Thyroid Storm
Abstract
Audience:
This is a practice oral boards case which may be given to emergency medicine (EM) residents at all levels of training and recent EM graduates.
Introduction/Background:
Thyroid storm is an acute, life-threatening endocrine emergency. It occurs when there is excess circulating thyroid hormone in the bloodstream. It may be precipitated by infection, surgery, pregnancy, trauma, thyroid medication changes, or iodinated contrast exposure. This condition must be quickly identified and treated by EM physicians in order to prevent morbidity and mortality. IThe mortality rate is between 10 and 30%ref. 1 Understanding and treating thyroid storm is included in the 2019 Model of Clinical Practice of Emergency Medicine.ref. 2
Educational Objectives:
At the end of this practice oral boards case, the learner will: 1) assess a patient with altered mental status in an oral boards format; 2) review appropriate laboratory testing and diagnostic imaging; 3) identify signs and symptoms of thyroid storm and 4) review appropriate pharmacologic therapies with the proper sequence and timing.
Educational Methods:
Practice boards case.
Research Methods:
This oral boards practice case was developed and then tested in several small group settings. First, EM resident learners discussed the case in a small group format. Their feedback was utilized to refine the case’s textual information. Subsequently, EM physicians preparing for the ABEM oral board examination provided additional general feedback of the case and completed an anonymous survey regarding case quality and educational value.
Results:
Minor changes were made based on feedback from small group sessions. The finalized case was tested with individuals, and surveys showed that 92% (12/13) of individuals rated the case quality as excellent (standard Likert scale 1–5 with 5 being Excellent). All participants responded affirmatively that the case enhanced their understanding of thyroid storm.
Discussion:
This oral boards practice case was effective in preparing learners for the ABEM oral boards exam. Based on learner feedback, several laboratory results were added to the stimulus package and wording was edited to improve the clarity of the case.
Topics:
Hyperthyroidism, thyrotoxicosis, thyroid storm, endocrine emergencies, altered mental status.
Affiliations: *Vanderbilt University Medical Center, Department of Emergency Medicine, Nashville, TN
License: © 2020 Ritter, et al. CC BY 4.0 This is an open access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) License. See: http://creativecommons.org/licenses/by/4.0/
Article links: DOI: 10.21980/J8RW71 | PubMed: 37465337 | PMC: PMC10334447
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (5.8 MB)
USER GUIDE
List of Resources: Abstract1 User Guide3 For Examiner Only5 Oral Boards Assessment11 Stimulus15 Debriefing and Evaluation Pearls30
Learner Audience:
Medical students, interns, junior residents, senior residents
Time Required for Implementation:
Case: 10 minutes as a single case
Debriefing: 15 minutes
Learners per instructor:
This case can be practiced with one learner per instructor or a small group observational setting.
Topics:
Hyperthyroidism, thyrotoxicosis, thyroid storm, endocrine emergencies, altered mental status.
Objectives:
By the end of this oral boards case, learners will be able to:
- Assess a patient with altered mental status in an oral boards format.
- Review appropriate laboratory testing and diagnostic imaging for a patient with altered mental status.
- Identify signs and symptoms of thyroid storm.
- Review appropriate pharmacologic therapies with the proper sequence and timing.
Linked objectives and methods
An oral boards format was selected as an alternative modality to teach this core EM topic in order to provide real-time feedback to the learner as the case progresses. Symptoms of thyroid storm are often initially non-specific and may mimic many other clinical entities, making this teaching style beneficial because learners must form a large differential diagnosis and remember to suspect endocrine abnormalities as a possible cause (Objective 1). After initial evaluation, learners must then order, review, and interpret appropriate laboratory testing and diagnostic imaging with attention given to information which leads them to the ultimate diagnosis (Objective 2). Based on the information provided, learners should hone in on signs and symptoms which point to thyroid storm (Objective 3). After establishing thyroid storm as the appropriate diagnosis, learners should order appropriate pharmacologic interventions in the proper order for treatment (Objective 4). The use of a one-on-one practice case format enables the teacher to tailor additional information to various levels of training when providing further information on clinical pearls after the case conclusion. Any gaps in knowledge may be identified by the examiner and then addressed in a focused debrief or mini-lecture after the conclusion of the practice case.
Recommended pre-reading for instructor
- Awad N. Thyroid storm: treatment strategies. Academic Life in Emergency Medicine. https://www.aliem.com/2013/11/thyroid-stormtreatment-strategies/. Published November 11, 2013. Accessed on February 7, 2019.
- Idrose A. Hyperthyroidism and Thyroid Storm. In: Tintinalli JE, Ma OJ, Yealy DM, et al eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 9th ed. New York, NY: McGraw-Hill; 2019; 1450–1456.
- Field A. Thyroid storm. In: Wolfson AB, ed. Harwood-Nuss’ Clinical Practice of Emergency Medicine. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014; 1025–1028.
Results and tips for successful implementation
This case was designed to be used as preparation for the emergency medicine oral board examination. Faculty members may administer the case to residents by presenting the initial case information and then requesting for residents to verbalize their evaluation and clinical treatment plan. In addition, it may be used as part of a didactic teaching curriculum, which begins with the case presentation and then focuses on key teaching points as a mini-lecture following the case resolution.
This oral boards case was developed and then previewed in small group settings to ensure inclusive information and to resolve any ambiguities of the case. The finalized version was then tested with thirteen physicians who were preparing for the ABEM oral boards and a survey was administered to assess case quality and educational value. 92% (12/13) of these physicians rated the case as excellent (standard Likert scale 1–5 with 5 being Excellent), and all residents responded affirmatively that the case enhanced their understanding of thyroid storm. Learners noted that the case was “complex” and “allowed for higher order thinking,” also stating that “there were subtle features that should clue the examinee not to anchor on sepsis” and that “it was helpful to think through the differential for a hyperthermic altered patient.” Based on feedback from these sessions, additional learning points were clarified.
| List of Resources: | |
|---|---|
| Abstract | 1 |
| User Guide | 3 |
| For Examiner Only | 5 |
| Oral Boards Assessment | 11 |
| Stimulus | 15 |
| Debriefing and Evaluation Pearls | 30 |
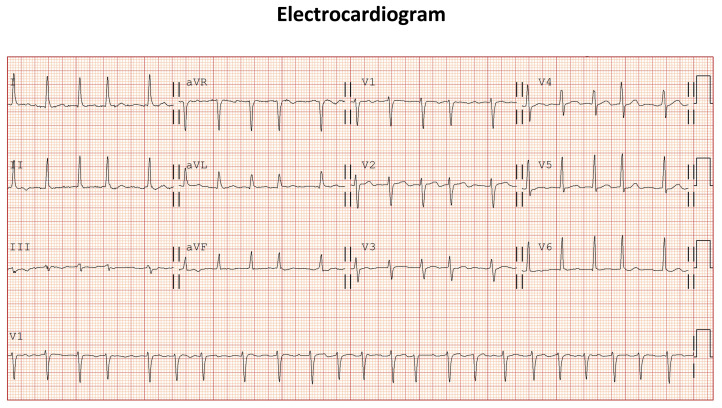
| Vitals: HR 142 | BP 158/99 | RR 24 | Temp 40.1°C | O2Sat 98% on room air |
| Milestone | Did not achieve level 1 | Level 1 | Level 2 | Level 3 | |
|---|---|---|---|---|---|
| 1 | Emergency Stabilization (PC1) | □Did not achieve Level 1 | □Recognizes abnormal vital signs | □Recognizes an unstable patient, requiring interventionPerforms primary assessmentDiscerns data to formulate a diagnostic impression/plan | □Manages and prioritizes critical actions in a critically ill patientReassesses after implementing a stabilizing intervention |
| 2 | Performance of focused history and physical (PC2) | □Did not achieve Level 1 | □Performs a reliable, comprehensive history and physical exam | □Performs and communicates a focused history and physical exam based on chief complaint and urgent issues | □Prioritizes essential components of history and physical exam given dynamic circumstances |
| 3 | Diagnostic studies (PC3) | □Did not achieve Level 1 | □Determines the necessity of diagnostic studies | □Orders appropriate diagnostic studiesPerforms appropriate bedside diagnostic studies/procedures | □Prioritizes essential testingInterprets results of diagnostic studiesConsiders risks, benefits, contraindications, and alternatives to a diagnostic study or procedure |
| 4 | Diagnosis (PC4) | □Did not achieve Level 1 | □Considers a list of potential diagnoses | □Considers an appropriate list of potential diagnosisMay or may not make correct diagnosis | □Makes the appropriate diagnosisConsiders other potential diagnoses, avoiding premature closure |
| 5 | Pharmacotherapy (PC5) | □Did not achieve Level 1 | □Asks patient for drug allergies | □Selects an appropriate medication for therapeutic intervention, considering potential adverse effects | □Selects the most appropriate medication(s) and understands mechanism of action, effect, and potential side effectsConsiders and recognizes drug-drug interactions |
| 6 | Observation and reassessment (PC6) | □Did not achieve Level 1 | □Reevaluates patient at least one time during the case | □Reevaluates patient after most therapeutic interventions | □Consistently evaluates the effectiveness of therapies at appropriate intervals |
| 7 | Disposition (PC7) | □Did not achieve Level 1 | □Appropriately selects whether to admit or discharge the patient | □Appropriately selects whether to admit or dischargeInvolves the expertise of some of the appropriate specialists | □Educates the patient appropriately about their dispositionAssigns patient to an appropriate level of care (ICU/Tele/Floor)Involves expertise of all appropriate specialists |
| 22 | Patient centered communication (ICS1) | □Did not achieve level 1 | □Establishes rapport and demonstrates empathy to patient (and family)Listens effectively | □Elicits patient’s reason for seeking health care | □Manages patient expectations in a manner that minimizes potential for stress, conflict, and misunderstanding. |
| 23 | Team management (ICS2) | □Did not achieve level 1 | □Recognizes other members of the patient care team during case (nurse, techs) | □Communicates pertinent information to other healthcare colleagues | □Communicates a clear, succinct, and appropriate handoff with specialists and other colleaguesCommunicates effectively with ancillary staff |
| #1 | Patient information form |
| #2 | Complete blood count (CBC) |
| #3 | Comprehensive metabolic panel (CMP) |
| #4 | Urinalysis |
| #5 | Pregnancy Test |
| #6 | Urine Drug Screen |
| #7 | Serum Toxicology Screen |
| #8 | Troponin |
| #9 | Creatine Kinase |
| #10 | Thyroid Function Studies |
| #11 | Lactate |
| #12 | Arterial blood gas |
| #13 | Electrocardiogram (ECG) |
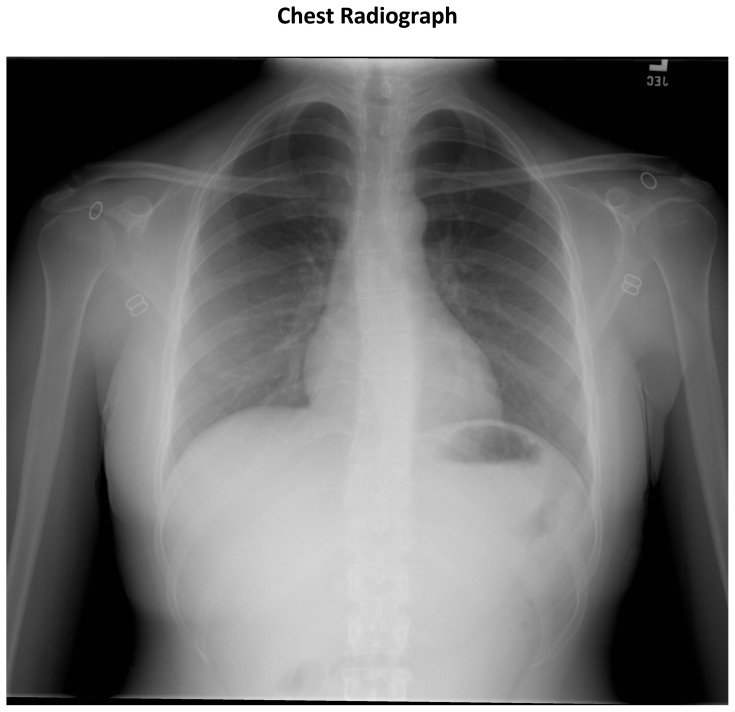
| #14 | Chest radiograph |
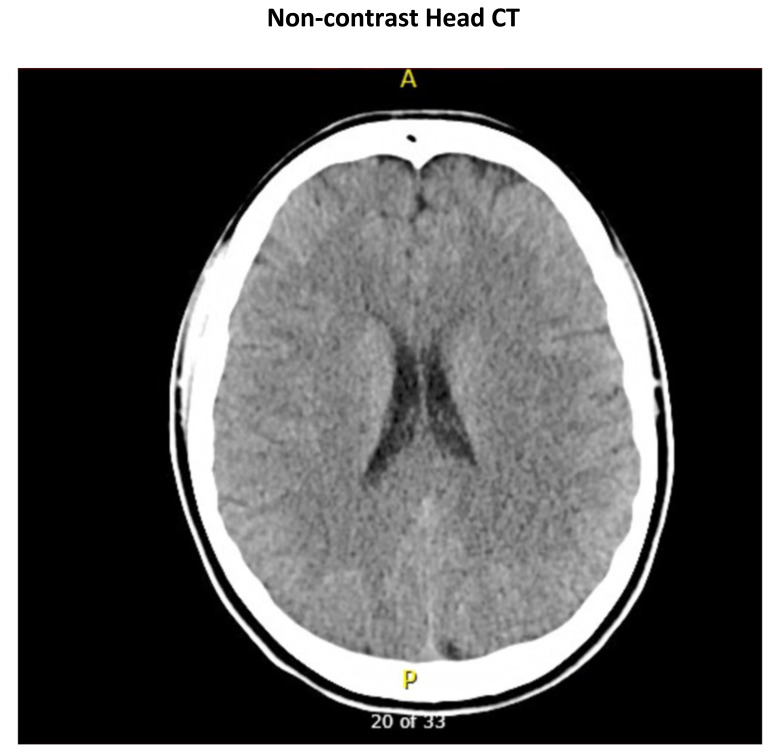
| #15 | Head Computed Tomography (CT) |
| Patient’s Name: | Andrea Mason | |
| Age: | 33 | |
| Gender: | Female | |
| Chief Complaint: | Altered mental status | |
| Person Providing History: EMS and patient’s husband | ||
| Vital Signs: | ||
| Temp: | 40.1°C | |
| BP: | 158/199 | |
| P: | 142 | |
| RR: | 24 | |
| O2sat: | 98% (room-air) | |
| Weight: | 65 kg | |
| White blood cell count (WBC) | 16.1 x1000/mm3 |
| Hemoglobin (Hgb) | 12.9 g/dL |
| Hematocrit (Hct) | 38.8% |
| Platelets | 270 x1000/mm3 |
| Neutrophils | 66% (10,626) |
| Lymphocytes | 26% (4,186) |
| Monocytes | 5% (805) |
| Eosinophils | 2.5% (402) |
| Basophils | 0.5% (81) |
| Sodium | 142 mEq/L |
| Potassium | 4.4 mEq/L |
| Chloride | 107 mEq/L |
| Bicarbonate | 24 mEq/L |
| Blood Urea Nitrogen (BUN) | 13 mg/dL |
| Glucose | 95 mg/dL |
| Creatinine (Cr) | 0.68 mg/dL |
| Calcium | 9.4 mg/dL |
| Anion Gap | 11 |
| Direct Bilirubin | 0.2 mg/dL |
| Total Bilirubin | 0.4 mg/dL |
| Albumin | 4.1 g/dL |
| Alkaline Phosphatase | 49 Units/L |
| ALT | 11 Units/L |
| AST | 15 Units/L |
| Total Protein | 7.3 g/dL |
| Color | Yellow |
| Appearance | Cloudy |
| Sp Gravity | 1.023 |
| pH | 5.5 |
| Glucose | Negative |
| Protein | 30 |
| Ketones | Negative |
| Bilirubin | Negative |
| Leukocyte Esterase | Large |
| Nitrite | Positive |
| Blood | Small |
| Microscopy | |
| WBC | 1123/high powered field (hpf) |
| Red blood cells (RBC) | 35/hpf |
| Bacteria | 3+ |
| Acetaminophen | Negative |
| Amphetamine | Negative |
| Barbituate | Negative |
| Benzodiazepine | Negative |
| Buprenorphine | Negative |
| Cannabinoid | Negative |
| Cocaine | Negative |
| Ethanol | Negative |
| Methadone | Negative |
| Opiate | Negative |
| Oxycodone | Negative |
| Salicylate | Negative |
| Tricyclic | Negative |
| Acetaminophen | Negative |
| Ethanol | Negative |
| Salicylate | Negative |
| Troponin | <0.01 ng/mL |
| CK | 380 Units/L |
| TSH | 0.04 mIU/L (normal 0.350 – 3.600) |
| Free T4 | 17.4 ng/dL (normal 0.70 – 1.37) |
| Lactate | 2.4 mEq/L |
| pH | 7.41 |
| pCO2 | 37 mmHg |
| pO2 | 94 mmHg |
| HCO3 | 26 mmol/L |
Treatment of Thyroid Storm
| Block peripheral thyroid hormone effects | Propranolol, esmolol |
| Inhibit release of thyroid hormones | Propylthiouracil, methimazole |
| Decrease peripheral conversion of T4 to T3 | Hydrocortisone, dexamethasone |
| Inhibit production of new thyroid hormones | Lugol solution, potassium iodide |
References
- M Chiha, S Samarasinghe, AS Kabaker. Thyroid storm: an updated review. J Intensive Care Med, 2015. [DOI | PubMed]
- MS Beeson, F Ankel, R Bhat, JN Keehbauch. The 2019 Model of the clinical practice of emergency medicine. J Emerge Med, 2020. [DOI]
- A Field. Thyroid Storm. Harwood-Nuss’ Clinical Practice of Emergency Medicine, 2014
- R Carroll, G Matfin. Endocrine and metabolic emergencies: thyroid storm. Ther Adv Endocrinol Metab, 2010. [DOI | PubMed]
- J Klubo-Gwiezdzinska, L Wartofsky. Thyroid emergencies. Med Clin North Am, 2012. [DOI | PubMed]