
Cannabinoid Therapies in Less-Common Disorders: Clinical Evidence and Formulation Strategies
Abstract
Background/Objectives: Cannabinoids are increasingly recognised for their therapeutic potential beyond well-established indications such as chronic pain, multiple sclerosis, and specific epileptic syndromes. Recent advances have highlighted their possible role in less-common or orphan diseases, opening new avenues for pharmaceutical research and clinical application. Methods: This review provides a critical synthesis of the most recent evidence (2020–2025), available in PubMed and Scopus, regarding the use of cannabinoids in conditions including refractory epilepsies beyond Dravet and Lennox–Gastaut syndromes, movement disorders such as dystonia and Tourette syndrome, rare dermatological diseases like epidermolysis bullosa, and emerging data in Crohn’s disease. Results: Negative outcomes, such as those reported in Fragile X syndrome trials, are also discussed as instructive examples of methodological and pharmacological challenges. Particular attention is given to the optimisation of pharmaceutical formulations and advanced separation technologies, including oromucosal sprays, transdermal gels, and novel nanocarrier systems, which aim to overcome issues of bioavailability and variability in patient response. Finally, safety concerns, regulatory aspects, and the need for robust clinical trials are addressed. Conclusions: Overall, cannabinoids represent a promising yet underexplored therapeutic option in rare and complex disorders, warranting further investigation supported by innovative pharmaceutical approaches.
Article type: Review Article
Keywords: cannabinoids, medical cannabis, rare and complex disorders, clinical evidence, drug delivery systems, safety and regulation
Affiliations: Faculty of Health Sciences, Department of Medical Sciences, University of Beira Interior, Avenida Infante D. Henrique, 6200-506 Covilhã, Portugal; silvia.afonso@ubi.pt (S.A.); anabrinca99@gmail.com (A.T.B.); may.rosendo@ubi.pt (L.M.R.); tiago.rosado@ubi.pt (T.R.); apduarte@fcsaude.ubi.pt (A.P.D.); Centre for the Research and Technology of Agroenvironmental and Biological Sciences, CITAB, Inov4Agro, University of Trás-os-Montes and Alto Douro, UTAD, Quinta de Prados, 5000-801 Vila Real, Portugal; RISE-Health, Faculty of Health Sciences, Department of Medical Sciences, University of Beira Interior, Avenida Infante D. Henrique, 6200-506 Covilhã, Portugal; Laboratory of Pharmacotoxicology, UBIMedical, University of Beira Interior, EM506, 6200-000 Covilhã, Portugal; Beiras Academic Clinical Center (CACB)—Group of “Problemas Relacionados com Toxicofilias”, UBIMedical, EM506, 6200-000 Covilhã, Portugal
License: © 2026 by the authors. CC BY 4.0 Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Article links: DOI: 10.3390/diseases14020083 | PubMed: 41745121 | PMC: PMC12939546
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (814 KB)
1. Introduction
Cannabinoids have gained increasing recognition as therapeutic agents over the past two decades, driven by advances in pharmacology, regulatory changes, and a growing body of clinical evidence supporting their medical use [ref. 1,ref. 2]. While cannabis-derived products have historically been associated with recreational consumption, contemporary research has progressively repositioned cannabinoids as pharmacologically relevant compounds with well-defined mechanisms of action mediated primarily through the endocannabinoid system [ref. 3,ref. 4]. This system plays a central role in the modulation of pain perception, neuroinflammation, immune responses, motor control, and gastrointestinal function, providing a strong biological rationale for therapeutic intervention across a range of clinical conditions [ref. 1,ref. 5].
At present, the medical use of cannabinoids is largely confined to a limited number of well-established indications. For example, in Portugal, medicinal cannabis is authorised by the National Authority of Medicines and Health Products (Infarmed) for specific conditions, including chronic pain associated with oncological or neurological disease, spasticity related to multiple sclerosis or spinal cord injury, chemotherapy-induced nausea and vomiting, appetite stimulation in palliative care, treatment-resistant glaucoma, Tourette syndrome, and severe childhood epilepsies such as Dravet and Lennox–Gastaut syndromes [ref. 6]. These approved indications reflect areas in which clinical efficacy has been demonstrated with sufficient consistency to justify regulatory acceptance, particularly through standardised cannabis-based preparations and purified cannabidiol formulations [ref. 2,ref. 7]. Nevertheless, they also highlight the relatively narrow therapeutic scope within which cannabinoids are currently prescribed, despite their broad pharmacodynamic profile and multisystem effects [ref. 7,ref. 8]. In parallel with these approved uses, there has been a marked expansion of experimental and off-label investigations exploring cannabinoid-based therapies in less-common, rare, or complex disorders [ref. 9,ref. 10]. Many of these conditions are characterised by chronic symptom burden, limited treatment options, and substantial impact on quality of life, often meeting criteria for orphan disease designation [ref. 10]. In such contexts, conventional pharmacological strategies frequently provide inadequate symptom control or are associated with significant adverse effects, creating a pressing need for alternative or adjunctive therapeutic approaches. Cannabinoids, particularly non-psychoactive compounds such as cannabidiol (CBD), have emerged as promising candidates due to their multimodal mechanisms, favourable tolerability profiles, and potential to modulate neuroinflammatory, neuromodulatory, and immune pathways [ref. 1,ref. 5].
Despite growing clinical interest, the translation of cannabinoid research into routine clinical practice for rare or less-common disorders remains challenging [ref. 10]. Evidence is often fragmented, derived from small clinical trials, observational studies, or heterogeneous patient populations, and outcomes are frequently variable [ref. 11]. In addition, cannabinoids present well-recognised pharmaceutical challenges related to poor aqueous solubility, variable bioavailability, extensive first-pass metabolism, and marked inter-individual pharmacokinetic variability [ref. 12]. These limitations have prompted the development of innovative formulation strategies, including oromucosal sprays, transdermal systems, and nanocarrier-based delivery platforms, aimed at improving absorption, reducing variability, and enhancing therapeutic consistency. The optimisation of formulation and route of administration is therefore a critical determinant of clinical success, particularly in vulnerable populations and rare disease settings [ref. 12].
Safety considerations and regulatory frameworks further complicate the clinical adoption of cannabinoid-based therapies. Although cannabinoids are generally well tolerated, their interaction with cytochrome P450 enzymes, potential for drug–drug interactions, and context-dependent adverse effects necessitate careful clinical monitoring [ref. 12,ref. 13]. Moreover, regulatory acceptance varies substantially between jurisdictions, reflecting differences in risk–benefit assessment, evidentiary standards, and historical perceptions of cannabis-derived products [ref. 1,ref. 8]. These factors underscore the importance of critically appraising both positive and negative clinical outcomes, as well as identifying methodological limitations and unmet research needs.
Against this background, the present review aims to provide a comprehensive and critical synthesis of the most recent clinical evidence published between 2020 and 2025 regarding the use of cannabinoids in less-common and emerging clinical indications. Particular emphasis is placed on disorders that fall outside currently approved therapeutic uses, including rare neurological, dermatological, gastrointestinal, psychiatric, and sleep-related conditions. In addition, this review examines contemporary formulation strategies designed to overcome pharmacokinetic limitations, discusses safety and regulatory considerations, and highlights key gaps in current knowledge. By integrating clinical evidence with pharmaceutical and regulatory perspectives, this article seeks to clarify the realistic therapeutic potential of cannabinoids in rare and complex disorders and to inform future research and clinical decision-making. In this review, terminology reflects the nomenclature used in the original studies. “Medicinal cannabis” generally refers to whole-plant preparations or extracts, “phytocannabinoids” to plant-derived compounds such as Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD), and “cannabinoid therapies” as an umbrella term encompassing plant-derived, synthetic, or purified cannabinoid-based interventions. Where possible, the specific compound or formulation evaluated in each study is explicitly indicated.
2. Overview of Cannabinoids and the Endocannabinoid System
2.1. Brief Description of the Main Cannabinoids
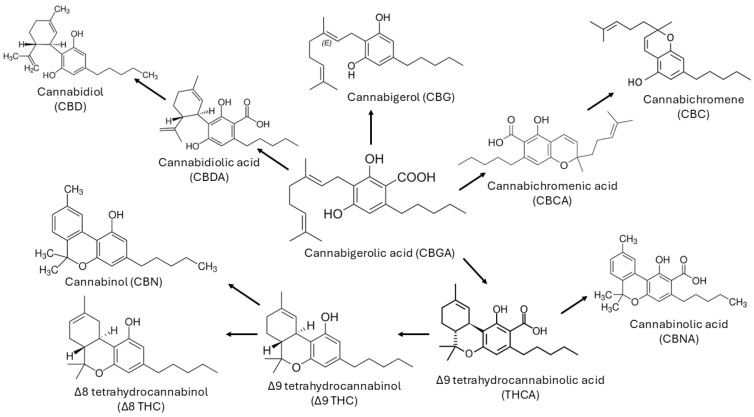
Terpenophenol cannabinoids are the most representative class of bioactive compounds present in Cannabis, with trans-Δ-9-tetrahydrocannabinol (THC) being the most potent in terms of psychoactive activity, among the more than 100 cannabinoids identified to date [ref. 14,ref. 15]. The (-)-trans isomer occurs naturally, although four stereoisomers of THC are known [ref. 16]. Other cannabinoids present in Cannabis include tetrahydrocannabinolic acid (THCA), cannabinol (CBN), CBD, and cannabidiolic acid (CBDA) [ref. 15]. Cannabigerolic acid (CBGA) is the precursor of CBDA and THCA [ref. 15]. When burned, it gives rise to THC and can also give rise, albeit in smaller quantities, to Δ-8-tetrahydrocannabinol (Δ8-THC) [ref. 15,ref. 16]. On the other hand, CBN results from the oxidative degradation of THC, especially in aged Cannabis samples [ref. 17,ref. 18,ref. 19,ref. 20] (Figure 1).
The legalisation of cannabis for medicinal purposes is growing, and several cannabinoids have been identified in cannabis strains. The main types of natural cannabinoids belong to the following families: cannabinol, cannabigerol (CBG), cannabitriol, cannabichromene, cannabinodiol, CBD, isocannabinoids, tetrahydrocannabinol, cannabicyclol, cannabielsoin, cannabicitran and cannabichromanone [ref. 16]. However, in these cases, the composition of the samples must be characterised by a specific composition, with reduced levels of THC (0.2–0.3% w/w) and with CBD and CBDA as major compounds [ref. 17,ref. 18,ref. 19]. The most promising compound for therapeutic purposes is CBD [ref. 21]. This compound has demonstrated several beneficial pharmacological effects, notably in combating inflammation, diabetes, cancer and affective or neurodegenerative diseases [ref. 21]. More recently, Δ-9-tetrahydrocannabivarin (THCV) has also shown potential use in the treatment of obesity [ref. 22]. Even so, Cannabis samples for use in the pharmaceutical and nutraceutical fields have CBDA as the most abundant compound [ref. 15].
2.2. Relevant Mechanisms of Action
The endocannabinoid system is the primary pathway through which cannabinoids exert their physiological and therapeutic effects. The action of these compounds occurs mainly through cannabinoid receptor type 1 (CB1) and cannabinoid receptor type 2 (CB2) receptors via mechanisms of agonism, modulation or antagonism [ref. 23]. These receptors are found coupled to Gi/Go proteins, leading to the inhibition of adenylate cyclase and, consequently, to the reduction of the conversion of AMP to cyclic AMP [ref. 23]. The diversity of pharmacological responses is largely linked to the fact that these receptors have a wide distribution in the body [ref. 16]. CB1 receptors are found primarily in the central and peripheral nervous system, but also in organs such as the heart, spleen, endocrine glands, and tissues of the gastrointestinal, urinary, and reproductive systems [ref. 24]. On the other hand, CB2 receptors predominate in immune and hematopoietic cells, namely leukocytes, spleen and tonsils, and are of particular therapeutic interest due to their regulatory role in inflammatory processes [ref. 23,ref. 25].
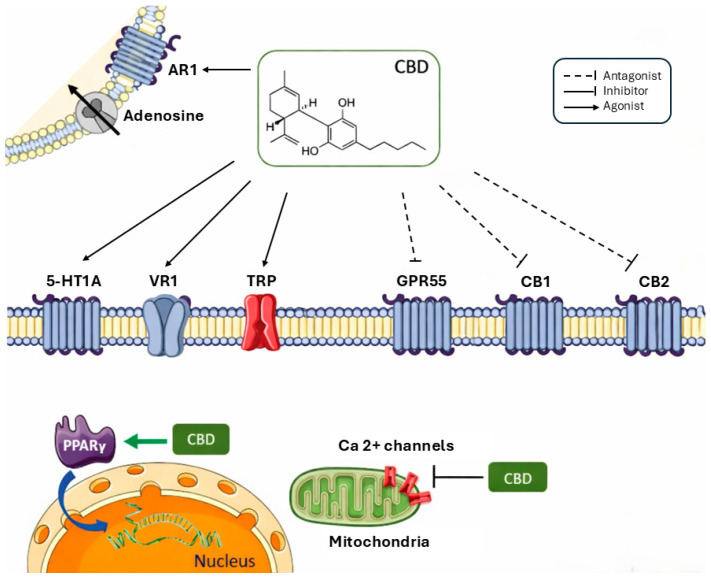
The affinity and effectiveness of cannabinoids depend on the receptor. In the specific case of THC, there is partial agonism of CB1 and CB2 receptors, being more effective on the former [ref. 23,ref. 26]. Activation of CB1 receptors explains both its psychoactive and analgesic effects, since these receptors directly modulate nociceptive transmission [ref. 17]. At the immunological level, the interaction of THC with CB2 receptors contributes to immunomodulatory effects, influencing inflammatory responses and neuroinflammation processes [ref. 17]. Thus, although THC has relevant therapeutic potential, its psychoactive profile and the possibility of inducing anxiety, dysphoria or psychotic symptoms in susceptible individuals limit its wider clinical applicability [ref. 27]. Conversely, CBD is widely recognised for its therapeutic properties without significant psychoactive effects. Despite having low affinity for CB1 and CB2 receptors [ref. 28,ref. 29], CBD exhibits a multi-target pharmacology [ref. 30], involving both modulators of the endocannabinoid system and other physiological pathways. Recent studies suggest that CBD may exert its beneficial effects through GPR55 receptors in the CA1 hippocampus [ref. 31,ref. 32]. Others have shown that CBD acts as an allosteric modulator of the CB1R receptor, indirectly influencing its activity [ref. 29]. CBD also non-competitively antagonises CB1 and CB2 agonists [ref. 33] and may modulate THC effects under certain circumstances. In addition, this compound inhibits anandamide reuptake as well as its enzymatic hydrolysis [ref. 34].
Cannabinoids also act on transient potential channels (TRP) [ref. 16]. These, found in cell membranes, interact with different molecules, triggering a response [ref. 35]. In the particular case of TRPV1s, which are distributed throughout the dorsal root and trigeminal ganglia, skin, bladder, brain, peripheral nerve endings, pancreas and testes, they are activated by the endocannabinoid anandamide under specific conditions [ref. 36]. Studies have shown that CBD also has the ability to stimulate vanilloid receptors (VR1), with effects similar to the natural agonist of this receptor [ref. 34]. This receptor is associated with effects such as inflammatory hyperalgesia, whose rapid desensitisation, with subsequent paradoxical analgesic and anti-inflammatory effects, is frequent [ref. 37]. However, CBD has been shown to be able to exert anti-inflammatory action by desensitising VR1 [ref. 34]. CBD also exerts significant actions on the serotonergic 5-hydroxytryptamine 1A (5-HT1A) receptor, acting as an agonist of these receptors [ref. 37,ref. 38]. This mechanism translates into anxiolytic and neuroprotective effects [ref. 39]. Another relevant mechanism is the action of CBD in decreasing adenosine reuptake [ref. 37]. This effect may lead to a decrease in inflammation through the inhibition of the reuptake of this compound [ref. 37].
The modulation of intracellular calcium homeostasis represents another mechanism of particular therapeutic relevance. CBD is able to exert its pharmacological effects by modulating the intracellular concentration of Ca2+, namely by increasing [Ca2+]i in hippocampal neurons, more specifically through the release of mitochondrial Ca2+ and L-type voltage-gated Ca2+ channels [ref. 21]. CBD also has a high antioxidant power; however, the increase in [Ca2+]i in a tumour environment leads to the formation of reactive oxygen species (ROS) and cell apoptosis [ref. 40,ref. 41]. In fact, studies have shown that CBD hydroxyquinone reduces colon cancer growth in athymic mice [ref. 42]. Furthermore, some cannabinoids activate peroxisome proliferator-activated receptors (PPARs), which consist of groups of nuclear receptor proteins that regulate gene expression, development, metabolism, cell differentiation, and tumorigenesis in higher organisms [ref. 16]. Some of the effects associated with the use of cannabinoids are triggered in this way, namely analgesic, antitumor, gastrointestinal, neuroprotective, anti-inflammatory, neuronal function modulation, metabolic and cardiovascular effects [ref. 43]. The main mechanisms of action are described in Figure 2.
Although less studied than THC and CBD, other cannabinoids act on the body through these and other mechanisms. The compounds CBG and cannabichromene (CBC) have the ability to inhibit anandamide inactivation, potentially enhancing the effects of endocannabinoids, as they exhibit very low affinity for CB1 and CB2 receptors [ref. 40]. CBG and CBC are also capable of activating TRPV1, and along with the latter, CBD, CGB, and CBDA exhibit the ability to activate TRPA1. Additionally, CBD, CGB, and CBDA act as antagonists of transient receptor potential melastatin type 8 (TRPM8) [ref. 40,ref. 44]. THCV also behaves as a potent partial agonist of CB2 and as an antagonist of CB1 [ref. 45]. Due to this dual action, this compound shows therapeutic potential in appetite control [ref. 46] or in epilepsy [ref. 47].
2.3. Formulation Challenges According to General Pharmacokinetic/Pharmacodynamic Processes
Cannabinoids have been increasingly attracting interest in the scientific community; however, the pharmacodynamics and pharmacokinetics of these compounds are not widely known [ref. 48]. In the case of cannabinoids with therapeutic applications, the scarcity of data is even more pronounced, limiting the possible applications [ref. 48]. Understanding pharmacokinetics is closely linked to the route of administration [ref. 16]. According to the literature, the processes of absorption, distribution, metabolism, and excretion exhibit high inter-individual variability, hindering the use of these compounds for medicinal purposes.
The respiratory tract is the preferred route for administering cannabinoids, with vaporisation being used, although not exclusively, for therapeutic purposes [ref. 48]. Inhalation allows cannabinoids to pass rapidly from the lungs into the bloodstream and subsequently to the brain, with CBD being detected seconds after inhalation [ref. 48,ref. 49]. This compound reaches its maximum concentration between approximately 3 and 10 min after consumption; however, its bioavailability is about 31% [ref. 23,ref. 50,ref. 51,ref. 52]. Factors such as depth and volume of inhalation, combustion temperature and device used, and compound losses due to pyrolysis lead to great variability [ref. 48,ref. 53,ref. 54,ref. 55].
Oral administration in capsule form is also widely used in a therapeutic context, with CBD exhibiting a bioavailability of less than 20%, due to the lipophilicity of the compound and hepatic metabolism [ref. 23,ref. 25,ref. 49,ref. 56,ref. 57]. Even so, CBD can reach peak concentration in the bloodstream between 1 and 2 h after consumption [ref. 23,ref. 48]. The oromucosal and sublingual routes are also common in a therapeutic context, allowing not only faster absorption but also avoiding first-pass hepatic metabolism [ref. 15,ref. 48]. Additionally, plasma concentrations of cannabinoids are higher compared to the oral route [ref. 48]. However, cannabinoids have a lipophilic character, which is one of the main obstacles to the formulation of this type of drug. In the case of CBD, it has an oil/water partition coefficient of 6.3, indicating a strong lipid preference [ref. 58]. This factor makes it difficult to dissolve in aqueous media, limits oral absorption, and contributes to significant variability in bioavailability [ref. 25,ref. 56,ref. 57]. In fact, studies report a great heterogeneity with respect to the range of concentrations detected, which vary from 0.4 to 16.5 μg/L [ref. 59,ref. 60]. Additionally, absorption of compounds when ingested orally is also highly influenced by diet, pH of the gastrointestinal tract and type of formulation [ref. 58,ref. 61]. Concomitant ingestion with foods rich in fat favours absorption (about 14 times) and contributes to the reduction of first-pass hepatic metabolism and lymphatic transport [ref. 58]. In the particular case of oromucous and sublingual formulations, these allow bypassing first-pass metabolism; however, a significant portion of the dose is absorbed in the gastrointestinal tract after swallowing, affecting bioavailability [ref. 58].
Also, for therapeutic purposes, the transdermal route is used, once again avoiding first-pass metabolism [ref. 23,ref. 49]. Although cannabinoids have a lipophilic character and, consequently, limited dermal diffusion, CBD permeates the skin more easily than THC [ref. 48,ref. 62,ref. 63]. Once again, this pathway allows bypassing first-pass hepatic metabolism [ref. 16]. Studies have shown that the use of gels and emulsions can contribute to an increase in plasma concentrations of CBD, when compared with oil formulations [ref. 58]. However, skin permeability remains a challenge and is also dependent on the use of excipients [ref. 62,ref. 64,ref. 65].
Finally, although less studied, both the ophthalmic and rectal routes constitute alternatives for therapeutic application [ref. 23]. Other routes of administration for recreational use include smoking and oral administration in the form of food products [ref. 16].
The distribution of cannabinoids throughout the body’s tissues occurs rapidly, so their plasma concentration decreases in the same way [ref. 49]. Some factors, such as the chemical properties of the molecules, the vascularisation of the tissues, the body composition and the health status of each individual, are closely linked to the degree of distribution of these compounds [ref. 66]. Thus, more vascularized tissues, such as the brain, lungs, heart, and liver, rapidly accumulate these compounds, with a volume of distribution for CBD of 32 L/kg [ref. 51,ref. 67,ref. 68,ref. 69,ref. 70]. The lipophilicity of cannabinoids favours their accumulation in adipose tissue, which can result in prolonged redistribution [ref. 23,ref. 48,ref. 51,ref. 67]. This accumulation can greatly influence elimination times, which can vary from hours to weeks. This fact could explain the persistence of cannabinoids in the body. Additionally, individual factors such as sex, body composition, or variations in metabolism can also influence tissue and plasma concentrations [ref. 23,ref. 66]. Once again, these factors contribute significantly to the difficulties in obtaining formulations with controlled release over time, especially in repeated doses.
After distribution, CBD undergoes metabolism in the liver, initially by CYP2C19 and CYP3A4 and subsequently by CYP1A1, CYP1A2, CYP2C9 and CYP2D6 [ref. 13,ref. 48]. Even though the metabolization reactions include oxidations at C-9 and in the side chain, a portion is excreted unchanged [ref. 49]. CBD exhibits a wide variation in its half-life, with elimination times ranging from 2 to 50 days after oral ingestion [ref. 71] and approximately 31 h after inhalation [ref. 51]. Cannabinoids are primarily metabolised by enzymes of the CYP family. However, CBD acts as a competitive inhibitor of these enzymes, which may lead to drug interactions with drugs metabolised by the same pathways [ref. 13,ref. 72]. In fact, studies have reported that this concomitant administration can triple plasma concentrations of active compounds [ref. 73]. CBD can also give rise to polymorphisms, which may result in reduced drug efficacy, side effects and interactions [ref. 74]. Finally, it was also described that CBD and THC can interact, interfering with their pharmacodynamics [ref. 37]. CBD has demonstrated inhibitory properties on drug metabolism [ref. 75,ref. 76], as well as the metabolic hydroxylation of THC in humans [ref. 77]. However, other studies describe the possible potentiation of the effects caused by THC, by CBD [ref. 37]. This interactive complexity represents an additional obstacle for combined formulations.
After being metabolised, cannabinoids are excreted for days, with 16% of CBD metabolites being excreted in the urine within 72 h, and a high proportion also being eliminated unchanged in the faeces [ref. 23,ref. 78]. In general, the elimination of cannabinoids is slow and variable [ref. 79]. Therefore, it becomes difficult to estimate the elimination time, which is also conditioned by redistribution from adipose tissue, and consequently, to determine safe and stable dosage intervals.
2.4. Regulatory Status and Approved Products for Common Indications
Since 2012, with the approval of cannabis for recreational use in some states of the United States of America, Uruguay and Canada, the debate about its prohibition/authorisation has been growing [ref. 16]. In fact, both cannabis and cannabis resin are listed in Schedules I and IV of the 1961 United Nations Single Convention on Narcotic Drugs [ref. 80]. However, with regard to its use for medicinal purposes, its use is not prohibited by international law [ref. 16]. It is important to understand that the term medicinal cannabis can refer to different forms with different legal implications [ref. 81]. Thus, there is cannabis in natura, which refers to any part of any plant of the genus Cannabis, including C. indica, C. sativa and C. ruderalis [ref. 81]. There is also cannabis extract, which consists of oil extracted from the plant or derived preparations, or cannabinoids, the compounds present in the cannabis plant [ref. 81].
In recent years, more countries have allowed the use of medicinal cannabis, so there has been a shift in policies. Still, there are some reservations due to concerns about dependence and adverse effects [ref. 81]. The European Medicines Agency (EMA) and the Food and Drug Administration (FDA) have also resisted approving cannabis-based medicines; however, several European countries and some US states have been changing their regulations, allowing the use of medicinal cannabis [ref. 81,ref. 82,ref. 83]. Thus, in Europe, THC can be used in capsules, cannabis flowers can be used in infusions/decoctions or in the form of vaporisation. Marijuana extract can be used as an oral spray [ref. 84]. However, most European countries prohibit the use of cannabis for consumption in its natural state, allowing cannabinoid-based medicines [ref. 81]. This is the case with Nabiximols (Sativex®), which has gained wide acceptance and is authorised for use in most countries of the European Union. This formulation, based on cannabis plant extract, consists of an oromucosal spray containing THC and CBD [ref. 85]. Nabiximols is indicated for the treatment of spasticity associated with multiple sclerosis, particularly after previous treatments have failed. Its use has also been authorised for neuropathic pain associated with multiple sclerosis [ref. 81,ref. 85,ref. 86]. Similarly, Nabilona (Cesamet® or Canemes®) has also been used in various European countries. It consists of oral capsules containing a synthetic cannabinoid similar to THC, indicated for the treatment of chemotherapy-induced nausea and vomiting in cancer patients [ref. 85,ref. 86]. The use of Dronabinol (Marinol® or Syndros®) has also been approved in some European countries. This medication consists of an oral solution or capsules containing synthetic THC and is indicated for treating anorexia associated with weight loss in patients with AIDS, and nausea and vomiting associated with chemotherapy for cancer [ref. 85,ref. 86].
In the US, California was the first state to authorise the use of medicinal cannabis, back in 1996 [ref. 81]. Currently, several other states have enacted their own laws regulating the use of medicinal cannabis [ref. 87]. However, some states require physicians to have a state registration or to complete a brief medical education program on cannabis as a prerequisite for their registration [ref. 88]. The FDA has approved Cesamet®, Marinol®, and Syndros® for therapeutic use in the United States [ref. 81,ref. 89,ref. 90]. Still, nearly all states limit the conditions under which cannabis can be prescribed, sometimes restricting it to cases where the doctor considers that the treatment outweighs the risks to the patient’s health [ref. 91,ref. 92].
In other countries, such as Canada, the use of cannabis for medicinal purposes has been permitted since 2014 [ref. 81]. In 2016, Health Canada created a Cannabis for Medical Purposes Regulation, under which patients authorised to use cannabis can register and produce a limited quantity of cannabis for their own medicinal purposes, or designate another person for this task [ref. 93,ref. 94,ref. 95]. Nabiximols can also be used in the treatment of spasticity or symptomatic relief of neuropathic pain associated with multiple sclerosis [ref. 81]. It can also be administered to patients with advanced cancer who experience moderate to severe pain during treatment [ref. 81]. Nabilone is also authorised for severe nausea and vomiting associated with cancer chemotherapy. Finally, dronabinol is also permitted for the treatment of AIDS-related anorexia and severe nausea and vomiting associated with cancer chemotherapy [ref. 96].
Raw cannabis is only authorised in a small number of countries, namely Canada, Germany, Israel and the Netherlands, as well as some US states, with magistral preparations of cannabis plants being more accepted [ref. 81]. The most widely accepted approach is for doctors to specifically indicate the purposes for which patients can use medicinal marijuana and its formulations. Nevertheless, many countries have been changing their legislation over the years to allow the use of these substances [ref. 81].
3. Clinical Evidence in Less-Common Disorders
The clinical conditions discussed in this section were identified through a structured literature search conducted in PubMed and Scopus, using the following search strategies: ((cannabinoids) OR (phytocannabinoids)) AND (medical applications) and ((cannabinoids) OR (cannabidiol) OR (medical cannabis) OR (phytocannabinoids)) AND (rare disorders). The search was restricted to publications between 2020 and 2025, and only peer-reviewed articles reporting clinical data were considered eligible for inclusion. Studies were excluded if full-text access was not available, if they reported protocols or ongoing trials without published outcomes, or if they focused on clinical indications that are already well established in clinical practice for cannabinoid-based therapies. These included spasticity associated with multiple sclerosis or spinal cord injury, chemotherapy-induced nausea and vomiting, appetite stimulation in palliative care, chronic pain, Tourette syndrome, severe childhood epilepsies (Dravet and Lennox–Gastaut syndromes), and treatment-resistant glaucoma [ref. 6]. Consequently, this section focuses exclusively on less-common, emerging, or off-label clinical indications for which cannabinoids are not yet formally approved, allowing a critical appraisal of both positive and negative clinical evidence in areas where therapeutic need remains largely unmet.
When interpreting the findings discussed throughout this section, several important limitations must be acknowledged. Across literature, sample sizes are frequently modest, substantially limiting statistical power and the reliability of effect estimates. Many investigations are further restricted to specific age groups or to a single sex, thereby reducing the generalizability of findings to broader, more heterogeneous patient populations. Participant cohorts are often clinically heterogeneous, particularly with respect to comorbid neurological or systemic conditions, which complicates the attribution of observed effects to cannabinoid-based interventions alone. Additionally, the routine exclusion of individuals with significant cardiovascular or psychiatric comorbidities, as well as the limited representation of ethnically diverse populations, further constrains external validity and limits the applicability of results to real-world clinical settings.
From a design perspective, several studies lack a control or placebo group, while others rely exclusively on observational methodologies. In paediatric and elderly populations in particular, outcome assessments frequently depend on caregiver or parent-reported measures, increasing susceptibility to subjective bias. Most available studies primarily evaluate short-term or acute effects of cannabinoid administration, leaving uncertainty as to whether repeated or long-term use leads to sustained neurobiological changes or clinically meaningful benefits over time. The frequent absence of objective behavioural, functional, or neurophysiological outcome measures further heightens the risk of bias, as improvements may reflect placebo effects, regression to the mean, expectancy bias, or indirect caregiver relief rather than true therapeutic efficacy.
Additional methodological concerns include potential crossover order effects in within-subject designs, insufficient pharmacokinetic and dose–response data, and reduced statistical power for secondary or exploratory outcomes. Collectively, these limitations underscore the need for larger, well-controlled, longitudinal trials incorporating objective outcome measures, diverse participant populations, and rigorous methodological frameworks to more accurately determine the clinical efficacy and safety profile of cannabinoid-based therapies.
Across multiple clinical trials, cannabinoid treatments were generally well tolerated in diverse patient populations [ref. 97,ref. 98,ref. 99,ref. 100,ref. 101,ref. 102,ref. 103,ref. 104,ref. 105,ref. 106,ref. 107,ref. 108,ref. 109,ref. 110,ref. 111]. Most adverse events reported were mild to moderate in severity, transient, and rarely required dose adjustment or treatment discontinuation [ref. 97,ref. 98,ref. 99,ref. 101,ref. 102,ref. 103,ref. 105,ref. 106,ref. 108,ref. 109]. Commonly observed AEs included somnolence, fatigue, decreased appetite, gastrointestinal symptoms (diarrhoea, nausea), dizziness, headache, and dry mouth [ref. 98,ref. 100,ref. 101,ref. 102,ref. 103,ref. 104,ref. 108,ref. 110,ref. 111]. Behavioural changes, transient seizure worsening, or increased anxiety were occasionally reported but were typically dose-dependent and resolved spontaneously or with dose adjustment [ref. 99,ref. 103,ref. 104].
Serious adverse events were rare, with only a few cases possibly related to treatment, such as tonic–clonic seizures requiring hospitalisation or persistent fatigue leading to discontinuation in isolated participants [ref. 99,ref. 103]. Hepatic enzyme elevations were generally mild, transient, and resolved without intervention, with no recurrent or clinically significant laboratory abnormalities reported [ref. 97,ref. 100,ref. 103,ref. 104,ref. 105,ref. 106]. No clinically relevant changes were observed in hematologic parameters, vital signs, or electrocardiographic measures, and drug–CBD interactions were minimal, even with concomitant medications [ref. 97,ref. 101,ref. 105,ref. 106].
The temporal pattern of adverse events suggests most occurred early during the titration phase and diminished with continued treatment [ref. 100]. Some studies highlighted advantages of specific formulations, such as transdermal CBD, reducing gastrointestinal side effects and avoiding first-pass hepatic metabolism [ref. 99], and ZTL-101 showing rapid resolution of side effects overnight, minimising next-day residual effects [ref. 107,ref. 111]. Across studies, careful dose titration and monitoring, especially in patients receiving concomitant medications such as valproate or benzodiazepines, helped mitigate adverse events [ref. 98,ref. 100,ref. 105,ref. 106].
Overall, cannabinoid formulations demonstrated an acceptable safety and tolerability profile, with most adverse events being mild, reversible, and manageable, supporting their potential use as adjunct therapies in various clinical populations [ref. 97,ref. 98,ref. 99,ref. 100,ref. 101,ref. 102,ref. 103,ref. 104,ref. 105,ref. 106,ref. 107,ref. 108,ref. 109,ref. 110,ref. 111].
3.1. Refractory Epilepsies Beyond Dravet and Lennox–Gastaut Syndromes
Refractory epilepsies beyond Dravet and Lennox–Gastaut syndromes comprise a heterogeneous group of conditions characterised by persistent seizures despite adequate trials of multiple antiseizure therapies. This category includes drug-resistant focal epilepsies and several developmental and epileptic encephalopathies, often associated with early onset, cognitive impairment, and significant neuropsychiatric comorbidity. Beyond Dravet and Lennox–Gastaut syndromes, cannabinoid-based therapies have been explored in other forms of refractory epilepsy, with emerging but less robust evidence. However, responses are variable and generally less pronounced than in approved indications. The main characteristics and clinical outcomes of the studies discussed in this section are summarised in Table 1.
Table 1: Cannabinoids in Refractory Neurological and Neurodevelopmental Disorders Beyond Dravet and Lennox–Gastaut Syndromes.
| Ref. | [ref. 97] | [ref. 112] | [ref. 101] | [ref. 104] | [ref. 102] | [ref. 113] | |
|---|---|---|---|---|---|---|---|
| Safety | Reported as safe and well tolerated (no major safety signals described) | Not specifically detailed | No major safety concerns reported | Well tolerated; no significant neuroscore changes | Somnolence correlated with response; generally acceptable tolerability | Suggests comparatively good tolerability | |
| Key Findings | Median seizure reduction 82%; 4/5 achieved ≥50% reduction; 3/5 > 75%; median seizures reduced from 32/month to ~6–7/month; 4 patients reduced/discontinued ≥1 ASM | Parental-reported improvements in irritability, emotional regulation, social responsiveness; 22 lipid biomarkers identified (46% significantly modulated); modulation of sphingolipids/phospholipids/fatty acids suggesting homeostatic effect | 90% improved in ≥1 severe symptom; 83.5% of symptoms improved; 30–40% mean improvement in irritability, withdrawal, hyperactivity; 50% improved RRBs; modest sleep improvement | Significant seizure reduction at week 14 and follow-up; 3/5 sustained ≥50% reduction; improved QoL; subjective functional gains | 49% “much/very much improved” with whole-plant vs. 21% placebo; modest BMI reduction; male sex/younger age associated with greater response; dose-response trend | 9/34 received CBD; partial seizure reduction in majority; no sustained seizure freedom; lower withdrawal rate vs. other ASMs | |
| MainOutcomes | Seizure frequency reduction | Behavioural domains; salivary lipid biomarkers | Behavioural scales (ABC, Vineland-II), sleep, parental stress | Seizure frequency; quality of life; neuroscore | Clinical Global Impression–Improvement; behavioural scales; BMI | Seizure control; long-term outcomes | |
| Compound/FormulationDose & Duration | CBDV2.5 mg/kg/day titrated to ~10 mg/kg/day; duration not explicitly stated | Individualised medical cannabis treatment (CBD 7.5–200 mg/dose; THC 0.05–50 mg/dose; up to TID)≥1 year | Purified CBDMedian initial dose 138.75 mg; median total 363.5 mg; median follow-up 11 months | Adjunctive CBD 5–25 mg/kg/day; long-term extension up to 63–80 weeks | Whole-plant CBD:THC (20:1); purified CBD:THC (20:1) 12 weeks | Oil-diluted cannabis extract, Bedrocan® 22% THC, 0.5% CBD, Olive Oil 50 mL, twice a day for 12 weeks | |
| Population | 5 female children; median age 12.6 years; severe drug-resistant epilepsy | 15 children (mean age 9.4 years) on medical cannabis ≥ 1 year; 9 controls | 20 paediatric patients (85% male); mean age 10 ± 4.6 years; multiple psychotropics | 5 patients (4F, 1M); mean age 8.8 ± 6.3 years | 150 participants aged 5–21 years | 34 patients (30F, 4M); age 1–28 years; early-onset refractory epilepsy | |
| Study Design | Phase 1, open-label | Observational | Prospective, observational, before–after | Open-label exploratory study | Randomised, double-blind, placebo-controlled trial | Multicentre observational | |
| Disease | Rett Syndrome (MECP2-related) with refractory epilepsy | Autism Spectrum Disorder | Autism Spectrum Disorder with intellectual disability | Sturge–Weber Syndrome with treatment-resistant epilepsy | Autism Spectrum Disorder (severe) | CDKL5 Deficiency Disorder | |
| Ref. | [103] | [100] | [114] | [98] | [99] | ||
| Safety | No cognitive deterioration; well tolerated | Dose-dependent transaminase elevations, especially with valproate | No major safety concerns reported (acute study) | Generally well tolerated; no major safety signals highlighted | Acceptable tolerability; no major safety concerns | ||
| Key Findings | Significant improvement in neurological function and QoL; reduced anxiety, depression, emotional dysregulation; stable cognition | Early efficacy (Day 6–10); median seizure reduction 37% (CBD25) & 36% (CBD50) vs. 18% placebo; higher ≥50% responder rates | CBDV modulated atypical striatal connectivity; attenuation of hyperconnectivity in language/social circuits; mechanistic relevance to ASD domains | 86% responders; 95.4% with baseline depression improved; mood/anxiety improvements independent of seizure response; QoL improved in 68% | No significant effect during blinded phase; 60.8% achieved ≥50% reduction by month 6 in OLE; sustained reductions in long-term follow-up | ||
| MainOutcomes | Neuroscore; QoL; behavioural and anxiety scales | Seizure frequency; timing of efficacy; AEs | Resting-state fMRI connectivity | Seizure response; depression (BDI-II); anxiety; QoL (QOLIE-10) | Seizure frequency | ||
| Compound/FormulationDose & Duration | Oral CBD 5–20 mg/kg/day for 6 months | Purified plant-derived CBD 25 or 50 mg/kg/day; 16 weeks | CBDV acute administration Single-dose600 mg | Highly purified CBD oil 250 mg/day, dose adjustment, escalation by 1 mL (100 mg), reaching 500 mg/day6 months, adjustment every 4 weeks | Transdermal CBD (195 mg or 390 mg)12-week RCT + OLE up to 2 years | ||
| Population | 10 patients (6F,4M); mean age 13.8 ± 9.7 years | 224 patients aged 1.1–56.8 years | 28 adult men (13 cases, 15 controls) | 44 adults | 150 participants (age 5–21 years) | ||
| Study Design | Prospective, open-label pilot | Post hoc analysis of Phase 3 RCT (double-blind, placebo-controlled) | Double-blind, placebo-controlled, repeated-measures pilot | Prospective, observational, open-label cohort | Randomised, double-blind, placebo-controlled; open-label extension | ||
| Disease | Sturge–Weber Syndrome (controlled seizures) | Tuberous Sclerosis Complex–related drug-resistant epilepsy | Autism Spectrum Disorder | Drug-resistant focal epilepsy | Drug-resistant focal epilepsy | ||
The evidence reviewed highlights the broad but heterogeneous clinical impact of cannabinoid-based interventions across refractory epilepsies and complex neurodevelopmental conditions. Across diverse disorders, these studies consistently suggest meaningful benefits in seizure burden, behavioural regulation, mood, sleep, and quality of life, often in populations with severe baseline impairment and extensive prior treatment failure. While antiseizure responses are variable and rarely curative, adjunctive cannabinoid treatment appears to exert multidimensional effects that extend beyond seizure control, potentially reflecting neuromodulatory and homeostatic mechanisms. Overall, the findings support cautious optimism regarding clinical utility in highly refractory populations.
3.2. Movement, Neurodegenerative and Sleep-Related Disorders
Movement, neurodegenerative, and sleep-related disorders share pathophysiological features that are directly relevant to the pharmacological mechanisms of drugs currently under investigation, particularly those modulating neurotransmission, neuroinflammation, and neural network stability. Dysregulation of excitatory-inhibitory balance, alterations in basal ganglia and cortico-thalamic circuits, chronic neuroinflammatory processes, and impaired synaptic plasticity are common across these conditions and constitute key therapeutic targets. Drugs under study aim to restore network homeostasis, reduce maladaptive neuroinflammatory signalling, and modulate systems involved in motor control, cognition, and sleep-wake regulation. As such, these disorders provide a biologically plausible framework for evaluating treatments that exert broad neuromodulator effects rather than targeting a single symptom domain or disease entity. Table 2 provides a structured overview of study design, patient populations, cannabinoid formulations, and key efficacy and safety findings across the included trials.
Table 2: Cannabinoids in Movement, Neurodegenerative, Psychiatric, and Sleep Disorders.
| Ref. | [ref. 115] | [ref. 106] | [ref. 116] | [ref. 105] | [ref. 117] | [ref. 118] | |||
|---|---|---|---|---|---|---|---|---|---|
| Safety | Well tolerated; no intervention-attributable serious Adverse Effects | Sub-milligram dosing; no major safety concerns reported | Generally well tolerated; uncontrolled design limits inference | Increased drowsiness vs. placebo | Mild Adverse Effects (somnolence, nausea); overall favourable tolerability | No major safety concerns reported | |||
| Key Findings | No substantial benefit for agitation; demonstrated feasibility in the frail elderly population | Significant MMSE advantage vs. placebo; 64% maintained/improved vs. 33% placebo; relative cognitive stabilisation | Reduced agitation, irritability, apathy, sleep disturbance; decreased caregiver distress; heterogeneous cognitive effects | No significant efficacy differences vs. placebo; subjective improvements in relaxation, communication, sleep in subset | No significant symptom or cognitive change; plasma THC increased more in the placebo group | CBD reduced anxiety and cognitive impairment in the nonsexual trauma subgroup; no effect in the sexual trauma subgroup | |||
| MainOutcomes | Agitation | MMSE cognitive performance | NPI-Q; CMAI; MMSE | Spasticity; caregiver-reported outcomes | Symptom severity; cognition | Subjective anxiety; cognitive impairment | |||
| Compound/FormulationDose & Duration | Nabiximols (THC:CBD 1:1 oromucosal spray)8 weeks (4-week titration + 4-week treatment) | Balanced THC–CBD oral extract (THC 0.350 mg + CBD 0.245 mg daily)26 weeks | THC-dominant extract (Bedrocan®; ~22% THC, 0.5% CBD)Twice daily for 12 weeks | Full-spectrum cannabis oil (CBD:THC 10:1)6-week double-blind phase + 6-week open-label extension phase | CBD 600 mg/day28 days | Single oral CBD 300 mgAcute administration prior to trauma recall | |||
| Population | 29 nursing home residents (moderate–severe cases) | 29 patients aged 60–80 years | 30 patients aged 65–90 years | 53 patients aged 5–25 years | 31 clinically stable individuals (≤5 years diagnosis) | 33 adults | |||
| Study Design | Randomised, double-blind, placebo-controlled feasibility trial | Phase II randomised, double-blind, placebo-controlled trial | Retrospective observational case series | Prospective, double-blind, randomised, placebo-controlled trial | Randomised, double-blind, placebo-controlled add-on trial | Randomised, double-blind, placebo-controlled experimental study | |||
| Disease | Alzheimer’s disease–related dementia (agitation) | Alzheimer’s disease–associated dementia | Alzheimers disease | Severe spastic cerebral palsy (Gross Motor Function Classification System IV–V) | Psychotic disorders (recent onset, cannabis users) | Post-traumatic Stress Disorder | |||
| Ref. | [119] | [120] | [121] | [107] | [109] | [111] | [108] | ||
| Safety | Well tolerated | Acute administration; no major safety issues described | Well tolerated; no serious Adverse Effects | Short-term use well tolerated | Well tolerated; no cognitive impairment | Well tolerated | No major safety concerns reported | ||
| Key Findings | Reduced recall-induced cognitive impairment; effect persisted at 1 week; limited anxiolytic effect at 300 mg | Increased vmPFC activation in PTSD (suggesting partial normalisation of extinction circuitry); increased amygdala activation during renewal; no behavioural change | Mean GAD-7 reduction −7.02 vs. placebo; HAM-A −11.9; significant improvements in anxiety, depression, sleep | Significant ISI reduction; ↓ sleep onset latency; ↑ total sleep time (>1 h); ↑ sleep efficiency; large effect size | No major ISI change; ↑ sleep efficiency; transient sleep quality improvement; improved well-being | No cognitive deterioration; improved calmness, alertness, energy; possible mood benefits | ~2/3 achieved clinically meaningful improvement; no overall superiority between formulations | ||
| MainOutcomes | Cognitive impairment after recall | Neural activation (vmPFC, amygdala); fear extinction | GAD-7; HAM-A; CGI; PHQ-9; PSQI | ISI; sleep diary; actigraphy | Sleep efficiency (actigraphy); sleep quality; WHO-5 | Neurocognition (CogPro); mood states | PROMIS Sleep Disturbance | ||
| Compound/FormulationDose & Durationtion | Single oral CBD 300 mgAcute + 1-week follow-up | Single administration prior to conditioning/extinction taskAcute low-dose oral THC | Nanodispersible oral CBD solution (150 mg/mL) 15 weeks | ZTL-101 sublingual cannabinoid extractTwo 2-week treatment periods | Sublingual CBD 150 mg nightly2 weeks | Sublingual CBD 150 mg nightly2 weeks | CBD isolate 15 mg; CBD + CBN ± CBC; melatonin ± cannabinoids4 weeks | ||
| Population | 33 adults | 71 participants (19 cases; 26 TEC; 26 HC) | 178 adults (89 CBD; 89 placebo) | 23 adults; mean age ~53 years | 30 adults (15 CBD; 15 placebo) | 30 adults (15 CBD; 15 placebo) | 1298 adults; mean age ~46 years(mixed population) | ||
| Study Design | Randomised, double-blind, placebo-controlled experimental study | Randomised, double-blind, placebo-controlled fMRI study | Phase III multicentre randomised, double-blind, placebo-controlled trial | Randomised, double-blind, placebo-controlled crossover (Phase 1b) | Randomised, placebo-controlled pilot (parallel) | Randomised, double-blind, placebo-controlled | Large randomised, double-blind comparative effectiveness trial | ||
| Disease | Post-traumatic Stress Disorder (memory reconsolidation focus) | Post-traumatic Stress Disorder (fear extinction paradigm) | Mild–moderate anxiety | Chronic insomnia | Primary insomnia | Primary insomnia (daytime cognition study) | Sleep disturbance | ||
Caption: ↑ increase; ↓ decrease.
The evidence across movement, neurodegenerative, psychiatric, and sleep-related disorders indicates that cannabinoid-based interventions exert broad but condition-specific effects that extend beyond a single symptom domain. In neurodegenerative and movement disorders, findings primarily support feasibility, safety, and modest benefits on agitation, cognition, spasticity, and caregiver burden, with clinically meaningful effects observed even at very low doses in vulnerable populations. In psychiatric conditions, cannabinoids—particularly CBD—demonstrate more consistent anxiolytic and trauma-related cognitive effects, with emerging evidence of network-level modulation despite variable short-term symptomatic change. In sleep disorders, the data are comparatively robust, showing reproducible improvements in subjective sleep disturbance and sleep continuity, albeit without clear formulation superiority. Collectively, these findings suggest that cannabinoids may act as neuromodulatory agents influencing network stability, emotional regulation, and sleep–wake processes.
3.3. Rare and Severe Dermatological Disorders
Rare dermatological disorders are frequently associated with chronic inflammation, impaired barrier function, persistent pain, and pruritus, leading to substantial reductions in quality of life and limited therapeutic options. In this context, cannabinoid-based interventions have attracted increasing attention due to their anti-inflammatory, analgesic, and antipruritic properties. Nevertheless, clinical evidence remains heterogeneous and is largely derived from early-phase studies, small cohorts, or exploratory clinical investigations. For clarity and comparability, the available evidence is synthesised in Table 3, highlighting both therapeutic signals and methodological considerations.
Table 3: Cannabinoids in Rare and Severe Dermatological and Oral Inflammatory Disorders.
| Ref. | [ref. 122] | [ref. 123] | [ref. 124] |
|---|---|---|---|
| Safety | Not yet reported (trial ongoing) | Well tolerated; no serious Adverse Effects | No safety concerns reported |
| Key Findings | Trial initiated to address prior anecdotal evidence; efficacy results pending; methodological advancement with quantitative endpoints | Sustained pruritus reduction; improved clinical severity scores; improved epidermal barrier function; reduced corticosteroid requirement (steroid-sparing effect) | Significant reductions in gingival index and bleeding vs. placebo; supports the feasibility of local cannabinoid delivery |
| Main Outcomes | Affective pain (validated pain scales); overall pain; pruritus; rescue analgesic use; functional neuroimaging | Pruritus severity; eczema area and severity indices; transepidermal water loss; corticosteroid use | Gingival index; bleeding on probing |
| Compound/FormulationDose & Duration | CBM oil/THC (100 mg/mL)/CBD (50 mg/mL) (Transvamix®);1 mL sublingually administration;Maximum Dose: 0.75 mL/day, 4 administrations/day;.64 days (baseline measurements, two intervention phases, washout period, follow-up) | Topical oil-in-water emulsion containing CBD and ginger extract (lipophilic CO2 extract)Topical application for 12 weeks | CBD-containing toothpaste and dental gel 56 days (adjunct to oral hygiene) |
| Population | 28 Adults (≥16) | 100 Adult and paediatric patients | 90 Adults |
| Study Design | Randomised, double-blind, placebo-controlled crossover trial (ongoing) | Clinical study | Randomised, double-blind, placebo-controlled trial |
| Disease | Epidermolysis bullosa (chronic pain) | Atopic dermatitis (mild–moderate; refractory cases included) | Periodontitis (gingival inflammation) |
Collectively, available evidence suggests that cannabinoid-based strategies may provide symptomatic benefits in rare and severe dermatological and oral inflammatory disorders, particularly when delivered via topical or local formulations. However, conclusions remain constrained by small sample sizes, heterogeneous study designs, and a reliance on subjective or short-term endpoints. Larger, well-controlled clinical trials with longer follow-up and clearly defined quantitative outcomes are required to establish the true therapeutic value of cannabinoids in these challenging dermatological contexts.
3.4. Gastrointestinal and Systemic Inflammatory Disorders
The endocannabinoid system plays a recognised role in gastrointestinal motility, visceral sensation, and immune regulation, providing a biological rationale for the investigation of cannabinoid-based therapies in chronic gastrointestinal disorders. Nevertheless, clinical evidence remains limited and heterogeneous, with outcomes frequently diverging between symptomatic relief and objective measures of disease activity. The paradoxical effects highlight the complexity of cannabinoid actions on gut sensory and motor pathways and raise important considerations regarding long-term clinical implications. A detailed summary of the controlled and observational studies evaluating cannabinoid-based interventions in this domain is presented in Table 4.
Table 4: Cannabinoids in Gastrointestinal and Systemic Inflammatory Disorders.
| Ref. | [ref. 125] | [ref. 126] |
|---|---|---|
| Safety | No major safety concerns reported in text | No major safety concerns reported; physiological slowing of gastric emptying noted |
| Key Findings | Significant reduction in Crohn’s Disease Activity Index (median 282→166; p < 0.05) and improved QoL vs. placebo; no significant changes in endoscopic scores or inflammatory biomarkers; no evidence of mucosal healing | Significant reduction in total Gastroparesis Cardinal Symptom Index (p = 0.008); improved nausea, vomiting, meal completion; increased tolerated intake volumes; paradoxical slowing of gastric emptying |
| Main Outcomes | Crohn’s Disease Activity Index; quality of life; endoscopy; CRP; faecal calprotectin | Gastroparesis Cardinal Symptom Index; gastric emptying; nutrient tolerance |
| Compound/FormulationDose & Duration | Oral CBD-rich cannabis oil (16% CBD, 4% THC)8 weeks | Pharmaceutical-grade CBD (Epidiolex®) Up to 20 mg/kg/day for 4 weeks |
| Population | 56 patients (34.5 ± 11 years), 30 men/26 women; 30 cases/26 placebo group | 44 patients (32 idiopathic, 6 diabetes mellitus type 1, 6 diabetes mellitus type 2) |
| Study Design | Randomised, double-blind, placebo-controlled trial | Randomised, double-blind, placebo-controlled trial |
| Disease | Crohn’s disease | Idiopathic or diabetic gastroparesis |
3.5. Negative or Unsuccessful Clinical Outcomes: Lessons Learned
Despite the growing number of clinical studies investigating cannabinoid-based interventions, several well-designed trials have failed to demonstrate consistent or clinically meaningful efficacy across neurodevelopmental, neurological, psychiatric, and sleep-related conditions. Importantly, these negative or inconclusive outcomes are supported by quantitative data derived from individual clinical studies rather than isolated observations, providing valuable insight into the translational limitations of cannabinoid-based therapies. To facilitate cross-study comparison, Table 5 consolidates the principal clinical endpoints, dosing strategies, and safety outcomes reported in the literature.
Table 5: Negative or Unsuccessful Clinical Outcomes with Cannabinoids.
| Ref. | [ref. 127] | [ref. 128] | [ref. 129] | [ref. 130] | [ref. 131] |
|---|---|---|---|---|---|
| Safety | No major safety concerns highlighted | Acceptable tolerability (no major safety signals reported) | Well tolerated | No serious adverse events reported; no clinically meaningful next-day cognitive or driving impairment; mild increase in subjective sedation | No major safety issues reported |
| Key Findings | Modest, inconsistent behavioural improvements; no robust statistical significance; limited power | Failed to meet primary and secondary endpoints; no clinically meaningful benefit | No significant reduction in tremor or motor improvement vs. placebo | No significant differences in 27/28 cognitive and psychomotor tests vs. placebo; small reduction in Stroop–Colour accuracy (−1.4%, p = 0.016; likely not clinically meaningful); no impairment in simulated driving performance; small increase in subjective sedation at 10 h post-dose | No significant between-group differences in objective sleep outcomes; substantial placebo response |
| Main Outcomes | Behavioural scales (caregiver- and clinician-rated) | Behavioural functioning (primary endpoint) | Tremor amplitude (accelerometry); motor performance | Next-day cognitive performance; psychomotor function; simulated driving performance; subjective drug effects; mood | Actigraphy sleep parameters; subjective sleep quality |
| Compound/FormulationDose & Duration | CBD 250 mg or 500 mg daily [weight-based]12 weeks | CBD 250 mg or 500 mg daily [weight-based]12 weeks | Single oral CBD 300 mg;Acute administration;two experimental sessions performed 2-weeks apart | Oral medicinal cannabis oil; 10 mg Δ9-THC + 200 mg CBD (1:20 THC:CBD ratio); suspended in medium-chain triglyceride (MCT);Single dose (10 mg THC + 200 mg CBD); administered 1 h before bedtime; outcomes assessed ≥9–10 h post-dose | Oral liquid dose of 30 mg CBN, 300 mg CBN |
| Population | 212 patients, mean age 9.7 years, 75% males | 240 patients; mean age 9.7 years (range 3–17 years); male (76.3%) | 19 patients; 10 males/9 females; mean 63 years of age | 20 adults; Mean age 46.1 ± 8.6 years; 16 females | 20 adults |
| Study Design | Early-phase clinical study | Phase III randomised, double-blind, placebo-controlled trial | Randomised, double-blind, placebo-controlled crossover | Pilot randomized, double-blind, placebo-controlled, crossover trial; two 24-h in-laboratory visits; 1:1 randomization; ≥7-day washout | Placebo-controlled trial |
| Disease | Fragile X syndrome | Fragile X syndrome | Essential tremor | Insomnia disorder (DSM-5 criteria) | Insomnia |
| Ref. | [132] | [133] | [134] | [135] | [136] |
| Safety | No major safety signals described | Generally well tolerated; mostly mild adverse events; no signal of worsening suicidality | Acceptable tolerability; mostly mild adverse events; no serious adverse events attributed to CBD | No major safety concerns reported | Increased cognitive adverse events |
| Key Findings | Symptom reduction in both groups; no significant between-group differences; high placebo response | Reduction in depressive symptom severity compared to placebo; improvement observed in secondary anxiety measures; effect size in the small-to-moderate range | No significant additive benefit vs. placebo; no increased risk of manic switch observed; response/remission rates not significantly different between groups | No improvement vs. placebo across motor, cognitive, or inflammatory outcomes | Worsened semantic verbal fluency; higher subjective cognitive AEs |
| Main Outcomes | Anxiety and depression scales | Change in depressive symptoms, Anxiety symptoms, sleep measures, safety/tolerability assessments | Change in depressive symptoms (Montgomery–Åsberg Depression Rating Scale); Response and remission rates; anxiety symptoms; manic symptom monitoring; safety and tolerability | Cognition; MDS-UPDRS III; affective symptoms; inflammatory markers | Cognitive measures; verbal fluency |
| Compound/FormulationDose & Duration | 300 mg oral CBD;3 and 6 months follow-up | Standard oral THC doses (5 mg);daily oral dose;4–8 weeks | Highly purified pharmaceutical-grade CBD; daily oral solution as adjunctive therapy to ongoing mood stabilizers/antipsychotics; Initiated at 150 mg/day, titrated up to 300 mg/day based on tolerability/clinical response; 8 weeks | Sublingual CBD-enriched product (101.9 mg/mL CBD, 4.8 mg/mL THC); CBD 26 mg/day, THC 1.2 mg/day; 12 weeks | Oral CBD/THC (100 mg CBD/3.3 mg THC) 16.3 (SD: 4.2) days; dosage escalating to twice/day |
| Population | 39 cases/41 placebos | n = 33;average age 40 years (range 20–66); 36% male/64% female | 30 adults | 51 participants (CBD: 27; placebo: 24) | 58 patients |
| Study Design | Randomised controlled trial | Randomised controlled trial | Randomized, double-blind, placebo-controlled, parallel-group pilot trial; adjunctive design | Randomized, double-blind, placebo-controlled, parallel-group clinical trial | Randomized, double-blind, parallel-group, placebo-controlled study |
| Disease | Anxiety and depressive disorders | Anxiety and depressive disorders | Bipolar depression (adjunctive) | Parkinson’s disease | Parkinson’s disease |
| Ref. | [137] | [110,138] | [110,138] | [139] | [140] |
| Safety | No major safety signals reported | Well tolerated | Well tolerated | ↑ systolic BP; transient delusions; hypertension; potential harm signal | Illustrates diagnostic risk rather than therapeutic effect |
| Key Findings | No superiority vs. placebo; some caregiver-reported domains favoured placebo | CBD did not reduce RBD manifestations in PD patients;No objective improvement on v-PSG;Temporary improvement in subjective sleep satisfaction | No improvement in sleep severity or objective parameters | CBD worsened delayed recall; greater increase in psychotic symptoms; 7 marked psychotic exacerbations | Cannabis use masked porphyria presentation, delaying diagnosis |
| Main Outcomes | Motor and non-motor outcomes | Transient improvement in sleep satisfaction at weeks 4 and 8 (CBD vs. placebo);No significant changes in motor, mood, anxiety, or polysomnography measures;No significant difference vs. placebo for RBD frequency;No significant difference in Clinical Global Impression—Severity and Improvement | Sleep scales; polysomnography | HVLT-R delayed recall; PANSS-P | Diagnostic course |
| Compound/FormulationDose & Duration | Oral cannabis extract (up to 2.5 mg/kg/day)2 weeks | CBD, 99.6% pure powderOral capsules (corn oil)Dose escalation (week 1: 75 mg/day; week 2: 150 mg/day; weeks 3–12: 300 mg/day)Once daily after dinner | CBD, 75–300 mg12 weeks | Single oral CBD 1000 mg prior to THC (20–60 mg inhaled) | Cannabis exposure (non-standardised) |
| Population | CBD/THC (n = 31)/placebo (n = 30) | 33 Adults(mean age ~57 years) | 18 adults (6 cases, 12 placebos) | 30 patients(18–65 years) | Single patient |
| Study Design | Randomised trial | Phase II/IIIRandomized, double-blind, placebo-controlled, parallel-group trial | Phase II/III, parallel, double-blind, placebo-controlled clinical trial | Randomised, double-blind, placebo-controlled crossover | Case report |
| Disease | Parkinson’s disease | REM Sleep Behavior Disorder in Parkinson’s Disease | Restless Legs Syndrome/Willis–Ekbom Disease in patients with Parkinson’s disease and Rapid Eye Movement sleep behavior disorder | Schizophrenia with cannabis use disorder | Porphyria (diagnostic interference case) |
Caption: ↑ increase.
Taken together, evidence from multiple independent clinical studies consistently demonstrates a lack of statistically significant superiority over placebo across several indications, alongside high placebo responsiveness, reliance on subjective endpoints, heterogeneous patient populations, and, in some cases, exposure-related adverse cognitive effects. These findings emphasise that biological plausibility and widespread use do not guarantee clinical efficacy and underscore the need for adequately powered, indication-specific trials employing robust and objective outcome measures to define the realistic therapeutic boundaries of cannabinoid-based interventions.
4. Formulation Strategies, Safety Considerations and Regulatory Aspects
4.1. Why Formulation Matters in Rare Disorders
Cannabinoids have received increasing attention for their therapeutic potential, although their pharmacokinetics are not fully understood [ref. 141]. Regardless of the route, once absorbed, cannabinoids are rapidly distributed systemically [ref. 142]. However, only 5% of CBD and THC do not bind to plasma proteins and are therefore responsible for the pharmacological effect [ref. 143]. Thus, one of the biggest determinants of the bioavailability of these compounds is related to the form of administration and, above all, to the formulation [ref. 142].
Cannabinoids have the ability to inhibit cytochrome P450 enzymes, namely CYP2C9 and CYP34A, which is why potential drug interactions may occur [ref. 142]. In fact, inhibiting these enzymes can alter the concentration of drugs in the plasma, leading to an increase in their concentration, which may result in toxicity or more adverse effects [ref. 144]. Additionally, given the inhibition of cytochrome P450 enzymes, the combined administration of THC and CBD may result in significant changes in the metabolism of these compounds [ref. 12].
The effects of cannabinoids are highly influenced by inter-individual variability, since factors such as genetics, physiology, and environment can affect therapy with these compounds. According to Wright et al. [ref. 145], there is a wide spectrum of potential changes in THC and CBD metabolism that contributes to pronounced interindividual variability in response. The results suggest that individuals classified as slow, normal, and ultra-rapid metabolizers for CYP2C9 and CYP34A may exhibit substantial differences in how they process THC and CBD, which could lead to divergent therapeutic outcomes. At the same time, changes in liver function or transporter activity can affect the pharmacokinetics of cannabinoids, influencing both efficacy and tolerability and further increasing interindividual variability [ref. 146]. One of the administration routes most influenced by interindividual variability is the oromucosal route. Factors such as differences in saliva production, absorption by the oral mucosa, and swallowing patterns significantly affect the absorption of cannabinoids, thus influencing therapeutic outcomes [ref. 147].
A study developed by Reddy et al. [ref. 148], demonstrated that pharmacokinetics can be improved by altering the formulations and their excipients. Strategies to improve the pharmacokinetics of cannabinoids focus on overcoming limitations such as low water solubility, first-pass metabolism and variability in absorption [ref. 148]. To overcome these limitations, approaches such as the use of lipid-based formulations or emulsions, which increase solubility and facilitate intestinal absorption, are important. Another approach worth mentioning is encapsulation in micro or nanoemulsions and lipid capsules, which protect the molecule and improve systemic delivery. Thus, to avoid first-pass metabolism, the use of transdermal and intranasal routes may constitute a viable alternative [ref. 149].
Another important factor for the effectiveness of cannabinoid treatments is patient adherence. Like all medications, both CBD and THC are associated with adverse effects, which can compromise adherence to and compliance with treatment. According to Pomey et al. [ref. 150], patients discontinue cannabinoid-based therapies mainly due to limited efficacy and adverse effects. In the case of rare diseases, the very heterogeneity of patients creates a significant obstacle. Furthermore, the small number of people affected makes the process even more challenging [ref. 151]. Similarly, the use of orphan drugs is also significant in the treatment of rare diseases. The choice and development of the formulation of these medications are fundamental to ensuring effective and appropriate results in the different profiles of patients with rare diseases [ref. 152].
4.2. Relevant Pharmaceutical Approaches
4.2.1. Oromucosal Sprays
Historically, oral administration of medication was the most common and accepted approach, due to its convenience and non-invasive nature. Initially intended for local effects, sublingual and buccal administration began to be used for systemic administration. This last one allows for faster action and better patient adherence, being considered a good alternative to intravenous administration [ref. 153]. The oral cavity is the first part of the gastrointestinal tract, extending from the mouth to the beginning of the pharynx, and is made up of the buccal, sublingual, gingival, palatine and labial mucosa [ref. 154]. The oral mucosa is characterised by being composed of non-keratinised tissue, which makes it more permeable and elastic [ref. 155]. Another important characteristic of this epithelium is that, although rigid, small molecules can pass through it, potentially avoiding first-pass metabolism. However, it is important to note that drug absorption may be limited due to the small contact area and the processes of swallowing and saliva production [ref. 155]. Therefore, for medications to be absorbed through the oral mucosa, they must first be dissolved in saliva, the volume of which is significantly lower in the mouth. On the other hand, high saliva concentration can lead to premature swallowing, resulting in inadequate drug release [ref. 154].
The drug must then diffuse through the mucosa itself, which is determined by lipophilicity and the degree of ionisation. To diffuse through the mucosa, drugs can permeate via both transcellular and paracellular pathways. Most lipophilic molecules diffuse via the transcellular pathway, while hydrophilic molecules permeate via the paracellular pathway [ref. 155]. In order to overcome these limitations, alternative administration methods have been developed, primarily through mucoadhesion and the use of mucoadhesive polymers.
Another strategy that has become very relevant is the use of medications with rapid disintegration of the drug and consequent almost immediate release, as is the case with sprays [ref. 154]. Oromucosal sprays are liquid formulations applied directly to the oral mucosa, allowing medications to be absorbed by the oral epithelium for local and systemic effects. Compared to conventional oral administration, they offer greater bioavailability, avoiding first-pass metabolism, and providing a faster onset of action due to direct systemic absorption. The main advantage is greater convenience for patients, especially those with swallowing difficulties, such as children, the elderly and uncooperative patients, as is the case with some patients with rare diseases [ref. 154,ref. 156].
Nabiximols are botanical preparations containing balanced amounts of THC and CBD and have been used as an oromucosal spray (Sativex®) for patients with multiple sclerosis with moderate to severe spasticity [ref. 157]. Studies have shown that nabiximols has significant efficacy in treating the symptoms of multiple sclerosis, showing that this is a consistent therapy, even as monotherapy [ref. 157]. Nabiximols have also been used in the treatment of Tourette syndrome [ref. 158]. Müller-Vahl et al. [ref. 158] carried out a study with nabiximols, where they found a greater number of responders compared to the placebo group. However, the difference was not statistically significant. Secondary analyses indicated that patients with Attention Deficit Hyperactivity Disorder (ADHD) showed a decrease in severe tics. Thus, the study showed that nabiximols may be a good approach to reduce tics in Tourette syndrome [ref. 158].
4.2.2. Transdermal/Topical: Gels and Patches
The skin is the largest organ in the body, composed of five layers, including an outer layer, the stratum corneum, which acts as a barrier against hydrophilic substances and large molecules [ref. 159]. Transdermal drug delivery systems (TDDS) and topical formulations are a promising non-invasive method for delivering active drugs across the skin barrier [ref. 160]. Typically, topical drug administration refers to the treatment of a localised area of skin, while TDDS refers to the administration of drugs through the skin and into the systemic circulation [ref. 161]. TDDS tablets are composed of several layers that facilitate the absorption of the medication. The support layer acts as an external protective barrier, shielding the system from the external environment. Next, the adhesive layer attaches the patch to the skin using a hypoallergenic adhesive that is gentle on the skin. At the core, the drug reservoir contains the active pharmaceutical ingredient, which is released at a constant rate through a membrane [ref. 159]. On the other hand, gels are systems formed by a polymer and a solvent, arranged in a three-dimensional structure in a cross-linked polymer network and have different drug delivery systems [ref. 162].
Drug penetration through the skin requires passage through both the stratum corneum and the skin’s cellular matrix. Drug penetration into the skin occurs through transcellular permeation and intercellular absorption. Transcellular permeation involves the direct absorption of drugs through individual skin cells, while intercellular absorption occurs within the extracellular matrix through the interstitial spaces between neighbouring cells. Another way drugs are absorbed through the skin is through skin appendages, such as hair follicles and sebaceous glands [ref. 161].
When developing effective drug delivery systems, several variables must be considered, namely, active pharmaceutical ingredients and skin morphology [ref. 161]. Most active pharmaceutical ingredients do not inherently meet the criteria for effective transdermal administration, so it is important to develop new strategies to improve their absorption [ref. 160]. Thus, organogels have been used in transdermal delivery systems to improve the transdermal administration of hydrophilic and hydrophobic drugs that present lipophilicity problems [ref. 159]. In recent years, several nanocarrier formulations have also been developed to improve transdermal drug delivery, including liposomes and polymeric micelles [ref. 163].
Cannabinoids are known for their medicinal properties, especially as anti-inflammatories. Its topical application as anti-inflammatory compounds has been at the forefront of research in the last decade, also receiving increasing attention in the cosmetics field, as it can help alleviate skin problems due to its topical anti-inflammatory effect [ref. 163]. However, unlike transdermal delivery systems, such as cannabinoid patches, this route does not involve systemic absorption [ref. 164]. Thus, transdermal delivery systems have gained great relevance not only because of the possibility of systemic absorption, but also because they help to bypass first-pass metabolism, increasing user adherence [ref. 165]. Studies have shown that emerging transdermal systems, such as transdermal patches, can significantly increase CBD absorption and therefore help in the treatment of skin conditions such as dermatitis and even epidermolysis bullosa, due to their anti-inflammatory action [ref. 166]. An experimental topical cream, INM-755, was tested for the treatment of epidermolysis bullosa [ref. 167]. In phase II studies, this topical formulation demonstrated good tolerability and safety, without negatively interfering with the healing process. Therefore, the absence of serious adverse effects on such fragile skin and the good acceptance by participants indicate that this type of formulation is suitable for repeated cutaneous application [ref. 167]. Another study with the transdermal gel ZYN2-CL-017, which contains CBD, investigated long-term efficacy and safety in populations with fragile X syndrome [ref. 128]. The main results of the study show a favourable safety profile and revealed clinically significant improvements [ref. 128]. Furthermore, these studies support the idea that transdermal formulations can be effective vehicles for the local and systemic administration of cannabinoids in rare diseases.
Despite some promising results, these systems still have inherent limitations, such as skin permeability, which can be overcome with permeability enhancers like ethanol and oleic acid. Furthermore, a preclinical study with guinea pigs demonstrated that the addition of transcutol HP, a permeation enhancer, increased plasma CBD concentration by 3.7 times when added to a topical CBD gel [ref. 168].
Physical permeation enhancers, such as microneedles, can solve the problem of cannabinoid permeation, but studies in this area are still few [ref. 164].
4.2.3. Nanocarriers
As previously described, cannabinoids have lower solubility and are easily subjected to oxidation and degradation reactions due to the action of light and temperature. These limitations make them interesting candidates for nanotechnology-based formulations [ref. 169]. The technology of encapsulating cannabinoids in nanocarriers has become a good bet to protect the compounds from degradation, increasing their stability [ref. 148]. In this regard, both lipid-based carriers and polymeric carriers have been investigated regarding their mode of action.
Polymeric nanocarriers can be produced in capsules and spherical shapes, allowing for better release, while lipid nanocarriers have been shown to favour targeted delivery [ref. 170]. Among lipid-based nanocarriers, nanoemulsions showed increased CBD absorption, demonstrating that bioavailability can increase up to 1.65 times, significantly reducing the time to reach peak plasma concentration. However, due to high production costs and instability, Self-Nanoemulsifying Drug Delivery Systems (SNEDDS) emerged, which consist of self-emulsifying systems that spontaneously form nanoemulsions in the gastrointestinal tract [ref. 171]. Evidence shows that these not only increase the solubility and stability of cannabinoids, but also their bioavailability. However, most studies consist of small clinical trials, so larger clinical trials are still needed [ref. 148]. Additionally, despite being a promising alternative, SNEDDS do not avoid the first-pass mechanism [ref. 171].
Liposomes, on the other hand, are spherical vesicles made up of phospholipids and cholesterol, in which one or more layers of phospholipids surround an aqueous core. Although these systems are widely studied, they have low encapsulation efficiency for cannabinoids. Even so, studies in dogs with osteoarthritis showed CBD bioavailability 17 times greater than that of free CBD, demonstrating that encapsulation increases CBD activity, even at reduced doses [ref. 169]. On the other hand, there are also polymeric micelles, which consist of amphipathic nanoparticles with a hydrophobic core and a hydrophilic layer, used as reservoirs for lipophilic drugs, such as cannabinoids. Studies have shown that polymeric nanoparticles allow for greater bioavailability. Studies with Polylactic-co-Glycolic Acid (PLGA) nanoparticles loaded with CBD showed rapid initial release and high encapsulation efficiency [ref. 171]. Villate et al. [ref. 172] developed a study with PLGA nanocapsules loaded with full-spectrum cannabis extract, demonstrating that these formulations protect cannabinoids from gastric degradation and allow their controlled release in the intestine, increasing the local concentration of cannabinoids. Thus, the study demonstrated that, with biocompatible polymers, nanotechnology can be promising in the treatment of gastrointestinal diseases [ref. 172]. However, most clinical evidence remains in vitro or in vivo models, so clinical validation is still limited [ref. 171].
4.3. Safety Profile Across Rare Conditions
Recreational use of cannabinoids is associated with very worrying side effects, namely psychosis, schizophrenia and cannabis use disorder, especially in adolescents [ref. 173]. The adverse effects associated with the use of cannabinoids for medicinal purposes are linked to an increased risk of short-term side effects but are rarely associated with serious effects. In fact, products containing medicinal THC are often associated with changes in perception and thinking, as well as dizziness and sedation, particularly in the elderly. However, CBD does not cause intoxication and presents fewer safety concerns than THC. Still, potential side effects, such as liver toxicity and drug interactions, as well as inadequate regulatory oversight of CBD products, may constitute legitimate concerns [ref. 5].
The main adverse effects of prolonged use of cannabinoids include gastrointestinal side effects, namely vomiting, cardiovascular effects such as tachycardia and orthostatic hypotension, and, mainly at the psychiatric level, an increased risk of depression and suicidal ideation [ref. 142]. Furthermore, CBD has been reported to cause liver abnormalities, diarrhoea, fatigue and drowsiness in some individuals [ref. 141]. Another problem that has been reported is the potential for interaction with other medications. According to a recent study developed by Nachnani et al. [ref. 174], cannabinoids can significantly alter the action of many medications, especially those with a narrow therapeutic index. The study reports that cannabinoids interact with warfarin, increasing its clotting time [ref. 174]. Other medications, such as tricyclic antidepressants and anticonvulsants like valproate, have also shown significant interactions with CBD [ref. 174]. Another study showed that CBD is the main culprit behind interactions with other medications. CBD primarily inhibits CYP2C19, CYP2C9, CYP3A and CYP1A2; therefore, interactions occur mainly during first-pass metabolism [ref. 175]. These results indicate that CBD increases exposure to the drug by inhibiting its initial clearance [ref. 175]. In fact, the medications with the highest risk of interaction with CBD are those that are metabolised by the enzymes mentioned above. Thus, antidepressants, opioids, benzodiazepines, antihypertensives and anticonvulsants have significant interactions because they are extensively metabolised by cytochrome P450 family enzymes [ref. 176]. Epidiolex® is approved for refractory epilepsies, including rare diseases such as Dravet and Lennox–Gastaut [ref. 177]. Despite its favourable safety profile, it can cause pharmacokinetic changes and interactions with other anticonvulsants. Concomitant administration with clobazam increases levels of its metabolite, increasing the risk of sedation [ref. 177]. Changes in liver enzyme levels can also occur with valproate. Minor interactions were observed with topiramate and levetiracetam; therefore, dose adjustments may be necessary [ref. 177].
Another legitimate concern when using medicinal cannabis is its administration to children. In fact, most studies on cannabinoids are conducted in adult animal models; therefore, research on long-term adverse effects in children and adolescents is still limited. As a result, there is some uncertainty about how cannabinoids affect a developing brain [ref. 178]. Children are very vulnerable to cannabinoid treatments because their pharmacokinetics vary greatly due to the immaturity of their physiological system. Consequently, oral absorption is less effective, and distribution is affected by the low percentage of fat. Metabolism is also affected by liver enzymes, which are still developing. Therefore, children are equally susceptible to drug interactions. In the specific case of concomitant use with antiepileptic drugs, it should be noted, once again, that CBD significantly increases the concentration of clobazam. It is also important to report the interaction of antidepressants such as sertraline with CBD in children, which can be equally dangerous [ref. 179].
Other vulnerable groups, particularly transplant patients whose immune systems are suppressed, have also been a cause for concern. According to a review on the use of CBD in post-organ transplant care, the use of cannabis has been shown to be a good supportive therapy for the relief of chronic pain [ref. 180]. However, this group is equally susceptible to the use of cannabinoids, as they can interfere with immunosuppressant medications. Studies report that CBD may interfere with the concentration of tacrolimus and other immunosuppressants, increasing their blood concentration and potentially resulting in increased toxic effects [ref. 142,ref. 181,ref. 182,ref. 183,ref. 184]. Thus, the use of cannabinoids should also be rigorously monitored in immunosuppressed patients [ref. 180].
4.4. Regulatory Considerations
With the expansion of the regulatory framework and the market for cannabis-derived products, the variety of cannabinoid products has increased significantly for both recreational and medicinal use, including in the treatment of diseases for which this use is not indicated. Thus, when these products are used without solid regulatory support regarding safety, patients may be exposed to uncertain risks [ref. 185].
The FDA acknowledges that there is growing interest in the therapeutic potential of cannabis in treating diseases, but so far has not approved any marketing authorisation applications for its use. The only approved medicines are cannabis-based, namely Epidiolex® and three synthetic cannabis-based medicines, such as dronabinol (Marinol® and Syndros®) and nabilone (Cesamet®) [ref. 83]. With regard to Europe, only dronabinol, nabilone and, in particular, nabiximols have been authorised by the EMA in European member countries. Nevertheless, the regulation of compounded preparations is a national responsibility, leading some Member States to independently authorise the prescription and sale of cannabinoid products [ref. 186].
Thus, medicinal cannabis and related products have been available in the Member States of the European Union as individual prescriptions without regular marketing authorisations [ref. 187]. Therefore, there is no specific framework for cannabis-based medicines in Europe. Depending on their composition, they may be considered medicinal plant-based products, which can be authorised for the market through registration for traditional use. In the US, despite federal regulations, state laws vary, allowing, in some cases, the medicinal use of cannabis without FDA approval [ref. 188]. However, there are very few approved cannabis-based medicines, so their use beyond the indicated options is considered off-label [ref. 188].
The FDA acknowledges that there are cannabinoid-based drugs being used for unofficial purposes, highlighting the importance of approved drugs undergoing rigorous evaluations, unlike unapproved products, which can cause unpredictable and serious adverse effects, since there are no clinical trials to prove their safety [ref. 83]. Thus, only standardised pharmaceutical cannabinoids are approved by the EMA and FDA, such as Epidiolex®, dronabinol, nabilone and nabiximols (Sativex®), while the use of other medicinal cannabis products remains outside the regulatory scope, without quality assurance and, especially, safety [ref. 187,ref. 188].
Epidiolex® is approved by the EMA and the FDA for the treatment of seizures associated with Lennox–Gastaut syndrome, Dravet syndrome or tuberous sclerosis complex in patients 1 year of age or older, especially with orphan drug designation: a drug used for the diagnosis and treatment of rare diseases [ref. 189,ref. 190].
Generally, orphan drugs are supported by incentives such as tax breaks and market exclusivity to encourage their development, despite serving a small patient population [ref. 191]. According to Orphanet, a major database of orphan drugs, they are intended to treat diseases so rare that the market is reluctant to develop them under normal market conditions, given their expensive and time-consuming development, which makes rare diseases unattractive to the pharmaceutical industry [ref. 152,ref. 192]. It is therefore understandable that these medicines are subject to certain limitations, such as high research and development costs, small patient populations involved and the regulatory and market dynamics that govern the industry [ref. 191]. To overcome market limitations, in particular, the Orphan Drugs Act (1983) [ref. 152] in the United States granted seven years of market exclusivity with tax exemptions to encourage the development of orphan drugs. Meanwhile, in Europe, the Orphan Medicinal Products Regulation (2000/2001) grants ten years of exclusivity with the same fee exemptions. It should be noted that both the FDA and the EMA assist in clinical trials for small populations [ref. 152].
Rare diseases also involve very small patient populations, which makes recruitment difficult and often renders traditional clinical trials unfeasible. To overcome this limitation, innovative methods, such as master protocols, have been used, but even so, they require ethical considerations and informed consent, which makes the process more time-consuming, limits the number of volunteers and, consequently, the existence of more robust studies [ref. 191]. The approval of orphan drugs, as often happens in smaller studies, can lead to the approval of therapies with uncertain safety and efficacy profiles. Therefore, more robust studies are important to detect risks that may not be evident in smaller studies [ref. 193,ref. 194]. Furthermore, post-marketing pharmacovigilance is essential to identify safety signals that do not appear in clinical trials or that are specific to subgroups, namely, in patients with rare diseases [ref. 195].
5. Conclusions
Cannabinoid-based therapies are increasingly recognised as pharmacologically plausible interventions beyond their currently approved indications. The evidence reviewed in this article highlights a growing, yet heterogeneous, body of clinical data supporting the potential role of cannabinoids in less-common, rare, and complex disorders, particularly in conditions characterised by high symptom burden and limited therapeutic alternatives. Across neurological, neurodevelopmental, psychiatric, dermatological, gastrointestinal, and sleep-related disorders, cannabinoids, most notably CBD, have demonstrated multidimensional effects extending beyond single symptom domains, including modulation of seizure burden, behaviour, mood, sleep, pain, and quality of life. Thus, cannabinoids may play an important role in the development of innovative therapies, particularly in the treatment of less-common diseases that often lack effective therapeutic options.
Importantly, the reviewed studies illustrate that clinical responses to cannabinoids are highly variable and context dependent. While some patient populations experience clinically meaningful benefits, others derive limited or no measurable advantage, as exemplified by well-conducted trials reporting neutral or negative outcomes. This highlights the need for more targeted studies in specific populations and clinical conditions. Recent studies suggest that specific effects in the brain region, which affect behavior, may be closely related to cannabinoid compounds, leading to the belief that this class of compounds presents a relevant (poly)pharmacology. Other findings underscore the necessity of avoiding overly generalised conclusions regarding cannabinoid efficacy and instead adopting a nuanced, indication-specific interpretation of available evidence. The inclusion of negative and inconclusive trials is particularly instructive, highlighting methodological challenges, placebo effects, and the limitations of current outcome measures. Therefore, the development of larger and better-controlled clinical trials is essential.
Pharmaceutical formulation emerges as a critical determinant of therapeutic success. Poor aqueous solubility, variable bioavailability, extensive first-pass metabolism, and inter-individual pharmacokinetic variability remain major obstacles to consistent clinical outcomes. Advances in drug delivery systems, including oromucosal, transdermal, and nanocarrier-based formulations, offer promising strategies to mitigate these limitations and may partly explain discrepancies observed across clinical studies. Optimising formulation and route of administration is therefore not merely a technical consideration but a central component of effective cannabinoid-based therapy, especially in vulnerable and rare disease populations.
From a safety perspective, cannabinoids generally exhibit acceptable tolerability profiles when appropriately dosed and monitored. Nevertheless, clinically relevant drug–drug interactions, particularly involving cytochrome P450 enzymes, and dose-dependent adverse effects reinforce the need for careful patient selection, titration, and longitudinal surveillance. Regulatory heterogeneity across jurisdictions further complicates clinical translation, reflecting ongoing uncertainties regarding risk–benefit balance and evidentiary thresholds.
References
- X. Zhai, P.R. Sarkar, K.P. Hill. Therapeutic Use of Cannabis and Cannabinoids: Benefits and Risks. Pol. Arch. Intern. Med., 2025. [DOI | PubMed]
- J. Renard, R. Gabrys, N. Sanger. Clearing the Smoke on Cannabis and Cannabinoids: Medical Use of Cannabis and Cannabinoids, 2024
- R.G. Pertwee. The Pharmacology of Cannabinoid Receptors and Their Ligands: An Overview. Int. J. Obes., 2006. [DOI]
- L. De Petrocellis, V. Di Marzo. An Introduction to the Endocannabinoid System: From the Early to the Latest Concepts. Best Pract. Res. Clin. Endocrinol. Metab., 2009. [DOI | PubMed]
- E. Hoch, N.D. Volkow, C.M. Friemel, V. Lorenzetti, T.P. Freeman, W. Hall. Cannabis, Cannabinoids and Health: A Review of Evidence on Risks and Medical Benefits. Eur. Arch. Psychiatry Clin. Neurosci., 2025. [DOI | PubMed]
- INFARMED Deliberação n.o 11/CD/2019
- R. Chou, A.Y. Ahmed, B.J. Morasco, C. Bougatsos, T. Dana, R. Fu, T. Gilbreath. Living Systematic Review on Cannabis and Other Plant-Based Treatments for Chronic Pain: 2023 Update, 2023
- G. Mick, P. Douek. Clinical Benefits and Safety of Medical Cannabis Products: A Narrative Review on Natural Extracts. Pain Ther., 2024. [DOI | PubMed]
- R. Bhuller, W.K. Schlage, J. Hoeng. Review of the Current Ongoing Clinical Trials Exploring the Possible Anti-Anxiety Effects of Cannabidiol. J. Cannabis Res., 2024. [DOI | PubMed]
- J. Parovincaka, J.V. Szijj, A. Serracino-Inglott, L.M. Azzopardi. Cannabis for Medicinal Use in Patients with Rare Diseases. Transl. Sci. Rare Dis., 2023. [DOI]
- C. Pagano, G. Navarra, L. Coppola, G. Avilia, M. Bifulco, C. Laezza. Cannabinoids: Therapeutic Use in Clinical Practice. Int. J. Mol. Sci., 2022. [DOI | PubMed]
- M. Kaszewska, K. Woźniczka, K. Sztormowska-Achranowicz, A. Mosińska, V. Trojan, P. Schreiber, N. Balog, T. Bączek, A. Roszkowska. Perspectives of Cannabis-Based Medicines in a View of Pharmacokinetic Studies of Δ9-THC and CBD in Humans. Biomed. Pharmacother., 2025. [DOI | PubMed]
- O. Zendulka, G. Dovrtělová, K. Nosková, M. Turjap, A. Šulcová, L. Hanuš. Cannabinoids and Cytochrome P450 Interactions. Curr. Drug Metab., 2016. [DOI | PubMed]
- S.A. Bonini, M. Premoli, S. Tambaro, A. Kumar, G. Maccarinelli, M. Memo, A. Mastinu. Cannabis sativa: A Comprehensive Ethnopharmacological Review of a Medicinal Plant with a Long History. J. Ethnopharmacol., 2018. [DOI | PubMed]
- M. Protti, V. Brighenti, M.R. Battaglia, L. Anceschi, F. Pellati, L. Mercolini. Cannabinoids from Cannabis sativa L.: A New Tool Based on HPLC–DAD–MS/MS for a Rational Use in Medicinal Chemistry. ACS Med. Chem. Lett., 2019. [DOI | PubMed]
- J. Gonçalves, T. Rosado, S. Soares, A.Y. Simão, D. Caramelo, Â. Luís, N. Fernández, M. Barroso, E. Gallardo, A.P. Duarte. Cannabis and Its Secondary Metabolites: Their Use as Therapeutic Drugs, Toxicological Aspects, and Analytical Determination. Medicines, 2019. [DOI | PubMed]
- G. Appendino, G. Chianese, O. Taglialatela-Scafati. Cannabinoids: Occurrence and Medicinal Chemistry. Curr. Med. Chem., 2011. [DOI | PubMed]
- M.A. ElSohly, D. Slade. Chemical Constituents of Marijuana: The Complex Mixture of Natural Cannabinoids. Life Sci., 2005. [DOI | PubMed]
- B. De Backer, B. Debrus, P. Lebrun, L. Theunis, N. Dubois, L. Decock, A. Verstraete, P. Hubert, C. Charlier. Innovative Development and Validation of an HPLC/DAD Method for the Qualitative and Quantitative Determination of Major Cannabinoids in Cannabis Plant Material. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci., 2009. [DOI]
- L.O. Hanuš, S.M. Meyer, E. Muñoz, O. Taglialatela-Scafati, G. Appendino. Phytocannabinoids: A Unified Critical Inventory. Nat. Prod. Rep., 2016. [DOI | PubMed]
- A.A. Izzo, F. Borrelli, R. Capasso, V. Di Marzo, R. Mechoulam. Non-Psychotropic Plant Cannabinoids: New Therapeutic Opportunities from an Ancient Herb. Trends Pharmacol. Sci., 2009. [DOI | PubMed]
- R.G. Pertwee. The Diverse CB1 and CB2 Receptor Pharmacology of Three Plant Cannabinoids: Delta9-Tetrahydrocannabinol, Cannabidiol and Delta9-Tetrahydrocannabivarin. Br. J. Pharmacol., 2008. [DOI | PubMed]
- F. Grotenhermen. Pharmacokinetics and Pharmacodynamics of Cannabinoids. Clin. Pharmacokinet., 2003. [DOI | PubMed]
- R.G. Pertwee. Pharmacology of Cannabinoid CB1 and CB2 Receptors. Pharmacol. Ther., 1997. [DOI | PubMed]
- K.S. Grant, R. Petroff, N. Isoherranen, N. Stella, T.M. Burbacher. Cannabis Use during Pregnancy: Pharmacokinetics and Effects on Child Development. Pharmacol. Ther., 2017. [DOI | PubMed]
- K. Solymosi, A. Kofalvi. Cannabis: A Treasure Trove or Pandora’s Box?. Mini Rev. Med. Chem., 2017. [DOI | PubMed]
- R.G. dos Santos, J.E.C. Hallak, J.A.S. Crippa. Neuropharmacological Effects of the Main Phytocannabinoids: A Narrative Review. Adv. Exp. Med. Biol., 2021. [DOI | PubMed]
- B.H. McCarberg, R.L. Barkin. The Future of Cannabinoids as Analgesic Agents: A Pharmacologic, Pharmacokinetic, and Pharmacodynamic Overview. Am. J. Ther., 2007. [DOI | PubMed]
- R.B. Laprairie, A.M. Bagher, M.E.M. Kelly, E.M. Denovan-Wright. Cannabidiol Is a Negative Allosteric Modulator of the Cannabinoid CB1 Receptor. Br. J. Pharmacol., 2015. [DOI | PubMed]
- F. Pellati, V. Borgonetti, V. Brighenti, M. Biagi, S. Benvenuti, L. Corsi. Cannabis sativa L. and Nonpsychoactive Cannabinoids: Their Chemistry and Role against Oxidative Stress, Inflammation, and Cancer. Biomed Res. Int., 2018. [DOI | PubMed]
- A. Manduca, V. Buzzelli, A. Rava, A. Feo, E. Carbone, S. Schiavi, B. Peruzzi, V. D’Oria, M. Pezzullo, A. Pasquadibisceglie. Cannabidiol and Positive Effects on Object Recognition Memory in an in Vivo Model of Fragile X Syndrome: Obligatory Role of Hippocampal GPR55 Receptors. Pharmacol. Res., 2024. [DOI | PubMed]
- V. Micale, M. Di Bartolomeo, S. Di Martino, T. Stark, B. Dell’Osso, F. Drago, C. D’Addario. Are the Epigenetic Changes Predictive of Therapeutic Efficacy for Psychiatric Disorders? A Translational Approach towards Novel Drug Targets. Pharmacol. Ther., 2023. [DOI | PubMed]
- A. Thomas, G.L. Baillie, A.M. Phillips, R.K. Razdan, R.A. Ross, R.G. Pertwee. Cannabidiol Displays Unexpectedly High Potency as an Antagonist of CB1 and CB2 Receptor Agonists in Vitro. Br. J. Pharmacol., 2007. [DOI | PubMed]
- T. Bisogno, L. Hanuš, L. De Petrocellis, S. Tchilibon, D.E. Ponde, I. Brandi, A.S. Moriello, J.B. Davis, R. Mechoulam, V. Di Marzo. Molecular Targets for Cannabidiol and Its Synthetic Analogues: Effect on Vanilloid VR1 Receptors and on the Cellular Uptake and Enzymatic Hydrolysis of Anandamide. Br. J. Pharmacol., 2001. [DOI | PubMed]
- V.D. Marzo, L.D. Petrocellis. Endocannabinoids as Regulators of Transient Receptor Potential (TRP) Channels: A Further Opportunity to Develop New Endocannabinoid-Based Therapeutic Drugs. Curr. Med. Chem., 2010. [DOI | PubMed]
- P.M. Zygmunt, J. Petersson, D.A. Andersson, H.H. Chuang, M. Sørgård, V. Di Marzo, D. Julius, E.D. Högestätt. Vanilloid Receptors on Sensory Nerves Mediate the Vasodilator Action of Anandamide. Nature, 1999. [DOI | PubMed]
- A.W. Zuardi. Cannabidiol: From an Inactive Cannabinoid to a Drug with Wide Spectrum of Action. Braz. J. Psychiatry, 2008. [DOI | PubMed]
- E.B. Russo, A. Burnett, B. Hall, K.K. Parker. Agonistic Properties of Cannabidiol at 5-HT1a Receptors. Neurochem. Res., 2005. [DOI | PubMed]
- A.C. Campos, F.S. Guimarães. Involvement of 5HT1A Receptors in the Anxiolytic-like Effects of Cannabidiol Injected into the Dorsolateral Periaqueductal Gray of Rats. Psychopharmacology, 2008. [DOI | PubMed]
- A. Ligresti, A.S. Moriello, K. Starowicz, I. Matias, S. Pisanti, L. De Petrocellis, C. Laezza, G. Portella, M. Bifulco, V. Di Marzo. Antitumor Activity of Plant Cannabinoids with Emphasis on the Effect of Cannabidiol on Human Breast Carcinoma. J. Pharmacol. Exp. Ther., 2006. [DOI | PubMed]
- P. Massi, A. Vaccani, S. Bianchessi, B. Costa, P. Macchi, D. Parolaro. The Non-Psychoactive Cannabidiol Triggers Caspase Activation and Oxidative Stress in Human Glioma Cells. Cell. Mol. Life Sci., 2006. [DOI | PubMed]
- N.M. Kogan, M. Schlesinger, M. Peters, G. Marincheva, R. Beeri, R. Mechoulam. A Cannabinoid Anticancer Quinone, HU-331, Is More Potent and Less Cardiotoxic than Doxorubicin: A Comparative in Vivo Study. J. Pharmacol. Exp. Ther., 2007. [DOI | PubMed]
- S.E. O’Sullivan. An Update on PPAR Activation by Cannabinoids. Br. J. Pharmacol., 2016. [DOI | PubMed]
- L. De Petrocellis, V. Vellani, A. Schiano-Moriello, P. Marini, P.C. Magherini, P. Orlando, V. Di Marzo. Plant-Derived Cannabinoids Modulate the Activity of Transient Receptor Potential Channels of Ankyrin Type-1 and Melastatin Type-8. J. Pharmacol. Exp. Ther., 2008. [DOI | PubMed]
- J.M. McPartland, M. Duncan, V. Di Marzo, R.G. Pertwee. Are Cannabidiol and Δ(9) -Tetrahydrocannabivarin Negative Modulators of the Endocannabinoid System? A Systematic Review. Br. J. Pharmacol., 2015. [DOI | PubMed]
- G. Riedel, P. Fadda, S. McKillop-Smith, R.G. Pertwee, B. Platt, L. Robinson. Synthetic and Plant-Derived Cannabinoid Receptor Antagonists Show Hypophagic Properties in Fasted and Non-Fasted Mice. Br. J. Pharmacol., 2009. [DOI | PubMed]
- A.J. Hill, S.E. Weston, N.A. Jones, I. Smith, S.A. Bevan, E.M. Williamson, G.J. Stephens, C.M. Williams, B.J. Whalley. Δ9-Tetrahydrocannabivarin Suppresses in Vitro Epileptiform and in Vivo Seizure Activity in Adult Rats. Epilepsia, 2010. [DOI | PubMed]
- C.J. Lucas, P. Galettis, J. Schneider. The Pharmacokinetics and the Pharmacodynamics of Cannabinoids. Br. J. Clin. Pharmacol., 2018. [DOI | PubMed]
- M.A. Huestis. Pharmacokinetics and Metabolism of the Plant Cannabinoids, Delta9-Tetrahydrocannabinol, Cannabidiol and Cannabinol. Handb. Exp. Pharmacol., 2005. [DOI]
- M.A. Huestis, J.E. Henningfield, E.J. Cone. Blood Cannabinoids. I. Absorption of THC and Formation of 11-OH-THC and THCCOOH during and after Smoking Marijuana. J. Anal. Toxicol., 1992. [DOI | PubMed]
- A. Ohlsson, J.-E. Lindgren, S. Andersson, S. Agurell, H. Gillespie, L.E. Hollister. Single-Dose Kinetics of Deuterium-Labelled Cannabidiol in Man after Smoking and Intravenous Administration. Biomed. Environ. Mass Spectrom., 1986. [DOI | PubMed]
- S.W. Toennes, J.G. Ramaekers, E.L. Theunissen, M.R. Moeller, G.F. Kauert. Comparison of Cannabinoid Pharmacokinetic Properties in Occasional and Heavy Users Smoking a Marijuana or Placebo Joint. J. Anal. Toxicol., 2008. [DOI | PubMed]
- N. Solowij, S.J. Broyd, H.H. van Hell, A. Hazekamp. A Protocol for the Delivery of Cannabidiol (CBD) and Combined CBD and ∆9-Tetrahydrocannabinol (THC) by Vaporisation. BMC Pharmacol. Toxicol., 2014. [DOI | PubMed]
- J.H. Martin, J. Schneider, C.J. Lucas, P. Galettis. Exogenous Cannabinoid Efficacy: Merely a Pharmacokinetic Interaction?. Clin. Pharmacokinet., 2018. [DOI | PubMed]
- J.P. Goullé, E. Saussereau, C. Lacroix. Pharmacocinétique Du Delta-9-Tétrahydrocannabinol (THC). Ann. Pharm. Fr., 2008. [DOI | PubMed]
- S. Agurell, S. Carlsson, J.E. Lindgren, A. Ohlsson, H. Gillespie, L. Hollister. Interactions of Delta 1-Tetrahydrocannabinol with Cannabinol and Cannabidiol Following Oral Administration in Man. Assay of Cannabinol and Cannabidiol by Mass Fragmentography. Experientia, 1981. [DOI | PubMed]
- M. Eichler, L. Spinedi, S. Unfer-Grauwiler, M. Bodmer, C. Surber, M. Luedi, J. Drewe. Heat Exposure of Cannabis sativa Extracts Affects the Pharmacokinetic and Metabolic Profile in Healthy Male Subjects. Planta Med., 2012. [DOI | PubMed]
- S.A. Millar, R.F. Maguire, A.S. Yates, S.E. O’sullivan. Towards Better Delivery of Cannabidiol (CBD). Pharmaceuticals, 2020. [DOI | PubMed]
- A.I.A. Ahmed, G.A.H. Van Den Elsen, A. Colbers, C. Kramers, D.M. Burger, M.A. Van Der Marck, M.G.M. Olde Rikkert. Safety, Pharmacodynamics, and Pharmacokinetics of Multiple Oral Doses of Delta-9-Tetrahydrocannabinol in Older Persons with Dementia. Psychopharmacology, 2015. [DOI | PubMed]
- E.W. Schwilke, D.M. Schwope, E.L. Karschner, R.H. Lowe, W.D. Darwin, D.L. Kelly, R.S. Goodwin, D.A. Gorelick, M.A. Huestis. Delta9-Tetrahydrocannabinol (THC), 11-Hydroxy-THC, and 11-nor-9-Carboxy-THC Plasma Pharmacokinetics during and after Continuous High-Dose Oral THC. Clin. Chem., 2009. [DOI | PubMed]
- E.R. Garrett, C.A. Hunt. Physicochemical Properties, Solubility, and Protein Binding of Δ9-tetrahydrocannabinol. J. Pharm. Sci., 1974. [DOI | PubMed]
- P.V.N. Challapalli, A.L. Stinchcomb. In Vitro Experiment Optimization for Measuring Tetrahydrocannabinol Skin Permeation. Int. J. Pharm., 2002. [DOI | PubMed]
- A.L. Stinchcomb, S. Valiveti, D.C. Hammell, D.R. Ramsey. Human Skin Permeation of Delta8-Tetrahydrocannabinol, Cannabidiol and Cannabinol. J. Pharm. Pharmacol., 2004. [DOI | PubMed]
- M. Lodzki, B. Godin, L. Rakou, R. Mechoulam, R. Gallily, E. Touitou. Cannabidiol—Transdermal Delivery and Anti-Inflammatory Effect in a Murine Model. J. Control. Release, 2003. [DOI | PubMed]
- S. Valiveti, D.C. Hammell, D.C. Earles, A.L. Stinchcomb. In Vitro/in Vivo Correlation Studies for Transdermal Δ 8-THC Development. J. Pharm. Sci., 2004. [DOI | PubMed]
- C.J. Lucas, P. Galettis, S. Song, N. Solowij, S.E. Reuter, J. Schneider, J.H. Martin. Cannabinoid Disposition After Human Intraperitoneal Use: An Insight Into Intraperitoneal Pharmacokinetic Properties in Metastatic Cancer. Clin. Ther., 2018. [DOI | PubMed]
- M.A. Huestis. Human Cannabinoid Pharmacokinetics. Chem. Biodivers., 2007. [DOI | PubMed]
- T.E. Gaston, D. Friedman. Pharmacology of Cannabinoids in the Treatment of Epilepsy. Epilepsy Behav., 2017. [DOI | PubMed]
- R.J. Dinis-Oliveira. Metabolomics of Δ9-Tetrahydrocannabinol: Implications in Toxicity. Drug Metab. Rev., 2016. [DOI | PubMed]
- T. Heiskanen, S. Mätzke, S. Haakana, M. Gergov, E. Vuori, E. Kalso. Transdermal Fentanyl in Cachectic Cancer Patients. Pain, 2009. [DOI | PubMed]
- P. Consroe, J. Laguna, J. Allender, S. Snider, L. Stern, R. Sandyk, K. Kennedy, K. Schram. Controlled Clinical Trial of Cannabidiol in Huntington’s Disease. Pharmacol. Biochem. Behav., 1991. [DOI | PubMed]
- J.D. Brown, A.G. Winterstein, J.D. Brown, A.G. Winterstein. Potential Adverse Drug Events and Drug–Drug Interactions with Medical and Consumer Cannabidiol (CBD) Use. J. Clin. Med., 2019. [DOI | PubMed]
- O. Devinsky, E. Marsh, D. Friedman. Cannabidiol in Patients with Treatment-Resistant Epilepsy—Authors’ Reply. Lancet Neurol., 2016. [DOI | PubMed]
- J. Atsmon, D. Heffetz, L. Deutsch, F. Deutsch, H. Sacks. Single-Dose Pharmacokinetics of Oral Cannabidiol Following Administration of PTL101: A New Formulation Based on Gelatin Matrix Pellets Technology. Clin. Pharmacol. Drug Dev., 2018. [DOI | PubMed]
- W.D.M. Paton, R.G. Pertwee. Effect of Cannabis and Certain of Its Constituents on Pentobarbitone Sleeping Time and Phenazone Metabolism. Br. J. Pharmacol., 1972. [DOI | PubMed]
- H.K. Borys, R. Karler. Cannabidiol and Δ9-Tetrahydrocannabinol Metabolism: In Vitro Comparison of Mouse and Rat Liver Crude Microsome Preparations. Biochem. Pharmacol., 1979. [DOI | PubMed]
- T. Nadulski, F. Pragst, G. Weinberg, P. Roser, M. Schnelle, E.M. Fronk, A.M. Stadelmann. Randomized, Double-Blind, Placebo-Controlled Study about the Effects of Cannabidiol (CBD) on the Pharmacokinetics of Delta9-Tetrahydrocannabinol (THC) after Oral Application of THC Verses Standardized Cannabis Extract. Ther. Drug Monit., 2005. [DOI | PubMed]
- H.H. Maurer, C. Sauer, D.S. Theobald. Toxicokinetics of Drugs of Abuse: Current Knowledge of the Isoenzymes Involved in the Human Metabolism of Tetrahydrocannabinol, Cocaine, Heroin, Morphine, and Codeine. Ther. Drug Monit., 2006. [DOI | PubMed]
- B. Costa, A.E. Trovato, F. Comelli, G. Giagnoni, M. Colleoni. The Non-Psychoactive Cannabis Constituent Cannabidiol Is an Orally Effective Therapeutic Agent in Rat Chronic Inflammatory and Neuropathic Pain. Eur. J. Pharmacol., 2007. [DOI | PubMed]
- The Single Convention on Narcotic Drugs
- R. Abuhasira, L. Shbiro, Y. Landschaft. Medical Use of Cannabis and Cannabinoids Containing Products—Regulations in Europe and North America. Eur. J. Intern. Med., 2018. [DOI | PubMed]
- FDA Regulation of Cannabis and Cannabis-Derived Products, Including Cannabidiol (CBD)|FDA
- FDA and Cannabis: Research and Drug Approval Process|FDA
- New Report Describes Growing Complexity and Change in Cannabis Laws in Europe|www.euda.europa.eu
- V. Kiran Vemuri, A. Makriyannis. Medicinal Chemistry of Cannabinoids. Clin. Pharmacol. Ther., 2015. [DOI | PubMed]
- V. Voicu, F.M. Brehar, C. Toader, R.A. Covache-Busuioc, A.D. Corlatescu, A. Bordeianu, H.P. Costin, B.G. Bratu, L.A. Glavan, A.V. Ciurea. Cannabinoids in Medicine: A Multifaceted Exploration of Types, Therapeutic Applications, and Emerging Opportunities in Neurodegenerative Diseases and Cancer Therapy. Biomolecules, 2023. [DOI | PubMed]
- D.S. Hasin. US Epidemiology of Cannabis Use and Associated Problems. Neuropsychopharmacology, 2018. [DOI | PubMed]
- 88. New York State Office of Cannabis Management|Office of Cannabis Management Available online: https://cannabis.ny.gov/(accessed on 17 December 2025)
- FDA CESAMETTM (Nabilone) Capsules. 2006
- FDA SYNDROS (Dronabinol) Oral Solution, CX
- S.B. Klieger, A. Gutman, L. Allen, R.L. Pacula, J.K. Ibrahim, S. Burris. Mapping Medical Marijuana: State Laws Regulating Patients, Product Safety, Supply Chains and Dispensaries, 2017. Addiction, 2017. [DOI | PubMed]
- Florida Department of State Constitutional Initiatives
- J. Ablin, P.A. Ste-Marie, M. Schäfer, W. Häuser, M.A. Fitzcharles. Medical Use of Cannabis Products. Schmerz, 2016. [DOI | PubMed]
- Canada Ministry of Justice Access to Cannabis for Medical Purposes Regulations. 2018
- Government of Canada Understanding the Access to Cannabis for Medical Purposes Regulations—Canada
- Government of Canada Information for Health Care Professionals: Cannabis (Marihuana, Marijuana) and the Cannabinoids
- E.N. Hurley, C.J. Ellaway, A.M. Johnson, L. Truong, R. Gordon, P. Galettis, J.H. Martin, J.A. Lawson. Efficacy and Safety of Cannabidivarin Treatment of Epilepsy in Girls with Rett Syndrome: A Phase 1 Clinical Trial. Epilepsia, 2022. [DOI | PubMed]
- J. Lamonarca, I. Mintz, L. Bayarres, S. Kochen, S. Oddo. Psychiatric Comorbidities before and after Cannabidiol Treatment in Adult Patients with Drug Resistant Focal Epilepsy. Epilepsy Behav., 2024. [DOI | PubMed]
- T.J. O’Brien, S.F. Berkovic, J.A. French, J.A. Messenheimer, T.B. Sebree, M.O. Bonn-Miller, D.L. Gutterman. Adjunctive Transdermal Cannabidiol for Adults with Focal Epilepsy: A Randomized Clinical Trial. JAMA Netw. Open, 2022. [DOI | PubMed]
- J.Y. Wu, H.R. Cock, O. Devinsky, C. Joshi, I. Miller, C.M. Roberts, R. Sanchez-Carpintero, D. Checketts, F. Sahebkar. Time to Onset of Cannabidiol Treatment Effect and Resolution of Adverse Events in Tuberous Sclerosis Complex: Post Hoc Analysis of Randomized Controlled Phase 3 Trial GWPCARE6. Epilepsia, 2022. [DOI | PubMed]
- P.S. Fortini, J.J. Toibaro, R.H. Caraballo. Purified Cannabidiol Leads to Improvement of Severe Treatment-Resistant Behavioral Symptoms in Children with Autism Spectrum Disorder. Pharmacol. Biochem. Behav., 2025. [DOI | PubMed]
- A. Aran, M. Harel, H. Cassuto, L. Polyansky, A. Schnapp, N. Wattad, D. Shmueli, D. Golan, F.X. Castellanos. Cannabinoid Treatment for Autism: A Proof-of-Concept Randomized Trial. Mol. Autism, 2021. [DOI | PubMed]
- L.F. Smegal, P. Vedmurthy, M. Ryan, M. Eagen, N.W. Andrejow, K. Sweeney, T.G. Reidy, S.E. Yeom, D.D. Lin, S.J. Suskauer. Cannabidiol Treatment for Neurological, Cognitive, and Psychiatric Symptoms in Sturge-Weber Syndrome. Pediatr. Neurol., 2023. [DOI | PubMed]
- E.H. Kaplan, E.A. Offermann, J.W. Sievers, A.M. Comi. Cannabidiol Treatment for Refractory Seizures in Sturge-Weber Syndrome. Pediatr. Neurol., 2017. [DOI | PubMed]
- M. Stefanović, D. Osredkar, Z. Rener-Primec, J. Peterlin, T. Laptoš, D. Neubauer. Plant-Derived Cannabinoids for Treatment of Spasticity in Children and Adolescents with Severe Cerebral Palsy: Double-Blind, Placebo-Controlled Trial. Eur. J. Paediatr. Neurol., 2025. [DOI | PubMed]
- R.D.M. Cury, T. da Silva, F. Cezar-dos-Santos, Y.R.C. Fakih, K.A.R. Narvaez, M.C. Gouvea, C. Espínola, C.F. Ferreira, W.A.C. de Castro, F.A. Pamplona. A Randomized Clinical Trial of Low-Dose Cannabis Extract in Alzheimer’s Disease. J. Alzheimer’s Dis., 2025. [DOI | PubMed]
- J.H. Walsh, K.J. Maddison, T. Rankin, K. Murray, N. McArdle, M.J. Ree, D.R. Hillman, P.R. Eastwood. Treating Insomnia Symptoms with Medicinal Cannabis: A Randomized, Crossover Trial of the Efficacy of a Cannabinoid Medicine Compared with Placebo. Sleep, 2021. [DOI | PubMed]
- J.L. Saleska, C. Bryant, A. Kolobaric, C.R. D’Adamo, C.S. Colwell, D. Loewy, J. Chen, E.K. Pauli. The Safety and Comparative Effectiveness of Non-Psychoactive Cannabinoid Formulations for the Improvement of Sleep: A Double-Blinded, Randomized Controlled Trial. J. Am. Nutr. Assoc., 2024. [DOI | PubMed]
- A.J. Narayan, L.A. Downey, S. Rose, L. Di Natale, A.C. Hayley. Cannabidiol for Moderate-Severe Insomnia: A Randomized Controlled Pilot Trial of 150 Mg of Nightly Dosing. J. Clin. Sleep Med., 2024. [DOI | PubMed]
- C.M.O. de Almeida, M.M.C. Brito, N.B. Bosaipo, A.V. Pimentel, V. Tumas, A.W. Zuardi, J.A.S. Crippa, J.E.C. Hallak, A.L. Eckeli. Cannabidiol for Rapid Eye Movement Sleep Behavior Disorder. Mov. Disord., 2021. [DOI | PubMed]
- A.J. Narayan, A.C. Hayley, S. Rose, L. Di Natale, L.A. Downey. The Effect of Nightly Use of 150 Mg Cannabidiol on Daytime Neurocognitive Performance in Primary Insomnia: A Randomized Controlled Pilot Trial. Psychopharmacology, 2025. [DOI | PubMed]
- M. Siani-Rose, R. McKee, S. Cox, B. Goldstein, D. Abrams, M. Taylor, I. Kurek. The Potential of Salivary Lipid-Based Cannabis-Responsive Biomarkers to Evaluate Medical Cannabis Treatment in Children with Autism Spectrum Disorder. Cannabis Cannabinoid Res., 2023. [DOI | PubMed]
- G.B. Dell’Isola, F. Antonella, P. Francesco, M. Mario, D.M. Cordelli, P. Piero, P. Pasquale, F. Alessandro, F.F. Operto, E. Maurizio. CDKL5 Deficiency-Related Neurodevelopmental Disorders: A Multi-Center Cohort Study in Italy. J. Neurol., 2024. [DOI | PubMed]
- C.M. Pretzsch, D.L. Floris, B. Voinescu, M. Elsahib, M.A. Mendez, R. Wichers, L. Ajram, G. Ivin, M. Heasman, E. Pretzsch. Modulation of Striatal Functional Connectivity Differences in Adults with and without Autism Spectrum Disorder in a Single-Dose Randomized Trial of Cannabidivarin. Mol. Autism, 2021. [DOI | PubMed]
- C.P. Albertyn, T.W. Guu, P. Chu, B. Creese, A. Young, L. Velayudhan, S. Bhattacharyya, H. Jafari, S. Kaur, P. Kandangwa. Sativex (Nabiximols) for the Treatment of Agitation & Aggression in Alzheimer’s Dementia in UK Nursing Homes: A Randomised, Double-Blind, Placebo-Controlled Feasibility Trial. Age Ageing, 2025. [DOI | PubMed]
- B. Palmieri, M. Vadalà. Oral Thc: Cbd Cannabis Extract in Main Symptoms of Alzheimer Disease: Agitation and Weight Loss. Clin. Ter., 2023. [DOI | PubMed]
- R. van Boxel, S.S. Gangadin, H. Janssen, S. van der Steur, L.J.C. van der Vinne, L. Dortants, T.A.D. Pelgrim, L.W.R. Draisma, R. Tuura, P. van der Meer. The Impact of Cannabidiol Treatment on Resting State Functional Connectivity, Prefrontal Metabolite Levels and Reward Processing in Recent-Onset Patients with a Psychotic Disorder. J. Psychiatr. Res., 2023. [DOI | PubMed]
- L.M. Bolsoni, J.A.S. Crippa, J.E.C. Hallak, F.S. Guimaraes, A.W. Zuardi. The Anxiolytic Effect of Cannabidiol Depends on the Nature of the Trauma When Patients with Post-Traumatic Stress Disorder Recall Their Trigger Event. Braz. J. Psychiatry, 2022. [DOI | PubMed]
- L.M. Bolsoni, J.A.S. Crippa, J.E.C. Hallak, F.S. Guimarães, A.W. Zuardi. Effects of Cannabidiol on Symptoms Induced by the Recall of Traumatic Events in Patients with Posttraumatic Stress Disorder. Psychopharmacology, 2022. [DOI | PubMed]
- N.L. Zabik, C.A. Rabinak, C.A. Peters, A. Iadipaolo. Cannabinoid Modulation of Corticolimbic Activation during Extinction Learning and Fear Renewal in Adults with Posttraumatic Stress Disorder. Neurobiol. Learn. Mem., 2023. [DOI | PubMed]
- P.R. Gundugurti, N. Banda, S.S.R. Yadlapalli, A. Narala, R. Thatikonda, C. Kocherlakota, K.S. Kothapalli. Evaluation of the Efficacy, Safety, and Pharmacokinetics of Nanodispersible Cannabidiol Oral Solution (150 mg/ML) versus Placebo in Mild to Moderate Anxiety Subjects: A Double Blind Multicenter Randomized Clinical Trial. Asian J. Psychiatr., 2024. [DOI | PubMed]
- N.H.B. Schräder, J.C. Duipmans, R.J. Renken, P. Sörös, K.M. Vermeulen, M.C. Bolling, A.P. Wolff. The C4EB Study—Transvamix (10% THC/5% CBD) to Treat Chronic Pain in Epidermolysis Bullosa: A Protocol for an Explorative Randomized, Placebo Controlled, and Double Blind Intervention Crossover Study. PLoS ONE, 2022. [DOI | PubMed]
- L. Herrmann, S. Andreev, R. Ziegler, C. Neubauer, K. Moritz, N. Maehler, H. Steindl, S. Daehnhardt-Pfeiffer, C. Abels. Long-Term Progressive Improvement of Atopic Dermatitis by an Herbal Emollient Plus Combination in a 12-Week Clinical Trial. Acta Derm. Venereol., 2025. [DOI | PubMed]
- P. Jirasek, A. Jusku, J. Frankova, M. Urbankova, D. Diabelko, F. Ruzicka, B. Papouskova, K. Chytilova, J. Vrba, J. Havlasek. Phytocannabinoids and Gingival Inflammation: Preclinical Findings and a Placebo-Controlled Double-Blind Randomized Clinical Trial with Cannabidiol. J. Periodontal Res., 2024. [DOI | PubMed]
- T. Naftali, L. Bar-Lev Schleider, S. Almog, D. Meiri, F.M. Konikoff. Oral CBD-Rich Cannabis Induces Clinical but Not Endoscopic Response in Patients with Crohn’s Disease, a Randomised Controlled Trial. J. Crohns Colitis, 2021. [DOI | PubMed]
- T. Zheng, J. BouSaba, A. Taylor, S. Dilmaghani, I. Busciglio, P. Carlson, M. Torres, M. Ryks, D. Burton, W.S. Harmsen. A Randomized, Controlled Trial of Efficacy and Safety of Cannabidiol in Idiopathic and Diabetic Gastroparesis. Clin. Gastroenterol. Hepatol., 2023. [DOI | PubMed]
- E. Berry-Kravis, R. Hagerman, D. Budimirovic, C. Erickson, H. Heussler, N. Tartaglia, J. Cohen, F. Tassone, T. Dobbins, E. Merikle. A Randomized, Controlled Trial of ZYN002 Cannabidiol Transdermal Gel in Children and Adolescents with Fragile X Syndrome (CONNECT-FX). J. Neurodev. Disord., 2022. [DOI | PubMed]
- E. Berry-Kravis, R. Hagerman, J. Cohen, D. Budimirovic, C.B. Buchanan, N. Silove, N. Tich, A. Thibodeau, T. Dobbins, T. Sebree. Long-Term Safety and Tolerability of Transdermal Cannabidiol Gel in Children and Adolescents with Fragile X Syndrome (ZYN2-CL-017): An Interim Analysis of an Ongoing Open-Label Extension Study. J. Neurodev. Disord., 2025. [DOI | PubMed]
- S. Santos de Alencar, J.A.S. Crippa, M.C.M. Brito, Â.V. Pimentel, J.E. Cecilio Hallak, V. Tumas. A Single Oral Dose of Cannabidiol Did Not Reduce Upper Limb Tremor in Patients with Essential Tremor. Parkinsonism Relat. Disord., 2021. [DOI | PubMed]
- A. Suraev, D. McCartney, N.S. Marshall, C. Irwin, R. Vandrey, R.R. Grunstein, A.L. D’Rozario, C. Gordon, D. Bartlett, C.M. Hoyos. Evaluating Possible ‘next Day’ Impairment in Insomnia Patients Administered an Oral Medicinal Cannabis Product by Night: A Pilot Randomized Controlled Trial. Psychopharmacology, 2024. [DOI | PubMed]
- I. Lavender, D. McCartney, N. Marshall, A. Suraev, C. Irwin, A.L. D’Rozario, C.J. Gordon, B. Saini, R.R. Grunstein, B. Yee. Cannabinol (CBN; 30 and 300 Mg) Effects on Sleep and next-Day Function in Insomnia Disorder (“CUPID” Study): Protocol for a Randomised, Double-Blind, Placebo-Controlled, Cross-over, Three-Arm, Proof-of-Concept Trial. BMJ Open, 2023. [DOI]
- C.M. Kwee, J.M. Baas, F.E. van der Flier, L. Groenink, P. Duits, M. Eikelenboom, D.C. van der Veen, M. Moerbeek, N.M. Batelaan, A.J. van Balkom. Cannabidiol Enhancement of Exposure Therapy in Treatment Refractory Patients with Social Anxiety Disorder and Panic Disorder with Agoraphobia: A Randomised Controlled Trial. Eur. Neuropsychopharmacol., 2022. [DOI | PubMed]
- D. Wolinsky, R.E. Mayhugh, R. Surujnarain, J. Thrul, R. Vandrey, J.C. Strickland. Acute and Chronic Effects of Medicinal Cannabis Use on Anxiety and Depression in a Prospective Cohort of Patients New to Cannabis. J. Affect. Disord., 2025. [DOI | PubMed]
- J.V. Pinto, J.A.S. Crippa, K.M. Ceresér, M.F. Vianna-Sulzbach, É.d.M. Silveira Júnior, G. Santana da Rosa, M.G. Testa da Silva, G.H. Hizo, L. Simão Medeiros, C.E. Santana de Oliveira. Cannabidiol as an Adjunctive Treatment for Acute Bipolar Depression: A Pilot Study: Le Cannabidiol Comme Traitement d’appoint de La Dépression Bipolaire Aiguë: Une Étude Pilote. Can. J. Psychiatry, 2024. [DOI | PubMed]
- W. Mitarnun, A. Kanjanarangsichai, P. Junlaor, L. Kongngern, W. Mitarnun, W. Pangwong, P. Nonghan. Cannabidiol and Cognitive Functions/Inflammatory Markers in Parkinson’s Disease: A Double-Blind Randomized Controlled Trial at Buriram Hospital (CBD-PD-BRH Trial). Parkinsonism Relat. Disord., 2025. [DOI | PubMed]
- C.H. Domen, S. Sillau, Y. Liu, M. Adkins, S. Rajkovic, J. Bainbridge, C. Sempio, J. Klawitter, M.A. Leehey. Cognitive Safety Data from a Randomized, Double-Blind, Parallel-Group, Placebo-Controlled Phase IIb Study of the Effects of a Cannabidiol and Δ9-Tetrahydrocannabinol Drug on Parkinson’s Disease-Related Motor Symptoms. Mov. Disord., 2023. [DOI | PubMed]
- Y. Liu, J. Bainbridge, S. Sillau, S. Rajkovic, M. Adkins, C.H. Domen, J.A. Thompson, T. Seawalt, J. Klawitter, C. Sempio. Short-Term Cannabidiol with Δ-9-Tetrahydrocannabinol in Parkinson’s Disease: A Randomized Trial. Mov. Disord., 2024. [DOI | PubMed]
- C.M.O. De Almeida, M.M.C. Brito, N.B. Bosaipo, A.V. Pimentel, M.A. Sobreira-Neto, V. Tumas, A.W. Zuardi, J.A. De Souza Crippa, J.E.C. Hallak, A.L. Eckeli. The Effect of Cannabidiol for Restless Legs Syndrome/Willis-Ekbom Disease in Parkinson’s Disease Patients with REM Sleep Behavior Disorder: A Post Hoc Exploratory Analysis of Phase 2/3 Clinical Trial. Cannabis Cannabinoid Res., 2023. [DOI | PubMed]
- E. Chesney, D. Oliver, A. Sarma, A.D. Lamper, I. Slimani, M. Lloyd, A.M. Dickens, M. Welds, M. Kråkström, I. Gasparini-Andre. Does Cannabidiol Reduce the Adverse Effects of Cannabis in Schizophrenia? A Randomised, Double-Blind, Cross-over Trial. Neuropsychopharmacology, 2025. [DOI | PubMed]
- B. Gertz, M. Mullen, T. Pesavento. An Adolescent Female with Disordered Eating and Cannabis Use Found to Have Acute Intermittent Porphyria. Case Rep. Psychiatry, 2025. [DOI | PubMed]
- Q. Zhang, P.W. Melchert, J.S. Markowitz. Pharmacokinetic Variability of Oral Cannabidiol and Its Major Metabolites after Short-Term High-Dose Exposure in Healthy Subjects. Med. Cannabis Cannabinoids, 2024. [DOI | PubMed]
- I.M. Braun, K. Bohlke, D.I. Abrams, H. Anderson, L.G. Balneaves, G. Bar-Sela, D.W. Bowles, P.R. Chai, A. Damani, A. Gupta. Cannabis and Cannabinoids in Adults with Cancer: ASCO Guideline. J. Clin. Oncol., 2024. [DOI | PubMed]
- N.M. Naya, J. Kelly, G. Corna, M. Golino, A.H. Polizio, A. Abbate, S. Toldo, E. Mezzaroma, N.M. Naya, J. Kelly. An Overview of Cannabidiol as a Multifunctional Drug: Pharmacokinetics and Cellular Effects. Molecules, 2024. [DOI | PubMed]
- J. Lee, J.L. Beers, R.M. Geffert, K.D. Jackson. A Review of CYP-Mediated Drug Interactions: Mechanisms and In Vitro Drug-Drug Interaction Assessment. Biomolecules, 2024. [DOI | PubMed]
- J.A. Wright, L. Huang, B.E. Katamesh, S. Yadav, A. Singla, A. Vincent. Hypothesized Pharmacogenomic and Medication Influences on Tetrahydrocannabinol and Cannabidiol Metabolism in a Cohort of Unselected Oral Cannabis Users. J. Cannabis Res., 2025. [DOI | PubMed]
- M. Shevchuk, O.-P. Hasiuk. Specific Features of Cannabidiol Metabolism and Excretion during Long-Term Consumption of Cannabis. Int. J. Minor Fruits Med. Aromat. Plants, 2025. [DOI]
- I.K. Storgaard, R.L. Nielsen, M.B. Houlind, O. Bornæs, L.W.S. Christensen, A.L. Andersen, H.G. Juul-Larsen, L.M. Jørgensen, T. Breindahl, B.N. Jawad. Population Pharmacokinetic Modelling Revealed Large Variability in Oromucosal Absorption of Δ9-Tetrahydrocannabinol in Older Patients with Poor Appetite. Br. J. Clin. Pharmacol., 2025. [DOI | PubMed]
- T.S. Reddy, R. Zomer, N. Mantri. Nanoformulations as a Strategy to Overcome the Delivery Limitations of Cannabinoids. Phytother. Res., 2023. [DOI | PubMed]
- S.E. O’Sullivan, S.S. Jensen, A.R. Kolli, G.N. Nikolajsen, H.Z. Bruun, J. Hoeng. Strategies to Improve Cannabidiol Bioavailability and Drug Delivery. Pharmaceuticals, 2024. [DOI | PubMed]
- M.P. Pomey, D. Jutras-Aswad, J. Paquette, K. Saadi, M. Taguemout, D.L. Ikene, N. Arbour, A. Zertal, N. Fréjeau, D. Morin. Perceptions and Engagement of Patients with Chronic Conditions on the Use of Medical Cannabis: A Scoping Review. Eur. J. Med. Res., 2024. [DOI | PubMed]
- M.A. Ahmed, R. Krishna, N. Rayad, S. Albusaysi, A. Mitra, E. Shang, Y.Y. Hon, B. AbuAsal, R. Bakhaidar, Y.M. Roman. Getting the Dose Right in Drug Development for Rare Diseases: Barriers and Enablers. Clin. Pharmacol. Ther., 2024. [DOI | PubMed]
- A. Debnath, R. Mazumder, A. Mazumder, P.K. Tyagi, R.K. Singh. Challenges and Progress of Orphan Drug Development for Rare Diseases. Curr. Pharm. Biotechnol., 2025. [DOI]
- S. Bahraminejad, H. Almoazen, S. Bahraminejad, H. Almoazen. Sublingual and Buccal Delivery: A Historical and Scientific Prescriptive. Pharmaceutics, 2025. [DOI | PubMed]
- I. Bácskay, P. Arany, P. Fehér, L. Józsa, G. Vasvári, D. Nemes, Á. Pető, D. Kósa, Á. Haimhoffer, Z. Ujhelyi. Bioavailability Enhancement and Formulation Technologies of Oral Mucosal Dosage Forms: A Review. Pharmaceutics, 2025. [DOI | PubMed]
- V.V. Nair, P. Cabrera, C. Ramírez-Lecaros, M.O. Jara, D.J. Brayden, J.O. Morales. Buccal Delivery of Small Molecules and Biologics: Of Mucoadhesive Polymers, Films, and Nanoparticles—An Update. Int. J. Pharm., 2023. [DOI | PubMed]
- A. Ahmad, J. Akhtar, M. Ahmad, R. Wasim, Badruddeen, M.I. Khan. Drug Delivery Approaches for Buccal and Sublingual Administration. Drug Res., 2025. [DOI]
- R. Sacco, G.C. Riccitelli, G. Disanto, J. Bogousslavsky, A. Cavelti, D. Czell, C.P. Kamm, U. Kliesch, S.P. Ramseier, C. Gobbi. Effectiveness, Safety and Patients’ Satisfaction of Nabiximols (Sativex®) on Multiple Sclerosis Spasticity and Related Symptoms in a Swiss Multicenter Study. J. Clin. Med., 2024. [DOI | PubMed]
- K.R. Müller-Vahl, A. Pisarenko, N. Szejko, M. Haas, C. Fremer, E. Jakubovski, R. Musil, A. Münchau, I. Neuner, D. Huys. CANNA-TICS: Efficacy and Safety of Oral Treatment with Nabiximols in Adults with Chronic Tic Disorders—Results of a Prospective, Multicenter, Randomized, Double-Blind, Placebo Controlled, Phase IIIb Superiority Study. Psychiatry Res., 2023. [DOI | PubMed]
- D. Sivadasan, O.A. Madkhali, D. Sivadasan, O.A. Madkhali. The Design Features, Quality by Design Approach, Characterization, Therapeutic Applications, and Clinical Considerations of Transdermal Drug Delivery Systems—A Comprehensive Review. Pharmaceuticals, 2024. [DOI | PubMed]
- E.O. Bakhrushina, M.M. Shumkova, Y.V. Avdonina, A.A. Ananian, M. Babazadeh, G. Pouya, V.V. Grikh, I.M. Zubareva, S.I. Kosenkova, I.I. Krasnyuk. Transdermal Drug Delivery Systems: Methods for Enhancing Skin Permeability and Their Evaluation. Pharmaceutics, 2025. [DOI | PubMed]
- S. Brito, M. Baek, B.H. Bin. Skin Structure, Physiology, and Pathology in Topical and Transdermal Drug Delivery. Pharmaceutics, 2024. [DOI | PubMed]
- M. Chelu, A.M. Musuc, M. Chelu, A.M. Musuc. Polymer Gels: Classification and Recent Developments in Biomedical Applications. Gels, 2023. [DOI | PubMed]
- P.C. Chu, M.H. Liao, M.G. Liu, C.Z. Li, P.S. Lai. Key Transdermal Patch Using Cannabidiol-Loaded Nanocarriers with Better Pharmacokinetics in Vivo. Int. J. Nanomedicine, 2024. [DOI | PubMed]
- C.A. Zamarripa, H.E. Tilton, S. Lin, E.J. Cone, R.E. Winecker, R.R. Flegel, D. Kuntz, M. Beals, M. Jacques, M. Clark. Pharmacokinetics and Pharmacodynamics of Five Distinct Commercially Available Hemp-Derived Topical Cannabidiol Products. J. Anal. Toxicol., 2024. [DOI | PubMed]
- H. Mahmoudinoodezh, S.R. Telukutla, S.K. Bhangu, A. Bachari, F. Cavalieri, N. Mantri. The Transdermal Delivery of Therapeutic Cannabinoids. Pharmaceutics, 2022. [DOI | PubMed]
- K. Marciniak, A. Jurczuk, M. Olszanska, A. Rafałowicz. The Role of Cannabinoids in the Treatment of Skin Diseases: A Review of Mechanisms of Action and Clinical Evidence. J. Educ. Health Sport, 2025. [DOI]
- InMed Pharmaceuticals INM-755 Topical Cream for Epidermolysis Bullosa (EB)
- K.S. Paudel, D.C. Hammell, R.U. Agu, S. Valiveti, A.L. Stinchcomb. Cannabidiol Bioavailability after Nasal and Transdermal Application: Effect of Permeation Enhancers. Drug Dev. Ind. Pharm., 2010. [DOI | PubMed]
- E.R. Lazzarotto Rebelatto, G.S. Rauber, T. Caon. An Update of Nano-Based Drug Delivery Systems for Cannabinoids: Biopharmaceutical Aspects & Therapeutic Applications. Int. J. Pharm., 2023. [DOI | PubMed]
- E. Assadpour, A. Rezaei, S.S. Das, B.V.K. Rao, S.K. Singh, M.S. Kharazmi, N.K. Jha, S.K. Jha, M.A. Prieto, S.M. Jafari. Cannabidiol-Loaded Nanocarriers and Their Therapeutic Applications. Pharmaceuticals, 2023. [DOI | PubMed]
- M. Paczkowska-Walendowska, P. Trzaskoma, A. Dziopa, A. Moeini, M. Soczawa, Z. Krasiński, J. Cielecka-Piontek, M. Paczkowska-Walendowska, P. Trzaskoma, A. Dziopa. Innovative Strategies to Enhance the Bioavailability of Cannabidiol: Nanotechnology and Advanced Delivery Systems. Pharmaceuticals, 2025. [DOI | PubMed]
- A. Villate, G.P. Barreto, M.S. Nicolás, O. Aizpurua-Olaizola, M. Olivares, A. Usobiaga. Development, Characterization and In Vitro Gastrointestinal Release of PLGA Nanoparticles Loaded with Full-Spectrum Cannabis Extracts. AAPS PharmSciTech, 2024. [DOI | PubMed]
- T. Rittiphairoj, L. Leslie, J.P. Oberste, T.W. Yim, G. Tung, L. Bero, P. Riggs, K. Hutchison, J. Samet, T. Li. Stronger Weed, Higher Risk? Potent THC Linked to Psychosis and Addiction. ScienceDaily, 2025. [DOI]
- R. Nachnani, A. Knehans, J.D. Neighbors, P.T. Kocis, T. Lee, K. Tegeler, T. Trite, W.M. Raup-Konsavage, K.E. Vrana. Systematic Review of Drug-Drug Interactions of Delta-9-Tetrahydrocannabinol, Cannabidiol, and Cannabis. Front. Pharmacol., 2024. [DOI | PubMed]
- S. Bansal, C.A. Zamarripa, T.R. Spindle, E.M. Weerts, K.E. Thummel, R. Vandrey, M.F. Paine, J.D. Unadkat. Evaluation of Cytochrome P450-Mediated Cannabinoid-Drug Interactions in Healthy Adult Participants. Clin. Pharmacol. Ther., 2023. [DOI | PubMed]
- H. Geneau, M. Kovasala, G. Brown, S. Holmes, O. Hime, M. McNally, M. McFayden, K. Brewer, G.K. Jones. Prevalence of Cannabidiol (CBD) Use Among Patients Taking Medications with Known Drug-Drug Interactions: A Cross-Sectional Analysis. J. Clin. Med., 2025. [DOI | PubMed]
- T.E. Gaston, E.M. Bebin, G.R. Cutter, L. Grayson, J.P. Szaflarski. Final Analysis of Potential Drug-Drug Interactions between Highly Purified Cannabidiol and Anti-Seizure Medications in an Open-Label Expanded Access Program. Epilepsia Open, 2023. [DOI | PubMed]
- K.Y. Tseng, H.M. Molla. Cannabinoid CB1 Receptor-Sensitive Neurodevelopmental Processes and Trajectories. Mol. Psychiatry, 2025. [DOI | PubMed]
- L. Qian, J.L. Beers, K.D. Jackson, Z. Zhou. CBD and THC in Special Populations: Pharmacokinetics and Drug-Drug Interactions. Pharmaceutics, 2024. [DOI | PubMed]
- S. Koyama, J. Etkins, J. Jun, M. Miller, G.C. So, D.L. Gisch, M.T. Eadon. Utilization of Cannabidiol in Post-Organ-Transplant Care. Int. J. Mol. Sci., 2025. [DOI | PubMed]
- A.D. Leino, C. Emoto, T. Fukuda, M. Privitera, A.A. Vinks, R.R. Alloway. Evidence of a Clinically Significant Drug-Drug Interaction between Cannabidiol and Tacrolimus. Am. J. Transplant., 2019. [DOI | PubMed]
- A. Lippert, B. Renner. Herb–Drug Interaction in Inflammatory Diseases: Review of Phytomedicine and Herbal Supplements. J. Clin. Med., 2022. [DOI | PubMed]
- K. Kreusel. Clinical Overview: Cannabis May Interact with Prescription Medications. Pharmacy Times, 2023
- G.C. So, J.B.L. Lu, S. Koyama, Y.H. Cheng, D.L. Gisch, K. McClara, P.R. Dexter, A.A. Sharfuddin, J. Etkins, E.M. Tillman. A Phase I Trial of the Pharmacokinetic Interaction Between Cannabidiol and Tacrolimus. Clin. Pharmacol. Ther., 2025. [DOI | PubMed]
- J.L.Q. Simei, J.D.R. Souza, J.F. Pedrazzi, F.S. Guimarães, A.C. Campos, A. Zuardi, J.E.C. Hallak, J.A.S. Crippa. Research and Clinical Practice Involving the Use of Cannabis Products, with Emphasis on Cannabidiol: A Narrative Review. Pharmaceuticals, 2024. [DOI | PubMed]
- R.F.d.O.E. Silva, E.N. Figueiredo. Current Legislation on Medical Cannabis in the European Union: Historical Background, Movements, Trends, and Counter-Trends Lessons for Brazil. BrJP, 2023. [DOI]
- M. Veit. Quality Requirements for Medicinal Cannabis and Respective Products in the European Union—Status Quo. Planta Med., 2023. [DOI | PubMed]
- C. Jardim, M.B. Delgado-Charro. The Regulatory Environment Surrounding Cannabis Medicines in the EU, the USA, and Australia. Pharmaceutics, 2025. [DOI | PubMed]
- 189. European Medicines Agency Epidyolex|European Medicines Agency (EMA) Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/epidyolex(accessed on 21 December 2025)
- E. Hahl, T. Kurko, H. Koskinen, M. Airaksinen, K. Sarnola. EMA Approved Orphan Medicines since the Implementation of the Orphan Legislation. Orphanet J. Rare Dis., 2025. [DOI | PubMed]
- E.U. Alum, J.E. Ekpang, P.O. Ekpang, C. Ainebyoona, K.E. Nwagu, O.A. Nwuruku, K. Muhammad. Toward an Ethical Future for Orphan Drugs: Balancing Access, Affordability, and Innovation. J. Med. Econ., 2025. [DOI | PubMed]
- Orphanet Orphanet: Quality Charter: Knowledge on Rare Diseases and Orphan Drugs
- T. Michaeli, H. Jürges, D.T. Michaeli. FDA Approval, Clinical Trial Evidence, Efficacy, Epidemiology, and Price for Non-Orphan and Ultra-Rare, Rare, and Common Orphan Cancer Drug Indications: Cross Sectional Analysis. BMJ, 2023. [DOI | PubMed]
- Q. Chen, Y. Xu, R. Qu, X. Luo, Y. Yang. Clinical Trial Evidence Supporting FDA Approval of Novel Orphan Drugs between 2017 and 2023. Drug Discov. Today, 2024. [DOI | PubMed]
- M. Xu, G. Li, J. Li, H. Xiong, S. He. Pharmacovigilance for Rare Diseases: A Bibliometrics and Knowledge-Map Analysis Based on Web of Science. Orphanet J. Rare Dis., 2023. [DOI | PubMed]