
Tetrahydrocannabinol vape-associated cannabis arteritis in a patient with minimal tobacco exposure
Abstract
Thromboangiitis obliterans (TAO) is an inflammatory vasculopathy that often presents in young men with substantial tobacco use. Cannabis arteritis is the cannabis-associated counterpart, but there remains controversy over its classification due to overwhelming concurrent tobacco use. A 31-year-old man developed lifestyle-limiting claudication that coincided with vaping high-potency tetrahydrocannabinol. Notably, his tobacco exposure was limited to a remote history of <1 pack-year. His claudication considerably improved after 4 weeks of cannabis cessation. This case demonstrates a rare instance of cannabis arteritis without concurrent tobacco use, suggesting cannabis may act as an independent causative agent of a distinct thromboangiitis obliterans-like arteritis.
Article type: Case Report
Keywords: Cannabis arteritis, Thromboangiitis obliterans (TAO), Delta-9-tetrahydrocannabinol (THC), Vaping, Vasculitis, Claudication
Affiliations: Johns Hopkins University School of Medicine, Baltimore, MD; Division of Vascular Surgery, Department of Surgery, Johns Hopkins Bayview Medical Center, Baltimore, MD
License: © 2024 The Authors CC BY 4.0 This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/).
Article links: DOI: 10.1016/j.jvscit.2024.101673 | PubMed: 39691796 | PMC: PMC11650286
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (390 KB)
Cannabis arteritis is a thromboangiitis obliterans-like (TAO) vasculitis linked to cannabis use rather than tobacco. This non-atherosclerotic vasculopathy manifests clinically as segmental occlusive lesions and obliterations of distal small and medium-sized arteries.ref. bib1,ref. bib2 It characteristically affects young adults in their 20s and 30s with a strong male predominance.ref. bib2 Cannabis arteritis is a diagnosis of exclusion in young patients with arteriopathy and significant cannabis use.ref. bib3 It remains challenging to definitively classify and characterize cannabis arteritis within the context of TAO and establish a causal link due to the substantial overlap in cannabis and tobacco exposure in many cases. Although the current evidence suggests that cannabis acts as an aggravating factor, there is not enough convincing data to suggest that it is a primary causative factor with a unique presentation.ref. bib2,ref. bib4,ref. bib5 This case of cannabis arteritis occurred in an otherwise healthy young man with chronic cannabis usage and tetrahydrocannabinol (THC) vaping but minimal tobacco exposure. He presented with severe bilateral lower extremity claudication, which substantially improved with cannabis cessation. The patient consented to the publication of the details and images included in this report.
Case description
A previously healthy 31-year-old man presented to the vascular surgery clinic with bilateral lower extremity claudication, right worse than left. He reported a 3-year history of gradually worsening calf tightness that limited his activity to 5 to 7 minutes of walking before needing to rest. Before symptom onset, the patient lived an active lifestyle, playing soccer and rock climbing regularly. The patient exhibited no Raynaud’s symptoms, phlebitis, or upper extremity complaints.
His social history is significant for a 12-year duration of chronic cannabis usage to alleviate anxiety. Notably, his claudication symptoms coincided with the transition from smoking cannabis daily from a pipe to vaping high-potency hash oil several times a day. Other substance use history includes occasional social alcohol use, smoking 2 to 3 cigarettes/day for 1 year in college, and no illicit drug use.
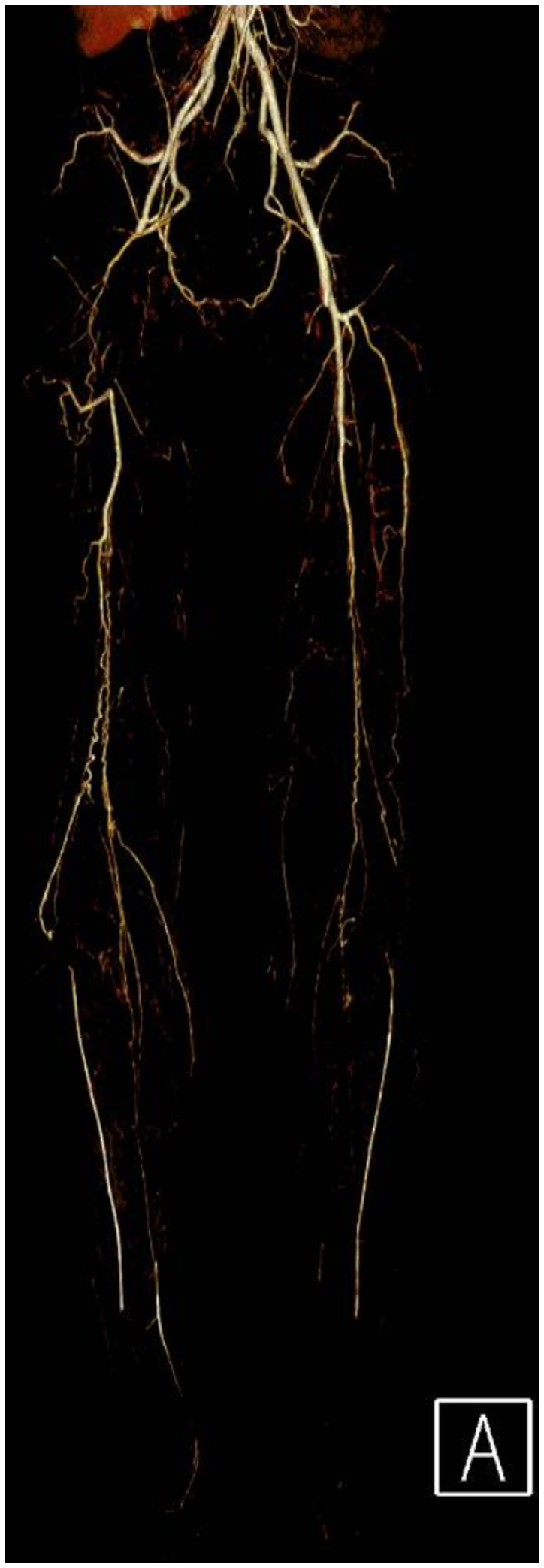
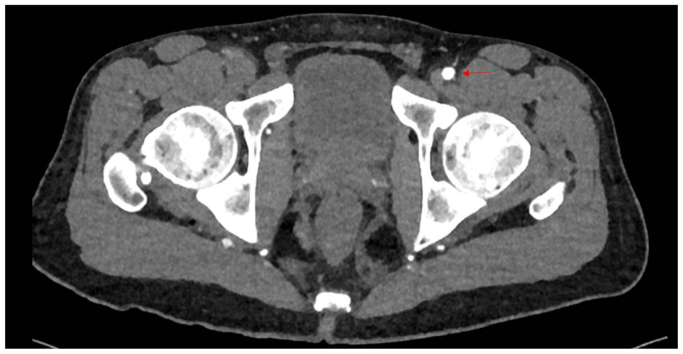
Clinical examination revealed non-palpable dorsalis pedis and posterior tibial pulses bilaterally. The lower extremities were warm, without sensory or motor deficits or evidence of tissue loss. Vascular studies demonstrated an ankle-brachial index of 0.36 on the right and 0.45 on the left. Subsequent workup including a computed tomographic angiography, and arterial duplex imaging revealed occlusion of the right common femoral and distal right superficial femoral arteries with reconstitution of tibial vessels. (Figs 1 and 2). The left lower extremity demonstrated a similar pattern of disease without the common femoral artery occlusion. Extensive workup of other possible etiologies for peripheral vascular disease, including hereditary thrombophilias and other vasculitic syndromes, was negative. Labs were notable for normal immunologic and inflammatory markers, a hemoglobin A1C of 5.7, and a normal lipid panel.
The patient received diet and exercise counseling and began taking low-dose aspirin and atorvastatin. He stopped using cannabis and started taking sertraline to address his anxiety. After 4 weeks of these interventions, he was able to exercise 6 days a week, walking for 30-minute intervals before claudicating. Repeat vascular studies at 4 months demonstrated an ankle-brachial index of 0.33 on the right and 0.45 on the left.
Discussion
TAO is a nonatherosclerotic inflammatory disease of distal small and medium-sized blood vessels, often presenting in young men with substantial tobacco use.ref. bib6 Cannabis arteritis is a contested disease entity that shares many of the same clinical features as TAO, although its presentation is likely confounded by concomitant tobacco exposure in almost all cases. These segmental lesions tend to present in the distal lower extremities and may be associated with distinct proximal lesions.ref. bib2 Although limited by the paucity of arterial biopsy data, the proposed pathophysiology of cannabis arteritis broadly relates to vasoconstriction and direct endothelial damage caused by delta-9-THC, the main psychoactive component of cannabis.ref. 7, ref. 8, ref. 9 Although delta-9-THC remains the focus of research efforts, it is also important to consider the toxicity of the products of combustion not only of the tobacco or cannabis, but also of the delivery method such as rolling papers.ref. bib4,ref. bib10
It is unclear if cannabis arteritis represents a subtype of TAO or a distinct clinical entity due to the predominance of concurrent tobacco and cannabis use in as many as 97% of cases reported in the literature.ref. bib2 Furthermore, many recorded substance use histories lack the detail necessary to identify other contributing sources of tobacco exposure, such as the cured tobacco leaves used in blunt wraps.ref. bib4 This case represents a rare instance in which there is minimal exposure to tobacco in both smoking history and “cross-contamination” of cannabis. This patient presented with extensive proximal lesions to the common and superficial femoral arteries and claudication without ischemic ulcerations, which is quite unusual for TAO and may better characterize the unique features of cannabis arteritis.ref. bib6,ref. bib11 To the authors’ knowledge, this also appears to be one of the first case reports linking THC vaping to cannabis arteritis.
This patient reports a 12-year history of habitual cannabis use, mainly by a water pipe or a dry pipe. In both cases, the user inhales delta-9-THC produced from combustion of the cannabis flower.ref. bib12 The patient denies mixing in tobacco products or using blunt wraps or rolling papers while smoking cannabis. Interestingly, the onset of symptoms began only in the most recent 2 to 3 years after the patient switched to vaping hash oil as the sole method of cannabis consumption. This method uses a heated coil to aerosolize highly concentrated delta-9-THC dissolved in liquid solvents such as propylene glycol and vegetable glycerin.ref. bib13 The potency of cannabis concentrates such as hash oil averages 50% but can soar up to 90% delta-9-THC compared with the 15% potency of traditional cannabis smoking.ref. bib12 This history suggests a dose-response relationship between delta-9-THC and cannabis arteritis without confounding exposure to tobacco or related combustion products, although exposure to additional products of vaporization should be taken into consideration. The scarcity of case reports of TAO-like arteritis with isolated cannabis use likely reflects a commonly occurring co-addiction in the population and, potentially, an additive or synergistic effect caused by concurrent cannabis and tobacco use.ref. bib14
The mainstay of treatment for TAO is smoking cessation, which is difficult for even the most compliant patients. The disease remains quiescent if patients can abstain from tobacco use.ref. bib6,ref. bib11 This patient with no recent tobacco exposure experienced marked symptomatic improvement with cannabis cessation along with the initiation of aspirin, a statin, and exercise. Notably, noninvasive testing at 4-month follow-up was unchanged, suggesting that the lesions in cannabis arteritis may primarily be inflammatory as opposed to vasospastic.
Conclusion
This case highlights the need for more detailed substance use histories to parse out relevant exposures as well as further exploration of the biological mechanisms involved in the pathophysiology of cannabis arteritis. Although there are still many unanswered questions surrounding cannabis arteritis, this case supports the hypothesis that delta-9-THC is an agent capable of causing a distinct TAO-like arteritis independent of tobacco exposure.
Disclosures
None.
References
- B. Noël, I. Ruf, R.G. Panizzon. Cannabis arteritis. J Am Acad Dermatol, 2008. [PubMed]
- O. Cottencin, L. Karila, M. Lambert. Cannabis arteritis: review of the literature. J Addiction Med, 2010
- Y. Banana, H. Bashir, S. Boukabous, A. Rezziki, A. Benzirar, O. El Mahi. Cannabis arteritis: a case report and brief review of the literature. Ann Med Surg (Lond), 2022
- E. Pilitsi, B. Kennamer, N. Trepanowski. Cannabis arteritis presenting with Raynaud’s and digital ulcerations: a case-based review of a controversial thromboangiitis obliterans-like condition. Clin Rheumatol, 2023. [PubMed]
- M. Sauvanier, J. Constans, S. Skopinski. [Lower limb occlusive arteriopathy: retrospective analysis of 73 patients with onset before the age of 50 years]. J Mal Vasc, 2002. [PubMed]
- J.W. Olin. Thromboangiitis obliterans (Buerger’s disease). N Engl J Med, 2000. [PubMed]
- R.T. Jones. Cardiovascular system effects of marijuana. J Clin Pharmacol, 2002. [PubMed]
- M. Adams, J. Earnhardt, W. Dewey, L. Harris. Vasoconstrictor actions of delta8-and delta9-tetrahydrocannabinol in the rat. J Pharmacol Exp Therapeut, 1976
- T.A. Sarafian, J.A.M. Magallanes, H. Shau, D. Tashkin, M.D. Roth. Oxidative stress produced by marijuana smoke: an adverse effect enhanced by cannabinoids. Am J Respir Cell Mol Biol, 1999. [PubMed]
- D.P. Tashkin. Smoked marijuana as a cause of lung injury. Monaldi Arch Chest Dis, 2005. [PubMed]
- J.W. Olin, J.R. Young, R.A. Graor, W.F. Ruschhaupt, J.R. Bartholomew. The changing clinical spectrum of thromboangiitis obliterans (Buerger’s disease). Circulation, 1990. [PubMed]
- D.S. Hasin, J. Borodovsky, D. Shmulewitz. Adult use of highly-potent Δ9-THC cannabis concentrate products by US state cannabis legalization status, 2021. Addict Behav, 2023
- A.B. Stefaniak, R.F. LeBouf, A.C. Ranpara, S.S. Leonard. Toxicology of flavoring-and cannabis-containing e-liquids used in electronic delivery systems. Pharmacol Ther, 2021
- A. Agrawal, A.J. Budney, M.T. Lynskey. The co-occurring use and misuse of cannabis and tobacco: a review. Addiction, 2012. [PubMed]