
A Systematic Review and Meta-Analysis of Cannabis Use Frequency and Metabolic Dysfunction-Associated Steatotic Liver Disease: Scapegoat or Healer?
Abstract
Potential associations have been investigated between metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease, and cannabis use. This study aimed to determine the association between cannabis use frequency and MASLD. Up to January 2025, the evidence from PubMed, Scopus, and Web of Science was synthesized in this systematic review and meta-analysis, which was registered in PROSPERO (CRD42025025065) and followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. Of the 711 initial records, 11 observational studies involving 5,968,702 individuals met the inclusion criteria. A pooled analysis revealed that cannabis use was associated with a reduced risk of hepatic steatosis (OR = 0.58; 95% CI: 0.42-0.81; p = 0.002; I² = 97%). The subgroup analysis revealed a protective association for past users (OR = 0.84; 95% CI: 0.77-0.93) and occasional users (OR = 0.35; 95% CI: 0.20-0.64), with no significant association observed for frequent users. The study revealed that cannabis users exhibited a decline in both the fatty liver index (mean difference (MD) = -11.02) and the BMI (MD = -1.89 kg/m²). However, the findings did not show any statistically significant changes in liver fat (%), transaminases (aspartate aminotransferase and alanine aminotransferase), and triglycerides. A risk-of-bias assessment identified notable methodological limitations. Overall, the findings suggest a strong association between cannabis use and MASLD, though causality cannot be established.
Article type: Review Article
Keywords: cannabis abuse, cannabis use, chronic cannabis use, fatty liver disease, metabolic dysfunction-associated steatotic liver disease
License: Copyright © 2025, Quinapanta Castro et al. CC BY 4.0 This is an open access article distributed under the terms of the Creative Commons Attribution License CC-BY 4.0., which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Article links: DOI: 10.7759/cureus.93183 | PubMed: 41141207 | PMC: PMC12553400
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (5.6 MB)
Introduction and background
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease [ref. 1], is the most common chronic liver disease worldwide [ref. 2–ref. 4]. Its prevalence has increased due to the popularity of Western diets and sedentary lifestyles [ref. 5]. The condition ranges from simple steatosis to non-alcoholic steatohepatitis (NASH) [ref. 1–ref. 3]. As part of the pathophysiological progression of MASLD, NASH represents a stage characterized by hepatic fat accumulation, sustained inflammation, and hepatocellular injury [ref. 5,ref. 6]. This can eventually lead to cirrhosis and the need for a liver transplant [ref. 5,ref. 6].
The overall incidence of EHMA is 47 cases per 1,000 people, occurring more frequently in men [ref. 7]. There was a significant 50.4% increase in its prevalence, rising from 25.26% between 1990 and 2006 to 38.00% between 2016 and 2019 (p < 0.001) [ref. 8]. The highest prevalence was observed in Latin America at 44.37% (30.66%-59.00%) [ref. 8].
MASLD is increasingly affecting younger people, which increases the risk of serious complications [ref. 3]. Due to changes in diet, urbanization, and the growth of obesity and type 2 diabetes, particularly in developing countries, the number of cases is expected to rise worldwide [ref. 3]. It is a public health problem associated with obesity, metabolic syndrome, and insulin resistance [ref. 9,ref. 10]. It results in the accumulation of fat in the liver and inflammation [ref. 9,ref. 10]. It is the hepatic manifestation of a systemic disease associated with type 2 diabetes and cardiovascular and renal disease [ref. 10].
Nowadays, it is understood that cannabis has emerged as a potential modulator of hepatic metabolism. The hepatic endocannabinoid system plays a key role in the accumulation of fat in the liver through cannabinoid receptor type 1 (CB1R) and cannabinoid receptor type 2 (CB2R) receptors [ref. 9]. Activation of the cannabinoid system has been linked to conditions such as cirrhosis and steatosis and also influences appetite regulation and energy metabolism [ref. 11]. The hepatic cannabinoid system is activated in MASLD, contributing to steatosis and insulin resistance [ref. 12]. CB1R is involved in the development of obesity and hepatic steatosis by stimulating de novo fatty acid synthesis [ref. 11]. CB1R expression is increased in fatty liver, and CB2R is involved in inflammation and hepatic fibrogenesis [ref. 11].
However, its management remains challenging due to its complexity [ref. 13]. Resmetirom is the first drug to be approved for treating MASLD with fibrosis, while the efficacy of other drugs is still under evaluation [ref. 13]. Meanwhile, research [ref. 14,ref. 15] suggests that cannabis users are less likely to have diabetes, obesity, and hyperlipidemia, which are closely related to MASLD.
Preclinical research, both in vivo and in vitro, has provided evidence supporting the therapeutic potential of cannabidiol (CBD) in a wide range of liver disorders [ref. 1]. Nonetheless, the underlying mechanisms remain insufficiently clarified, and the current scarcity of clinical data constrains their translation into routine clinical practice [ref. 1]. Contradictory evidence on the impact of cannabis on liver disease has been reported [ref. 16]. Cannabinoid receptors CB1 and CB2 are sparsely expressed in a healthy liver but overexpressed in chronic liver disease, potentially influencing the progression of steatosis and fibrosis [ref. 16].
This study aimed to determine the association between cannabis use frequency and MASLD, based on evidence obtained from a systematic review and meta-analysis of the literature.
Review
Methods
A systematic peer review and meta-analysis of the specialized academic literature was performed in the PubMed/MEDLINE, Scopus, and Web of Science databases. This meta-analysis followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) protocol.
Search Strategy
A systematic search was conducted using the Population, Intervention, Comparison, Outcome (PICO) strategy, focusing on the following main question: What is the association between cannabis use and metabolic dysfunction-associated steatotic liver disease?, based on evidence obtained from a systematic review and meta-analysis of the literature. In April 2024, the first searches were conducted using a combination of Medical Subject Headings (MeSH): “Cannabis”, “Cannabinoids”, “Marijuana Use”, “Nonalcoholic Fatty Liver Disease”, and “Fatty Liver”.
Selection Criteria
Quantitative, prospective, and retrospective observational studies, as well as cross-sectional studies, were included. Additionally, studies published in English or Spanish between 2005 and January 2025 should be considered. People over 18 years of age who use or consume cannabinoids, in any form, dose, or frequency, either for medical or recreational reasons, were included in the study. Editorials, letters to the editor, case series, and studies with nonhuman samples and in vitro tissue were excluded. Studies that addressed alcoholic fatty liver disease were also ruled out.
Primary and Secondary Outcomes
The primary outcomes of this review focused on the potential effect of cannabis use on the risk of hepatic steatosis, with prevalence assessed through imaging techniques, biochemical markers, or liver biopsy. The analysis also considered the fatty liver index (FLI) and BMI as additional indicators of liver health. Secondary outcomes included measurements of hepatic fat percentage and serum levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST), and triglycerides.
Data Extraction and Synthesis
Data extraction was performed using a form based on the Cochrane Consumers and Communication Group template for quality assessment and evidence synthesis. The form was adapted to collect all relevant information on the included studies and their results. The following data were extracted: authors, years, database consulted, journal of publication, date of publication, location of the study, type of article, DOI, original title, full abstracts, methodology applied, and results obtained. Two reviewers (NQC and ABS) independently extracted data, with disagreements resolved through consensus or consultation with an expert.
Each outcome’s findings were described in a narrative in the data synthesis. The quality of evidence will be assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method, considering characteristics such as risk of bias, inconsistency, indirectness, imprecision, and publication bias.
Analysis Methods
The exposure impact measures included ORs with 95% CIs for dichotomous data and mean difference (MD) and standardized MD (SMD) for continuous data, depending on the consistency of the outcome measures.
The random-effects model was used for analyses with high heterogeneity (I² >50%) or interstudy variations in design or population. Conversely, the fixed-effects model was used for subgroups with low heterogeneity, analyses with few studies, or when a large, high-quality study predominated in the statistical weighting. Heterogeneity was assessed using Tau², Chi², and I² statistics. All analyses were performed using Review Manager (RevMan) version 5.7.0 (The Cochrane Collaboration, Copenhagen, Denmark). The subgroup analysis included the frequency of use, as well as current and past use of cannabis, in the meta-analysis.
Risk of Bias Assessment
Risk of bias was independently assessed by two reviewers (NQC and ABS), with disagreements resolved through consensus or consultation with an expert. The Risk of Bias in Non-Randomized Exposure Studies (ROBINS-E) tool was employed to evaluate the risk of bias in observational studies. The overall risk of bias was classified as low, high, or uncertain.
Register
This systematic review is registered in PROSPERO under the registration number CRD42025025065. Additionally, the findings were presented as a scientific poster at the ESCI 2025 Annual Scientific Meeting of the European Society for Clinical Investigation, held on May 21-23, 2025.
Results
A total of 711 records were identified, 187 of which were eliminated due to duplication. Following an initial evaluation of the remaining 524 records, 475 were excluded because they did not meet the inclusion criteria. Of the 49 full texts reviewed, three could not be retrieved. Ultimately, 46 studies were evaluated, and 36 were excluded due to methodological or eligibility issues. Finally, 11 eligible studies were included, published across 10 scientific articles [ref. 17–ref. 26]. The process is detailed in the PRISMA diagram (Figure 1).
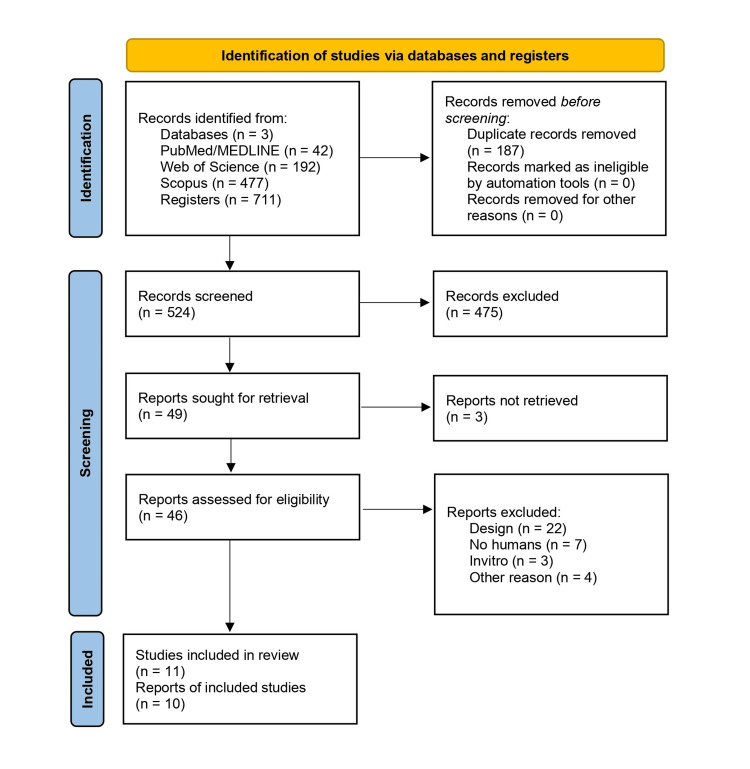
Table 1 presents the characteristics of the included studies. The mean (SD) age of the 5,968,702 participants was 41.29 (8.76) years. The studies were published between 2008 and 2023. Geographically, six of the 11 studies (55%) were conducted in North America [ref. 18,ref. 20,ref. 22,ref. 24,ref. 26], four (36%) in Europe [ref. 17,ref. 19,ref. 21,ref. 23], and one (9%) in Oceania [ref. 25]. In terms of study design, most were cross-sectional (n = 7), followed by retrospective (n = 2) and prospective (n = 2) studies.
Table 1: ALT, alanine aminotransferase; FLI, fatty liver index; ICD-9: International Classification of Diseases, 9th Revision; MRS, magnetic resonance spectroscopy; NHANES, National Health and Nutrition Examination Survey; VCTE, vibration-controlled transient elastography
| Author(s) | Country | Year | Study design | Diagnostic method | Baseline BMI (kg/m²) | Age (years) | Sex |
| Vázquez-Bourgon et al. [ref. 17] | Spain | 2019 | Prospective cohort | FLI | Nonusers: 33.7 (9.9); users: 25.2 (6.0) | 30.4 (9.5) | 217 males, 173 females |
| Liu et al. [ref. 18] | Canada | 2014 | Retrospective cohort | Liver biopsy | Not specified | Users: 43.9 ± 9.1; nonusers: 46.7 ± 8.1 | 265 males, 112 females |
| Hézode et al. [ref. 19] | France | 2008 | Cross-sectional | Liver biopsy | 24.8 (4.1) | 45.1 (10.9) | 223 males, 92 females |
| Du et al. [ref. 20] | USA | 2023 | Cross-sectional, probabilistic | VCTE | Not specified | 39.97 ± 11.65 | 1,287 males, 1,335 females |
| Barré et al. [ref. 21] | France | 2021 | Multicenter prospective cohort | FLI | Nonusers: 22.0; users: 20.9 | 47.8 ± 4.5 | 69.7% males, 30.3% females |
| Kim et al. [ref. 22] (NHANES) | USA | 2017 | Cross-sectional | ALT threshold | Never: 29.2 ± 0.1; former: 28.8 ± 0.1; current: 27.3 ± 0.3 | 39.6 | 7,040 males, 7,040 females |
| Kim et al. [ref. 22] (NHANES III) | USA | 2017 | Cross-sectional | Abdominal ultrasound | Never: 27.1 ± 0.2; former: 26.0 ± 0.2; current: 25.7 ± 0.4 | 37.6 | 4,002 males, 4,284 females |
| Nordmann et al. [ref. 23] | France | 2017 | Multicenter cross-sectional | Abdominal ultrasound | Not specified | 44.9 (95% CI: 44.5-45.4) | 585 males, 253 females |
| Adejumo et al. [ref. 24] | USA | 2017 | Retrospective case-control | Discharge diagnosis (ICD-9: 571.8) | Not specified | Not specified | 2,373,361 males, 3,459,451 females |
| Stuart et al. [ref. 25] | New Zealand | 2020 | Cross-sectional | MRS | Never: 26.8; non-regular: 27.9; regular: 34.3 | Never: 58; non-regular: 52; regular: 54 | 83 males, 37 females |
| Muniyappa et al. [ref. 26] | USA | 2013 | Cross-sectional, case-control | MRS | 27 ± 6 | 27 ± 8 | 18 males, 12 females per group |
Hepatic steatosis was assessed using imaging techniques, such as ultrasound, elastography, and magnetic resonance spectroscopy [ref. 20,ref. 22,ref. 23,ref. 25,ref. 26]; biochemical indices, including the FLI, liver biopsy, and serum ALT levels [ref. 18,ref. 19,ref. 21,ref. 22]; and diagnostic codes (ICD-9-MC 571.8) [ref. 24], as detailed in Table 1.
Primary Outcomes
MASLD: The nine studies [ref. 17–ref. 24] included in this meta-analysis indicated that individuals who used cannabis had a lower likelihood of presenting hepatic steatosis compared with nonusers. The pooled OR was 0.58 (95% CI: 0.42-0.81; p = 0.002), as shown in Figure 2, suggesting a potential protective association between cannabis use and this liver condition. Nonetheless, three individual studies crossed the null value, introducing some inconsistency in the interpretation of the results.
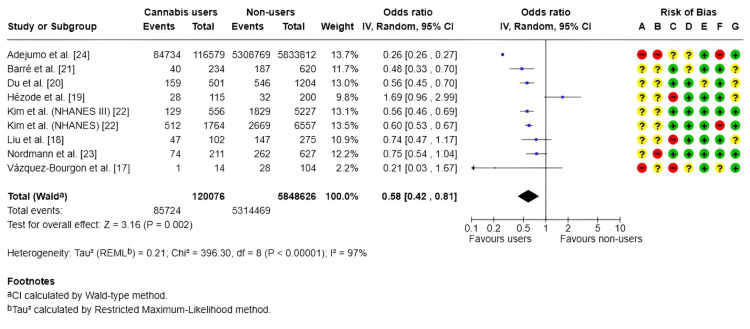
A high level of heterogeneity was observed among the studies (I² = 97%), reflecting substantial variability in the findings. This heterogeneity may be explained by methodological differences, variations in study populations, and clinical diversity. Furthermore, several studies exhibited high or unclear risks of bias, particularly in domains related to participant selection and outcome assessment.
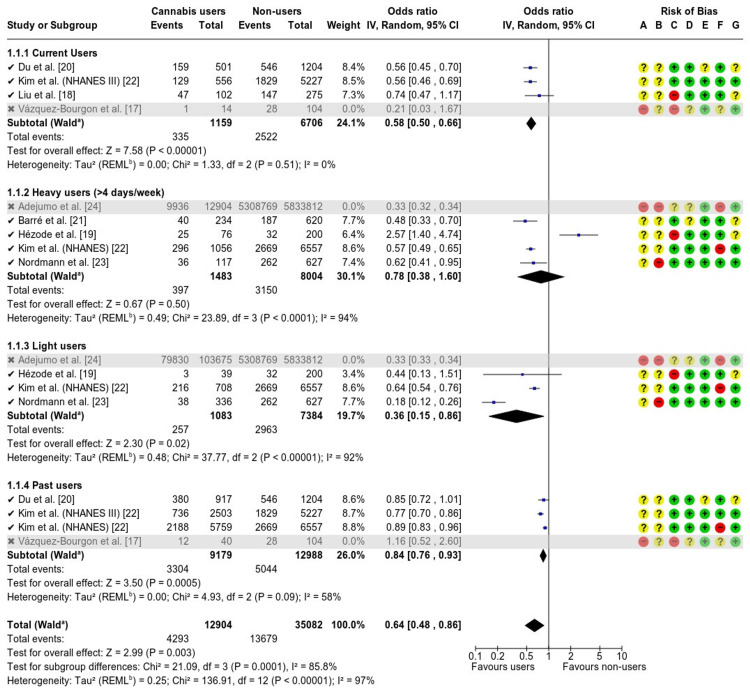
Subgroup analysis: The included studies [ref. 17–ref. 24] were classified according to the type and frequency of cannabis use, encompassing current users, heavy users (≥4 days/week), moderate users, and former users. While some studies compared only current users with nonusers, others differentiated between levels of use (moderate or heavy) or included multiple exposure categories, also accounting for past use.
The meta-analysis demonstrated that cannabis use was generally associated with a reduced likelihood of developing hepatic steatosis. The pooled effect estimate indicated a statistically significant reduction in risk among cannabis users compared with nonusers, with an OR of 0.59 (95% CI: 0.45-0.77; p < 0.00001), as presented in Figure 3.
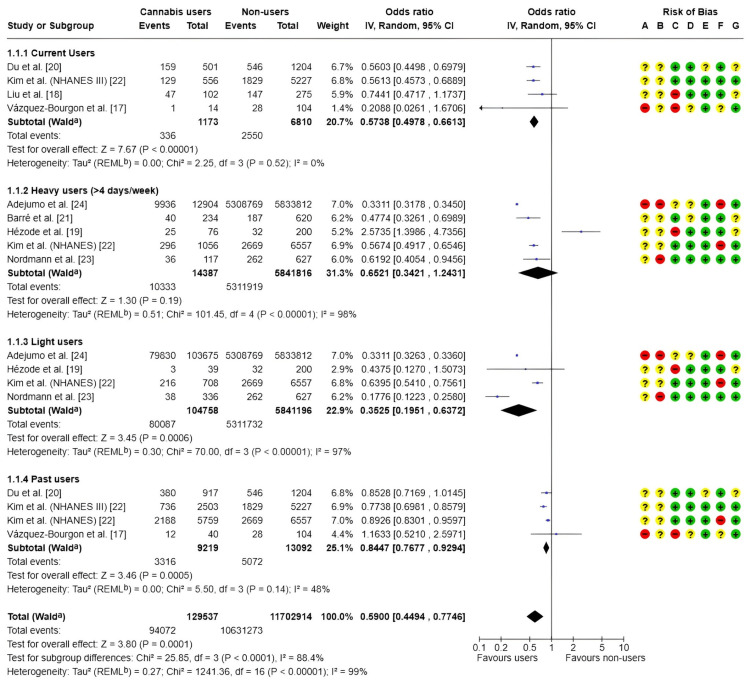
Subgroup analyses based on frequency and timing of cannabis use revealed that current users experienced a significant reduction in the risk of hepatic steatosis (OR = 0.57; 95% CI: 0.5-0.66), with no observed heterogeneity between studies (I² = 0%). Light users also demonstrated a protective effect, with an OR of 0.35 (95% CI: 0.20-0.64); however, substantial heterogeneity was present (I² = 97%). Among heavy users (≥4 days per week), no statistically significant association was identified (OR = 0.65; 95% CI: 0.34-1.24), and high heterogeneity (I² = 98%) limited the interpretability of results for this subgroup. Ex-users exhibited a modestly reduced risk of steatosis (OR = 0.84; 95% CI: 0.77-0.93), although moderate heterogeneity was observed (I² = 48%).
Overall, a high degree of heterogeneity was present across all studies (I² = 99%), likely attributable to methodological, clinical, and population differences. The risk of bias assessment further highlighted important limitations, particularly in domains related to participant selection and exposure measurement.
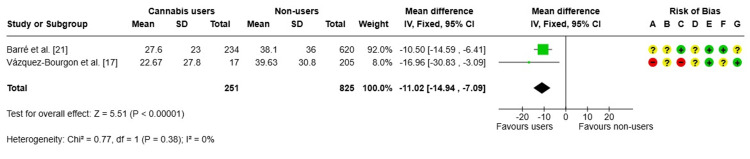
FLI: The findings [ref. 17,ref. 21] demonstrated that individuals who currently used cannabis exhibited a substantial reduction in FLI values compared to nonusers (MD: -11.02 points), as illustrated in Figure 4. This association was statistically significant and consistent across studies (I² = 0%). However, these results should be interpreted with caution due to the potential for high or uncertain risk of bias across multiple methodological domains, particularly in one of the included studies.
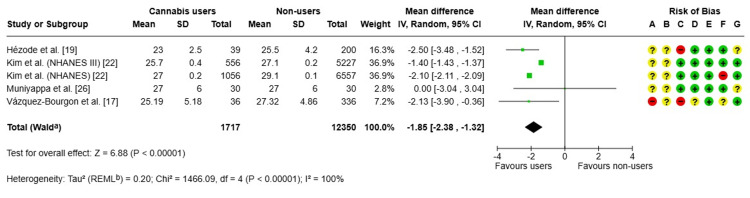
BMI: A meta-analysis [ref. 17,ref. 19,ref. 22,ref. 26] was performed to evaluate differences in BMI between current cannabis users and nonusers, based on data from five observational studies. Cannabis users exhibited a significantly lower mean BMI, with a pooled MD of -1.85 kg/m² (95% CI: -2.38 to -1.32; p < 0.00001), as illustrated in Figure 5. High heterogeneity was observed across studies (I² = 100%), reflecting substantial methodological and population variability. Several studies also presented potential risks of selection and measurement bias. Consequently, while a significant association between cannabis use and lower BMI was identified, causality cannot be inferred.
Secondary Results
Liver fat (%): A meta-analysis [ref. 25,ref. 26] was conducted to evaluate the difference in liver fat levels between current cannabis users and nonusers, using data from two observational studies. The combined results revealed an SMD of 0.30, 95%CI (-0.12 to 0.71), which did not reach statistical significance (p = 0.16), as shown in Figure 6. Additionally, the included studies showed no heterogeneity (I² = 0%).
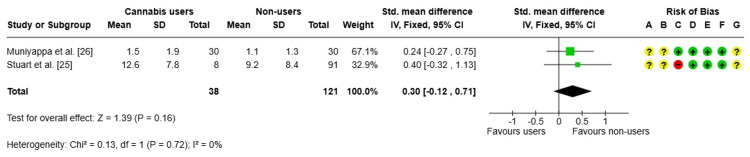
Although there is an apparent trend toward higher values in cannabis users, the current evidence does not allow us to conclude that there is a significant difference between the groups. The risk of bias analysis revealed minimal overall concern in most domains, though a high risk was identified in the selection of participants in one study and an uncertain risk in the measurement of exposure. The limited number of studies and small sample size limit the strength of the conclusions.
AST and ALT: For AST, the estimated MD was 1.86 units (95% CI: -0.84 to 4.57; p = 0.18) [ref. 17,ref. 26]. For ALT, the MD was -0.82 units (95% CI: -6.07 to 4.43; p = 0.76) [ref. 17,ref. 18,ref. 26], as shown in Figure 7. In both analyses, the CIs included the null value, indicating no statistically significant association. No heterogeneity was observed between studies (I² = 0%), supporting the consistency of these findings.
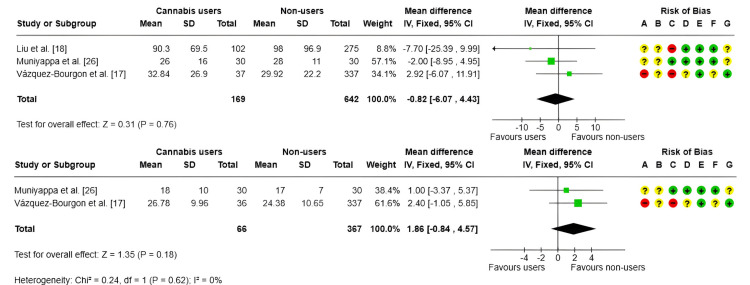
Overall, the results suggest that current cannabis use is not associated with significant changes in AST or ALT levels. However, some of the included studies presented risks of bias in specific domains, particularly regarding participant selection and exposure measurement.
Triglycerides: A fixed-effects meta-analysis [ref. 17,ref. 26] was conducted to assess differences in triglyceride levels between current cannabis users and nonusers, based on two primary studies. The pooled MD was 1.30 mg/dL (95% CI: -18.72 to 21.32; p = 0.90), as shown in Figure 8, indicating no statistically significant differences between the groups.
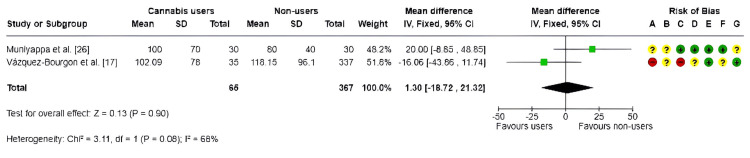
Moderate heterogeneity was observed (I² = 68%), reflecting variability between the included studies. Furthermore, potential risks of bias were noted, particularly related to confounding factors and participant selection, which may have affected the internal validity of the results.
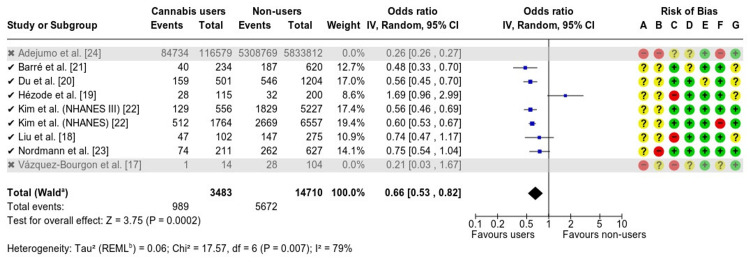
Sensitivity Analysis
A sensitivity analysis was conducted to evaluate the robustness of the findings and reduce the influence of studies with a high risk of bias. Excluding the studies by Vázquez-Bourgon et al. [ref. 17] and Adejumo et al. [ref. 24] yielded an OR of 0.66 (95% CI: 0.53-0.82; p = 0.0002), closely matching the initial estimate but indicating a slight attenuation of the effect on MASLD risk (Appendix A), thereby confirming the consistency of the results. A subgroup sensitivity analysis produced an overall OR of 0.64 (95% CI: 0.48-0.86; p = 0.0005), also consistent with the initial estimate, further supporting the robustness of the findings (Appendix B).
Publication Bias
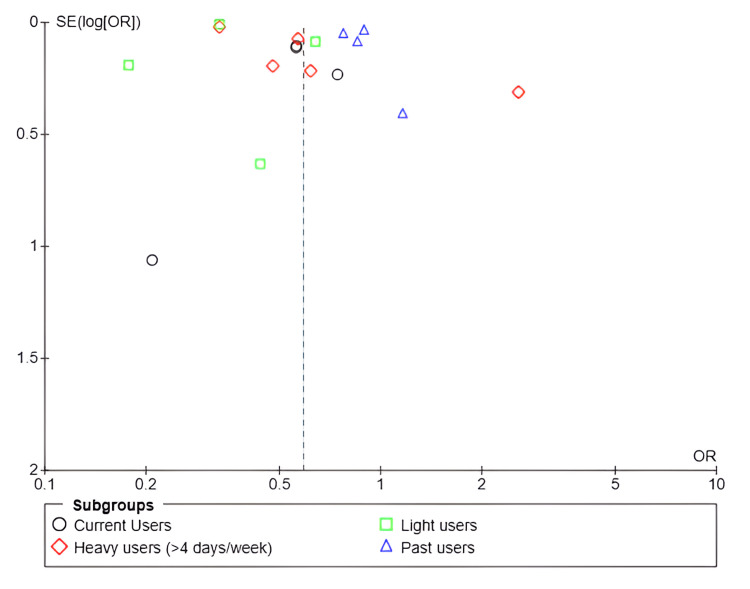
The funnel plot (Figure 9) demonstrated an asymmetric distribution of studies, suggesting the potential presence of publication bias or substantial heterogeneity in the results. Most studies, particularly those involving current, light, and past cannabis users, reported ORs below 1, supporting the hypothesis that cannabis use may confer a protective effect against hepatic steatosis. Nevertheless, the observed dispersion, especially among studies with lower precision, indicates that these findings should be interpreted with caution.
Risk of Bias
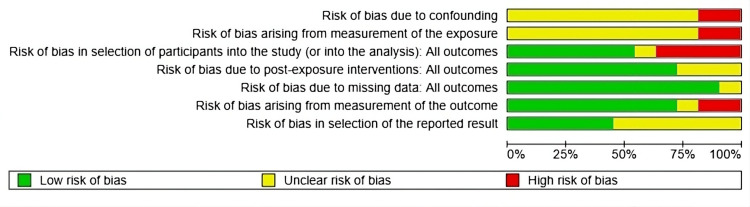
The risk of bias analysis (Figure 10) revealed significant methodological limitations in several domains, particularly regarding the control of confounding factors, the measurement of exposure, and participant selection. A substantial proportion of the included studies were classified as having a high or unclear risk of bias in these areas. In contrast, the domains related to subsequent interventions, missing data, and outcome measurement predominantly exhibited a low risk of bias; however, certain methodological uncertainties persisted.
Discussion
Cannabis use was associated with a lower risk of hepatic steatosis, as well as reduced FLI scores and BMI values. Light cannabis use demonstrated a significant protective effect against MASLD, whereas heavy use showed no significant association. Former users exhibited a modest reduction in risk. No statistically significant differences were observed in liver fat content, ALT, AST, or triglyceride levels, likely reflecting the limited number of studies included in these meta-analyses.
A study [ref. 27] revealed that, overall, cannabis use was not linked to liver stiffness. However, it was associated with a reduced risk of MASLD in women. A further meta-analysis [ref. 28] revealed that individuals who use cannabis have a lower BMI (25.5 vs. 27.5 kg/m²) and a reduced risk of obesity (AOR = 0.68). Individuals who are obese are particularly susceptible to MASLD, with a prevalence rate of 80% [ref. 29]. These results are similar to ours.
CBD may play a protective role in preventing hepatic steatosis through several molecular mechanisms. Suppression of NLRP3 inflammasome activation by deactivation of the NF-κB pathway in macrophages has been proposed as one of the most relevant anti-inflammatory mechanisms of CBD at the hepatic level [ref. 30].
Studies in vitro and in mouse models suggest that CBD and indole-3-carbinol can reduce fat accumulation in the liver by inhibiting lipogenesis and lipid storage, thereby helping to alleviate hepatic steatosis [ref. 31]. Furthermore, CBD has been found to reduce oxidative stress and selectively regulate intracellular signaling pathways that are involved in liver damage, such as JNK, without affecting p38 MAPK [ref. 32]. This suggests that it may have a hepatoprotective and metabolically beneficial effect.
Although public discourse often focuses on the potential therapeutic benefits of cannabis, the main scientific concerns are directed towards the physical, psychological, and social risks associated with its use, particularly when inhaled [ref. 33]. Cannabis smoke contains carcinogenic compounds at concentrations similar to or higher than those found in tobacco smoke, and cannabis use has been associated with respiratory conditions such as chronic bronchitis and epithelial damage [ref. 33]. Furthermore, the impact of the drug on the immune system has been observed, which is especially relevant for individuals with HIV/AIDS [ref. 33], as well as changes in cardiovascular [ref. 34] and reproductive functions [ref. 35].
Limitations
The review’s main limitation was the heterogeneity of methodology among the studies it included. Furthermore, the populations studied differed significantly. This variability introduced substantial differences in clinical and sociodemographic characteristics, which limited the generalizability of the findings.
Additional methodological limitations were identified, including the lack of standardization in the assessment of cannabis use, the absence of adequate control for relevant confounding variables, and the heterogeneity in diagnostic approaches for liver disease. Moreover, the potential influence of publication bias could not be excluded. These methodological constraints highlight the imperative need for well-designed longitudinal studies and rigorously conducted clinical trials to accurately evaluate the potential causal relationship between metabolic dysfunction and fatty liver disease.
Conclusions
The results of this review indicate a potential relationship between cannabis use and the presence of fatty liver disease associated with metabolic dysfunction. However, such an association should be interpreted with caution for several reasons. First, there is methodological heterogeneity among the studies. Second, there is high variability in the populations analyzed. Third, there are inherent limitations of the predominant cross-sectional and retrospective observational designs.
While some studies report that cannabis may protect against hepatic steatosis, a direct causal relationship cannot be established. The lack of standardization in the diagnostic tools used, as well as differences in frequency, duration, and modality of use, limits the robustness of the conclusions.
References
- S Chen, JK Kim. The role of cannabidiol in liver disease: a systemic review. Int J Mol Sci, 2024. [PubMed]
- E Amini-Salehi, N Letafatkar, N Norouzi. Global prevalence of nonalcoholic fatty liver disease: an updated review meta-analysis comprising a population of 78 million from 38 countries. Arch Med Res, 2024. [PubMed]
- VW Wong, M Ekstedt, GL Wong, H Hagström. Changing epidemiology, global trends and implications for outcomes of NAFLD. J Hepatol, 2023. [PubMed]
- ZM Younossi, M Kalligeros, L Henry. Epidemiology of metabolic dysfunction-associated steatotic liver disease. Clin Mol Hepatol, 2025
- B Zhu, SL Chan, J Li, K Li, H Wu, K Cui, H Chen. Non-alcoholic steatohepatitis pathogenesis, diagnosis, and treatment. Front Cardiovasc Med, 2021. [PubMed]
- F Savari, SA Mard. Nonalcoholic steatohepatitis: a comprehensive updated review of risk factors, symptoms, and treatment. Heliyon, 2024
- ML Teng, CH Ng, DQ Huang. Global incidence and prevalence of nonalcoholic fatty liver disease. Clin Mol Hepatol, 2023
- ZM Younossi, P Golabi, JM Paik, A Henry, C Van Dongen, L Henry. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology, 2023. [PubMed]
- YY Yang, HC Lin. Cross-regulation of cannabinoid CB1 and CB2 receptors governs hepatic steatosis. Liver Int, 2010. [PubMed]
- FM Trovato, P Castrogiovanni, L Malatino, G Musumeci. Nonalcoholic fatty liver disease (NAFLD) prevention: role of Mediterranean diet and physical activity. Hepatobiliary Surg Nutr, 2019. [PubMed]
- KA Alswat. The role of endocannabinoids system in fatty liver disease and therapeutic potentials. Saudi J Gastroenterol, 2013. [PubMed]
- A Mallat, S Lotersztajn. Cannabinoid receptors as novel therapeutic targets for the management of non-alcoholic steatohepatitis. Diabetes Metab, 2008. [PubMed]
- D Zhou, J Fan. Drug treatment for metabolic dysfunction-associated steatotic liver disease: progress and direction. Chin Med J (Engl), 2024. [PubMed]
- SE Mousavi, F Tondro Anamag, S Sanaie. Association between cannabis use and risk of diabetes mellitus type 2: a systematic review and meta-analysis. Phytother Res, 2023. [PubMed]
- T Barré, S Pol, C Ramier. Cannabis use is inversely associated with overweight and obesity in hepatitis B virus-infected patients (ANRS CO22 Hepather Cohort). Cannabis Cannabinoid Res, 2022. [PubMed]
- MT Farooqui, MA Khan, G Cholankeril. Marijuana is not associated with progression of hepatic fibrosis in liver disease: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol, 2019. [PubMed]
- J Vázquez-Bourgon, V Ortiz-García de la Foz, I Suarez-Pereira. Cannabis consumption and non-alcoholic fatty liver disease. A three years longitudinal study in first episode non-affective psychosis patients. Prog Neuropsychopharmacol Biol Psychiatry, 2019. [PubMed]
- T Liu, GT Howell, L Turner, K Corace, G Garber, C Cooper. Marijuana use in hepatitis C infection does not affect liver biopsy histology or treatment outcomes. Can J Gastroenterol Hepatol, 2014. [PubMed]
- C Hézode, ES Zafrani, F Roudot-Thoraval. Daily cannabis use: a novel risk factor of steatosis severity in patients with chronic hepatitis C. Gastroenterology, 2008. [PubMed]
- R Du, XY Tang, C Yang, WH Gao, SJ Gao, HJ Xiang, L Yang. Marijuana use is inversely associated with liver steatosis detected by transient elastography in the general United States population in NHANES 2017-2018: a cross-sectional study. PLoS ONE, 2023
- T Barré, T Rojas Rojas, K Lacombe. Cannabis use and reduced risk of elevated fatty liver index in HIV-HCV co-infected patients: a longitudinal analysis (ANRS CO13 HEPAVIH). Expert Rev Anti Infect Ther, 2021. [PubMed]
- D Kim, W Kim, MS Kwak, GE Chung, JY Yim, A Ahmed. Inverse association of marijuana use with nonalcoholic fatty liver disease among adults in the United States. PLoS ONE, 2017
- S Nordmann, A Vilotitch, P Roux. Daily cannabis and reduced risk of steatosis in human immunodeficiency virus and hepatitis C virus-co-infected patients (ANRS CO13-HEPAVIH). J Viral Hepat, 2018. [PubMed]
- AC Adejumo, S Alliu, TO Ajayi. Cannabis use is associated with reduced prevalence of non-alcoholic fatty liver disease: a cross-sectional study. PLoS ONE, 2017
- CE Stuart, J Ko, GC Alarcon Ramos, AE Modesto, J Cho, MS Petrov. Associations between cannabis use, abdominal fat phenotypes and insulin traits. J Clin Med Res, 2020. [PubMed]
- R Muniyappa, S Sable, R Ouwerkerk. Metabolic effects of chronic cannabis smoking. Diabetes Care, 2013. [PubMed]
- Y Wu, F Fang, X Fan, H Nie. Associations of cannabis use, metabolic dysfunction-associated steatotic liver disease, and liver fibrosis in U.S. adults. Cannabis Cannabinoid Res, 2025. [PubMed]
- TM Clark, JM Jones, AG Hall, SA Tabner, RL Kmiec. Theoretical explanation for reduced body mass index and obesity rates in cannabis users. Cannabis Cannabinoid Res, 2018. [PubMed]
- FA Muñoz Rossi, J Salazar Agudelo, NI Quinapanta Castro. Relationship between metabolic dysfunction-associated steatotic liver disease and lipoprotein (a) and other biomarkers. Cureus, 2024
- Y Huang, T Wan, N Pang. Cannabidiol protects livers against nonalcoholic steatohepatitis induced by high-fat high cholesterol diet via regulating NF-κB and NLRP3 inflammasome pathway. J Cell Physiol, 2019. [PubMed]
- S Senthilkumar, ME Solan, MT Fernandez-Luna. Cannabidiol and indole-3-carbinol reduce intracellular lipid droplet accumulation in HepaRG, a human liver cell line, as well as in human adipocytes. Nat Prod J, 2024
- L Yang, R Rozenfeld, D Wu, LA Devi, Z Zhang, A Cederbaum. Cannabidiol protects liver from binge alcohol-induced steatosis by mechanisms including inhibition of oxidative stress and increase in autophagy. Free Radic Biol Med, 2014. [PubMed]
- A Mack, J Joy. How harmful is marijuana?. Marijuana as Medicine?: The Science Beyond the Controversy, 2000
- SR Archie, L Cucullo. Harmful effects of smoking cannabis: a cerebrovascular and neurological perspective. Front Pharmacol, 2019. [PubMed]
- KS Ryan, JC Bash, CB Hanna, JC Hedges, JO Lo. Effects of marijuana on reproductive health: preconception and gestational effects. Curr Opin Endocrinol Diabetes Obes, 2021. [PubMed]