI]
- S. Venkateshulu, B.R. Kiran Kumar. Intensity modulated radiotherapy with cisplatin or cetuximab in patients undergoing chemoradiation for squamous cell carcinoma head and neck. Onkol. Radioter., 2021
- P. Vias, M. Gupta. PO-133 Concurrent Chemoradiation in Head and Neck Cancers Comparing Weekly Cisplatin vs. Oral Hydroxyurea. Radiother. Oncol., 2019. [DOI]
- B. Tamaskovics, M. Hecht, P. Schubert, A. Kallies, T. Illmer, J. Radke, O. Koelbl, F. Steger, T. Brunner, C. Rödel. 944TiP Randomized phase II study of immune stimulation with pembrolizumab and radiotherapy of recurrent and/or metastatic head and neck squamous cell carcinoma: The IMPORTANCE trial. Ann. Oncol., 2023. [DOI]
- J. Bourhis, B. Burtness, L.F. Licitra, C. Nutting, J.D. Schoenfeld, R.A. Sarkouh, F. Bouisset, H. Nauwelaerts, Y. Urfer, C. Zanna. TrilynX: A phase 3 trial of xevinapant and concurrent chemoradiation for locally advanced head and neck cancer. J. Clin. Oncol., 2021. [DOI]
- S. Yom, Z. Takacsi-Nagy, X. Liem, S. Salas, A. Debard, L. Finzi, O. Vivar, L. Farber, M. Gogishvili, G. Kristesashvili. NANORAY-312: A Phase III Pivotal Study of NBTXR3 Activated by Investigator’s Choice of Radiotherapy Alone or Radiotherapy in Combination with Cetuximab for Platinum-Based Chemotherapy-Ineligible Elderly Patients with Locally Advanced HNSCC. Int. J. Radiat. Oncol. Biol. Phys., 2022. [DOI]
- L. Mell, P. Torres-Saavedra, S. Wong, S. Chang, J. Kish, A. Minn, R. Jordan, T. Liu, M. Truong, E. Winquist. Radiotherapy with Durvalumab vs. Cetuximab in Patients with Locoregionally Advanced Head and Neck Cancer and a Contraindication to Cisplatin: Phase II Results of NRG-HN004. Int. J. Radiat. Oncol. Biol. Phys., 2022. [DOI]
- V.M. Patil, V. Noronha, N. Menon, A. Singh, S. Ghosh-Laskar, A. Budrukkar, A. Bhattacharjee, M. Swain, V. Mathrudev, K. Nawale. Results of Phase III Randomized Trial for Use of Docetaxel as a Radiosensitizer in Patients with Head and Neck Cancer, Unsuitable for Cisplatin-Based Chemoradiation. J. Clin. Oncol., 2023. [DOI | PubMed]
- B. Krishnamurthyreddy, M.S. Vidyasagar, R. Koteshwar, A. Shenoy, L. Viswanath, N. Thimmaiah, G. Babu, B. Joseph, R. Bonnathiya, P.P. Bapsy. A phase IIb 4-arm open-label randomized study to assess the safety and efficacy of h-R3 monoclonal antibody against EGFR in combination with chemoradiation therapy or radiation therapy in patients with advanced (stage III or IVA) inoperable head and neck cancer. J. Clin. Oncol., 2009. [PubMed]
- M. Ghi, A. Paccagnella, R. Orecchia, S. Parisi, F. Bertoni, N. Minguzzi, V. Baggio, G. Turcato, M. Polsinelli, I. Floriani. Cetuximab/Radiation Therapy (CET + RT) Versus Concomitant Chemoradiation Therapy (cCHT + RT) with or Without Induction Docetaxel/Cisplatin/5Fluorouracil (TPF) in Locally Advanced Head-and-Neck Squamous Cell Carcinoma (LASCCHN)—Preliminary Results on Toxicity of a Randomized, 2 × 2 Factorial, Phase II-III Study (NCT01086826). Int. J. Radiat. Oncol. Biol. Phys., 2012
- K.G. Babu, L. Viswanath, B.K. Reddy, K. Shenoy, A. Shenoy, T. Naveen, B. Joseph, M.S. Vidyasagar, R. Bonanthaya, C.T. Pasha. An open-label, randomized, study of h-R3mAb (nimotuzumab) in patients with advanced (stage III or IVa) squamous cell carcinoma of head and neck (SCCHN): Four-year survival results from a phase IIb study. J. Clin. Oncol., 2010
- L. Liu. Clinical Study of PD-1 Inhibitors Combined with Concurrent Radiotherapy and Chemotherapy in the Treatment of Locally Advanced Head and Neck Squamous cell Carcinoma: A Prospective, Randomized, Paralle Controlled Study
- EU Clinical Trials Register, Randomized Phase IV Trial to Compare Cetuximab with Concomitant Radiation Therapy with Concomitant Mitomycin-C and 5-FU with Radiation Therapy for Locally Advanced Squamous Cell Carcinomas of the Head and Neck. 2013
- EU Clinical Trials Register, Open Label Randomized Phase II, Multicentre, Pilot Study to Evaluate Safety and Efficacy of the Combination of Cetuximab and Concomitant-Boost Accelerated Radiotherapy Followed or Not by a Complementary Treatment with Cetuximab in Patients with Locally Advanced Oropharynx Squamous Cell Carcinoma. 2005
- EU Clinical Trials Register, A Phase 3 Study of Nivolumab or Nivolumab Plus Cisplatin, in Combination with Radiotherapy in Patients with Advanced Cancer of the Head and Neck. 2018
- R. Haddad, K. Harrington, L. Licitra, P. Brossart, D. Soulieres, L. Mell, L. Toms, J. Kopit, M. Lynch, V. Jayaprakash. CheckMate 9TM: Phase 3 study of nivolumab + radiotherapy (RT) vs. cetuximab + RT in cisplatin-ineligible patients with intermediate-/high-risk locally advanced squamous cell carcinoma of the head/neck. J. Immunother. Cancer, 2018
- Iranian Registry of Clinical Trials, Evaluation the Efficacy and Safety of Cetuximab Bio-Similar Compared to Erbitux in the Patients with Head and Neck Squamous Cell Carcinoma. 2019
- K.F. Klinghammer, T.C. Gauler, C. Stromberger, G. Kofla, M. De Wit, J. Gollrad, I. Rauer, P. Martus, I. Tinhofer, V. Budach. DURTRERAD: A phase II openlabel study evaluating feasibility and efficacy of durvalumab (D) and durvalumab and tremelimumab (DT) in combination with radiotherapy (RT) in non-resectable locally advanced HPV-negative HNSCC-Results of the preplanned feasibility interim analysis. J. Clin. Oncol., 2020
- H. Skinner. Randomized Phase II Trial of Stereotactic Body Radiation Therapy (SBRT) with Cetuximab +/− Docetaxel Followed by Adjuvant Cetuximab +/− Docetaxel in Recurrent, Previously-Irradiated Squamous Cell Carcinoma of the Head and Neck (SCCHN). 2013
- C. Wilke. A Randomized, Phase II Study of Definitive Radiotherapy with Concurrent Cisplatin vs. Docetaxel-cetuximab in Locally Advanced Head and Neck Squamous Cell Carcinoma: An ERCC1 Biomarker Enrichment and Interaction Design. 2014
- Randomized Trial of Avelumab-Cetuximab-Radiotherapy Versus SoCs in LA SCCHN (REACH). 2016
- L. Mell. Chemoradiation vs. Immunotherapy and Radiation for Head and Neck Cancer. 2017
- Institut Claudius Regaud, Cisplatin or ImmunoTHerapy in Association with Definitive Radiotherapy in HPV-Related Oropharyngeal Squamous Cell Carcinoma: A Randomized Phase II Trial. 2018
- P. Harari. Testing Docetaxel-Cetuximab or the Addition of an Immunotherapy Drug, Atezolizumab, to the Usual Chemotherapy and Radiation Therapy in High-risk Head and Neck Cancer. 2020
- NBTXR3 With or Without Cetuximab in LA-HNSCC. 2021
- D. Sher. Combining Radiation Therapy with Immunotherapy for the Treatment of Metastatic Squamous Cell Carcinoma of the Head and Neck. 2023
- M.-H. Hu, L.-W. Wang, H.-J. Lu, P.-Y. Chu, S.-K. Tai, T.-L. Lee, M.-H. Chen, M.-H. Yang, P.M.-H. Chang. Cisplatin-based chemotherapy versus cetuximab in concurrent chemoradiotherapy for locally advanced head and neck cancer treatment. BioMed Res. Int., 2014. [DOI | PubMed]
- C. Tang, C. Chan, W. Jiang, J.D. Murphy, R. von Eyben, A.D. Colevas, H. Pinto, N. Lee-Enriquez, C. Kong, Q.-T. Le. Concurrent cetuximab versus platinum-based chemoradiation for the definitive treatment of locoregionally advanced head and neck cancer. Head Neck, 2015. [PubMed]
- J. Baselga, J.M. Trigo, J. Bourhis, J. Tortochaux, H. Cortés-Funes, R. Hitt, P. Gascón, N. Amellal, A. Harstrick, A. Eckardt. Phase II multicenter study of the antiepidermal growth factor receptor monoclonal antibody cetuximab in combination with platinum-based chemotherapy in patients with platinum-refractory metastatic and/or recurrent squamous cell carcinoma of the head and neck. J. Clin. Oncol., 2005. [PubMed]
- J.-P. Pignon, A. le Maître, E. Maillard, J. Bourhis. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother. Oncol., 2009. [DOI | PubMed]
- A. Chauhan, H. Singh, T. Sharma, K.K. Manocha. Gemcitabine concurrent with radiation therapy for locally advanced head and neck carcinomas. Afr. Health Sci., 2008. [PubMed]
- Q. Li, J. Guan, Y. Zhang, M. Chen, L. Li, N. Xiao, M. Yang, Y. Dai, C. Zhang, L. Chen. A meta-analysis comparing cisplatin-based to carboplatin-based chemotherapy in moderate to advanced squamous cell carcinoma of head and neck (SCCHN). J. Clin. Oncol., 2015. [DOI]
- B. Caroline, Y. Sundus, D. Dawn, G. Carol, M. Susan. Cost analysis of cetuximab (Erbitux) plus radiotherapy (ERT) versus concomitant cisplatin plus radiotherapy (CRT) within an NHS oncology unit (single institution): A pilot study. Br. J. Radiol., 2016. [DOI | PubMed]
- A. Levy, P. Blanchard, S. Bellefqih, N. Brahimi, J. Guigay, F. Janot, S. Temam, J. Bourhis, E. Deutsch, N. Daly-Schveitzer. Concurrent use of cisplatin or cetuximab with definitive radiotherapy for locally advanced head and neck squamous cell carcinomas. Strahlenther. Onkol., 2014. [DOI | PubMed]
- R.H. Hamed, E. Elzahaf. Low dose weekly paclitaxel versus low dose weekly cisplatin with concomitant radiation in locally advanced head and neck cancers. J. Cancer Sci. Ther., 2011. [DOI]
- R. Jain, P. Kirar, G. Gupta, S. Dubey, S. Gupta, J. Goyal. A comparative study of low dose weekly paclitaxel versus cisplatin with concurrent radiation in the treatment of locally advanced head and neck cancers. Indian J. Cancer, 2009. [DOI | PubMed]
- J.K. Salama, D.J. Haraf, K.M. Stenson, E.A. Blair, M.E. Witt, R. Williams, R. Kunnavakkam, E.E.W. Cohen, T. Seiwert, E.E. Vokes. A randomized phase II study of 5-fluorouracil, hydroxyurea, and twice-daily radiotherapy compared with bevacizumab plus 5-fluorouracil, hydroxyurea, and twice-daily radiotherapy for intermediate-stage and T4N0-1 head and neck cancers. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol., 2011
- J.S. Tobias, K. Monson, N. Gupta, H. MacDougall, J. Glaholm, I. Hutchison, L. Kadalayil, A. Hackshaw. Chemoradiotherapy for locally advanced head and neck cancer: 10-year follow-up of the UK Head and Neck (UKHAN1) trial. Lancet Oncol., 2010. [DOI | PubMed]
- G.O. Janssens, S.E. Rademakers, C.H. Terhaard, P.A. Doornaert, H.P. Bijl, P. van den Ende, A. Chin, H.A. Marres, R. de Bree, A.J. van der Kogel. Accelerated radiotherapy with carbogen and nicotinamide for laryngeal cancer: Results of a phase III randomized trial. J. Clin. Oncol., 2012. [DOI | PubMed]
- M.G. Ghi, A. Paccagnella, D. Ferrari, P. Foa, F. Nole, F. Morelli, G. Azzarello, C. D’Ambrosio, C. Casanova, M. Guaraldi. Cetuximab/radiotherapy (CET + RT) versus concomitant chemoradiotherapy (cCHT + RT) with or without induction docetaxel/cisplatin/5-fluorouracil (TPF) in locally advanced head and neck squamous cell carcinoma (LASCCHN): Preliminary results on toxicity of a randomized, 2 × 2 factorial, phase II-III study (NCT01086826). J. Clin. Oncol., 2012
- J.J. Caudell, M.L. Gillison, E. Maghami, S. Spencer, D.G. Pfister, D. Adkins, A.C. Birkeland, D.M. Brizel, P.M. Busse, A.J. Cmelak. NCCN Guidelines® Insights: Head and Neck Cancers, Version 1.2022. J. Natl. Compr. Cancer Netw., 2022. [DOI | PubMed]
- F. Petrelli, F. Trevisan, M. Nardone, D. Carioli, A. Gasparini, C. Bramati, L. Bruschieri, V. Riboldi, V. Capriotti, A. De Stefani. Non-cisplatin concurrent agents plus definitive radiotherapy for locally advanced head and neck cancer: A network meta-analysis of randomized studies. Radiother. Oncol., 2025. [PubMed]
- J.R. Dettori, D.C. Norvell, J.R. Chapman. Fixed-Effect vs. Random-Effects Models for Meta-Analysis: 3 Points to Consider. Glob. Spine J., 2022. [DOI]
- G. Fabbrocini, L. Panariello, G. Caro, S. Cacciapuoti. Acneiform Rash Induced by EGFR Inhibitors: Review of the Literature and New Insights. Skin Appendage Disord., 2015. [PubMed]
- Y. Tian, C. Zhang, Q. Dang, K. Wang, Q. Liu, H. Liu, H. Shang, J. Zhao, Y. Xu, T. Wu. Risk of Rash in PD-1 or PD-L1-Related Cancer Clinical Trials: A Systematic Review and Meta-Analysis. J. Oncol., 2022. [PubMed]
- O. Iocca, A. Farcomeni, A. Di Rocco, P. Di Maio, P. Golusinski, S.P. López, A. Savo, R. Pellini, G. Spriano. Locally advanced squamous cell carcinoma of the head and neck: A systematic review and Bayesian network meta-analysis of the currently available treatment options. Oral Oncol., 2018. [DOI | PubMed]
- T. Gupta, S. Kannan, S. Ghosh-Laskar, J.P. Agarwal. Systematic review and meta-analyses of intensity-modulated radiation therapy versus conventional two-dimensional and/or or three-dimensional radiotherapy in curative-intent management of head and neck squamous cell carcinoma. PLoS ONE, 2018. [DOI | PubMed]
- L.J. Peters, B. O’Sullivan, J. Giralt, T.J. Fitzgerald, A. Trotti, J. Bernier, J. Bourhis, K. Yuen, R. Fisher, D. Rischin. Critical Impact of Radiotherapy Protocol Compliance and Quality in the Treatment of Advanced Head and Neck Cancer: Results from TROG 02.02. J. Clin. Oncol., 2010. [DOI | PubMed]
- C. Hong, G. Salanti, S.C. Morton, R.D. Riley, H. Chu, S.E. Kimmel, Y. Chen. Testing small study effects in multivariate meta-analysis. Biometrics, 2020. [PubMed]