
Prevalence Rates, Perceptions of Risk, and Motivations for Nonmedical Cannabis Use in Pediatric Pain
Abstract
This cross-sectional study evaluates cannabis use rates, risk perceptions, and motivations for use among treatment-seeking youths with diagnosed pain disorders.
Affiliations: Department of Anesthesiology, Critical Care, and Pain Medicine, Boston Children’s Hospital, Boston, Massachusetts; Department of Anesthesia, Harvard Medical School, Boston, Massachusetts; Division of Sleep Medicine, Harvard Medical School, Boston, Massachusetts; Department of Psychology, Endicott College, Beverly, Massachusetts; Institute for Implementation Science in Health Care, University of Zürich, Zürich, Switzerland; Division of Addiction Medicine, Boston Children’s Hospital, Boston, Massachusetts; Division of Adolescent and Young Adult Medicine, Boston Children’s Hospital, Boston, Massachusetts; Department of Pediatrics, Harvard Medical School, Boston, Massachusetts; Computational Health Informatics Program, Boston Children’s Hospital, Boston, Massachusetts
License: Copyright 2025 Kossowsky J et al. JAMA Network Open. CC BY 4.0 This is an open access article distributed under the terms of the CC-BY License.
Article links: DOI: 10.1001/jamanetworkopen.2025.12870 | PubMed: 40440015 | PMC: PMC12123470
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (14 KB)
Introduction
Pediatric pain affects nearly 40% of youths globally1,2,3 and is associated with functional impairment,4 comorbid internalizing disorders,5 interpersonal stressors,6 and other lifestyle disruptions, including sleep disturbance.7,8 Among adolescents without pain disorders, these challenges often correlate with increased cannabis use (CU),9,10,11,12 the second most common psychotropic substance among US adolescents.13 In pediatric pain samples, CU prevalence is less established.
In adults with pain, CU rates are high.14,15,16,17 The main phytocannabinoids found in cannabis are delta 9-tetrahydrocannabinol (THC) and cannabidiol (CBD).18 THC is the primary psychoactive compound and is linked to potential adverse effects, including anxiety, addiction, and psychosis. In contrast, CBD is nonpsychoactive and has a relatively high toxicity threshold.18 Adults with CU or other substance use disorders are more likely to report pain than those without such disorders.19 Theoretical models explaining the high co-occurrence of pain and substance use suggest pathways of bidirectional reinforcement, whereby pain and substance use each reciprocally increase longitudinal risk for and exacerbation of the other.20 Adults with chronic pain often report CU to relieve pain,21,22 yet such instrumental use (IU) may worsen pain and substance use over time.20 In adults, meta-analytical findings indicate that cannabis has minimal effects on pain control,23,24 no significant impact on sleep,24 and may exacerbate anxiety25 compared with placebo.
Prior work shows that CU is more likely in youths with chronic medical conditions as compared with healthy peers.26 Many of these youths also report cannabis IU to manage pain and other discomfort.27,28 Studies in nationally representative youth samples have found that increased pain is associated with increases in substance use.29,30,31 To the authors’ knowledge, though, no study to date has investigated CU and IU rates in treatment-seeking youths with chronic pain.
Characterizing CU rates in pediatric pain is critical, as adolescence marks a developmental window of increased substance use risk32 and negative outcomes,33 like impaired cognitive function,34 increased suicide risk,35,36 and poor sleep.35 Recent work indicates age-dependent associations between CU and psychosis, particularly during adolescence, highlighting the vulnerability of this development stage.37,38 Understanding why youths with pain engage in CU or IU can guide interventions toward more adaptive coping skills. The current survey study aims to examine CU rates, risk perceptions, and motivations for use or abstinence in a treatment-seeking sample of youths with diagnosed pain disorders. We also explored differences in these variables across different subgroups (eg, youth with CU vs no CU and youths with IU vs no IU). We hypothesized that youths who report IU perceive cannabis as less harmful than youths with no CU and no IU, which, to some extent, may explain their increased CU.
Methods
Participants and Procedures
Participants were recruited from a pediatric pain clinic in the Northeast US, in a state where both medical and recreational cannabis use are legal for adults aged 21 years and older. This study occurred from September 2021 to May 2024. A sample size of 200 was calculated to detect small-to-moderate differences (d = 0.4, α = 0.05, power = 0.8) between cannabis users (estimated 25% prevalence) and nonusers. To account for potential nonresponses, 312 patients were approached, 251 enrolled, and 245 completed surveys. Participants aged 14 to 19 years receiving treatment for diagnosed chronic pain conditions (headache or migraine, whole-body pain, joint pain, or neuropathic pain) were eligible. Exclusion criteria included severe cognitive impairment or inability to respond to questions in English. Eligible patients were identified weekly from clinic schedules and recruited via phone, email, mail, secure patient portal, or in-person. Participants and their guardians provided informed consent or assent. Surveys were administered securely online via REDcap.39,40 Participants received a $20 gift card. The study was approved by the Boston Children’s Hospital institutional review board and adheres to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
Measures
Demographics
Demographic questions assessed participant’s age, grade, race (American Indian, Asian, Black, White, and other or multiple races), ethnicity (Hispanic or Latino, not Hispanic or Latino, or prefer not to answer), and self-reported gender. Race and ethnicity were assessed in this study because of previously documented differences in youth cannabis use in different racial and ethnic groups.41
Pain
Participants completed the Numerical Rating Scale42 to assess mean pain intensity on a 0 to 10 scale (0 = no pain to 10 = worst pain imaginable), and the Pain Frequency and Duration Scale43 to characterize pain symptoms experienced over the past 2 weeks. Participants also completed the 8-item Patient Reported Outcomes Measurement Information System Pain Interference scale,44 which measures pain-related disruptions across multiple life domains, and has demonstrated good reliability and validity in youths45 and adults.46 Participants indicate the degree to which pain hinders both physical and psychosocial functioning in certain activities (1, never; 2, almost never; 3, sometimes; 4, often; or 5, almost always). Participants completed pediatric (<18 years) or adult (≥18 years) versions of this measure. Summed raw scores were converted into t scores, with higher scores indicating greater pain interference. Reliability was excellent (Cronbach α= 0.86 pediatric; 0.95 adult).
Participants also completed the 15-item Functional Disability Inventory,47 which assesses perceived difficulty completing physical activities in school, home, or recreational settings (0, no trouble; 1, a little trouble; 2, some trouble; 3, a lot of trouble; or 4, impossible). Raw scores were summed to a total score (0-60). Higher scores indicate greater functional pain disability. Cronbach α was 0.91, suggesting excellent reliability.
Cannabis Use
Participants were asked whether they had used cannabis at any point in their lifetime, in the past year, and in the past month, and to specify their age at first use. Those who endorsed CU then completed items regarding frequency, motives, perceived risks, beliefs, and likelihood of future use. Items were selected and combined from several validated self-report questionnaires.48,49 Further information is in eAppendix 1 in Supplement 1.
Frequency
Participants estimated the number of CU occasions (0 to ≥40) over their lifetime, past year, past month, and on a typical day. Participants with CU specified their most frequent methods of cannabis ingestion (eg, joints, hookah, edibles, and so forth). See eAppendix 2 in Supplement 1 for a sample question.
Motivations
Participants with CU reported (yes vs no) whether alleviating physical or psychological symptoms motivated their use (ie, IU). If endorsed, participants identified such symptoms (eg, pain, nausea, anxiety, and so forth). Participants endorsed (yes vs no) whether their CU was upon a physician’s recommendation (ie, medical marijuana). Participants also reported how frequently they used cannabis instead of alcohol for pain (1, never; 2, rarely; 3, sometimes; 4, often; or 5, all the time).
Adverse Effects, Importance of Risks, and Likelihood of Future Use
Participants with CU reported past-year frequency of hallucinations, anxiety, or paranoia during or after CU (1, never; 2, once or twice; 3, sometimes; 4, often). Participants without CU indicated the extent to which CU risks were important to them (1, not at all; 2, somewhat; or 3, very important) including psychological or physical damage, addiction, and financial expense. Participants with CU reported their estimated likelihood of future CU in the next 30 days and the next year (1, definitely will; 2, probably will; 3, probably will not; or 4, definitely will not).
Beliefs
All participants reported their and their parents’ beliefs regarding riskiness of regular CU (1, risk; 2, slight risk; 3, moderate risk; 4, great risk; or 5, unsure risk). All participants also reported the extent to which they agreed or disagreed (1, strongly disagree; 2, disagree; 3, neither agree nor disagree; 4, agree; or 5, strongly agree) with commonly held cannabis beliefs (eg, “Cannabis can be addictive”).
Statistical Analysis
Python version 3.8.20 (Python Software Foundation) was used for descriptive analyses of demographic, pain, and CU variables and for inferential statistics. Independent t tests compared age, pain intensity, number of pain days, functional disability, and pain interference variables between participants with CU vs no CU, and between those with IU vs no IU. Monte Carlo χ2 tests compared gender, race, ethnicity, and pain characteristics across groups. Beliefs response categories were grouped with “strongly agree” and “agree” combined and “neither agree nor disagree,” “disagree,” and “strongly disagree” combined. Risk perception responses were categorized into low risk (“no risk” and “slight risk”) and higher risk (“moderate risk” and “great risk”). χ2 tests were conducted for these categorical comparisons. Pairwise deletion was applied for missing data, which accounted for 1.59% of responses. A 2-sided P value less than .05 was considered significant.
Results
The total sample consisted of 251 adolescents (mean [SD] age 16.9 [1.4] years; 168 [68.6%] female; 1 [0.4%] American Indian, 3 [1.2%] Asian, 3 [1.2%] Black, 19 [7.8%] Hispanic or Latino, and 201 [82.1%] White) with diagnosed pain disorders; 245 (97.6%) provided complete data and were included in the final analysis. Of 312 eligible patients approached, 40 did not complete the survey, and 4 were excluded from the analysis due to being either out of study age range, scam person, or a test participant. Our sample did not differ significantly in age or gender from the pediatric chronic pain population seen at the hospital where data were collected (Table 1).
Table 1. : Participant’s Cannabis Use (CU) Characteristicsa
| Characteristic | Participants, No. (%) | P valuezoi250425t1n2 | Participants, No. (%) | P valuezoi250425t1n3 | |||
|---|---|---|---|---|---|---|---|
| Total sample (N = 245) | No CU (n = 183) | Total lifetime CU (n = 183) | Within CU group | ||||
| IU (n = 48) | No IU (n = 14) | ||||||
| Demographics | |||||||
| Age, mean (SD), y | 16.91 (1.42) | 16.7 (1.4) | 17.6 (1.2) | <.001zoi250425t1n4 | 17.4 (1.2) | 18.1 (1) | .04zoi250425t1n4 |
| Self-reported gender | |||||||
| Female | 168 (68.6) | 132 (72.1) | 36 (58.1) | .03zoi250425t1n4 | 23 (47.9) | 13 (92.9) | .05 |
| Male | 36 (14.7) | 24 (13.1) | 12 (19.4) | 11 (22.9) | 1 (7.1) | ||
| Nonbinary | 25 (10.2) | 13 (7.1) | 12 (19.4) | 12 (25.0) | 0 | ||
| Prefer not to answer | 7 (2.8) | 6 (3.3) | 1 (1.6) | 1 (2.1) | 0 | ||
| Prefer to self-describe | 9 (3.7) | 8 (4.4) | 1 (1.6) | 1 (2.1) | 0 | ||
| Ethnicity | |||||||
| Hispanic or Latino | 19 (7.8) | 13 (7.1) | 6 (9.7) | .57 | 5 (10.4) | 1 (6.2) | .80 |
| Not Hispanic or Latino | 224 (91.4) | 169 (92.3) | 55 (88.7) | 13 (92.9) | 42 (87.5) | ||
| Prefer not to answer | 1 (0.8) | 1 (0.5) | 1 (1.6) | 1 (2.1) | 0 | ||
| Race | |||||||
| American Indian | 1 (0.4) | 0 | 1 (1.6) | .12 | 0 | 1 (7.1) | .05 |
| Asian | 3 (1.2) | 1 (0.6) | 2 (3.2) | 2 (4.2) | 0 | ||
| Black | 3 (1.2) | 3 (1.6) | 0 | 0 | 0 | ||
| White | 201 (82.1) | 153 (83.6) | 48 (77.4) | 35 (72.9) | 13 (92.9) | ||
| Other or multiple races | 37 (15.1) | 26 (14.2) | 11 (17.8) | 11 (22.9) | 0 | ||
| Pain characteristics, mean (SD) | |||||||
| Pain days in the last 2 wk | 11.8 (3.7) | 11.8 (3.7) | 11.9 (3.3) | .76 | 12.0 (2.7) | 10.4 (4.6) | .14 |
| Usual pain intensity | 5.5 (1.7) | 5.6 (1.8) | 5.3 (1.5) | .16 | 5.3 (1.5) | 5.4 (1.4) | .65 |
| Worst pain intensity | 7.8 (1.7) | 7.9 (1.7) | 7.7 (1.7) | .46 | 7.7 (1.5) | 7.1 (2.2) | .20 |
| Functional disability | 23.9 (11.5) | 23.4 (12.1) | 25.5 (9.6) | .18 | 27.4 (8.7) | 19.0 (10.2) | .01zoi250425t1n4 |
| Pain interference pediatric (n = 177)zoi250425t1n5 | 60.0 (7.3) | 59.6 (7.7) | 62.3 (4.5) | .01zoi250425t1n4 | 61.8 (4.8) | 61.8 (2.5) | .67 |
| Pain interference adults (n = 66)zoi250425t1n5 | 60.0 (8.1) | 59.2 (8.3) | 61.8 (7) | .12 | 62.6 (4.2) | 58.9 (10.3) | .25 |
| Pain regularity | |||||||
| Recurrent | 66 (26.3) | 50 (27.3) | 16 (25.8) | .74 | 11 (22.9) | 5 (35.7) | .33 |
| Continuous | 180 (71.7) | 129 (70.5) | 46 (74.2) | 37 (77.1) | 9 (64.3) | ||
| Psychological characteristics, t score, mean (SD) | |||||||
| Depressive symptoms pediatric | 56.9 (11.6) | 55.6 (12.0) | 61.8 (8.3) | <.001zoi250425t1n4 | 63.1 (7.4) | 54.9 (10.6) | .12 |
| Depressive symptoms adults | 55.6 (9.2) | 54.9 (9.7) | 56.6 (8.4) | .46 | 58.8 (7.4) | 52.1 (8.9) | .07 |
| Anxiety pediatric | 56.5 (11.5) | 56.0 (11.7) | 58.5 (10.5) | .22 | 58.5 (10.9) | 58.5 (9.0) | >.99 |
| Anxiety adult | 57.4 (10.3) | 56.0 (11.6) | 59.4 (7.9) | .15 | 61.4 (7.0) | 55.6 (8.6) | .10 |
Comparisons between CU and no CU groups reflect differences within the full sample. Comparisons between IU and no IU groups reflect differences within cannabis users. Percentages in IU and no IU columns are based on lifetime cannabis users (62 participants), not the full sample. Overall IU prevalence in the full sample is 19.6% (48 of 245 participants).
P values represent differences between CU and No CU groups.
P values represent differences between IU and No IU groups.
Indicates significance.
Indicates t scores.
Abbreviation: IU, instrumental use.
Group Differences of Participant Characteristics
Participants with CU were older (mean difference, 0.9 years; 95% CI, 0.5 to 1.2 years; P < .001) and included fewer female participants (difference, −14.0%; 95% CI, −32.6% to −2.9%; P = .03) compared with those without CU. The pediatric CU group reported higher pain interference scores (mean difference, 2.7; 95% CI, 0.8 to 4.6; P = .01) and higher depressive symptoms scores (mean difference, 6.2; 95% CI, 2.8 to 9.5; P < .001) than the no CU group. Participants with IU were younger (mean difference, −0.7 years; 95% CI, −1.3 to −0.1 years; P = .04) and reported significantly higher functional disability scores (mean difference, 8.4; 95% CI, 2.1 to 12.6; P = .01) compared with those with no IU. No other significant differences emerged between CU vs no CU or IU vs no IU groups (Table 1).
Cannabis Use (CU)
Participant lifetime CU was 62 of 245 participants (25.3%), and age of first CU ranged from 7 to 19 years (mean [SD] age, 15.3 [1.9] years). Prevalence rates for past year and past month were 22.9% (56 of 245 participants) and 16.3% (40 of 245 participants), respectively. Among those endorsing CU, past-year prevalence was 90.2% (56 of 62 participants) and past-month prevalence was 64.5% (40 of 62 participants).
Frequency
Frequency of CU ranged from 0 to more than 40 occasions. For lifetime use, median use was 6 to 9 occasions, with most participants endorsing use on either 3 to 5 occasions (15 of 62 participants [24.2%]) or on more than 40 occasions (16 of 62 participants [25.8%]). Median use over the past year was 6 to 9 occasions, and most participants endorsed use on 3 to 5 occasions (15 of 62 participants [24.2%]). Over the past month, median use was 0 occasions, and most participants reported either 0 (22 of 62 participants [35.5%]) or 1 to 2 occasions of use (19 of 62 participants [30.6%]). On a typical day of cannabis use, 56 of 62 participants (90.3%) reported using 1 to 2 times.
Preferred methods for ingesting cannabis were edibles (32 of 62 participants [51.6%]), vaporizer (28 of 62 participants [45.2%]), joints (27 of 62 participants [43.5%]), bong (15 of 62 participants [24.2%]), blunts (8 of 62 participants [12.9%]), and hand pipe (8 of 62 participants [12.9%]) (see eTable in Supplement 1 for additional information). The primary form of CU varied, with 37 of 62 participants (59.7%) endorsing marijuana with high THC content, 24 of 62 (38.7%) endorsing edibles, 20 of 62 (32.3%) endorsing marijuana with high CBD content, 9 of 62 (14.5%) endorsing concentrates, and 2 of 62 (3.2%) endorsing other unspecified methods.
Adverse Experiences
Participants reported experiencing hallucinations never (51 of 62 participants [82.3%]), once or twice (8 of 62 participants [12.9%]), sometimes (1 of 62 participants [1.6%]), or often (2 of 62 participants [3.2%]). They reported anxiety or paranoia never (47 of 62 participants [75.8%]), once or twice (11 of 62 participants [17.7%]), sometimes (3 of 62 participants [4.8%]), or often (1 of 62 participants [1.6%]) during or after CU over the past year.
Motivations for Use and Nonuse
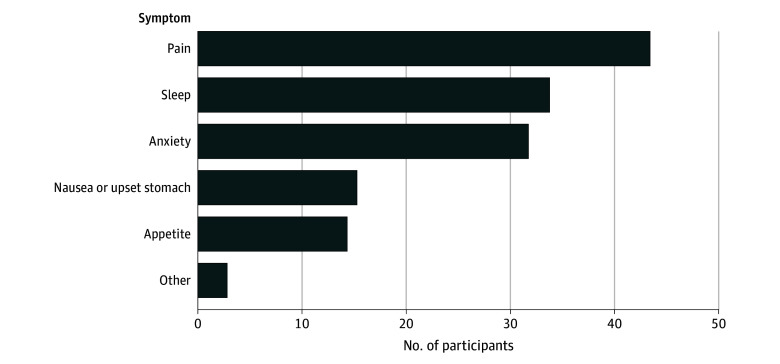
Rates of CU to alleviate physical or psychological symptoms were 77.4% (48 of 62 participants), with 93.8% (45 of 48 participants) endorsing use for pain, 72.9% (35 of 48 participants) for sleep, 68.8% (33 of 48 participants) for anxiety, 33.3% (16 of 48 participants) for nausea, 31.3% (15 of 48 participants) for appetite, and 6.3% (3 of 48 participants) for other unspecified symptoms. The overall IU prevalence was 19.6% (48 of 245 participants) in the full sample, highlighting that nearly 1 in 5 youths with pain reported CU specifically for symptom relief (Figure).
Also, 7 of 62 participants (11.3%) endorsed current medical CU, indicating their CU was upon a physician’s recommendation, and 1 of 62 (1.6%) endorsed medical CU in the past. Participants indicated how often they chose cannabis over alcohol because they perceived alcohol to worsen their pain: 34 of 62 participants (54.8%) chose never, 5 of 62 (8.1%) chose rarely, 4 of 62 (6.5%) chose sometimes, 8 of 62 (12.9%) chose often, and 11 of 62 (17.7%) chose all the time.
Participants with no CU reported the extent to which cannabis-associated risks were important to them (Table 2). More than 50% reported the following possible negative consequences to be very important to them: becoming addicted (117 of 183 participants [63.9%]), physical damage (109 of 183 participants [59.6%]), leading to stronger drugs (103 of 183 participants [56.3%]), don’t feel like getting high (102 of 183 participants [55.7%]), losing control (101 of 183 participants [55.2%]), psychological damage (100 of 183 participants [54.6%]), and parents would disapprove (92 of 183 participants [50.3%]).
Table 2. : Stated Reasons for Not Using Cannabis (N = 183)
| Reason | Participants, No. (%) | ||
|---|---|---|---|
| Not at all important | Somewhat important | Very important | |
| Concerned about psychological damage | 33 (18) | 50 (27.3) | 100 (54.6) |
| Concerned about physical damage | 34 (18.6) | 40 (21.9) | 109 (59.6) |
| Concerned about getting arrested | 47 (25.7) | 55 (30.1) | 81 (44.3) |
| Concerned about becoming addicted | 27 (14.8) | 39 (21.3) | 117 (63.9) |
| It’s against my beliefs | 98 (53.6) | 33 (18) | 52 (28.4) |
| Concerned about loss of energy or ambition | 51 (27.9) | 62 (33.9) | 70 (38.3) |
| Concerned about possible loss of control of myself | 37 (20.2) | 45 (24.6) | 101 (55.2) |
| It might lead to stronger drugs | 41 (22.4) | 39 (21.3) | 103 (56.3) |
| Not enjoyable, I wouldn’t like it | 51 (27.9) | 50 (27.3) | 82 (44.8) |
| My parents would disapprove | 45 (24.6) | 46 (25.1) | 92 (50.3) |
| My boyfriend/girlfriend would disapprove | 116 (63.4) | 18 (9.8) | 49 (26.8) |
| I wouldn’t like being with the people who use it | 72 (39.3) | 41 (22.4) | 70 (38.3) |
| My friends don’t use it | 79 (43.2) | 48 (26.2) | 56 (30.6) |
| Too expensive | 94 (51.4) | 43 (23.5) | 46 (25.1) |
| Not available | 117 (63.9) | 36 (19.7) | 30 (16.4) |
| Don’t feel like getting high | 35 (19.1) | 46 (25.1) | 102 (55.7) |
Cannabis-Related Beliefs and Risk-Perception
Results of χ2 tests indicated participants with CU endorsed more agreement with the belief that “cannabis is safe because it is natural” (odds ratio [OR], 2.76; 95% CI, 1.48-5.12: P = .001) compared with participants with no CU. Participants with no CU indicated more agreement with the belief that “cannabis can be addictive” (OR, 0.28; 95% CI, 0.13-0.64; P = .003) and “using cannabis can make my medical condition worse” (OR, 0.17; 95% CI, 0.09-0.33; P < .001). No other significant differences emerged in cannabis-related beliefs between the IU and no IU groups. (see Table 3). Overall, most participants reported they believed regular CU would carry slight (64 of 244 participants [26.2%]) or moderate (64 of 244 participants [26.2%]) risk. Most participants further reported their parent or guardian would believe that regular CU would harm their (ie, participants’) health (162 of 244 participants [66.4%]) vs help their health (36 of 244 participants [14.8%]) or have no impact (46 of 244 participants [18.9%]). Similarly, χ2 tests showed that participants with no CU reported higher perceived risk of CU compared with those with CU (OR, 2.37; 95% CI, 1.28-4.39; P = .01). No other significant differences in perceived CU risks between the IU and no IU groups.
Table 3. : Beliefs About Cannabis Use (CU)
| Belief | Participants, No. (%) | P valuezoi250425t3n1 | Participants, No. (%) | P valuezoi250425t3n2 | |||
|---|---|---|---|---|---|---|---|
| Total (N = 245) | No CU (n = 183) | Lifetime-CU (n = 62) | No IU (n = 14) | IU (n = 48) | |||
| Cannabis is safe because it is natural | |||||||
| Strongly agree/agree | 130 (53.1) | 86 (47) | 44 (71) | <.001 | 8 (57.1) | 36 (75) | .34 |
| Neither agree nor disagree/disagree/strongly disagree | 115 (46.9) | 97 (53) | 18 (29) | 6 (42.9) | 12 (25) | ||
| Cannabis can be addictive | |||||||
| Strongly agree/agree | 217 (88.6) | 169 (92.3) | 48 (77.4) | .003 | 12 (85.7) | 36 (75) | .63 |
| Neither agree nor disagree/disagree/strongly disagree | 28 (11.4) | 14 (7.7) | 14 (22.6) | 2 (14.3) | 12 (25) | ||
| Using cannabis can make my medical condition worse | |||||||
| Strongly agree/agree | 182 (74.3) | 153 (83.6) | 29 (46.8) | <.001 | 10 (71.4) | 19 (39.6) | .07 |
| Neither agree nor disagree/disagree/strongly disagree | 63 (25.7) | 30 (16.4) | 33 (53.2) | 4 (28.6) | 29 (60.4) | ||
| Risk of harm associated with regular cannabis use (n = 244) | |||||||
| Low risk: risk/slight risk | 108 (44.3) | 82 (45.0) | 26 (41.9) | .009 | 8 (57.1) | 18 (37.5) | .32 |
| High risk: moderate risk/great risk | 84 (34.4) | 48 (26.4) | 36 (58.1) | 6 (42.9) | 30 (63.5) | ||
| Can’t say, not familiar with the drug | 52 (21.3) | 52 (28.6) | 0 | NA | 0 | 0 | NA |
P values relate to differences between total CU and no CU.
P values relate to differences between IU and no IU.
Abbreviations: IU, instrumental use; NA, not applicable.
Likelihood of Future Use
For those with CU, when asked about the likelihood of CU in the next month, 16 of 62 participants (25.8%) reported they definitely will, 16 of 62 (25.8%) probably will, 17 of 62 (27.4%) probably will not, and 13 of 62 (21.0%) definitely will not. When asked about likelihood of CU in the next year, 24 of 62 (38.7%) reported they definitely will, 25 of 62 (40.3%) probably will, 7 of 62 (11.3%) probably will not, and 6 of 62 (9.7%) definitely will not.
Discussion
This study examined CU and IU rates in youths with diagnosed pain disorders. Lifetime CU prevalence was approximately 25%, with past year and past month rates of 23% and 16%, respectively, which is similar to those of nationally-representative adolescent samples (lifetime: 22.4%, past year: 17.8%, past month: 10.3%).50 The mean age of first use was 15 years, raising concerns, since initiating CU at younger ages (12-17 years) doubles the risk of developing CU disorders compared with initiating later.51 Additionally, youths with CU demonstrated a bimodal distribution, typically using cannabis either occasionally (3-5 occasions) or heavily (over 40 occasions). Taken together, these results highlight unique vulnerability for CU among youths with diagnosed pain disorders.52 Early identification of high-risk groups remains crucial.
Youths with CU reported greater pain interference than youths with no CU. One explanation is that more severe pain increases CU, potentially exacerbating pain interference. Alternatively, both cannabis use and pain interference may share an underlying driver such as depressive symptoms, which could increase both pain sensitivity and substance use likelihood. Further, CU influences endogenous pain systems through activation of cannabinoid receptor 1,53 setting youths up for a vicious cycle of increased pain and urge of use.54 Nearly 80% of youths reporting CU endorsed IU primarily for pain, anxiety, and sleep disturbances. This IU prevalence is higher than reported among other pediatric populations with chronic conditions27 but similar to adult populations using cannabis for pain, stress, and sleep relief.55,56 The high IU prevalence suggests that CU among youths with pain may be influenced by a complex interplay of biological (pain severity),53 psychological (anxiety or sleep disturbances), and social (peer influence or accessibility) factors, highlighting the importance of multidimensional interventions beyond pain management alone. Youths reporting IU also had higher functional disability than those with no IU, possibly reflecting unsuccessful attempts at using more adaptive coping strategies or elevated symptom severity, leaving CU for symptom relief as their only effective strategy. Future work should explore contextual factors associated with IU to enhance targeted interventions.
Findings regarding cannabis risk perceptions revealed youths with CU perceived cannabis as less harmful than their peers without CU. This discrepancy may result from greater exposure among those with use to cannabis’ purported analgesic properties, shaping their perceptions of risk and benefits. Given mixed evidence of cannabis’ effectiveness for pain relief,24,25 this underscores the importance of educating youths about cannabis risks in clinical settings, particularly for those who respond poorly to conventional treatments. Integrating adaptive coping skills training may reduce reliance on cannabis, potentially improving treatment outcomes.
Finally, our findings also reveal reasons why some youths with pain may not use cannabis. Most youths in our sample with no CU reported concerns about psychological or physical damage, addiction, and loss of control as very important to them. Most of these youths also reported they did not feel like getting high and that their parents would disapprove if they were to use cannabis. This information may help clarify what beliefs distinguish youths with pain who do vs do not use cannabis and may ultimately guide supportive strategies for abstinence.
Limitations
Limitations of this study also provide avenues for future research. First, this study is cross-sectional, so temporal or causal claims about CU trajectories cannot be determined. Inclusion of a control group along with a longitudinal design would be necessary for determining true associations and clarifying fluctuations in pain and CU over time. Second, the current sample was drawn from 1 pediatric hospital in the northeast where CU is legal, which may influence youths’ perceptions of cannabis-related risks and beliefs.57,58 Although their demographics largely mirror those of other larger samples of pediatric pain patients,59 future work should seek more diverse samples to investigate CU rates across different geographic locations, as well as among patients with varying gender, sexual orientation, and cultural identities. Third, while our statistical comparisons were hypothesis-driven rather than exploratory, we acknowledge that multiple testing can increase the risk of type I error, and we report CIs and effect sizes alongside P values to provide a more complete interpretation of findings. Additionally, the current study lacked a measure of social desirability, which may have biased responses and did not include certain relevant demographic factors, such as socioeconomic status.
Conclusions
In this cross-sectional study of treatment-seeking youths with pediatric pain, approximately 25% of participants reported CU, and more than 75% of cannabis-using youths reported IU for symptom relief. Given the immediate and longer-term risks associated with youth CU in pain populations,20,60 these findings highlight the importance of targeted education about cannabis risks and the need to develop alternative coping strategies in pediatric pain care.
References
- The severity of chronic pediatric pain: an epidemiological study.. J Pain., 2008. [DOI | PubMed]
- The epidemiology of chronic pain in children and adolescents revisited: a systematic review.. Pain., 2011. [DOI | PubMed]
- An international survey of pain in adolescents.. BMC Public Health., 2014. [DOI | PubMed]
- Association between widespread pain scores and functional impairment and health-related quality of life in clinical samples of children.. J Pain., 2016. [DOI | PubMed]
- Psychosocial aspects of spinal cord injury pain: a meta-analysis.. Spinal Cord., 2016. [DOI | PubMed]
- Social functioning and peer relationships in children and adolescents with chronic pain: a systematic review.. Pain Res Manag., 2010. [DOI | PubMed]
- Daily sleep quality and mood as predictors of pain in children with juvenile polyarticular arthritis.. Health Psychol., 2012. [DOI | PubMed]
- A longitudinal study of bidirectional associations between frequent pain and insomnia symptoms in adolescents.. Sleep Health., 2022. [DOI | PubMed]
- Cannabis use for sleep aid among high school students: concurrent and prospective associations with substance use and sleep problems.. Addict Behav., 2022. [DOI | PubMed]
- Assessing changes in sleep across four weeks among adolescents randomized to incentivized cannabis abstinence.. Drug Alcohol Depend., 2023. [DOI | PubMed]
- A review of psychosocial factors linked to adolescent substance use.. Pharmacol Biochem Behav., 2020. [DOI | PubMed]
- The correlation between loneliness and substance use proclivity in child and adolescent substance users.. J Subst Use., 2022. [DOI]
- Declines in adolescent substance use after the COVID-19 pandemic onset: the role of initiation in grades 7 and 9.. J Adolesc Health., 2023. [DOI | PubMed]
- Substance-related disorders: a review of prevalence and correlates among patients with chronic pain.. Prog Neuropsychopharmacol Biol Psychiatry., 2018. [DOI | PubMed]
- Patterns of marijuana use in a 6-month pain management sample in the United States.. Subst Abuse.. [DOI | PubMed]
- Alcohol and opioid use, co-use, and chronic pain in the context of the opioid epidemic: a critical review.. Alcohol Clin Exp Res., 2018. [DOI | PubMed]
- Cannabis use in hospitalized patients with chronic pain.. Adv Ther., 2020. [DOI | PubMed]
- Long-term and serious harms of medical cannabis and cannabinoids for chronic pain: a systematic review of non-randomised studies.. BMJ Open., 2022. [DOI | PubMed]
- Pain interference and alcohol, nicotine, and cannabis use disorder in a national sample of substance users.. Drug Alcohol Depend., 2018. [DOI | PubMed]
- A reciprocal model of pain and substance use: transdiagnostic considerations, clinical implications, and future directions.. Annu Rev Clin Psychol., 2019. [DOI | PubMed]
- Medical use of cannabis in Switzerland: analysis of approved exceptional licences.. Swiss Med Wkly., 2017. [DOI | PubMed]
- Pain relief as a motivation for cannabis use among young adult users with and without chronic pain.. J Pain., 2019. [DOI | PubMed]
- Cannabis and cannabinoids for the treatment of people with chronic noncancer pain conditions: a systematic review and meta-analysis of controlled and observational studies.. Pain., 2018. [DOI | PubMed]
- Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: a systematic review and meta-analysis of randomised clinical trials.. BMJ., 2021. [DOI | PubMed]
- Cannabinoids for the treatment of mental disorders and symptoms of mental disorders: a systematic review and meta-analysis.. Lancet Psychiatry., 2019. [DOI | PubMed]
- Substance use patterns through early adulthood: results for youth with and without chronic conditions.. Am J Prev Med., 2016. [DOI | PubMed]
- Marijuana use to address symptoms and side effects by youth with chronic medical conditions.. Pediatrics., 2021. [DOI | PubMed]
- Instrumental substance use among youth with rheumatic disease-a biopsychosocial model.. Rheum Dis Clin North Am., 2022. [DOI | PubMed]
- Increased substance use and poorer mental health in adolescents with problematic musculoskeletal pain.. J Orthop Sports Phys Ther., 2017. [DOI | PubMed]
- Back pain, mental health and substance use are associated in adolescents.. J Public Health (Oxf)., 2019. [DOI | PubMed]
- Comorbidity of mental disorders and chronic pain: chronology of onset in adolescents of a national representative cohort.. J Pain., 2015. [DOI | PubMed]
- 32Johnston LD, Miech RA, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the future national survey results on drug use, 1975-2021: overview, key findings on adolescent drug use. 2022. Accessed April 22, 2025. https://monitoringthefuture.org/wp-content/uploads/2022/08/mtf-overview2021.pdf
- Cannabis use among U.S. adolescents in the era of marijuana legalization: a review of changing use patterns, comorbidity, and health correlates.. Int Rev Psychiatry., 2020. [DOI | PubMed]
- Brain morphology predictors of alcohol, tobacco, and cannabis use in adolescence: a systematic review.. Brain Res., 2022. [DOI | PubMed]
- Predictors and prevalence of alcohol and cannabis co-use among Filipino adolescents: evidence from a school-based student health survey.. J Prev Med Public Health., 2024. [DOI | PubMed]
- Cannabis use disorder, suicide attempts, and self-harm among adolescents: a national inpatient study across the United States.. PLoS One., 2023. [DOI | PubMed]
- Age-dependent association of cannabis use with risk of psychotic disorder.. Psychol Med., 2024. [DOI | PubMed]
- Acute mental health symptoms in adolescent marijuana users.. JAMA Pediatr., 2019. [DOI | PubMed]
- The REDCap consortium: building an international community of software platform partners.. J Biomed Inform., 2019. [DOI | PubMed]
- Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support.. J Biomed Inform., 2009. [DOI | PubMed]
- 41Mattingly DT, Richardson MK, Hart JL. Prevalence of and trends in current cannabis use among US youth and adults, 2013–2022. Drug Alcohol Depend Rep. 2024;12:100253. doi:10.1016/j.dadr.2024.100253
- Numerical rating scale for self-report of pain intensity in children and adolescents: recent progress and further questions.. Eur J Pain., 2009. [DOI | PubMed]
- The pain frequency-severity-duration scale as a measure of pain: preliminary validation in a pediatric chronic pain sample.. Pain Res Treat., 2014. [DOI | PubMed]
- PROMIS Pediatric Pain Interference Scale: an item response theory analysis of the pediatric pain item bank.. J Pain., 2010. [DOI | PubMed]
- The clinical utility of a brief psychological stress measure (patient-reported outcomes measurement information system) in youth with chronic pain.. Pain Med., 2021. [DOI | PubMed]
- Evidence from diverse clinical populations supported clinical validity of PROMIS pain interference and pain behavior.. J Clin Epidemiol., 2016. [DOI | PubMed]
- The functional disability inventory: measuring a neglected dimension of child health status.. J Pediatr Psychol., 1991. [DOI | PubMed]
- 48Johnston L, Miech R, O’Malley P, Bachman J, Schulenberg J, Patrick M. Monitoring the Future national survey results on drug use, 1975-2019: overview, key findings on adolescent drug use. 2020. Accessed April 22, 2025. https://eric.ed.gov/?id=ED604018
- 492019 National Survey on Drug Use and Health Public Use File Codebook. Substance Abuse and Mental Health Services Administration. Center for Behavioral Health Statistics and Quality; 2020.
- 50Miech RA, Johnston LD, Patrick ME, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future National Survey Results on Drug Use, 1975-2022: Secondary School Students. Institute for Social Research; 2023.
- Effects of age at first substance use and psychiatric comorbidity on the development of substance use disorders.. Drug Alcohol Depend., 2004. [DOI | PubMed]
- Youth cannabis use and subsequent health service use for mood and anxiety disorders: a population-based cohort study.. Psychiatry Res., 2024. [DOI | PubMed]
- Cannabinoids and pain: new insights from old molecules.. Front Pharmacol., 2018. [DOI | PubMed]
- Effect of cannabis use in people with chronic non-cancer pain prescribed opioids: findings from a 4-year prospective cohort study.. Lancet Public Health., 2018. [DOI | PubMed]
- Prevalence of cannabis use disorder and reasons for use among adults in a US state where recreational cannabis use is legal.. JAMA Netw Open., 2023. [DOI | PubMed]
- Frequency of cannabis and illicit opioid use among people who use drugs and report chronic pain: a longitudinal analysis.. PLoS Med., 2019. [DOI | PubMed]
- Cannabis use, attitudes, and legal status in the U.S.: a review.. Prev Med., 2017. [DOI | PubMed]
- Assessing the impact of recreational cannabis legalization on cannabis use disorder and admissions to treatment in the United States.. Curr Addict Rep., 2023. [DOI | PubMed]
- Chronic pain in pediatric patients: epidemiology, pathophysiology, and mitigation strategies.. Curr Opin Anaesthesiol., 2024. [DOI | PubMed]
- Adverse effects of recreational and medical cannabis.. Psychopharmacol Bull., 2021. [PubMed]