Sarcomatoid carcinoma of the common bile duct
Abstract
Rationale:
Sarcomatoid carcinoma is an extremely rare lesion in the common bile duct (CBD).
Patient concerns:
We present a case of sarcomatoid carcinoma of the distal CBD in a 51-year-old woman who presented with jaundice and abdominal pain. Whipple’s operation was performed successfully. Microscopically, the tumor was a poorly differentiated carcinoma containing a component of sarcoma-like differentiation. The tumor cells displayed spindle-shaped nuclei with occasional mitotic figures. Cytokeratin (CK) 7, CK19, CK18, and pan-CK (AE1/AE3) staining was positive on immunohistochemistry. Vimentin and carcinoembryonic antigen (CEA) staining were also positive.
Diagnoses:
Sarcomatoid carcinoma of the distal CBD.
Interventions:
The patient received three cycles of chemotherapy after surgery.
Outcomes:
The patient has experienced no adverse events in the 3 years post-surgery.
Lessons:
We present here a case report of sarcomatoid carcinoma of the distal CBD. The patient received chemotherapy after surgery, and was event-free for 3 years post-surgery, suggesting a relatively better prognosis, despite the infiltrative pattern of the tumor.
Article type: Case Report
Keywords: chemotherapy, common bile duct, cytokeratin, pancreaticoduodenectomy, pathology, sarcomatoid carcinoma, Vimentin
Affiliations: Department of Abdominal Surgical Oncology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College; Department of Pathology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College; Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
License: Copyright © 2017 the Author(s). Published by Wolters Kluwer Health, Inc. CC BY-ND 4.0 This is an open access article distributed under the Creative Commons Attribution-NoDerivatives License 4.0, which allows for redistribution, commercial and non-commercial, as long as it is passed along unchanged and in whole, with credit to the author. http://creativecommons.org/licenses/by-nd/4.0
Article links: DOI: 10.1097/MD.0000000000005751 | PubMed: 28099333 | PMC: PMC5279078
Relevance: Relevant: mentioned in keywords or abstract
Full text: PDF (1019 KB)
Introduction
Sarcomatoid carcinoma, which is characterized by poorly differentiated carcinoma tissue containing a component of sarcoma-like (spindle and/or giant cell) differentiation, is a rare malignant tumor in the gastrointestinal tract and hepatobiliary-pancreatic system.[1] Sarcomatoid carcinomas have been found at diverse sites including the liver,[2,3] gallbladder,[4–6] pancreas,[7–9] and ampulla of Vater.[10] Case reports of sarcomatoid carcinoma arising in the common bile duct (CBD) are extremely rare. To our knowledge, only 2 cases of sarcomatoid carcinoma of the CBD have been reported.[1,11] Here, we present an additional case and a review of the relevant literature.
Case report
In May 2013, a 51-year-old woman was admitted to our hospital with jaundice, abdominal pain, and weight loss over the course of 2 weeks. Physical examination revealed icteric sclera and mild epigastric pain. The patient had a history of hepatitis B for more than 10 years without regular treatment, although her liver function had previously been normal. An uncle of the patient had died of liver cancer; however, other family histories were unremarkable.
The liver function tests revealed increased alanine aminotransferase (53 U/L), γ-glutamyl transferase (143 U/L), and alkaline phosphatase (186 U/L) levels. Total, direct, and indirect bilirubin levels were elevated to 240.3, 179.7, and 60.6 mmol/L, respectively. Routine urine analysis revealed increased urobilinogen (4 mg/dL) and urine bilirubin (6 mg/dL) levels. Other routine laboratory tests including complete blood count, renal function test, and electrolytes test were unremarkable. The serum levels of carcinoembryonic antigen (CEA) and carbohydrate antigen 242 were within the normal reference range, but the carbohydrate antigen 19-9 levels were increased (99.55 U/mL).
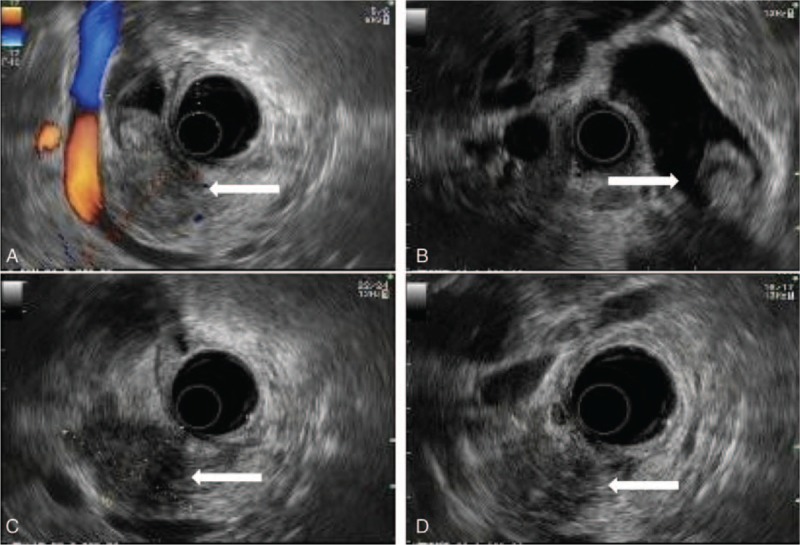
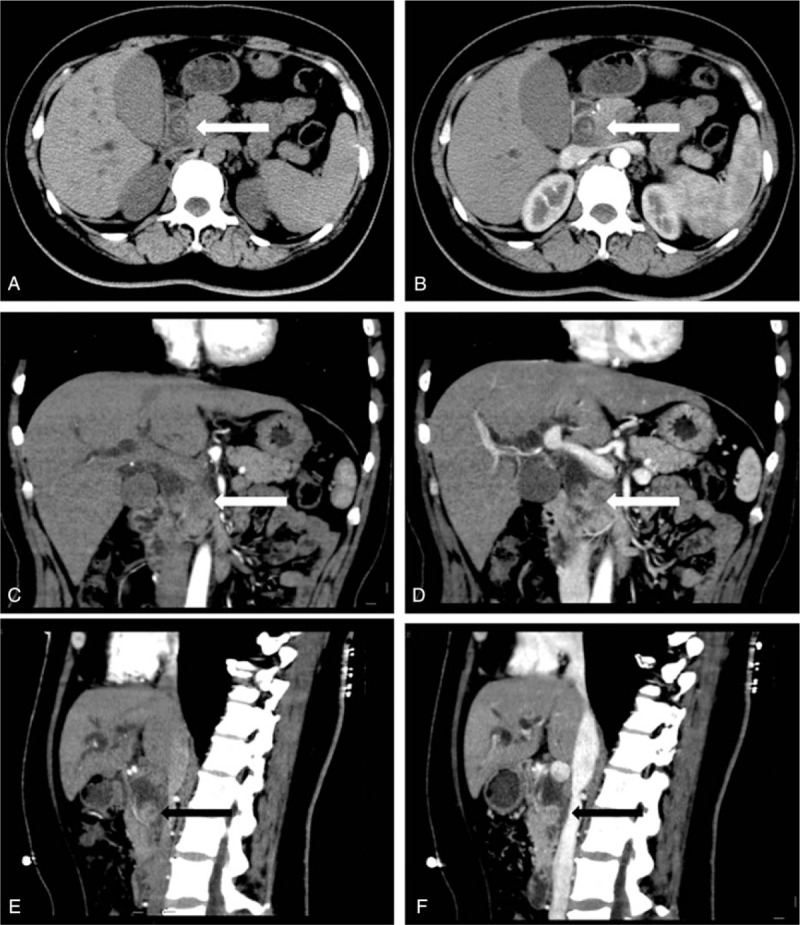
The endoscopic ultrasonography and abdominal computed tomography scans prior to surgery displayed a mass measuring 4.0 × 3.5 cm located in the distal CBD, which had penetrated from the bile duct to the pancreas, with the presence of marked dilatation of the proximal CBD, gallbladder, and right and left common hepatic and intrahepatic ducts (Figs. 1 and 2). No lymphadenopathy was noted in the upper abdomen.
Pancreaticoduodenectomy (Whipple operation) was performed successfully. Intraoperative findings included a mass measuring 3.8 × 3.3 × 2.6 cm located in the distal part of the CBD. The mass penetrated the bile duct and involved the surrounding pancreatic parenchyma. The interior of the tumor was gray-whitish and displayed focal hemorrhages and necrosis. No lymphadenopathy was found in the peripancreatic soft tissue.
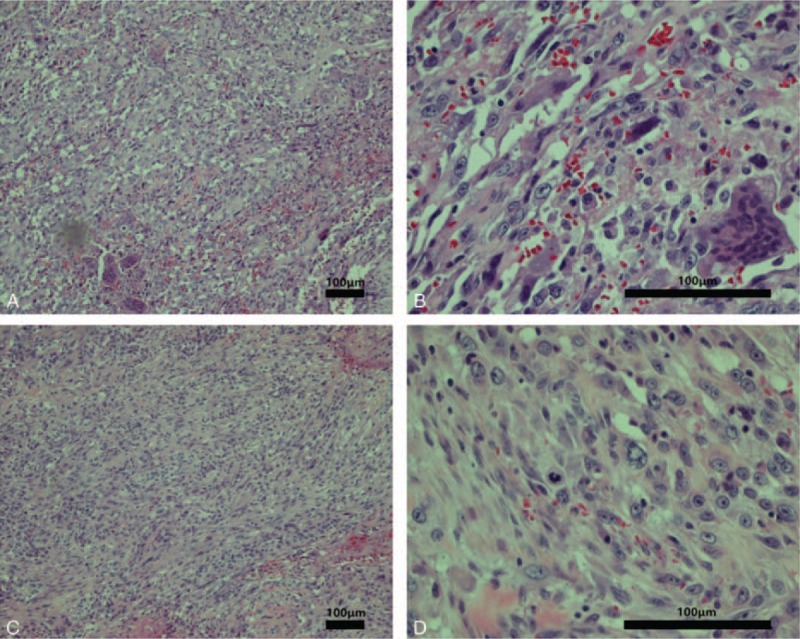
Microscopically, the tumor was a poorly differentiated carcinoma containing a component of sarcoma-like (spindle and/or giant cell) differentiation (Fig. 3). Adenoid structures were visible in the focal area. The tumor cells had spindle-shaped nuclei with occasional mitotic figures forming bundles and whirls. Oval and epithelioid cells were also present, and giant cells, including multinucleated cells and tumor giant cells, were visible in the focal section. There were also necrotic regions within the focal section. No heterologous sarcomatous elements were identified. No metastasis was found in the regional lymph nodes.
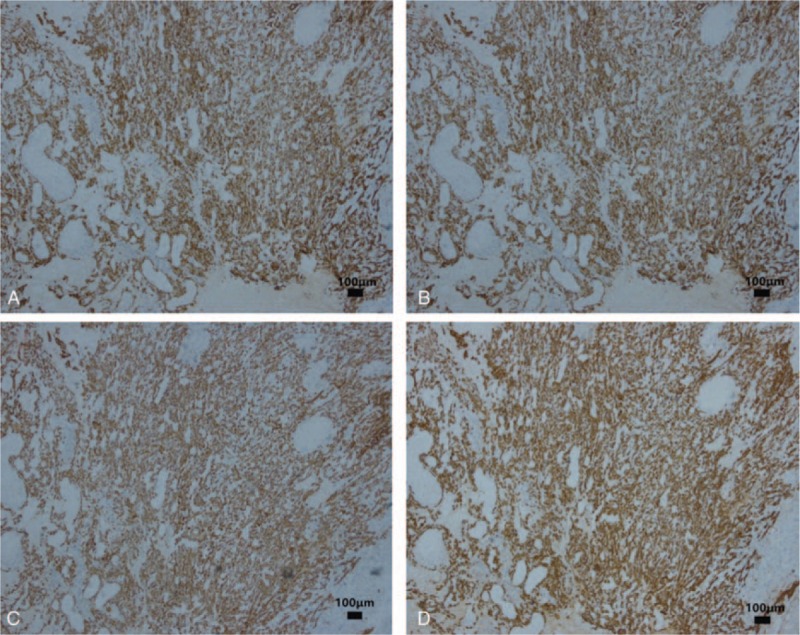
On immunohistochemistry, the sample was positive for several cytokeratins (CKs), including CK7 (Fig. 4A), CK19 (Fig. 4B), CK18, and pan-CK (AE1/AE3) (Fig. 4C). Immunohistochemistry also showed Vimentin and CEA staining (Fig. 4D). The sample was negative for smooth muscle actin, desmin, myoglobin, and S-100 protein.
Two months after surgery, the patient received three 21-day cycles of chemotherapy. Cisplatin 40 mg/m2 was administrated intravenously on days 1 and 2, with gemcitabine 1000 mg/m2 on days 1 and 8. Drug-related toxic effects of the chemotherapy included mild gastrointestinal reactions and bone marrow depression. As of 3 years postsurgery, the patient shows no signs of recurrence.
Because this report just reviewed previous data and did not involve any human trials, there is no need to conduct special ethic review, and the ethical approval is not necessary. Informed consent was provided by the patient for the publication of the case report.
Discussion
Sarcomatoid carcinoma is characterized by poorly differentiated carcinoma tissue containing a component of sarcoma-like differentiation without any heterologous sarcomatous elements.[1] Sarcomatoid carcinoma is an extremely rare malignant tumor in the hepatobiliary-pancreatic system, which has been found in the liver,[2,3] gallbladder,[4–6] pancreas,[7–9] and ampulla of Vater.[10]
To our knowledge, only 2 cases of sarcomatoid carcinoma of the CBD have been reported.[1,11] The clinicopathologic features of the present case and former cases are summarized in Table 1.
Table 1: Clinicopathological features of 3 cases of sarcomatoid carcinoma of the CBD.

The patient reported by Yoon et al[1] was a 78-year-old male. The tumor, which measured 4 cm in the greatest dimension, arose in the mid CBD, and was infiltrative. Of 22 regional lymph nodes, 2 were metastatic. The patient died of cardiac problem 5 days postsurgery. Another case was reported by Jang et al. The patient was a 68-year-old female. The tumor, which measured 3.5 cm at the greatest dimension, was located in the distal CBD. The growth pattern of the tumor was polypoid, and there was no lymphadenopathy. The patient showed no recurrence 1 year after treatment. Our patient was a 51-year-old female with a tumor located in the distal CBD. The infiltrative growing mass measured 3.8 × 3.3 × 2.6 cm. No metastatic lymph nodes or distant metastases were discovered. The patient received chemotherapy after surgery and remains event-free after 3 years.
The histogenesis or underlying cause of sarcomatoid carcinoma remains unclear, although 3 major theories have been suggested.[10] Sarcomatoid carcinoma can arise from the metaplastic change of carcinomatous cells to sarcomatous cells. Alternatively, sarcomatoid carcinoma may be generated from a single multipotent uncommitted reserve cell with the capacity for divergent differentiation. Another hypothesis is that sarcomatoid carcinoma is the result of separate but concurrent malignant proliferation of epithelial and stromal elements.
Our case appears to be in agreement with the first theory. Owing to the expression pattern of CK and other markers, and the coexpression of CK and Vimentin, the sarcomatoid cells may be carcinoma cells with sarcomatoid differentiation or metaplastic carcinoma. As no heterologous sarcomatous elements were found, we used the term of “sarcomatoid carcinoma” instead of “carcinosarcoma.”
There is no survival data for sarcomatoid carcinoma of the CBD. Based on previously reported behavior and survival figures on sarcomatoid carcinoma of other organs, such as the gallbladder,[4–6] sarcomatoid carcinomas are locally invasive and metastasize systemically, with the prognosis resembling carcinoma. An attempt to remove the tumor should be a top priority. Yoon et al[1] suggested that the poor prognosis of sarcomatoid carcinoma of the CBD is partly due to diffuse tumor infiltration, resulting in diffuse thickening and narrowing of the CBD. Additionally, the pathological finding of regional metastatic lymph nodes supports the aggressive behavior of sarcomatoid carcinoma of the CBD. However, Jang et al[11] suggested that tumors in the CBD may have a better prognosis owing to their polypoid nature. A polypoid tumor in the CBD could easily lead to early obstruction of the bile duct and symptoms of jaundice, resulting in early diagnosis and resection of the tumor, achieving clearance before the tumor spreads.
Our patient received chemotherapy after surgery, and was event-free for 3 years postsurgery, suggesting a relatively better prognosis, despite the infiltrative pattern of the tumor.
References
- GS Yoon, DL Choi. Sarcomatoid carcinoma of common bile duct: a case report.. Hepatogastroenterology, 2004. [PubMed]
- Q Leng, XI Xiang, Y Tang. Primary hepatic sarcomatoid carcinoma: a case report.. Exp Ther Med, 2015. [PubMed]
- JW Lee, MW Kim, NK Choi. Double primary hepatic cancer (sarcomatoid carcinoma and hepatocellular carcinoma): a case report.. Mol Clin Oncol, 2014. [PubMed]
- A Dong, H Dong, W Jing. FDG PET/CT in sarcomatoid carcinoma of the gallbladder with chondroid differentiation.. Clin Nucl Med, 2016. [PubMed]
- DC Doval, S Azam, A Mehta. A report of sarcomatoid carcinoma of the gallbladder treated with palliative deocetaxel and gemcitabine chemotherapy.. J Gastrointest Cancer, 2014. [PubMed]
- K Kataria, R Yadav, V Seenu. Sarcomatoid carcinoma of the gall bladder.. J Surg Case Rep, 2012
- JR Kane, WB Laskin, KA Matkowskyj. (Spindle cell) carcinoma of the pancreas: a case report and review of the literature.. Oncol Lett, 2014. [PubMed]
- CL Ren, P Jin, CX Han. Unusual early-stage pancreatic sarcomatoid carcinoma.. World J Gastroenterol, 2013. [PubMed]
- J Yao, JJ Qian, CR Zhu. Laparoscopic left pancreatectomy for pancreatic sarcomatoid carcinoma: a case report and review of the literature.. Oncol Lett, 2013. [PubMed]
- JG Kench, DJ Frommer. Sarcomatoid carcinoma of the ampulla of Vater.. Pathology, 1997. [PubMed]
- KS Jang, SH Jang, YH Oh. Sarcomatoid carcinoma of the distal common bile duct: a case report.. Korean J Pathol, 2005