
Trends in resource utilization for new‐onset psychosis hospitalizations at children’s hospitals
Abstract
Background:
Children with new‐onset psychosis often require hospitalization for medical evaluation.
Objectives:
The goal of this study was to assess variations in the management of children with new‐onset psychosis and characterize trends in resource utilization.
Methods:
The study included index hospitalizations for children ages 7–18 admitted to children’s hospitals with a primary diagnosis of psychosis from 2011 to 2022 using the Pediatric Health Information System (PHIS) database. Children with a complex chronic condition were excluded. Resource utilization categories included medication, imaging, laboratory, and other clinical resources. Variability in resource utilization was assessed using covariance tests for random intercepts with generalized linear modes after adjusting for age, sex, payor, and severity. Trends in resource utilization were examined using generalized estimating equations adjusting for the same factors and accounting for hospital clustering.
Results:
Our data set included 7126 new‐onset psychosis hospitalizations from 37 children’s hospitals. Teenage males and non‐Hispanic Whites were most likely to be hospitalized. There was a significant variation in resource utilization across hospitals in all categories (p < .001). The most frequently utilized resources were antipsychotic medications (76%), serum chemistry (77%), toxicology labs (72%), and brain magnetic resonance imaging (22%). The most notable increases in utilization were in the performance of laboratory tests, brain imaging, anesthetic use, and intravenous immunoglobulin use.
Conclusion:
Study findings suggest that there has been a stable rate of hospitalization for children with new‐onset psychosis, yet a significant variation in the medical evaluation exists. Significant increases and variations in resource utilization across all categories suggest an emerging need for robust evidence and consensus‐based practice guidelines.
Affiliations: Department of Pediatrics, Division of Pediatric Hospital Medicine University of Texas Southwestern Dallas Texas USA; Children’s Medical Center Dallas Texas USA; Children’s Hospital Association Lenexa Kansas USA
License: © 2025 The Author(s). Journal of Hospital Medicine published by Wiley Periodicals LLC on behalf of Society of Hospital Medicine. CC BY 4.0 This is an open access article under the terms of the http://creativecommons.org/licenses/by/4.0/ License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Article links: DOI: 10.1002/jhm.13597 | PubMed: 39893566 | PMC: PMC12217426
Relevance: Moderate: mentioned 3+ times in text
Full text: PDF (1.8 MB)
INTRODUCTION
Psychosis, defined as impaired reality with disruptions in thinking, perceptions, and behaviorref. jhm13597-bib-0001, is one of the most frequent and costly pediatric mental health diagnoses requiring hospitalization.ref. jhm13597-bib-0002 Symptoms can include hallucinations, delusions, disorganized speech, and other abnormal psychomotor behaviors.ref. jhm13597-bib-0003 Each year, 100,000 young adults experience new‐onset psychosis in the United States, with peak onset between ages 15 and 25.ref. jhm13597-bib-0001, ref. jhm13597-bib-0004 Recent data suggest that the prevalence of psychosis symptoms in pediatric patients is approximately 17% for children between 9 and 12 years of age and 7.5% among children between 13 and 18 years of age.ref. jhm13597-bib-0005
Despite its incidence, managing psychosis in an inpatient setting remains a clinical challenge. Most patients with new‐onset psychosis do not go on to develop a primary psychotic disorder, and the differential diagnosis for secondary psychosis is broad.ref. jhm13597-bib-0001, ref. jhm13597-bib-0006 Secondary psychosis can be the presenting feature of multiple medical conditions such as neurologic disorders, endocrine disorders, drug or toxin‐mediated syndromes, and others.ref. jhm13597-bib-0007 Expert opinions vary on the extent of medical evaluation that patients should undergo during an index hospitalization.ref. jhm13597-bib-0008, ref. jhm13597-bib-0009, ref. jhm13597-bib-0010 Crucially, a delay in or nontreatment of secondary psychosis in pediatric inpatients can lead to significant morbidity and even mortality.ref. jhm13597-bib-0007
Not enough is known about how to evaluate a child presenting with new‐onset psychosis in the hospital setting. Thus, the objectives of this study were to assess variations in the evaluation and management of children hospitalized with a new‐onset psychosis across US children’s hospitals and to characterize trends in resource utilization over time.
METHODS
This was a retrospective, cross‐sectional study of the Pediatric Health Information System (PHIS; Children’s Hospital Association) database, which contains data from 49 tertiary care children’s hospitals. Of the 49 hospitals, 37 consistently participated in PHIS during the study period and were included in the study. All submitted data are de‐identified. Data quality and reliability are assured through a joint effort between the Children’s Hospital Association and the respective hospitals. This study was approved for exemption by the institutional review board of the University of Texas Southwestern.
Study population
Children 7–18 years of age with a primary discharge diagnosis of psychosis between January 2011 and December 2022 were included. Patient‐level variables included age (stratified as 7–10, 11–14, and 15–18), gender, race and ethnicity, payor (government, private, or other), discharge disposition (home, skilled facility, or other), and year (stratified as 2011–2013, 2014–2016, 2017–‐2019, and 2020–2022). Only index encounters were included to capture new‐onset psychosis. Children with complex chronic conditions were excluded as they may have underlying conditions affecting their evaluation and management.ref. jhm13597-bib-0011 The Childhood and Adolescent Mental Health Disorders Classification System (CAMHD‐CS) was used to identify diagnoses that met the criteria for inclusion.ref. jhm13597-bib-0012 Diagnoses were manually identified under categories of bipolar disorders, schizophrenia, and other psychotic disorders to best define a patient with psychosis symptoms (Appendix A).
Measures of resource utilization
Utilization was identified from billing data and categorized as medication, imaging, laboratory, and other clinical resourcesref. jhm13597-bib-0010 (Appendix B). Medications included anesthetics, antidepressants, antiemetics, antiepileptics, antipsychotics, anxiolytics, intravenous immunoglobulin (IVIG), mood stabilizers, and steroids. Imaging included brain magnetic resonance imaging ((MRI), head computer tomography (CT), head ultrasound, abdominal imaging, reproductive imaging, and spinal imaging. Laboratory studies evaluated blood, urine, and cerebrospinal fluid samples and were categorized as autoimmune, chemistry, cerebrospinal (CSF) studies, endocrine, thyroid labs, hematology, infectious disease, toxicology, and urine studies. Other clinical resources included electroencephalogram (EEG), electrocardiogram (EKG), and therapy services such as physical (PT), occupational (OT), and speech therapy (ST). The tests and treatments were included based on existing literature, our local experience, availability at most children’s hospitals, and data from the PHIS database.
Statistical analysis
Categorical variables were summarized using frequencies and percentages. Variability in resource use across hospitals was assessed using covariance tests for random intercepts with generalized linear models with binomial distributions after adjusting for age, sex, payor, and severity. Trends in resource utilization across years were examined using generalized estimating equations adjusting for age, sex, payor, severity, and accounting for hospital clustering. All statistical analyses were performed using SAS version 9.4 (SAS Institute), and p < .05 was considered statistically significant.
RESULTS
This study included 7126 new‐onset psychosis hospitalizations from 37 hospitals. About half of them were male and had government payors, and a large proportion (80.6%) were discharged home following hospitalization (Table 1).
Table 1: Demographic and clinical characteristics of children hospitalized with new‐onset psychosis.
| N (%) | ||
|---|---|---|
| Age (years) | 7–10 | 883 (12.4) |
| 11–14 | 2080 (29.2) | |
| 15–18 | 4163 (58.4) | |
| Gender | Male | 4138 (58.1) |
| Female | 2986 (41.9) | |
| Race and ethnicity | Non‐Hispanic White | 2958 (41.5) |
| Non‐Hispanic Black | 2129 (29.9) | |
| Hispanic | 1256 (17.6) | |
| Asian | 162 (2.3) | |
| Other | 621 (8.7) | |
| Payor | Government | 3716 (57.5) |
| Private | 2346 (36.3) | |
| Other | 401 (6.2) | |
| Discharge disposition | Home | 5215 (80.7) |
| Skilled Facility | 132 (1.9) | |
| Othera | 1116 (17.3) | |
| Year | 2011–2013 | 1704 (23.9) |
| 2014–2016 | 1863 (26.1) | |
| 2017–2019 | 1674 (23.5) | |
| 2020–2022 | 1885 (26.5) |
Other Discharge Disposition includes transfer to a Psychiatric Hospital (67.8%) Designated Cancer Center or Children’s Hospital (11.2%), Type of Health Care Institution not Defined Elsewhere (6.3%), Against Medical Advice (4.2%), and Inpatient Rehabilitation Facility (1.8%).
Variations in resource utilization
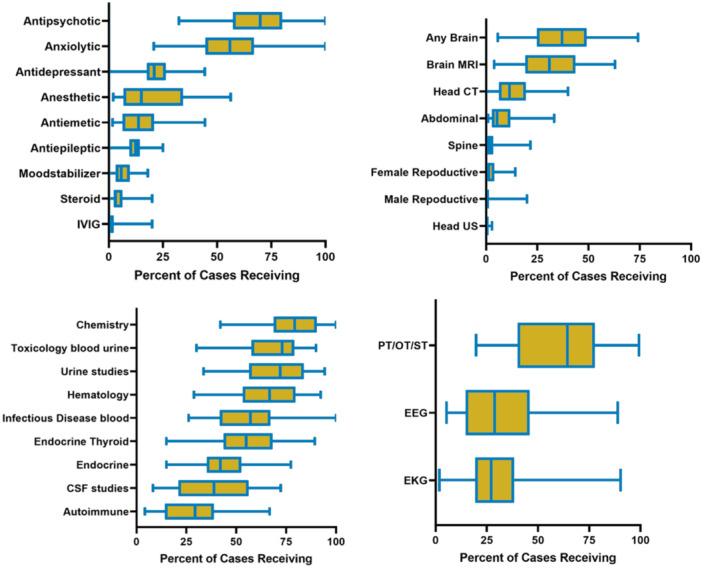
There was a statistically significant variation in resource use across all hospitals. This variation was significant in all categories of medications, imaging, laboratory, and other clinical resources (all p < .01, Figure 1). The most notable variation was in the utilization of CSF studies (median: 38.8 [interquartile range (IQR): 21.8, 55.8]), brain MRI (median: 30.9, [IQR: 19.3, 42.9]), anesthetic use (median: 15, [IQR: 7.6–33.3]), and use of therapy services (median: 64.3, [IQR: 43.8,75.4]).
Trends in resource utilization
Although the number of children hospitalized with new‐onset psychosis did not increase notably over the study period (p = .059; Table 1), resource utilization has significantly increased in all categories including medications, imaging, laboratory, and other clinical resources (all p < .001, Figure 2).
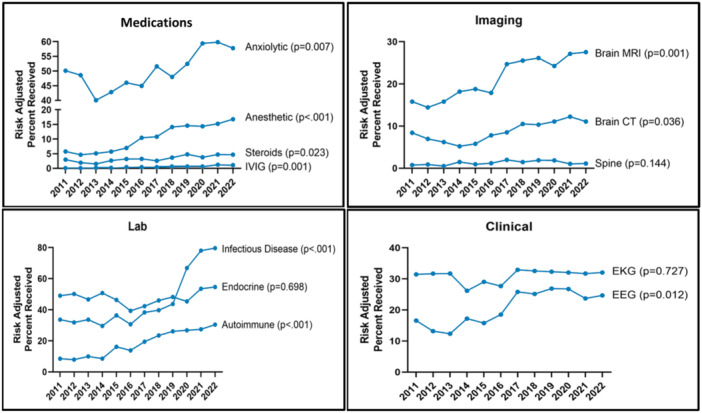
- Medication utilization: Trends suggest a significant increase in the use of anesthetic medication (adjusted odds ratio [aOR]: 3.4, 95% confidence interval [CI]: 2.0–5.8) and IVIG (aOR: 1.7, 95% CI: 1.3–2.2) (Figure 2).
- Imaging utilization: Brain MRI use (aOR: 1.9, 95% CI: 1.4–2.5) has significantly increased over time. Head CT was commonly performed, and frequency was stable over the course of the study.
- Laboratory utilization: Trends in laboratory utilization suggest a significant increase in the use of autoimmune labs (aOR: 4.1, 95% CI: 2.5–6.7) and infectious disease labs (aOR: 6.2, 95% CI: 3.7–10.4).
- Other clinical resources: Performance of both EEG (aOR: 2.1, 95% CI: 1.4–3.1) and EKGs (aOR: 1.0, 95% CI: 0.6–1.6) have increased over time (p = .012 and p = .72, respectively).
DISCUSSION
Our multicenter, retrospective study results show that there is a significant variation across children’s hospitals in the management of children with new‐onset psychosis. Findings also suggest an increase in resource utilization over the study period.
There is significant interhospital variability in the management of patients with new‐onset psychosis across all four resource categories, most notable in CSF studies, brain MRI, anesthetic use, and use of therapy services. This variation in the management may be due to a number of reasons. Many medical conditions such as infectious disease, endocrinopathies, drug and toxin ingestions, and neurological conditions can present with symptoms of new‐onset psychosis.ref. jhm13597-bib-0010, ref. jhm13597-bib-0013 Because psychosis is often the only presenting symptom, the broad differential can make it challenging to limit the labs and imaging studies that are ordered for an otherwise undifferentiated patient, even after a thorough history and physical exam.ref. jhm13597-bib-0009, ref. jhm13597-bib-0014 Variability may also exist because of a lack of national, standardized guidelines for diagnostic approaches to this patient population.ref. jhm13597-bib-0015 National guidelines can facilitate a stepwise approach to the identification and management of common and uncommon diagnoses.ref. jhm13597-bib-0016 Balancing early, accurate diagnosis with judicious use of healthcare resources for these patients is important. Nondiagnostic or low‐yield testing may delay diagnosis and treatment of psychosis,ref. jhm13597-bib-0017, ref. jhm13597-bib-0018, ref. jhm13597-bib-0019, ref. jhm13597-bib-0020 and misdiagnosis or unnecessary treatment can be equally harmful.ref. jhm13597-bib-0004 Our findings add to existing literature that highlights the need for future multidisciplinary investigation to help optimize the care of this complex patient population.
There are several implications when attempting to understand the increase in utilization of resources from 2011 to 2022, despite a stable rate of hospitalization for new‐onset psychosis. The increase in diagnostic testing for new‐onset psychosis may be part of a global trend of increasing unnecessary testing across the entire healthcare spectrum.ref. jhm13597-bib-0021 As previously mentioned, the lack of consensus guidelines can place physicians caring for children with new‐onset acute psychosis in a difficult situation when deciding the extent of medical workup to pursue. Part of the reason for increased resource utilization could be related to increased awareness of and/or prevalence of pediatric mental health disorders in the last decade.ref. jhm13597-bib-0002, ref. jhm13597-bib-0022, ref. jhm13597-bib-0023 The increase in utilization of anesthetic medication, brain MRI, and CSF studies is of particular clinical interest. A potential explanation may be due to an increased concern for neurologic causes of new‐onset psychosis such as autoimmune encephalitis (AIE).ref. jhm13597-bib-0024, ref. jhm13597-bib-0025 In 2014, psychosis was found to be the 3rd most resource‐demanding pediatric inpatient mental health diagnosis.ref. jhm13597-bib-0002 While our study did not specifically analyze costs related to resource utilization for children with new‐onset psychosis, it does shed light on the potential impact of increasing imaging, labs, and other testing over time. Increased utilization of laboratory tests such as infectious disease labs, hematology labs, and autoimmune labs may be of little consequence as the benefits of lab work far outweigh the risks. However, increased utilization of invasive procedures such as brain MRI and lumbar puncture to obtain CSF studies, which often require sedation in the pediatric population, must be approached in a thoughtful and considerate manner. This study did not allow an analysis of any results or outcomes of medical testing and evaluation that was conducted. However, Muhrer et al. suggested that extensive medical workup for new‐onset psychosis is typically unrevealing.ref. jhm13597-bib-0026 This is similar to prior studies done in the adult patient population.ref. jhm13597-bib-0027 For example, structural brain imaging in children with new‐onset psychosis is often unrevealing and does not affect the management of patients undergoing medical evaluation.ref. jhm13597-bib-0028, ref. jhm13597-bib-0029, ref. jhm13597-bib-0030 Since caring for children often involves multiple disciplines, perhaps a strategy to manage resources and mitigate risks could be to approach care in a multidisciplinary fashion with hospitalists, neurologists, and psychiatrists sharing clinical perspectives regarding the extent of medical testing that should be done in each case.ref. jhm13597-bib-0015
There are several limitations to this study. First, the study population was identified using primary discharge diagnosis codes, which are subject to coding errors. A lack of an established definition for “new‐onset psychosis” and the heterogeneity of the population make it possible that the 10th revision of the International Classification of Diseases (ICD‐10) codes selected in this study may not be fully representative of the population. This introduces the opportunity for misclassification bias in our analysis. Also, the details of the initial presentation could not be captured. An understanding of the patient’s initial presentation including the presence or absence of focal neurologic findings on exam or any “red flag” features on history would provide more insight into the trends in resource utilization. The inability to capture the full clinical picture could lead to interpretation bias. Additionally, the PHIS database uses billing data to identify resource utilization, but it cannot capture the indication for an intervention or the results of any test. Patients receiving intense psychotic therapies may need tests and treatments for monitoring and titration of medicines including sedation during testing. Thus, it is possible that the study findings, specifically regarding resource utilization over time, are overstated or lack important clinical context. Lastly, this study is limited to practices at tertiary care children’s hospitals and cannot be generalized to all settings that may care for children with new‐onset psychosis.
CONCLUSIONS
In conclusion, our study suggests that there is a significant variation across children’s hospitals in the evaluation and management of children hospitalized with new‐onset psychosis. Resource utilization for the initial workup for this patient population increased significantly in all examined categories. The next steps would involve additional subgroup analyses within conditions presenting as acute psychosis. This could then help develop an evidence‐based practice guideline to guide clinicians in managing hospitalized children with new‐onset psychosis.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
| Mental health disorder group | International classification of diseases code | Version | Description |
|---|---|---|---|
| Bipolar and related disorders | 2967 | 9 | Bipolar I disorder, most recent episode (or current) unspecified |
| Bipolar and related disorders | 29600 | 9 | Bipolar I disorder, single manic episode, unspecified |
| Bipolar and related disorder | 29601 | 9 | Bipolar I disorder, single manic episode, mild |
| Bipolar and related disorders | 29602 | 9 | Bipolar I disorder, single manic episode, moderate |
| Bipolar and related disorders | 29604 | 9 | Bipolar I disorder, single manic episode, severe, specified as with psychotic behavior |
| Bipolar and related disorders | 29644 | 9 | Bipolar I disorder, most recent episode (or current) manic, severe, specified as with psychotic behavior |
| Bipolar and related disorders | 29654 | 9 | Bipolar I disorder, most recent episode (or current) depressed, severe, specified as with psychotic behavior |
| Bipolar and related disorders | F302 | 10 | Manic episode, severe with psychotic symptoms |
| Mental health symptom | 7801 | 9 | Hallucinations |
| Mental health symptom | R440 | 10 | Auditory hallucinations |
| Mental health symptom | R441 | 10 | Visual hallucinations |
| Mental health symptom | R442 | 10 | Other hallucinations |
| Mental health symptom | R443 | 10 | Hallucinations, unspecified |
| Mental health symptom | R462 | 10 | Strange and inexplicable behavior |
| Miscellaneous | F28 | 10 | Other psychotic disorders not due to a substance or known physiological condition |
| Neurocognitive disorders | 29381 | 9 | Psychotic disorder with delusions in conditions classified elsewhere |
| Neurocognitive disorders | 29382 | 9 | Psychotic disorder with hallucinations in conditions classified elsewhere |
| Schizophrenia spectrum and other psychotic disorders | 2970 | 9 | Paranoid state, simple |
| Schizophrenia spectrum and other psychotic disorders | 2971 | 9 | Delusional disorder |
| Schizophrenia spectrum and other psychotic disorders | 2972 | 9 | Paraphrenia |
| Schizophrenia spectrum and other psychotic disorders | 2973 | 9 | Shared psychotic disorder |
| Schizophrenia spectrum and other psychotic disorders | 2978 | 9 | Other specified paranoid states |
| Schizophrenia spectrum and other psychotic disorders | 2979 | 9 | Unspecified paranoid state |
| Schizophrenia spectrum and other psychotic disorders | 2980 | 9 | Depressive type psychosis |
| Schizophrenia spectrum and other psychotic disorders | 2981 | 9 | Excitative type psychosis |
| Schizophrenia spectrum and other psychotic disorders | 2983 | 9 | Acute paranoid reaction |
| Schizophrenia spectrum and other psychotic disorders | 2984 | 9 | Psychogenic paranoid psychosis |
| Schizophrenia spectrum and other psychotic disorders | 2988 | 9 | Other and unspecified reactive psychosis |
| Schizophrenia spectrum and other psychotic disorders | 2989 | 9 | Unspecified psychosis |
| Schizophrenia spectrum and other psychotic disorders | 29500 | 9 | Simple type schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29501 | 9 | Simple type schizophrenia, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29502 | 9 | Simple type schizophrenia, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29503 | 9 | Simple type schizophrenia, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29504 | 9 | Simple type schizophrenia, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29505 | 9 | Simple type schizophrenia, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29510 | 9 | Disorganized type schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29511 | 9 | Disorganized type schizophrenia, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29512 | 9 | Disorganized type schizophrenia, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29513 | 9 | Disorganized type schizophrenia, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29514 | 9 | Disorganized type schizophrenia, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29515 | 9 | Disorganized type schizophrenia, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29520 | 9 | Catatonic type schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29521 | 9 | Catatonic type schizophrenia, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29522 | 9 | Catatonic type schizophrenia, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29523 | 9 | Catatonic type schizophrenia, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29524 | 9 | Catatonic type schizophrenia, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29525 | 9 | Catatonic type schizophrenia, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29530 | 9 | Paranoid type schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29531 | 9 | Paranoid type schizophrenia, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29532 | 9 | Paranoid type schizophrenia, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29533 | 9 | Paranoid type schizophrenia, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29534 | 9 | Paranoid type schizophrenia, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29535 | 9 | Paranoid type schizophrenia, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29540 | 9 | Schizophreniform disorder, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29541 | 9 | Schizophreniform disorder, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29542 | 9 | Schizophreniform disorder, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29543 | 9 | Schizophreniform disorder, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29544 | 9 | Schizophreniform disorder, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29545 | 9 | Schizophreniform disorder, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29550 | 9 | Latent schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29551 | 9 | Latent schizophrenia, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29552 | 9 | Latent schizophrenia, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29553 | 9 | Latent schizophrenia, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29554 | 9 | Latent schizophrenia, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29555 | 9 | Latent schizophrenia, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29560 | 9 | Schizophrenic disorders, residual type, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29561 | 9 | Schizophrenic disorders, residual type, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29562 | 9 | Schizophrenic disorders, residual type, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29563 | 9 | Schizophrenic disorders, residual type, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29564 | 9 | Schizophrenic disorders, residual type, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29565 | 9 | Schizophrenic disorders, residual type, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29570 | 9 | Schizoaffective disorder, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29571 | 9 | Schizoaffective disorder, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29572 | 9 | Schizoaffective disorder, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29573 | 9 | Schizoaffective disorder, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29574 | 9 | Schizoaffective disorder, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29575 | 9 | Schizoaffective disorder, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29580 | 9 | Other specified types of schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29581 | 9 | Other specified types of schizophrenia, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29582 | 9 | Other specified types of schizophrenia, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29583 | 9 | Other specified types of schizophrenia, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29584 | 9 | Other specified types of schizophrenia, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29585 | 9 | Other specified types of schizophrenia, in remission |
| Schizophrenia spectrum and other psychotic disorders | 29590 | 9 | Unspecified schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | 29591 | 9 | Unspecified schizophrenia, subchronic |
| Schizophrenia spectrum and other psychotic disorders | 29592 | 9 | Unspecified schizophrenia, chronic |
| Schizophrenia spectrum and other psychotic disorders | 29593 | 9 | Unspecified schizophrenia, subchronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29594 | 9 | Unspecified schizophrenia, chronic with acute exacerbation |
| Schizophrenia spectrum and other psychotic disorders | 29595 | 9 | Unspecified schizophrenia, in remission |
| Schizophrenia spectrum and other psychotic disorders | F060 | 10 | Psychotic disorder with hallucinations due to known physiological condition |
| Schizophrenia spectrum and other psychotic disorders | F061 | 10 | Catatonic disorder due to known physiological condition |
| Schizophrenia spectrum and other psychotic disorders | F200 | 10 | Paranoid schizophrenia |
| Schizophrenia spectrum and other psychotic disorders | F201 | 10 | Disorganized schizophrenia |
| Schizophrenia spectrum and other psychotic disorders | F202 | 10 | Catatonic schizophrenia |
| Schizophrenia spectrum and other psychotic disorders | F203 | 10 | Undifferentiated schizophrenia |
| Schizophrenia spectrum and other psychotic disorders | F205 | 10 | Residual schizophrenia |
| Schizophrenia spectrum and other psychotic disorders | F2081 | 10 | Schizophreniform disorder |
| Schizophrenia spectrum and other psychotic disorders | F2089 | 10 | Other schizophrenia |
| Schizophrenia spectrum and other psychotic disorders | F209 | 10 | Schizophrenia, unspecified |
| Schizophrenia spectrum and other psychotic disorders | F22 | 10 | Delusional disorders |
| Schizophrenia spectrum and other psychotic disorders | F23 | 10 | Brief psychotic disorder |
| Schizophrenia spectrum and other psychotic disorders | F24 | 10 | Shared psychotic disorder |
| Schizophrenia spectrum and other psychotic disorders | F250 | 10 | Schizoaffective disorder, bipolar type |
| Schizophrenia spectrum and other psychotic disorders | F251 | 10 | Schizoaffective disorder, depressive type |
| Schizophrenia spectrum and other psychotic disorders | F258 | 10 | Other schizoaffective disorders |
| Schizophrenia spectrum and other psychotic disorders | F259 | 10 | Schizoaffective disorder, unspecified |
| Schizophrenia spectrum and other psychotic disorders | F29 | 10 | Unspecified psychosis not due to a substance or known physiological condition |
| Medications |
|---|
| Anesthetics |
| Propofol |
| Fentanyl (base) (citrate) |
| Dexmedetomidine HCl |
| Rocuronium bromide |
| Ketamine HCl |
| Morphine sulfate |
| Pentobarbital sodium |
| Etomidate |
| Vecuronium bromide |
| Antibiotics |
| Cephalexin (HCl) (monohydrate) |
| Antibiotic combinations |
| Azithromycin (dihydrate) |
| Ceftriaxone sodium |
| Sulfamethoxazole and trimethoprim (co‐trimoxazole) |
| Clindamycin (HCl) (palmitate) (phosphate) |
| Amoxicillin trihydrate and potassium clavulanate |
| Doxycycline (calcium) (hyclate) (monohydrate) |
| Metronidazole (HCl) |
| Vancomycin (HCl) |
| Cefazolin sodium |
| Nitrofurantoin |
| Ciprofloxacin (HCl) |
| Penicillin V potassium |
| Penicillin G benzathine |
| Antibiotic and steroid combinations |
| Cefdinir |
| Ampicillin sodium and sulbactam sodium |
| Cefotaxime sodium |
| Penicillin G benzathine and procaine |
| Ampicillin (anhydrous) (sodium) (trihydrate) |
| Nafcillin sodium |
| Cefadroxil (monohydrate) |
| Cefoxitin sodium |
| Cefprozil (anhydrous) |
| Cefixime |
| Clarithromycin |
| Tetracycline HCl |
| Linezolid |
| Rifaximin |
| Neomycin sulfate and polymyxin B sulfate |
| Rifampin |
| Amoxicillin trihydrate |
| Minocycline (HCl) |
| Antidepressants |
| Sertraline HCl |
| Fluoxetine HCl |
| Trazodone HCl |
| Escitalopram oxalate |
| Bupropion (HBr) (HCl) |
| Citalopram HBr |
| Duloxetine HCl |
| Venlafaxine |
| Amitriptyline HCl |
| Paroxetine (HCl) (mesylate) |
| Desvenlafaxine |
| Mirtazapine |
| Anti‐emetics |
| Promethazine HCl |
| Ondansetron HCl |
| Anti‐epileptics |
| Valproic acid and derivatives |
| Clonazepam |
| Oxcarbazepine |
| Topiramate |
| Levetiracetam |
| Zonisamide |
| Carbamazepine |
| Clobazam |
| Ethosuximide |
| Lacosamide |
| Antipsychotics |
| Risperidone |
| Olanzapine |
| Aripiprazole |
| Haloperidol (decanoate) (lactate) |
| Quetiapine fumarate |
| Ziprasidone (HCl) (mesylate) |
| Chlorpromazine HCl |
| Clozapine |
| Asenapine |
| Paliperidone |
| Lurasidone HCl |
| Perphenazine |
| Anxiolytics |
| Lorazepam |
| Diphenhydramine (citrate) (HCl) |
| Hydroxyzine (HCl) (pamoate) |
| Midazolam HCl |
| Alprazolam |
| Diazepam |
| Buspirone HCl |
| Immune globulin (IVIG) |
| Mood stabilizers |
| Lithium (carbonate) (citrate) |
| Lamotrigine |
| Steroids |
| Dexamethasone |
| Methylprednisolone |
| Prednisone |
| Prednisolone |
| Hydrocortisone |
| Beclomethasone dipropionate |
| Imaging Brain MRI |
| Head CT |
| Head ultrasound |
| Abdominal imaging |
| Abdomen supine X‐ray |
| Upper abdomen ultrasound real‐time |
| Noninvasive vascular ultrasound of the abdomen |
| Retroperitoneum ultrasound real‐time |
| Abdomen supine upright decubitus and cross‐table X‐ray |
| Abdomen and pelvis CT scan |
| Noninvasive vascular Doppler of the abdomen |
| Lower abdomen MRI |
| Upper abdomen MRI |
| Upper abdomen ultrasound B‐mode |
| Lower abdomen CT scan |
| Noninvasive vascular ultrasound of thoracic and abdominal aorta |
| Noninvasive vascular Doppler of thoracic and abdominal aorta |
| Abdomen arteriography CT scan |
References
- Practitioner review: psychosis in children and adolescents.. J Child Psychol Psychiatry., 2023. [DOI | PubMed]
- Common and costly hospitalizations for pediatric mental health disorders.. Pediatrics., 2014. [DOI | PubMed]
- 3 American Psychiatric Association . Diagnostic and statistical manual of mental disorders (5th ed., text rev). 2022. 10.1176/appi.books.9780890425787
- Collaborative care in the identification and management of psychosis in adolescents and young adults.. Pediatrics., 2021. [DOI | PubMed]
- Prevalence of psychotic symptoms in childhood and adolescence: a systematic review and meta‐analysis of population‐based studies.. Psychol Med., 2012. [DOI | PubMed]
- Schizophrenia: a concise overview of incidence, prevalence, and mortality.. Epidemiol Rev., 2008. [DOI | PubMed]
- Secondary psychoses: an update.. World Psychiatry., 2013. [DOI | PubMed]
- Practice parameter for the assessment and treatment of children and adolescents with schizophrenia.. J Am Acad Child Adolesc Psychiatry., 2013. [DOI | PubMed]
- Initial medical work‐up of first‐episode psychosis: a conceptual review.. Early Interv Psychiatry., 2009. [DOI | PubMed]
- First episode psychosis medical workup.. Child Adolesc Psychiatr Clin N Am., 2020. [DOI | PubMed]
- Pediatric complex chronic conditions classification system version 2: updated for ICD‐10 and complex medical technology dependence and transplantation.. BMC Pediatr., 2014. [DOI | PubMed]
- Classification system for international classification of diseases, ninth revision, clinical modification and tenth revision pediatric mental health disorders.. JAMA Pediatr., 2020. [DOI | PubMed]
- Medical etiologies of secondary psychosis in children and adolescents.. Child Adolesc Psychiatr Clin N Am., 2020. [DOI | PubMed]
- An overview of medical risk factors for childhood psychosis: implications for research and treatment.. Schizophr Res., 2018. [DOI | PubMed]
- Approach to New‐Onset psychosis in pediatrics: a review of current practice and an interdisciplinary consensus‐driven clinical pathway at a single‐center institution.. J Child Neurol., 2023. [DOI | PubMed]
- Clinical practice guidelines: the good, the bad, and the ugly.. Injury., 2023. [DOI | PubMed]
- Primary psychosis: risk and protective factors and early detection of the onset.. Diagnostics., 2021. [DOI | PubMed]
- Psychosocial treatment for First‐Episode psychosis: a research update.. Am J Psychiatry., 2005. [DOI | PubMed]
- Early intervention services, cognitive‐behavioural therapy and family intervention in early psychosis: systematic review.. Br J Psychiatry., 2010. [DOI | PubMed]
- Relationship between duration of untreated psychosis and outcome in first‐episode schizophrenia: a critical review and meta‐analysis.. Am J Psychiatry., 2005. [DOI | PubMed]
- Evidence for overuse of medical services around the world.. Lancet., 2017. [DOI | PubMed]
- US national and State‐Level prevalence of mental health disorders and disparities of mental health care use in children.. JAMA Pediatr., 2019. [DOI | PubMed]
- National trends in mental health‐related emergency department visits by children and adults, 2009‐2015.. Am J Emerg Med., 2020. [DOI | PubMed]
- A clinical approach to new‐onset psychosis associated with immune dysregulation: the concept of autoimmune psychosis.. J Neuroinflammation., 2018. [DOI | PubMed]
- Autoimmune encephalitis: clinical spectrum and management.. Pract Neurol., 2021. [DOI | PubMed]
- Acute medical workup for New‐Onset psychosis in children and adolescents: a retrospective cohort.. J Hosp Med., 2022. [DOI | PubMed]
- The occurrence of organic disease of possible or probable aetiological significance in a population of 268 cases of first episode schizophrenia.. Psychol Med., 1987. [DOI | PubMed]
- Structural neuroimaging in psychosis: a systematic review and economic evaluation.. Health Technol Assess., 2008. [DOI]
- The role of MRI and CT of the brain in first episodes of psychosis and behavioural abnormality.. Clin Radiol., 2021. [DOI]
- On the usefulness of structural brain imaging for young first episode inpatients with psychosis.. Psychiatry Res Neuroimaging., 2014. [DOI]