
Validation of the Child Depression Screening Tool in three African settings: Rwanda, Senegal and South Africa
Abstract
The unavailability of reliable, easy-to-use depression screening tools adapted for Sub-Saharan African children is a significant barrier to the treatment of childhood depression. We thus adapted the Child Depression Screening Tool (CDST) to the South African (SA), Senegalese (S) and Rwandan (R) contexts, as a tool to screen for depression in children suffering from chronic illnesses, trauma and difficulties related to COVID-19, family and community hardships. A DSM-5-based diagnostic interview and the CDST screening measure were administered to 1,001 participants aged between 7 and 16 years. The prevalence of depression ranged between 9.5 and 16.8%. It was more prevalent in youth with chronic illness and those exposed to adverse life events. Older age (R and SA), female sex (S), dislike of school (R and SA) and cannabis use (SA) were also associated with worse depression. Receiver operating characteristic analysis showed satisfactory performance (79-89%) and that sensitivity and specificity were optimized at a CDST cut-point of 5.0. The CDST is a valid tool to screen for depression in the settings assessed. If found to be suitable in other countries and settings, it may offer a clinically sound, sustainable path towards the identification of child depression in Africa.
Article type: Research Article
Keywords: child depression, child depression screening tool, Sub-Saharan Africa
Affiliations: MRC Genomics of Brain Disorders Unit and Department of Psychiatry, https://ror.org/05bk57929Stellenbosch University, Cape Town, South Africa; Zambia National Public Health Institute, https://ror.org/03gh19d69University of Zambia School of Medicine, Lusaka, Zambia; Non-communicable Diseases (NCDs), Injuries and Mental Health Program, https://ror.org/01d9dbd65Africa Centres for Disease Control and Prevention (Africa CDC), Ethiopia; Rwanda Biomedical Centre, https://ror.org/04c8tz716University of Global Health Equity (UGHE), Kigali, Rwanda; Division of Disease Control and Prevention, https://ror.org/01d9dbd65Africa Centres for Disease Control and Prevention (Africa CDC), Ethiopia; Department of Psychology, https://ror.org/04je6yw13The Cheikh Anta Diop University (UCAD), Dakar, Senegal; Faculty of Medicine, https://ror.org/04je6yw13The Cheikh Anta Diop University (UCAD), Dakar, Senegal; https://ror.org/03dbr7087University of Montreal, Montreal, QC, Canada; Institute for Training and Research in Population, Development and Health Reproduction (IPDSR), https://ror.org/02ysgwq33The Cheikh Anta Diop University (UCAD), Dakar, Senegal; Department of Pediatrics, https://ror.org/04c8tz716University of Global Health Equity, Kigali, Rwanda; London School of Hygiene and Tropical Medicine, London, UK
License: © The Author(s) 2025 CC BY 4.0 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0), which permits unrestricted re-use, distribution and reproduction, provided the original article is properly cited.
Article links: DOI: 10.1017/gmh.2025.10022 | PubMed: 40625840 | PMC: PMC12231306
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (497 KB)
Impact statement
- There are few affordable and easy-to-use measures adapted for childhood depression in Africa.
- The Child Depression Screening Tool (CDST), developed in Africa, is a free, rapid screening tool for depression in children that may fill this gap.
- This new tool can contribute to improved identification of depression and referral to appropriate mental health care for children at risk of depression.
- Cannabis use was associated with depression, poor school performance and considerations of dropping out of school. The use of the CDST may provide opportunities to evaluate and treat associated difficulties such as these.
Background
Mental health difficulties are a major burden for children and adolescents globally, with the World Health Organisation (ref. 2021) estimating that ~14% of 10- to 19-year-olds worldwide experience mental disorders. Evidence suggests that depression is one of the most commonly experienced mental disorders in adolescents and that its prevalence is increasing (Daly, ref. 2022; Mojtabai et al., ref. 2016. Around 1.1% of children and adolescents aged 10–14 years, and 2.8% of adolescents aged 15–18 years are estimated to have clinical depression (WHO, ref. 2021a). In Sub-Saharan Africa (SSA), a systematic review encompassing 20 studies reported clinically significant depressive symptoms in 27% of adolescents in the general population and in 29% of adolescents from at-risk groups (Jorns-Presentati et al., ref. 2021). A more recent review among SSA youth under 19 years of age found a pooled prevalence rate of 15% (Jakobsson et al., ref. 2024). More specifically, in Rwanda, rates of clinically assessed depression in children with human immunodeficiency virus (HIV) were found to range between 14 and 25% (Binagwaho et al., ref. 2016, ref. 2021). South African (SA) studies have reported that between 4 and 41% of adolescents report experiencing symptoms of depression, potentially indicative of a diagnosis (Pluddemann et al., ref. 2008; Morojele et al., ref. 2013; De Vries et al., ref. 2018).
Risk factors for child and adolescent depression in Africa include biopsychosocial stressors, such as age, sex, food insecurity, bullying and low perceived levels of social support, substance use, poor access to healthcare and exposure to stressful and traumatic events (Partap et al., ref. 2023). Medical risk factors include chronic diseases, such as diabetes, cancer, HIV, tuberculosis and asthma (Harrison et al., ref. 2023). In addition, studies, mostly from high-income countries, report increased levels of depressive symptoms during and after the recent coronavirus disease 2019 (COVID-19) pandemic (Racine et al., ref. 2021; Wang et al., ref. 2022). Youth well-being during this time was likely affected by stress about one’s own or loved one’s health, social isolation and increased family stressors (i.e., parental job loss and domestic violence) (Loades et al., ref. 2020; Liang and Zeng, ref. 2021; Barendse et al., ref. 2023). Although in SSA youth, low levels of depressive symptoms have been associated with the pandemic, further studies are needed to explore the longer-term effects (Matovu et al., ref. 2021; Wang et al., ref. 2021).
Childhood and adolescent depression are associated with functional impairment in home, school and social domains, as well as increased suicide risk (WHO, ref. 2021b). It is also associated with negative health outcomes in adulthood, such as higher levels of adult anxiety and substance use disorders, worse health and social functioning, less financial and educational achievement and increased criminal behaviour (Johnson et al., ref. 2018; Clayborne et al., ref. 2019; Copeland et al., ref. 2021).
Despite their prevalence and long-lasting effects, child and adolescent mental health and well-being have been overlooked in global health planning (UNICEF, ref. 2021). Most mental health needs in young people are still unmet, especially in low- and middle-income countries (LMICs) where adversity is most prevalent. It is estimated that about four out of five people in LMICs who need services for mental health conditions do not receive them, despite there being effective treatments available (Mangione et al., ref. 2022).
Systematic and scoping reviews have identified several barriers to treatment seeking and accessing professional help for mental health problems. These include limited mental health literacy, perceived social stigma and embarrassment, perceptions around confidentiality and trust of an unknown person, financial costs, resource shortages (i.e., limited access to mental healthcare providers) and logistical barriers (Radez et al., ref. 2021; Saade et al., ref. 2023). Another systematic review, from the primary care providers’ perspective, identified barriers related to identification, management and/or referral (O’Brien et al., ref. 2016). A scoping review of barriers specific to African youth found that a preference for traditional or complementary treatments, stigma and mental health literacy was the most common (Saade et al., ref. 2023).
Given the above, there is consensus that child and adolescent mental health services need to be strengthened. This is particularly so in LMICs and SSA, where risk factors may be greater and resources fewer (WHO | Regional Office for Africa, ref. 2021). In a system such as this, it is understandable that many depressed youths may slip through the cracks and not receive the help they need. A brief free screening test will greatly assist in this regard. First, it may assist with the early diagnosis of depression in children and adolescents, allowing them to receive the care that they need to recover. Second, being short and concise, it should not place more of a burden on an already stretched healthcare system where time and capacity are in short supply. Finally, as a free tool, it can be administered without limitations to those children and adolescents who might need it.
In Rwanda, the Children’s Depression Inventory (CDI) and the Center for Epidemiological Studies Depression Scale for Children (CES-DC) have been validated with reasonable results (Betancourt et al., ref. 2012; Binagwaho et al., ref. 2016). The CDI, however, requires an administration fee and the CES-DC was not validated in youth with HIV. Thus, Binagwaho et al. undertook to develop a tool that was both free and tailored to young people with HIV (Binagwaho et al., ref. 2021). The Child Depression Screening Tool (CDST) was developed with the support of skilled and knowledgeable local professionals with the assurance that the tool is valid, reliable, affordable and easy for primary care level providers to use (Binagwaho et al., ref. 2021). This approach has the advantage of ensuring that socio-economic and cultural differences are considered, to fully capture the symptoms of depression, ensuring that respondents would fully understand the questionnaire, and that the expression of depression within the Rwandan (R) cultural context is truly actualized (Owen et al., ref. 2016).
Given the positive psychometric results obtained in the R validation, CDST may also offer a clinically sound, sustainable path forward to support the diagnosis and treatment of child depression, particularly in at-risk youth, in SSA. However, for a tool to be used with confidence, validation and adaptation of mental health screening tools for use in a particular setting are crucial to ensure that they accurately identify mental health issues, are culturally appropriate and linguistically accessible (Juhász et al., ref. 2003).
The primary aim of this study was to adapt and validate the CDST, a rapid screening tool, to effectively screen for depression in at-risk children in three SSA countries – Rwanda, Senegal and South Africa (Binagwaho et al., ref. 2021). This included children suffering from HIV and other chronic illnesses, displacement, trauma, as well as experiencing difficulties because of COVID-19, family and community hardships that put them at higher risk of depression (Davidson et al., ref. 2017; Boyes et al., ref. 2019; Awad et al., ref. 2024; Collings and Valjee, ref. 2024). Secondary aims were to assess the prevalence and correlates of depression in the three countries.
Methodology
Study design and setting
This was a multi-country cross-sectional study design and was conducted in Rwanda, Senegal and South Africa between December 2021 and March 2022.
Participants
The sample size calculation was calculated using the Buderer formula and assuming a sensitivity of 88% and a specificity of 96%, based on the results of the initial CDST study conducted in Rwanda (with the cut-off of 6), a 10% width for sensitivity and specificity and a 95% confidence interval (95% CI). The sample size calculation was adjusted for non-response (5–10%), and the sample size and allocation were adjusted to the study population size in each country to give the following sample sizes: Rwanda N = 340, Senegal N = 500 and South Africa N = 300.
At all sites, we included children aged 7–16 years who gave written assent and whose parents/guardians gave consent to participate. Recruitment took place via convenience sampling. Participants from refugee/displacement camps (e.g., youth who left their countries/homes to escape conflict, violence, persecution or natural disaster) were required to have lived in the camp for a minimum of 12 months. No additional inclusion or exclusion criteria were applied. We did, however, select sites where our yield of participants living with chronic diseases (HIV, cancer, diabetes or cardiovascular diseases) and other adverse events (lifetime Diagnostic and Statistical Manual of Mental Disorders, 5th Edition [DSM-5] trauma), recent frightening events (including DSM-5 trauma in the last month) and experiencing COVID or the effects of COVID (e.g., loss of income or close family members) would be high.
In Rwanda, recruitment took place at refugee camps, schools and health facilities. In Senegal, recruitment sites included refugee camps, schools, sites with street-involved youth (e.g., at homeless shelters and with those living and engaged in begging on the streets) and impoverished (poor) youth. In South Africa, recruitment took place at health facilities, children’s homes, schools and in communities with high levels of trauma.
Measures
The data collection tools included a socio-demographic questionnaire, the Child Depression Screening Tool (CDST) (Binagwaho et al., ref. 2021) and a DSM-5-based clinical interview as a gold standard to assess depression. Further, medical data were extracted from patient files, where available. The CDST comprised 11 items, each with 4 response options that are scored from 0 to 3 (0 = absence of symptoms, 1 = symptoms sometimes present, 2 = symptoms frequently present and 3 = symptoms always present). The 11 items cover the following areas: mood, representation of the future, interest in games, sleep, fatigue, appetite, attention, agitation, relationships with others and suicidal thoughts. Scores range from 0 to 33, with a cut-point of 6 suggested in the original validation study (Binagwaho et al., ref. 2021).
In Senegal and South Africa, the CDST was translated from English to the local languages by a team of experienced research nurses, clinical psychologists or psychiatrists. To ensure accuracy, the tool was back-translated to English by a different team of clinicians. The translation process had already been completed in Rwanda as part of the development and first validation study (Binagwaho et al., ref. 2021). After testing the tool in small pilot studies and adapting it to each setting, the tool was programmed into the ODK, an open-source Android application, which was used to gather data in electronic format. Data were collected by trained psychologists, nurses and counsellors.
Procedures
Ethical approvals were obtained before the start of the study.
Children and adolescents who gave written assent and whose parents gave consent to participate were included in the study. The purpose of the study, procedures involved, voluntary nature, potential risks and benefits and assurance of confidentiality of collected information were fully explained, and children were given the option to opt out at the time of the assessment. Measures were made available in the most common languages used in the setting (Rwanda: Kinyarwanda; Senegal: Wolof and French; SA: Afrikaans, English and isiXhosa) to ensure the efficacy and accuracy of the cut-offs obtained.
Psychologists, research nurses and psychological counsellors were trained to administer the CDST and evaluate depression in a standardized manner in the child’s preferred language. The interviewer who administered the CDST was blinded to the outcome of the clinical interview and vice versa. Children who were identified as requiring further assessment or treatment were referred to mental health clinicians and further specialized services.
Data analysis
Percentages and 95% CIs were calculated to describe sample characteristics. Scores on the CDST were then compared to MDD diagnoses on the clinical interview to determine sensitivity (proportion of children who have depression according to clinical interview and who are correctly identified by the CDST) and specificity (proportion of children without depression and who have been correctly identified as non-depressed by the CDST) at different cut-points. Receiver operating characteristic (ROC) curve analysis was used to determine the ability of the CDST to discriminate between individuals who did and did not meet the criteria for depression according to the diagnostic interview. The area under the curve (AUC) provides an indication of the diagnostic ability of the CDST: values between 0.5 and 0.7 indicate low discriminatory ability; values between 0.7 and 0.9 indicate moderate discriminatory ability; and values above 0.9 indicate high discriminatory ability of a measure (Hosmer and Lemeshow, ref. 2000).
Assumptions for computing CIs were met as follows: (i) independent observations – visual inspection of our data suggests that each case represents a distinct respondent; (ii) normality – given our sample size, the central limit theorem ensures that the sampling distributions for means, sums and proportions approximate normal distributions.
Results
Sample characteristics
A total of 1,001 children and adolescents participated in the study. In Rwanda, 340 children and adolescents participated: (a) 186 (54%) with chronic diseases, (b) 80 (24%) primary and high school children and (c) 75 (22%) children from refugee camps. Their ages ranged between 7 and 15 years. In Senegal, 345 vulnerable youth participated in the study: (a) 151 (43.8%) of these had chronic diseases and (b) 122 (35.4%) were street-involved, refugee and displaced youth, as well as those living in poverty and from schools. Nearly half the children classified as vulnerable were street-involved youth from the capital city of Dakar, approximately one-third were refugee or displaced children and 18% were living in extreme poverty. The most common chronic diseases among the children were sickle-cell anaemia (34%) and HIV (29%), followed by diabetes and cancer. Ages ranged between 7 and 14 years. In South Africa, 315 children and adolescents were included: (a) 9 (2.9%) with a known chronic disease, that is, HIV+, diabetic or direct COVID experience and (b) 84 (26%) who had ever been exposed to DSM-5 trauma and 50 (15.8%) who had experienced a frightening event in the last few weeks. Ages ranged between 7 and 16 years.
Rwanda
A total of 340 children with a mean age of 11.3 years participated in the study. Table 1. shows that while 88.5% of participants lived with their parents, 11.5% were not living with their parents for various reasons, including the death of parents or separation. The majority of participants (78.8%) were students in primary school and 21.2% were in high school. A considerable proportion of participants had poor academic performance, as 60% repeated a year at least once in their lifetime. In addition, 48.4% missed class time due to health or family reasons, and 9.06% considered dropping out of school.
Table 1.: Socio-demographic characteristics of the samples: Rwanda, South Africa and Senegal
| Rwanda | Senegal | South Africa | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Percent | Prevalence of depression | 95% Cl | n | Percent | Prevalence of depression | 95% Cl | n | Percent | Prevalence of depression | 95% Cl | |
| Overall | 336 | 14.3 | [10.9,18.5] | 345 | 16.8 | [13.2,21.2] | 315 | 9.2 | [6.5,13.0] | |||
| Age group (years) | ||||||||||||
| 7–9 | 85 | 25.3 | 5.9 | [2.5,13.4] | 110 | 31.90 | 16.4 | [10.5,24.5] | 67 | 21.3 | 1.5 | [0.2,9.9] |
| 10–12 | 113 | 33.6 | 13.3 | [8.1,20.9] | 130 | 37.70 | 16.2 | [10.8,23.5] | 98 | 31.2 | 3.1 | [1.0,9.1] |
| 13–14/15/16 | 138 | 41.1 | 20.3 | [14.4,27.9] | 105 | 30.40 | 18.1 | [11.8,26.7] | 149 | 47.5 | 16.8 | [11.6,23.7] |
| Sex | ||||||||||||
| Male | 172 | 51.2 | 14.5 | [10.0,20.7] | 212 | 61.40 | 13.2 | [9.3,18.5] | 151 | 3.8 | 7.9 | [4.6,13.5] |
| Female | 164 | 48.8 | 14 | [9.5,20.3] | 133 | 38.60 | 27.8 | [16.2,30.5] | 164 | 96.2 | 11.0 | [7.0,16.8] |
| Parents are alive | ||||||||||||
| Both parents alive | 296 | 85.90 | 15.9 | [12.1,20.5] | ||||||||
| At least one parent deceased | 49 | 14.10 | 22.4 | [12.9,36.2] | ||||||||
| Is your mom alive? | ||||||||||||
| Yes | 285 | 90.8 | 8.4 | [5.7,12.3] | ||||||||
| no | 29 | 9.2 | 20.7 | [9.6,39.2] | ||||||||
| Is your dad alive? | ||||||||||||
| Yes | 247 | 80.2 | 8.5 | [5.6,12.7] | ||||||||
| no | 61 | 19.8 | 14.8 | [7.8,26.1] | ||||||||
| What is your parents’ marital situation? | ||||||||||||
| Married | 57 | 19.4 | 14.0 | [7.1,25.7] | ||||||||
| Divorced | 12 | 4.1 | 16.7 | [4.2,47.9 | ||||||||
| Never married/single | 201 | 68.4 | 7.0 | [4.2,11.4] | ||||||||
| Widow(ed) | 24 | 8.2 | 8.3 | [2.1,28.1] | ||||||||
| Child live with both parents | ||||||||||||
| Yes | 296 | 88.1 | 13.2 | [9.8,17.6] | ||||||||
| No | 39 | 11.6 | 23.1 | [12.4,38.8] | ||||||||
| Place of residence | ||||||||||||
| Urban | 273 | 79.10 | 13.9 | [10.3,18.6] | 306 | 96.1 | 9.8 | [6.5,13.1] | ||||
| Rural | 72 | 20.90 | 27.8 | [18.6,39.2] | 9 | 3.9 | 0 | [0] | ||||
| Region | ||||||||||||
| Dakar | 171 | 49.60 | 9.4 | [5.8,14.8] | ||||||||
| Matam | 29 | 8.40 | 44.8 | [28.0,62.9] | ||||||||
| Saint Louis | 63 | 18.30 | 7.9 | [3.3,17.8] | ||||||||
| Ziguinchor | 82 | 23.80 | 29.3 | [20.4,40.0] | ||||||||
| Number of meals per day | ||||||||||||
| One | 16 | 4.60 | 25.0 | [9.7,51.0] | ||||||||
| Two | 39 | 11.30 | 17.9 | [8.8,33.2] | ||||||||
| Three or more | 290 | 84.10 | 16.2 | [12.4,20.9] | ||||||||
| Religion of the child | ||||||||||||
| Christian | 256 | 82.3 | 10.2 | [7.0,14.5] | ||||||||
| Muslim | 21 | 6.8 | 4.8 | [0.7,27.4] | ||||||||
| None/others | 28 | 10.9 | 7.1 | [1.8,24.6] | ||||||||
| Child live in a boarding school | ||||||||||||
| No | 255 | 76.8 | 17.3 | [13.1,22.4] | 241 | 76.8 | 9.1 | [5.9,12.3] | ||||
| Yes | 71 | 21.1 | 2.8 | [0.7,10.6] | 73 | 23.2 | 11.0 | [7.5,14.5] | ||||
| Current education level | ||||||||||||
| Primary | 266 | 79.1 | 14.3 | [10.6,19.1] | 182 | 52.80 | 20.3 | [15.1,26.8] | 215 | 68.7 | 4.7 | [2.5,8.5] |
| Secondary | 70 | 20.8 | 14.3 | [7.8,24.6] | 73 | 21.20 | 16.4 | [9.6,26.8] | 98 | 31.3 | 20.4 | [13.5,29.6] |
| Daara (Islamic school) | 69 | 20.00 | 7.2 | [3.0,16.3] | ||||||||
| No formal education | 21 | 6.10 | 19.0 | [7.3,41.3] | ||||||||
| Ever repeated school year | ||||||||||||
| No | 151 | 44.9 | 18.5 | [13.1,25.6] | ||||||||
| Yes | 101 | 30.1 | 15.8 | [9.9,24.4] | ||||||||
| Are you often absent from school? | ||||||||||||
| Yes | 120 | 35.7 | 26.7 | [19.5,35.3] | 36 | 27.8 | 8.3 | [2.7,23.0] | ||||
| No | 131 | 39.0 | 9.2 | [5.3,15.5] | 278 | 72.2 | 9.7 | [6.7,13.8] | ||||
| Considered dropping out of school | ||||||||||||
| Yes | 23 | 6.8 | 43.5 | [25.1,63.8] | 18 | 5.8 | 27.8 | [22.8,32.8] | ||||
| No | 228 | 67.9 | 14.9 | [10.8,20.2] | 295 | 94.2 | 8.1 | [5.1,11.1] | ||||
| Population type | ||||||||||||
| Students | 76 | 22.0 | 13.2 | [7.2,22.8] | ||||||||
| Vulnerable children (street-involved, refugee/displaced, impoverished | 118 | 34.20 | 16.1 | [10.5,23.9] | ||||||||
| Street-involved | 55 | 45.10 | 9.1 | [1.5,16.7] | ||||||||
| Refugee | 24 | 19.70 | 29.2 | [11.0,47.4] | ||||||||
| Displaced | 22 | 18.00 | 27.3 | [8.7,45.8] | ||||||||
| Impoverished | 21 | 17.20 | 9.5 | [−3.0,22.1] | ||||||||
| Children with chronic disease | 151 | 43.80 | 19.2 | [13.7,26.3] | ||||||||
| Ever exposed to DSM–5 trauma | 84 | 26.7 | 11.9 | [5.6,18.4][81.6, 94.4] | ||||||||
| Recent frightening event | 50 | 15.8 | 22 | [17.4,26.6]69.9,86.1 | ||||||||
| HIV+, diabetic + or had COVID | 9 | 2.9 | 33.3 | [28.1,38.5]57.8, 76.2 | ||||||||
The mean score on the CDST was 2.9 (95% CI: 1.6, 4.2). Based on the clinical interview, 14.3% (95% CI: 10.9, 18.5) of children were found to have depression. Prevalence was similar in male (14.5%, 95% CI: 10.0, 20.7) and female (14.0%, 95% CI: 9.5, 20.3) participants, but was higher in adolescents aged 13–15 (20.3%, 95% CI: 14.4, 27.9) years than in children in younger age groups (ages 7–9 years = 5.9% 95% CI: 2.5, 13.4 and 10–12 years = 13.3%, 95% CI: 8.1, 20.9). Children living with their parents reported fewer depressive symptoms than those living elsewhere (13.2%, 95% CI: 9.8, 17.6 vs. 23.1%, 95% CI: 12.4, 38.8). Higher rates of depression were observed in children not attending school regularly (26.7%, 95% CI: 19.5, 35.3 vs. 9.2%, 95% CI: 5.3, 15.5) and in those contemplating dropping out of school (43.5%, 95% CI: 25.1, 63.8 vs. 14.9%, 95% CI: 10.8, 20.2).
Senegal
A sample of 345 participants with a mean age of 11.0 years was included. As shown in Table 1., the vulnerable children included more boys than girls, which largely reflects the much higher number of street-involved boys than girls (52 boys vs. 3 girls, respectively). A similar proportion of boys and girls was represented among the students and the children with chronic diseases, except for sickle-cell anaemia (32 boys vs. 16 girls).
The overall prevalence of depression determined by a standard clinical interview was 16.8% (95% CI: 13.2, 21.2). Table 1. displays the prevalence of depression for the sample according to socio-demographic characteristics. More girls experienced depression than boys (22.6%, 95% CI: 16.2, 30.5 vs. 13.2%, 95% CI: 9.3, 18.5), as did children living in rural versus urban areas (27.8%, 95% CI: 18.6, 39.2 vs. 13.9%95% CI: 10.3, 18.6).
The mean CDST score was 4.1 (95% CI: 3.7, 4.4). The prevalence of depression based on clinical interview was particularly high in the Matam and Ziguinchor regions (44.8%, 95% CI: 28.0, 62.9 and 29.3%, 95% CI: 20.4, 40.0, respectively). Children educated in traditional Islamic schools (Daaras) had lower depression prevalence (7.2%, 95% CI: 3.0, 16.3) as compared to those in primary or secondary formal schools (20.3%, 95% CI: 15.1, 26.8), and nearly 16.4% (95% CI: 9.6, 26.8) were boys. Among participants classified as vulnerable children, children with chronic diseases and students, depression prevalence was 16.1% (95% CI: 10.5, 23.9), 19.2% (95% CI: 13.7, 26.3) and 13.2% (95% CI: 7.2, 22.8), respectively. While sample sizes are small when stratified by type of vulnerability, results suggest that refugee (29.2%, 95% CI: 11.0, 47.4) and displaced (27.3%, 95% CI: 8.7, 45.8) children are more likely to suffer from depression compared with street-involved youth (9.1%, 95% CI: 1.5, 16.7) and children living in extreme poverty (9.5%, 95% CI: −3.0, 22.1). More than one in five children with cancer, sickle-cell anaemia and HIV were identified to have depression. When we stratified results by sex, vulnerable girls had a particularly elevated prevalence of depression (32.3%, 95% CI: 15.8, 48.7) compared to boys (10.3%, 95% CI: 3.9, 16.7).
South Africa
In South Africa, 315 participants with a mean age of 11.6 years were included. Just over a quarter, 26.7%, of the 315 children endorsed lifetime trauma exposure, and 15.9% had experienced a frightening event in the last few weeks. Only a few children had direct exposure to COVID-related trauma, with 1.0% indicating that they had lost a close family member to COVID. Of the 2.9% who indicated that they were aware of having a chronic disease, 1.9% indicated that they were HIV+ and 1.0% indicated that they were diabetic. A large number of participants were from disadvantaged environments, with just over a third (36.5%) indicating that their family received a government grant (e.g., disability grant or pension). The majority (96.1%) resided in urban areas in the Cape Metropole region of South Africa. While 27.8% had lived away from home for more than 3 months at some time, at the time of this study, only 23.2% were currently living in a group or boarding home. Socio-demographic characteristics of participants are displayed in Table 1.
The mean CDST score was 5.4 (95% CI: 4.9, 5.9). The number of children who scored above the recommended cut-off of 6 on the CDST (Binagwaho et al., ref. 2021), that is, those with probable depression, was 22 (26.7%). The prevalence of depression, as determined by clinicians conducting the clinical interviews, was 9.5%. A diagnosis of major depressive disorder was more prevalent in older children (13–16 years old [16.8%, 95% CI: 11.6, 23.7]), than in younger children (7–9 years old [1.5%, 95% CI: 0.2, 9.9] and 10–12 years old [3.1%, 95% CI: 1.0, 9.1]). Children who indicated that they considered dropping out of school (27.8%, 95% CI: 22.8, 32.8 vs. 8.1%, 95% CI: 5.1, 11.1) and children who had lost their mothers were more likely to be depressed (20.7% 95% CI: 9.6, 39.2 vs. 8.4% 95% CI: 5.7, 12.3). Those who experienced a recent frightening event (22%, 95% CI: 17.4, 26.6 vs. 95% CI: 69.9, 86.1) and those who had experienced COVID or had a chronic illness (33.3%, 95% CI: 28.1, 38.5 vs. 57.8, 76.2) were also more likely to be depressed. Of note, almost half (43%) of the participants who smoked cannabis were depressed. Cannabis use was related to age, with older children more likely to be using the substance (95% CI: −0.003, 0.052).
Criterion validity of the CDST
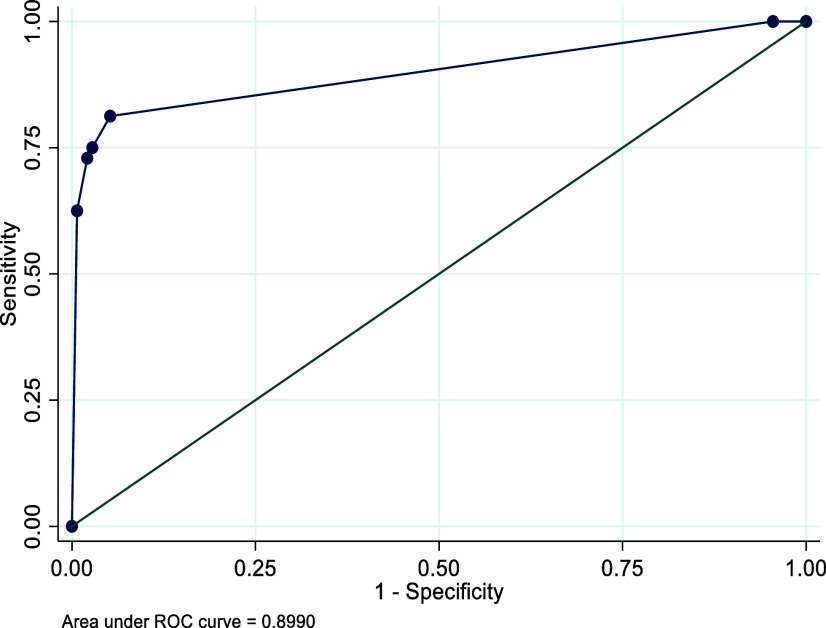
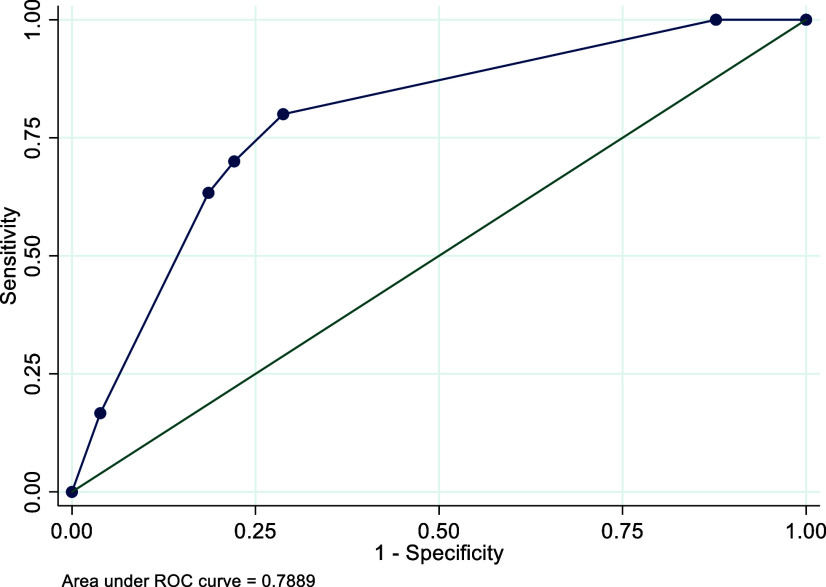
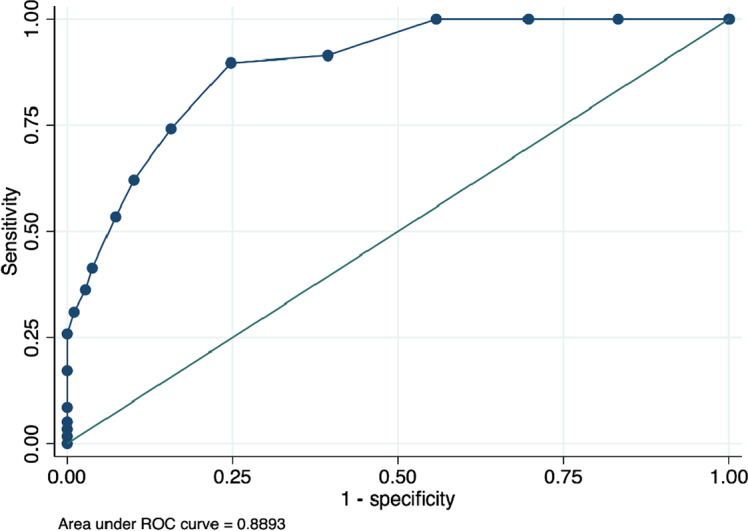
CDST scores were compared to the clinical interview results to obtain sensitivity and specificity. Table 2 provides the sensitivity and specificity of different scores per country. For all three countries, Rwanda, Senegal and South Africa, the cut-point of 5 provided the best sensitivity and specificity.
Table 2.: Sensitivity and specificity of the CDST at different cut-points for Rwanda, Senegal and South Africa
| Sensitivity | Specificity | |
|---|---|---|
| Rwanda | ||
| Score – 4 | 81% | 90% |
| Score – 5 | 81% | 95% |
| Score – 6 | 75% | 97% |
| Score – 7 | 65% | 99% |
| Score – 8 | 63% | 99% |
| Senegal | ||
| Score – 4 | 91% | 61% |
| Score – 5 | 90% | 75% |
| Score – 6 | 74% | 84% |
| Score – 7 | 62% | 90% |
| Score – 8 | 53% | 93% |
| Score – 9 | 41% | 96% |
| South Africa | ||
| Score – 4 | 80% | 59% |
| Score – 5 | 80% | 71% |
| Score – 6 | 70% | 78% |
| Score – 7 | 53% | 82% |
| Score – 8 | 47% | 85% |
The AUC is used to assess the overall performance of a test. In ROC analyses, the CDST showed good discriminatory power relative to the DSM-5-based structured clinical interview for depression, with an AUC of 0.90 for Rwanda, 0.89 for Senegal and 0.79 for South Africa. See Figures 1–3. These AUCs of above 0.79 indicate that the CDST performed significantly better than chance at discriminating between those with and without depression in the three countries.
Discussion
Although numerous tools to screen for depression in children are available, few are accessible and adapted to African settings. This cross-sectional study aimed to adapt the CDST, a rapid tool to screen for childhood depression. Accurate assessments can be critical to targeting resources, especially when there are limited resources for mental health treatment. A total sample of 1,001 children and adolescents was recruited across three countries (Rwanda: n = 340; Senegal: n = 345; South Africa: n = 316).
ROC analysis was conducted to identify the CDST cut-point that best predicted depressive status as assessed by the clinical interview. The ROC curve demonstrated that sensitivity and specificity in all three samples were optimized at a cut-point of 5.0. This is one point lower than the recommended cut-off of 6, based on the original validation study (Binagwaho et al., ref. 2021). At the cut-point of 5, sensitivity was highest in the Senegalese (S) sample (90%) as compared to the R (81%) and SA (80%) samples. Specificity at this cut-point was best in the R sample (95%) as compared to the S (75%) and SA (71%) samples. In addition, the performance of the measure, according to the ROC analysis, was satisfactory, which was 89–90% (medium–high) in the R and S samples and 79% (medium) in the SA sample. These robust AUC statistics indicate that depressed youth are 79–90% more likely to have a high total score on the CDST than those who do not have depression. The sound psychometric properties and anecdotal ease of use expressed by those who administered the CDST suggest that the CDST can be a useful tool to screen for depression in children and adolescents in these settings.
Secondary aims included estimating the prevalence and correlates of depression in the three countries. Based on diagnostic clinical interviews, the prevalence of depression was lowest in SA youth (9.3%) as compared to R and S youth (14.3% and 16.8%, respectively). Given the heterogeneity of the youth samples in the three countries, these prevalence estimates cannot be directly compared. The sample from South Africa was predominantly composed of children exposed to family and community hardships and had a lower number of children diagnosed with chronic illnesses − <3% of the sample as compared to 54% and 43.8% in the R and S samples, respectively.
In accordance with studies showing an association between chronic disease and depression (Binagwaho et al., ref. 2021; Dessauvagie et al., ref. 2020; Too et al., ref. 2021), elevated rates of depression were found in youth with chronic illness in all three countries. The risk of depression was also significantly higher among children and adolescents exposed to adverse life events, such as the death of a family member, physical or sexual abuse or being a refugee, in all countries. Exposure to adverse events such as these has consistently been identified as a risk factor for depression (Rao and Chen, ref. 2009; Thapar et al., ref. 2012; Oldehinkel et al., ref. 2015; Beck et al., ref. 2021; Jorns-Presentati et al., ref. 2021).
The prevalence rates are similar to global prevalence rates and a study done in Ethiopia (Belfer, ref. 2008; Girma et al., ref. 2021; Racine et al., ref. 2021). Although lower than those found in other African countries (e.g., Uganda [21%] and Nigeria [21.2%]), these studies based their findings on self-report measures, which are known to provide higher estimates (Fatiregun and Kumapayi, ref. 2014; Nalugya-Sserunjogi et al., ref. 2016). We found that older children/adolescents were more likely to be at risk of depression than were younger children. Numerous studies have confirmed this finding of adolescents being more at risk than children, possibly due to the emotional, psychological and physical changes that they undergo during this developmental period (Belfer, ref. 2008; Costello et al., ref. 2011; Jorns-Presentati et al., ref. 2021; Oldehinkel et al., ref. 2015; Racine et al., ref. 2021).
Girls had a higher rate of depression than boys in the S sample. Female sex has commonly been found to be a risk factor for depression, including in LMICs, such as Ethiopia, India and Uganda (Patten et al., ref. 2006; Nalugya-Sserunjogi et al., ref. 2016; Trivedi et al., ref. 2016; Riecher-Rössler, ref. 2017; Beck et al., ref. 2021; Girma et al., ref. 2021; Racine et al., ref. 2021; Too et al., ref. 2021). However, this was not so in both the SA and R samples. This may be explained by the younger age of participants, as while similar rates of depression have been found during childhood, females are at increased risk during and after adolescence (Hyde et al., ref. 2008; Alsaad et al., ref. 2022).
Depression has been associated with a number of long-term psychosocial outcomes. These include a lower likelihood of entering post-secondary education, poor performance at school, an increased risk of leaving secondary school and substance abuse (Dunn and Goodyer, ref. 2006; Lund et al., ref. 2010; Cairns et al., ref. 2014; Maras et al., ref. 2015; Gunnell et al., ref. 2016; Clayborne et al., ref. 2019; Beck et al., ref. 2021; Olisaeloka et al., ref. 2024; Ward-Smith et al., ref. 2024). Similarly, we found that those who indicated that they disliked school and those who considered dropping out of school were more likely to be depressed, and, in the SA sample, close to half of those who smoked cannabis were depressed.
Recent reviews and meta-analyses of cannabis use in SSA adolescents have reported rates of 4–8% (Asante and Atorkey, ref. 2023; Belete et al., ref. 2023). A 2007 review of cannabis use in South Africa reported a current self-reported rate of 5–10% among adolescents (Peltzer and Ramlagan, ref. 2007). Although the rate of cannabis use in this sample was lower, almost half of those who did use met criteria for depression. Systematic reviews and a meta-analysis determined that cannabis use in adolescence is associated with both higher levels of depression and predictive of depression, with some reporting that the links between heavy cannabis use during adolescence and poorer academic success and educational attainment are thought to be associated with lower academic motivation (Cairns et al., ref. 2014; Pacheco-Colón et al., ref. 2019).
The findings should be viewed in light of the study’s limitations. First, as the samples from each country were largely convenience-based, they cannot be considered representative of the populations they were drawn from. Second, we unfortunately did not capture data on the frequency and length of substance use; this would be important to include in future studies. Third, we unintentionally omitted capturing the language in which the CDST was administered; this could have provided useful information regarding cut-off scores in each of the languages. Despite this, strengths of this study include that the validation process and assessment of predictors remain substantially robust, and that the CDST is developed in Africa and is a free, open-access rapid assessment tool for depression. In addition, anecdotally, the researchers who administered the CDST found it easy to use in all three countries. Thus, the CDST can allow early diagnosis as a first step towards access to treatment for depression management in Rwanda, Senegal and South Africa.
Conclusion
This study demonstrates the validity of the CDST in Rwanda, Senegal and South Africa. If found to be valid and reliable in other African settings, it may be used to enhance the capacity of community-based healthcare providers to identify and refer youth with depression. In addition, given the association between cannabis use and depression, as well as cannabis use and poorer school performance/considerations of dropping out of school, the use of the CDST and similar tools may open up possibilities for healthcare professionals and community health workers to evaluate and treat these associated difficulties and conditions. Accurate and early identification of symptoms that take socio-economic and cultural differences into account can facilitate referral for appropriate treatment and improve long-term well-being (Patton et al., ref. 2016).
References
- Alsaad AJ, Azhar Y and Nasser Y Al (2022) Depression In Children. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK534797/ (accessed 22 May 2023).
- Cannabis and amphetamine use among school-going adolescents in sub-Saharan Africa: A multi-country analysis of prevalence and associated factors.. BMC Psychiatry, 2023. [DOI | PubMed]
- Assessment of displaced Sudanese school-age children’s mental health at ad-Damar, River Nile, Sudan, 2024: A descriptive cross-sectional study.. BMC Public Health, 2024. [DOI]
- Longitudinal change in adolescent depression and anxiety symptoms from before to during the COVID‐19 pandemic.. Journal of Research on Adolescence, 2023. [DOI | PubMed]
- Screening for depression in children and adolescents: A protocol for a systematic review update.. Systematic Reviews, 2021. [DOI]
- Cannabis use in sub-Saharan Africa: A systematic review and meta-analysis.. Addiction., 2023. [DOI]
- Child and adolescent mental disorders: The magnitude of the problem across the globe.. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 2008. [DOI | PubMed]
- Validating the center for epidemiological studies depression scale for children in Rwanda.. Journal of the American Academy of Child and Adolescent Psychiatry, 2012. [PubMed]
- Validating the children’s depression inventory in the context of Rwanda.. BMC Pediatrics, 2016. [DOI | PubMed]
- Addressing the mental health needs of children affected by HIV in Rwanda: Validation of a rapid depression screening tool for children 7-14 years old.. BMC Pediatrics, 2021. [DOI]
- Mental health in south African adolescents living with HIV: Correlates of internalising and externalising symptoms.. AIDS Care, 2019. [DOI | PubMed]
- Risk and protective factors for depression that adolescents can modify: A systematic review and meta-analysis of longitudinal studies.. Journal of Affective Disorders, 2014. [DOI | PubMed]
- Clarke D, Australia KC-MJ of and 2009 undefined (2009.) Depression, anxiety and their relationship with chronic diseases: a review of the epidemiology, risk and treatment evidence. Wiley Online Library. https://onlinelibrary.wiley.com/doi/abs/10.5694/j.1326-5377.2009.tb02471.x (accessed 2 June 2023).
- Systematic review and meta-analysis: Adolescent depression and long-term psychosocial outcomes.. Journal of the American Academy of Child & Adolescent Psychiatry, 2019. [DOI | PubMed]
- A multi-mediation analysis of the association between adverse childhood experiences and non-suicidal self-injury among south African adolescents.. International Journal of Environmental Research and Public Health, 2024. [DOI]
- Associations of childhood and adolescent depression with adult psychiatric and functional outcomes.. Journal of the American Academy of Child and Adolescent Psychiatry, 2021. [DOI | PubMed]
- Trends in psychopathology across the adolescent years: What changes when children become adolescents, and when adolescents become adults?. Journal of Child Psychology and Psychiatry., 2011. [DOI]
- Prevalence of depression among adolescents in the U.S. from 2009 to 2019: Analysis of trends by sex, race/ethnicity, and income.. Journal of Adolescent Health, 2022. [DOI]
- Adolescent nephrology: An emerging frontier for kidney care in sub-Saharan Africa.. Nephrology (Carlton, Vic.), 2017. [DOI | PubMed]
- Measuring adolescent mental health around the globe: Psychometric properties of the self-report strengths and difficulties questionnaire in South Africa, and comparison with UK, Australian and Chinese data.. Epidemiology and Psychiatric Sciences, 2018. [DOI | PubMed]
- The prevalence of mental health problems in sub-Saharan adolescents living with HIV: A systematic review.. Global Mental Health (Cambridge, England), 2020. [DOI]
- Longitudinal investigation into childhood- and adolescence-onset depression: Psychiatric outcome in early adulthood.. The British Journal of Psychiatry : The Journal of Mental Science, 2006. [DOI | PubMed]
- Prevalence and correlates of depressive symptoms among in-school adolescents in a rural district in Southwest Nigeria.. Journal of Adolescence, 2014. [DOI | PubMed]
- Depression and its determinants among adolescents in Jimma town, Southwest Ethiopia.. PLoS One, 2021. [DOI]
- Examining the bidirectional relationship between physical activity, screen time, and symptoms of anxiety and depression over time during adolescence.. Preventive Medicine., 2016. [DOI]
- Better together: Acceptability, feasibility and preliminary impact of chronic illness peer support groups for South African adolescents and young adults.. Journal of the International AIDS Society, 2023. [DOI | PubMed]
- Applied logistic regression.. Applied Logistic Regression., 2000. [DOI]
- The ABCs of depression: Integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression.. Psychological Review, 2008. [DOI | PubMed]
- Meta-analysis: Prevalence of youth mental disorders in sub-Saharan Africa.. Cambridge Prisms: Global Mental Health, 2024. [DOI | PubMed]
- Adult mental health outcomes of adolescent depression: A systematic review.. Depression and Anxiety, 2018. [DOI | PubMed]
- The prevalence of mental health problems in sub-Saharan adolescents: A systematic review.. PLoS One, 2021. [DOI | PubMed]
- The use of RBANS test (repeatable battery for the assessment of neuropsychological status) in neurocognitive testing of patients suffering from schizophrenia and dementia].. Ideggyogyaszati Szemle, 2003. [PubMed]
- Factors affecting children’s mental health during the coronavirus disease 2019 pandemic.. JAMA Pediatrics, 2021. [DOI | PubMed]
- Rapid systematic review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19.. Journal of the American Academy of Child & Adolescent Psychiatry, 2020. [DOI | PubMed]
- Poverty and common mental disorders in low and middle income countries: A systematic review.. Social Science & Medicine, 2010. [DOI | PubMed]
- Screening for depression and suicide risk in children and adolescents: US preventive services task force recommendation statement.. JAMA, 2022. [DOI | PubMed]
- Screen time is associated with depression and anxiety in Canadian youth.. Preventive Medicine, 2015. [DOI | PubMed]
- COVID-19 awareness, adoption of COVID-19 preventive measures, and effects of COVID-19 lockdown among adolescent boys and Young men in Kampala, Uganda.. Journal of Community Health, 2021. [DOI | PubMed]
- National trends in the prevalence and treatment of depression in adolescents and young adults.. Pediatrics, 2016. [DOI]
- Morojele N, Myers B, Townsend L, Lombard C, Plüddemann A and Carney T (2013) Survey on substance use, risk behaviour and mental health among grade 8–10 learners in Western Cape provincial schools, 2011 | Health and Education Resource Centre. https://healtheducationresources.unesco.org/library/documents/survey-substance-use-risk-behaviour-and-mental-health-among-grade-8-10-learners (accessed 28 March 2025).
- Prevalence and factors associated with depression symptoms among school-going adolescents in Central Uganda.. Child and Adolescent Psychiatry and Mental Health, 2016. [DOI | PubMed]
- Barriers to managing child and adolescent mental health problems: A systematic review of primary care practitioners’ perceptions.. British Journal of General Practice, 2016. [DOI]
- Cohort profile update: The TRacking adolescents’ individual lives survey (TRAILS).. International Journal of Epidemiology, 2015. [DOI | PubMed]
- Psychosocial interventions for depression among young people in sub-Saharan Africa: A systematic review and meta-analysis.. International Journal of Mental Health Systems, 2024. [DOI | PubMed]
- Child and adolescent mental health in sub-Saharan Africa: A perspective from clinicians and researchers.. BJPsych International, 2016. [DOI | PubMed]
- Effects of adolescent Cannabis use on motivation and depression: A systematic review.. Current Addiction Reports, 2019. [DOI | PubMed]
- Depressive symptoms among adolescents in six sub-Saharan African countries: A pooled analysis of associated factors.. Preventive Medicine Reports, 2023. [DOI | PubMed]
- Descriptive epidemiology of major depression in Canada.. The Canadian Journal of Psychiatry, 2006. [PubMed]
- Our future: A lancet commission on adolescent health and wellbeing.. Lancet (London, England), 2016. [DOI | PubMed]
- Cannabis use trends in South Africa.. South African Journal of Psychiatry, 2007. [DOI]
- Adolescent methamphetamine use and sexual risk behaviour in secondary school students in Cape Town, South Africa.. Drug and Alcohol Review, 2008. [DOI | PubMed]
- Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: A meta-analysis.. JAMA Pediatrics, 2021. [DOI | PubMed]
- Why do children and adolescents (not) seek and access professional help for their mental health problems? A systematic review of quantitative and qualitative studies.. European Child and Adolescent Psychiatry, 2021. [DOI | PubMed]
- Characteristics, correlates, and outcomes of childhood and adolescent depressive disorders.. Dialogues in Clinical Neuroscience, 2009. [DOI | PubMed]
- Sex and gender differences in mental disorders.. The Lancet Psychiatry, 2017. [DOI | PubMed]
- What barriers could impede access to mental health services for children and adolescents in Africa? A scoping review.. BMC Health Services Research, 2023. [DOI | PubMed]
- Seminar Child & Adolescent Psychiatry Section, Department of Psychological Medicine and Neurology (Prof A Thapar FRCPsych, S Collishaw DPhil, A K Thapar depression in adolescence.. Lancet, 2012. [DOI | PubMed]
- Prevalence and factors associated with common mental disorders in young people living with HIV in sub-Saharan Africa: A systematic review.. Journal of the International AIDS Society,, 2021. [DOI | PubMed]
- Depression among adolescent students in South India: How serious is the issue?. Indian Journal of Psychiatry, 2016. [DOI | PubMed]
- UNICEF (2021) 65 per cent of young people with mental health related issues did not seek help – UNICEF. Retrieved from https://www.unicef.org/southafrica/press-releases/65-cent-young-people-mental-health-related-issues-did-not-seek-help-unicef
- The COVID-19 pandemic and adolescents’ experience in sub-Saharan Africa: A cross-country study using a telephone survey.. The American Journal of Tropical Medicine and Hygiene, 2021. [DOI | PubMed]
- Depression and anxiety among children and adolescents pre and post COVID-19: A comparative meta-analysis.. Frontiers in Psychiatry, 2022. [DOI]
- An investigation into symptoms of depression and anxiety and emotion regulation among older adolescents from low-income settings in South Africa.. Comprehensive Psychiatry, 2024. [DOI | PubMed]
- WHO (2021a) Global Health Estimates. https://www.who.int/data/global-health-estimates (accessed 12 May 2023).
- WHO (2021b) Mental health of adolescents. https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed 19 May 2023).
- WHO | Regional Office for Africa (2021) Access to mental health and psychosocial support services remains unequal for children and adolescents in Africa, alert UNICEF & WHO |. https://www.afro.who.int/news/access-mental-health-and-psychosocial-support-services-remains-unequal-children-and (accessed 23 May 2023).